
Configuration Path Study of Influencing Factors on Health Information-Sharing Behavior among Users of Online Health Communities: Based on SEM and fsQCA Methods

Abstract
:1. Introduction
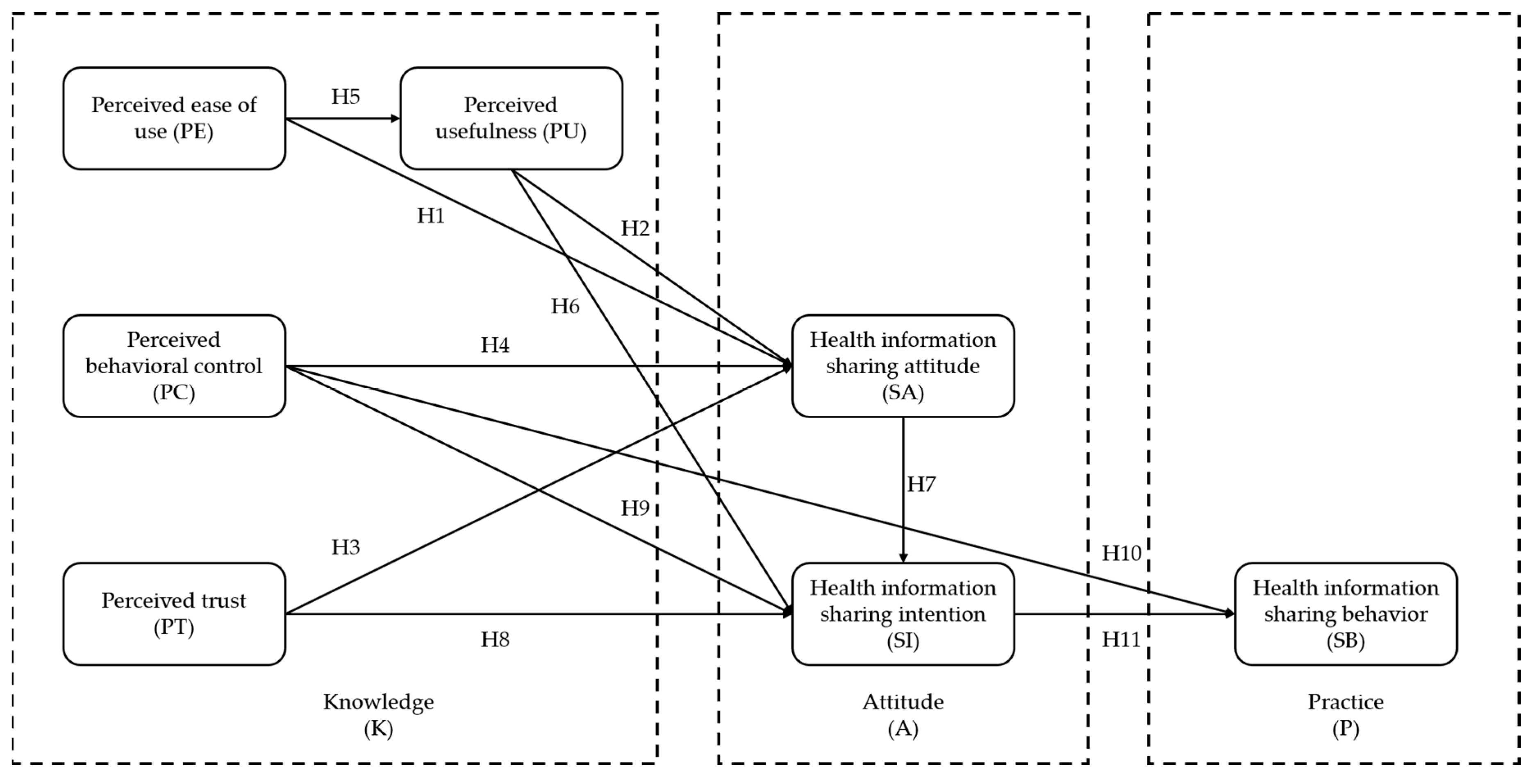
1.1. Research Model and Hypothesis Development
1.1.1. Technology Acceptance Model
1.1.2. Theory of Planned Behavior
1.1.3. “Knowledge-Attitude-Practice” Theory
1.1.4. Analysis of Factors Affecting Health Information-Sharing Attitude
1.1.5. Factors Affecting Perceived Usefulness
1.1.6. Analysis of Factors Influencing Health Information-Sharing Intention
1.1.7. Analysis of Factors Influencing Health Information-Sharing Behavior
2. Methods
2.1. Data Collection
2.2. Data Analysis
2.2.1. Exploratory Factor Analysis
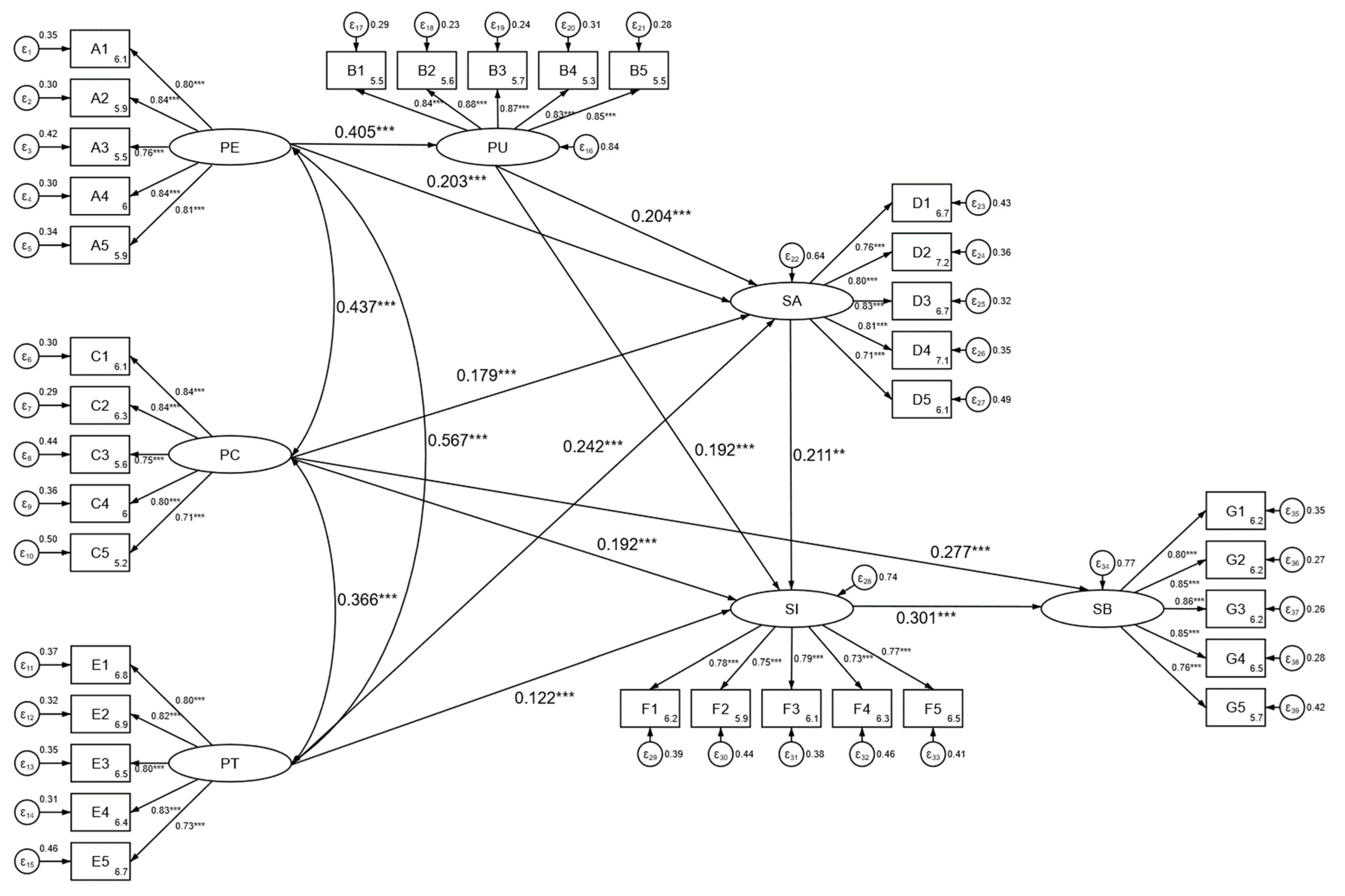
2.2.2. Confirmatory Factor Analysis
2.2.3. Model Verification
2.3. Empirical Analysis Based on fsQCA
2.3.1. Configuration Path Decomposition
2.3.2. Variable Assignment and Calibration
2.3.3. Necessity Analysis
2.3.4. Condition Configuration Analysis
3. Result
3.1. Configuration Path Analysis with Health Information-Sharing Attitude and Health Information-Sharing Intention as Outcome Variables
3.2. Configuration Path Analysis with Health Information-Sharing Behavior as Outcome Variable
4. Discussion
4.1. Main Findings
4.2. Theoretical Contributions and Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chu, J.T.; Wang, M.P.; Shen, C.; Viswanath, K.; Lam, T.H.; Chan, S.S.C. How, When and Why People Seek Health Information Online: Qualitative Study in Hong Kong. Interact. J. Med. Res. 2017, 6, e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, Y.; Shi, W. The influence of the community climate on users’ knowledge-sharing intention: The social cognitive theory perspective. Behav. Inf. Technol. 2020, 41, 307–323. [Google Scholar] [CrossRef]
- Zhou, J. Factors Influencing People’s Personal Information Disclosure Behaviors in Online Health Communities: A Pilot Study. Asia-Pac. J. Public Health 2018, 30, 286–295. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, K.; Street, N. Analyzing and Predicting User Participations in Online Health Communities: A Social Support Perspective. J. Med. Internet Res. 2017, 19, e130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priya, N. Information seeking and social support in online health communities: Impact on patients’ perceived empathy. J. Am. Med. Inform. Assoc. 2011, 18, 298–304. [Google Scholar]
- McLoughlin, C.; Patel, K.; O’Callaghan, T.; Reeves, S. The Use of Virtual Communities of Practice to Improve Interprofessional Collaboration and Education: Findings from an Integrated Review. J. Interprof. Care. 2018, 32, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Gao, S.; Cheng, Y.; Meng, F. Encouraging physicians’ continuous knowledge-sharing in online health communities: A motivational perspective. Front. Public Health 2022, 10, 1036366. [Google Scholar] [CrossRef]
- Zhou, T. Examining online health community users’ sharing behaviour: A social influence perspective. Inf. Dev. 2021, 38, 599–608. [Google Scholar] [CrossRef]
- Hajli, M.N. Developing online health communities through digital media. Int. J. Inf. Manag. 2014, 34, 311–314. [Google Scholar] [CrossRef]
- Maloney-Krichmar, D.; Preece, J. A multilevel analysis of sociability, usability, and community dynamics in an online health community. ACM Trans. Comput. Hum. Interact. 2005, 12, 201–232. [Google Scholar] [CrossRef]
- Martijn, V.D.; Faber, M.J.; Aarts, J.W.; Kremer, J.A.; Munneke, M.; Bloem, B.R. Using online health communities to deliver patient-centered care to people with chronic conditions. J. Med. Internet Res. 2013, 15, e115. [Google Scholar]
- Yan, Z.; Wang, S.; Chen, J. Knowledge sharing in online health communities: A social exchange theory perspective. Inf. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Hargreaves, S.; Bath, M.; Duffin, D. Sharing and empathy in digital spaces: Qualitative study of online health forums for breast cancer and motor neuron disease (amyotrophic lateral sclerosis). J. Med. Internet Res. 2018, 20, e222. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.; Koola, J.; Contreras, A.; Castillo, A.K.; Ruiz, M.; Tedone, K.G.; Yakuta, M.; Schiaffino, M.K. Consumer Health Informatics Adoption among Underserved Populations: Thinking beyond the Digital Divide. Yearb. Med. Inform. 2018, 27, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Lober, W.B.; Zierler, B.; Herbaugh, A.; Shinstrom, S.E.; Stolyar, A.; Kim, E.H.; Kim, Y. Barriers to the use of a personal health record by an elderly population. In Proceedings of the AMIA Annual Symposium Proceedings, Washington, DC, USA, 22–26 October 2005; AMIA: Bethesda, MD, USA, 2006; pp. 514–518. [Google Scholar]
- Alipour, J.; Payandeh, A. Assessing the Level of Digital Health Literacy among Healthcare Workers of Teaching Hospitals in the Southeast of Iran. Informatics Med. Unlocked. 2022, 29, 100868. [Google Scholar] [CrossRef]
- Goh, J.M.; Gao, G.G.; Agarwal, R. The Creation of Social Value: Can an Online Health Community Reduce Rural-Urban Health Disparities? MIS Q. 2016, 40, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Guo, F.; Xu, T.; Li, Y. What motivates physicians to share free health information on online health platforms? Inf. Process. Manag. 2020, 57, 102166. [Google Scholar] [CrossRef]
- Meng, F.; Zhang, X.; Liu, L.; Ren, C. Converting readers to patients? From free to paid knowledge-sharing in online health communities. Inf. Process. Manag. 2021, 58, 102490. [Google Scholar] [CrossRef]
- Liu, Y.; Ren, C.; Shi, D.; Li, K.; Zhang, X. Evaluating the social value of online health information for third-party patients: Is uncertainty always bad? Inf. Process. Manag. 2020, 57, 102259. [Google Scholar] [CrossRef]
- Guo, F.; Zhou, A.; Chang, W.; Sun, X.; Zou, B. Is physician online information sharing always beneficial to patient education? An attention perspective. Front. Public Health 2022, 10, 987766. [Google Scholar] [CrossRef]
- Lei, Y.; Xu, S.; Zhou, L. User Behaviors and User-Generated Content in Chinese Online Health Communities: Comparative Study. J. Med. Internet Res. 2021, 23, e19183. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, S.; Deng, Z.; Chen, X. Knowledge sharing motivations in online health communities: A comparative study of health professionals and normal users. Comput. Hum. Behav. 2017, 75, 797–810. [Google Scholar] [CrossRef]
- Gabarron, E.; Serrano, J.A.; Wynn, R.; Armayones, M. Avatars using computer/smartphone mediated communication and social networking in prevention of sexually transmitted diseases among North-Norwegian youngsters. BMC Med. Inform. Decis. Mak. 2012, 12, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, F.D. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Cust, G. Sutherland Health Education: Perspectives and Chances; George Allan and Unwin: London, UK, 1979; pp. 82–83. [Google Scholar]
- Suh, M.; Hsieh, G. The “Had Mores”: Exploring Korean Immigrants’ Information Behavior and ICT Usage When Settling in the United States. J. Assoc. Inf. Sci. Technol. 2019, 70, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.P.; Chiang, Y.F.; Huang, H.C. How experience-driven community identification generates trust and engagement. Online Inf. Rev. 2012, 36, 72–88. [Google Scholar] [CrossRef] [Green Version]
- Hansen, J.M.; Saridakis, G.; Benson, V. Risk, Trust, and the Interaction of Perceived Ease of Use and Behavioral Control in Predicting Consumers’ Use of Social Media for Transactions. Comput. Hum. Behav. 2018, 80, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Koufaris, M. Applying the Technology Acceptance Model and Flow Theory to Online Consumer Behavior. Inf. Syst. Res. 2002, 13, 205–223. [Google Scholar] [CrossRef] [Green Version]
- Rese, A.; Schreiber, R.S.; Baier, R.D. Technology acceptance modeling of augmented reality at the point of sale: Can surveys be replaced by an analysis of online reviews? J. Retail. Consum. Serv. 2014, 21, 869–876. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A model of the antecedents of perceived ease of use: Development and test. Decis. Sci. 1996, 27, 451–481. [Google Scholar] [CrossRef]
- Yoon, C. Theory of planned behavior and ethics theory in digital piracy: An integrated model. J. Bus. Ethics. 2011, 100, 405–417. [Google Scholar] [CrossRef]
- Wang, W.T.; Wang, Y.S.; Liu, E.R. The Stickiness Intention of Group-buying Websites: The Integration of the Commitment-trust Theory and E-commerce Success Model. Inf. Manag. 2016, 53, 625–642. [Google Scholar] [CrossRef]
- Oum, S.; Han, D.W. An empirical study of the determinants of the intention to participate in user-created contents (UCC) services. Expert Syst. Appl. 2011, 38, 15110–15121. [Google Scholar] [CrossRef]
- McKnight, D.H.; Choudhury, V.; Kacmar, C. Developing and Validating Trust Measures for E-Commerce: An Integrative Typology. Inf. Syst. Res. 2002, 13, 334–359. [Google Scholar] [CrossRef] [Green Version]
- Ragin, C.C. The Comparative Method: Moving Beyond Qualitative and Quantitative Strategies; University of California Press: Berkeley, CA, USA; Los Angeles, CA, USA; London, UK, 1987; p. 59. [Google Scholar]
- Ragin, C.C. Redesigning Social Inquiry: Fuzzy Sets and Beyond; University of Chicago Press: Chicago, IL, USA, 2008. [Google Scholar]
- Ragin, C.C.; Rubinson, C.; Schaefer, D. User’s Guide to Fuzzy-Set/Qualitative Comparative Analysis; University of Arizona: Tucson, AZ, USA, 2008; Volume 3, pp. 87–101. [Google Scholar]
- Rihoux, B.; Ragin, C.C. Configurational Comparative Methods: Qualitative Comparative Analysis (QCA) and Related Techniques; Sage Publications: Thousand Oaks, CA, USA, 2009; pp. 23–45. [Google Scholar]
- Fiss, P.C. Building better casual theories: A fuzzy set approach to typologies in organizational research. Acad. Manag. J. 2011, 54, 393–420. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Serial Number | Variable | Measurement Item Content | Source |
|---|---|---|---|
| 1 | Perceived ease of use (PE) | A1. The way of sharing health information in online health communities is easy to learn and does not take too much time. A2. The interface design of online health communities is user-friendly and easy to understand. A3. The health information shared in the communities is highly relevant to the topic and easy to share. A4. Sharing health information in online health communities is quick and easy for me. A5. Editing and sharing health information in online health communities is easy, and I can express the information I want to share clearly through text, images, videos, and other means. | Hansen J M [30], Koufaris M [31] |
| 2 | Perceived usefulness (PU) | B1. Sharing health information in the communities can help me solve some health problems. B2. Sharing health information in the communities allows me to obtain comments and feedback from other users and experts. B3. Health information in the communities broadens my relevant knowledge. B4. Most of the health information pushed by the communities is what I need. B5. High-quality information that I share in the communities will be promptly pushed by the communities. | Rese A [32], Venkatesh and Davis [33] |
| 3 | Perceived behavioral control (PC) | C1. Whether or not I share health information in the communities depends entirely on me. C2. I am confident that I can share health information in the communities. C3. The communities provide me with all the necessary conditions for sharing health information online. C4. I can withdraw the health information I shared in the communities at any time. C5. I can decide who to share my health information with. | Yoon C [34] |
| 4 | Health information-sharing attitude (SA) | D1. I am willing to share health information in the online health communities. D2. Sharing health information in the communities gives me pleasure. D3. I think sharing health information in the online health communities can help others. D4. I think sharing health information in the online health communities can benefit me. D5. I will continue to choose the online health communities to deal with my health problems. | Wang W T [35], Venkatesh and Davis [33] |
| 5 | Perceived trust (PT) | E1. I believe the communities are trustworthy and will not disclose my personal information at will. E2. I believe the communities have the ability to ensure the authenticity of health information in the communities. E3. I believe that the health information shared among community members is trustworthy. E4. I trust that the online health communities have the ability to provide me with useful health information. E5. I can choose not to provide personal information that I do not want to provide (such as the communities’ anonymous system). | Oum S [36], McKnight [37] |
| 6 | Health information-sharing intention (SI) | F1. I am willing to share health information through the online health communities. F2. When I encounter problems, I am willing to share my health information to get advice on solving them. F3. I am willing to forward and disseminate health information shared by others. F4. I agree with the way and process of sharing health information in the online health communities. F5. I am willing to recommend others to use the online health communities to share health information. | Venkatesh Davis [33] |
| 7 | Health information-sharing behavior (SB) | G1. I often browse health information in the communities and continue to pay attention to some shared information. G2. I often share health information in the communities, such as health problems, treatment methods, and experiences. G3. When discussing related health issues with community members, I will continue to participate in the discussion. G4. I often comment and forward health information in the communities. G5. When encountering problems, I often seek help through the communities. | Yan Z J [12] |
| Name | Factor Loading Coefficient | Communality | ||||||
|---|---|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 | Factor 7 | ||
| A1 | 0.754 | 0.706 | ||||||
| A2 | 0.819 | 0.772 | ||||||
| A3 | 0.774 | 0.687 | ||||||
| A4 | 0.767 | 0.746 | ||||||
| A5 | 0.789 | 0.733 | ||||||
| B1 | 0.830 | 0.772 | ||||||
| B2 | 0.852 | 0.813 | ||||||
| B3 | 0.845 | 0.802 | ||||||
| B4 | 0.805 | 0.757 | ||||||
| B5 | 0.841 | 0.789 | ||||||
| C1 | 0.811 | 0.741 | ||||||
| C2 | 0.859 | 0.793 | ||||||
| C3 | 0.741 | 0.650 | ||||||
| C4 | 0.805 | 0.715 | ||||||
| C5 | 0.744 | 0.613 | ||||||
| D1 | 0.702 | 0.647 | ||||||
| D2 | 0.754 | 0.699 | ||||||
| D3 | 0.777 | 0.743 | ||||||
| D4 | 0.780 | 0.736 | ||||||
| D5 | 0.786 | 0.663 | ||||||
| E1 | 0.752 | 0.707 | ||||||
| E2 | 0.799 | 0.744 | ||||||
| E3 | 0.766 | 0.716 | ||||||
| E4 | 0.789 | 0.747 | ||||||
| E5 | 0.740 | 0.648 | ||||||
| F1 | 0.787 | 0.694 | ||||||
| F2 | 0.771 | 0.667 | ||||||
| F3 | 0.776 | 0.702 | ||||||
| F4 | 0.776 | 0.658 | ||||||
| F5 | 0.783 | 0.675 | ||||||
| G1 | 0.770 | 0.719 | ||||||
| G2 | 0.816 | 0.774 | ||||||
| G3 | 0.801 | 0.787 | ||||||
| G4 | 0.805 | 0.772 | ||||||
| G5 | 0.802 | 0.705 | ||||||
| Eigenvalue | 3.937 | 3.728 | 3.622 | 3.555 | 3.553 | 3.462 | 3.435 | - |
| Variance explained ratio | 11.248% | 10.651% | 10.349% | 10.158% | 10.150% | 9.890% | 9.815% | - |
| Cumulative variance explained ratio | 11.248% | 21.899% | 32.248% | 42.406% | 52.556% | 62.447% | 72.262% | - |
| KMO measure | 0.933 | - | ||||||
| Bartlett’s sphericity test | 13,540.698 | - | ||||||
| df | 595 | - | ||||||
| p-value | *** | - | ||||||
| Variable | Cronbach’s α | AVE | CR |
|---|---|---|---|
| Perceived ease of use | 0.905 | 0.659 | 0.906 |
| Perceived usefulness | 0.931 | 0.730 | 0.931 |
| Perceived behavioral control | 0.887 | 0.622 | 0.891 |
| Health information-sharing attitude | 0.886 | 0.615 | 0.889 |
| Perceived trust | 0.897 | 0.637 | 0.897 |
| Health information-sharing intention | 0.878 | 0.592 | 0.879 |
| Health information-sharing behavior | 0.914 | 0.685 | 0.916 |
| Variable | PE | PU | PC | SA | PT | SI | SB |
|---|---|---|---|---|---|---|---|
| Perceived ease of use (PE) | 0.812 | ||||||
| Perceived usefulness (PU) | 0.352 | 0.855 | |||||
| Perceived behavioral control (PC) | 0.382 | 0.276 | 0.789 | ||||
| Health information-sharing attitude (SA) | 0.432 | 0.392 | 0.368 | 0.784 | |||
| Perceived trust (PT) | 0.498 | 0.408 | 0.316 | 0.447 | 0.798 | ||
| Health information-sharing intention (SI) | 0.366 | 0.339 | 0.333 | 0.364 | 0.317 | 0.769 | |
| Health information-sharing behavior (SB) | 0.414 | 0.385 | 0.341 | 0.437 | 0.454 | 0.339 | 0.828 |
| Fit Indices | χ2 | df | χ2/df | GFI | RMSEA | CFI | NFI | NNFI |
|---|---|---|---|---|---|---|---|---|
| Optimal standard values | - | - | <3 | >0.9 | <0.10 | >0.9 | >0.9 | >0.9 |
| Statistical values | 1130.672 | 545 | 2.075 | 0.900 | 0.043 | 0.956 | 0.918 | 0.952 |
| Fit status | - | - | Ideal | Ideal | Ideal | Ideal | Ideal | Ideal |
| Hypothesis | X→Y | Non-Standardized Regression Coefficient (N-β) | Standardized Regression Coefficient (β) | Standard Error (SE) | z (CR Value) | p |
|---|---|---|---|---|---|---|
| Hypothesis 1 | Perceived ease of use→Health information-sharing attitude | 0.172 | 0.203 | 0.047 | 3.624 | *** |
| Hypothesis 2 | Perceived usefulness→Health information-sharing attitude | 0.152 | 0.204 | 0.032 | 4.697 | *** |
| Hypothesis 3 | Perceived trustworthiness→Health information-sharing attitude | 0.234 | 0.242 | 0.049 | 4.739 | *** |
| Hypothesis 4 | Perceived behavioral control→Health information-sharing attitude | 0.146 | 0.179 | 0.037 | 3.944 | *** |
| Hypothesis 5 | Perceived ease of use→Perceived usefulness | 0.458 | 0.405 | 0.051 | 9.000 | *** |
| Hypothesis 6 | Perceived usefulness→Health information-sharing intention | 0.162 | 0.192 | 0.038 | 4.228 | *** |
| Hypothesis 7 | Health information-sharing attitude→Health information-sharing intention | 0.237 | 0.211 | 0.061 | 3.868 | *** |
| Hypothesis 8 | Perceived trustworthiness→Health information-sharing intention | 0.132 | 0.122 | 0.054 | 2.433 | 0.019 |
| Hypothesis 9 | Perceived behavioral control→Health information-sharing intention | 0.175 | 0.192 | 0.044 | 3.986 | *** |
| Hypothesis 10 | Perceived behavioral control→Health information-sharing behavior | 0.254 | 0.277 | 0.042 | 5.984 | *** |
| Hypothesis 11 | Health information-sharing intention→Health information-sharing behavior | 0.302 | 0.301 | 0.048 | 6.35 | *** |
| Variable | Descriptive Statistics of Variables | Calibration Threshold | |||||
|---|---|---|---|---|---|---|---|
| Mean | Standard Deviation | Minimum Value | Maximum Value | Fully Membership | Crossover Point | Fully Non-Membership | |
| PE | 0 | 1 | −5.557 | 1.873 | 1.803 | 0.083 | −1.920 |
| PU | 0 | 1 | −5.569 | 2.049 | 1.601 | 0.243 | −1.767 |
| PC | 0 | 1 | −5.948 | 1.937 | 1.520 | 0.172 | −1.584 |
| SA | 0 | 1 | −3.861 | 1.786 | 1.639 | 0.144 | −1.587 |
| PT | 0 | 1 | −5.549 | 1.643 | 1.658 | 0.241 | −1.978 |
| SI | 0 | 1 | −4.902 | 1.600 | 1.517 | 0.146 | −2.034 |
| SB | 0 | 1 | −5.382 | 1.803 | 1.352 | 0.326 | −1.974 |
| Dependent Variable | Health Information-Sharing Attitude (SA) | Health Information-Sharing Intention (SI) | Health Information-Sharing Behavior (SB) | |||
|---|---|---|---|---|---|---|
| Consistency | Coverage | Consistency | Coverage | Consistency | Coverage | |
| PE | 0.774890 | 0.746666 | 0.752731 | 0.760490 | 0.814127 | 0.784273 |
| ~PE | 0.592860 | 0.573944 | 0.616449 | 0.778862 | 0.596409 | 0.577233 |
| PU | 0.745474 | 0.759891 | 0.728743 | 0.778862 | 0.798801 | 0.814042 |
| ~PU | 0.627480 | 0.575813 | 0.640231 | 0.616007 | 0.626086 | 0.574387 |
| PC | 0.746304 | 0.741163 | 0.735222 | 0.765568 | 0.764315 | 0.758856 |
| ~PC | 0.609699 | 0.573123 | 0.616793 | 0.607909 | 0.614482 | 0.577471 |
| PT | 0.762169 | 0.769400 | 0.724123 | 0.766444 | 0.799668 | 0.807048 |
| ~PT | 0.611506 | 0.566128 | 0.651088 | 0.632005 | 0.609891 | 0.564489 |
| SA | - | - | 0.729708 | 0.765097 | 0.769160 | 0.768963 |
| ~SA | - | - | 0.607245 | 0.594621 | 0.599625 | 0.559858 |
| SI | - | - | - | - | 0.780691 | 0.744391 |
| ~SI | - | - | - | - | 0.604867 | 0.591545 |
| Dependent Variable | Solution | Combination of Conditions | Raw Coverage | Unique Coverage | Consistency | Coverage of Solution | Consistency of Solution |
|---|---|---|---|---|---|---|---|
| SA | Complex solution | ~PE * PU * ~PC * ~PT | 0.355643 | 0.0801566 | 0.811764 | 0.601966 | 0.830939 |
| PE * PU * PC * PT | 0.521809 | 0.246323 | 0.885611 | ||||
| Parsimonious solution | ~PE * PU * ~PC * ~PT | 0.355643 | 0.0801566 | 0.811764 | 0.601966 | 0.830939 | |
| PE * PU * PC * PT | 0.521809 | 0.246323 | 0.885611 | ||||
| Intermediate solution | ~PE * PU * ~PC * ~PT | 0.355643 | 0.0801566 | 0.811764 | 0.601966 | 0.830939 | |
| PE * PU * PC * PT | 0.521809 | 0.246323 | 0.885611 | ||||
| SI | Complex solution | ~PE * PU * ~PC * ~PT * ~SA | 0.334712 | 0.103057 | 0.872194 | 0.548926 | 0.862403 |
| PE * PU * PC * PT * SA | 0.445869 | 0.214214 | 0.895907 | ||||
| Parsimonious solution | ~PE * PU * ~PC * ~PT * ~SA | 0.334712 | 0.103057 | 0.872194 | 0.548926 | 0.862403 | |
| PE * PU * PC * PT * SA | 0.445869 | 0.214214 | 0.895907 | ||||
| Intermediate solution | ~PE * PU * ~PC * ~PT * ~SA | 0.334712 | 0.103057 | 0.872194 | 0.548926 | 0.862403 | |
| PE * PU * PC * PT * SA | 0.445869 | 0.214214 | 0.895907 |
| Dependent Variable | Solution | Combination of Conditions | Raw Coverage | Unique Coverage | Consistency | Coverage of Solution | Consistency of Solution |
|---|---|---|---|---|---|---|---|
| SB | Complex solution | PE * PU * SA * PT * SI | 0.491795 | 0.0287377 | 0.944923 | 0.645424 | 0.905978 |
| PE * PU * PC * SA * PT | 0.493819 | 0.0493057 | 0.946118 | ||||
| PE * PU * PC * SA * SI | 0.467395 | 0.0228819 | 0.939475 | ||||
| PU * PC * PT * SA * SI | 0.472456 | 0.019556 | 0.943478 | ||||
| ~PE * ~PU * ~PC * ~SA * PT * SI | 0.311705 | 0.0534987 | 0.905777 | ||||
| Parsimonious solution | PE * PU * SA * PT * SI | 0.491795 | 0.056716 | 0.902363 | 0.648642 | 0.903389 | |
| PE * PU * PC * SA * PT | 0.493819 | 0.0493056 | 0.946118 | ||||
| PE * PU * PC * SA * SI | 0.467395 | 0.022882 | 0.939475 | ||||
| PU * PC * PT * SA * S | 0.472456 | 0.0175318 | 0.943478 | ||||
| ~PE * ~PU * ~PC * PT * SI | 0.338093 | 0.056716 | 0.902363 | ||||
| Intermediate solution | PE * PU * SA * PT * SI | 0.491795 | 0.0287377 | 0.944923 | 0.645424 | 0.905978 | |
| PE * PU * PC * SA * PT | 0.493819 | 0.0493057 | 0.946118 | ||||
| PE * PU * PC * SA * SI | 0.467395 | 0.0228819 | 0.939475 | ||||
| PU * PC * PT * SA * SI | 0.472456 | 0.019556 | 0.943478 | ||||
| ~PE * ~PU * ~PC * ~SA * PT * SI | 0.311705 | 0.0534987 | 0.905777 |
| Dependent Variable | Health Information-Sharing Attitude | Health Information-Sharing Intention | ||
|---|---|---|---|---|
| configuration | A1 | A2 | B1 | B2 |
| Perceived ease of use | ⊗ |  | ⊗ | |
| Perceived usefulness | | | | |
| Perceived behavioral control | ⊗ | | ⊗ | |
| Perceived trust | ⊗ | | ⊗ | |
| Health information-sharing attitude | - | - | ⊗ | |
| Consistency | 0.811764 | 0.885611 | 0.872194 | 0.895907 |
| Raw coverage | 0.355643 | 0.521809 | 0.334712 | 0.445869 |
| Unique coverage | 0.0801566 | 0.246323 | 0.103057 | 0.214214 |
| overall consistency | 0.830939 | 0.862403 | ||
| overall coverage | 0.601966 | 0.548926 | ||
represents the presence of core condition; ⊗ represents the absence of core condition; “Blank” represents that the existence or absence of the condition is uncertain.| Configuration | C1a | C1b | C1c | C2a | C2b |
|---|---|---|---|---|---|
| Perceived ease of use | | ⭙ | | | |
| Perceived usefulness | | ⭙ | | | |
| Perceived behavioral control | ⭙ | | | | |
| Perceived trust | | | | | |
| Health information-sharing attitude | | ⨂ | | | |
| Health information-sharing intention | | | | | |
| Consistency | 0.944923 | 0.905777 | 0.943478 | 0.939475 | 0.946118 |
| Coverage | 0.491795 | 0.311705 | 0.472456 | 0.467395 | 0.493819 |
| Net coverage | 0.0287377 | 0.0534987 | 0.019556 | 0.0228819 | 0.0493057 |
| overall consistency | 0.905978 | ||||
| overall coverage | 0.645424 | ||||
represents the presence of core condition; ⭙ represents the absence of core condition; ⨂ represents the absence of marginal condition; “Blank” represents that the existence or absence of the condition is uncertain.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiang, M.; Guan, T.; Lin, M.; Xie, Y.; Luo, X.; Han, M.; Lv, K. Configuration Path Study of Influencing Factors on Health Information-Sharing Behavior among Users of Online Health Communities: Based on SEM and fsQCA Methods. Healthcare 2023, 11, 1789. https://doi.org/10.3390/healthcare11121789
Xiang M, Guan T, Lin M, Xie Y, Luo X, Han M, Lv K. Configuration Path Study of Influencing Factors on Health Information-Sharing Behavior among Users of Online Health Communities: Based on SEM and fsQCA Methods. Healthcare. 2023; 11(12):1789. https://doi.org/10.3390/healthcare11121789
Chicago/Turabian StyleXiang, Minhao, Tianning Guan, Mengqi Lin, Yujie Xie, Xingyu Luo, Minghua Han, and Kun Lv. 2023. "Configuration Path Study of Influencing Factors on Health Information-Sharing Behavior among Users of Online Health Communities: Based on SEM and fsQCA Methods" Healthcare 11, no. 12: 1789. https://doi.org/10.3390/healthcare11121789