
Utilising the Implementation of Integrated Care to Develop a Pragmatic Framework for the Sustained Uptake of Service Innovations (SUSI)
 , , , , , and
, , , , , and
Abstract
:1. Introduction
Facilitating Change in Healthcare Services
2. Materials and Methods
2.1. Identifying the Core Components of the SUSI Framework
- Clinical and consumer expertise was determined in a Participatory Action Research (PAR) study conducted by the authors CF, AS, JA, JL, and RC, which identified the key issues for managers and clinicians in moving from the independent delivery of AOD and MH services to IC [34].
2.2. Establishing a Panel of Research and Clinical Experts to Construct the SUSI Framework
2.3. Organising the Core Components into a Sequential Framework
- Mapping the key change transition processes that were identified in the PAR study (securing participation; developing relationships between teams; building ownership and confidence; and embedding sustainability mechanisms (at treatment and workforce levels) into the key elements of successful organisational change models [30,31,32,33], which included establishing motivation, identifying sponsors and leadership, building support for change, managing change transition, and sustaining momentum. The goal of this activity was to identify repetition and synergy across the information and identify evidence-based core components that each related to a key focus of action that could be standardised across settings, thus establishing the core components of uptake to be articulated in the SUSI framework.
- Grouping those core components into sequential phases to reflect both the learning from the PAR study’s real-time change transition and the steps that are widely used to implement existing organisational change models. The SUSI framework was then circulated for feedback amongst clinical and research experts through ten iterations. Feedback was requested regarding whether the core components were sufficient and easy to understand and whether the sequence for implementation was pragmatic and feasible. The responses were provided by email and at monthly meetings, reviewed by the Research Advisory Group, and the final analysis was conducted by two reviewers (CF and AS). The comments were analysed deductively using the key principles identified in the research evidence [40,41,42,43], and they were analysed inductively to identify any ideas expressed that were not identified in the literature. Disagreements were discussed by CF and AS, and the framework was recirculated to the respondents until a consensus was reached on the framework that accurately reflected the feedback. The goal of this activity was to organise the agreed core components into a sequence of steps that would have most efficiently and effectively resulted in the timelier uptake of IC into routine practice, thus establishing a pragmatic and feasible process for applying the SUSI framework in practice.
3. Results
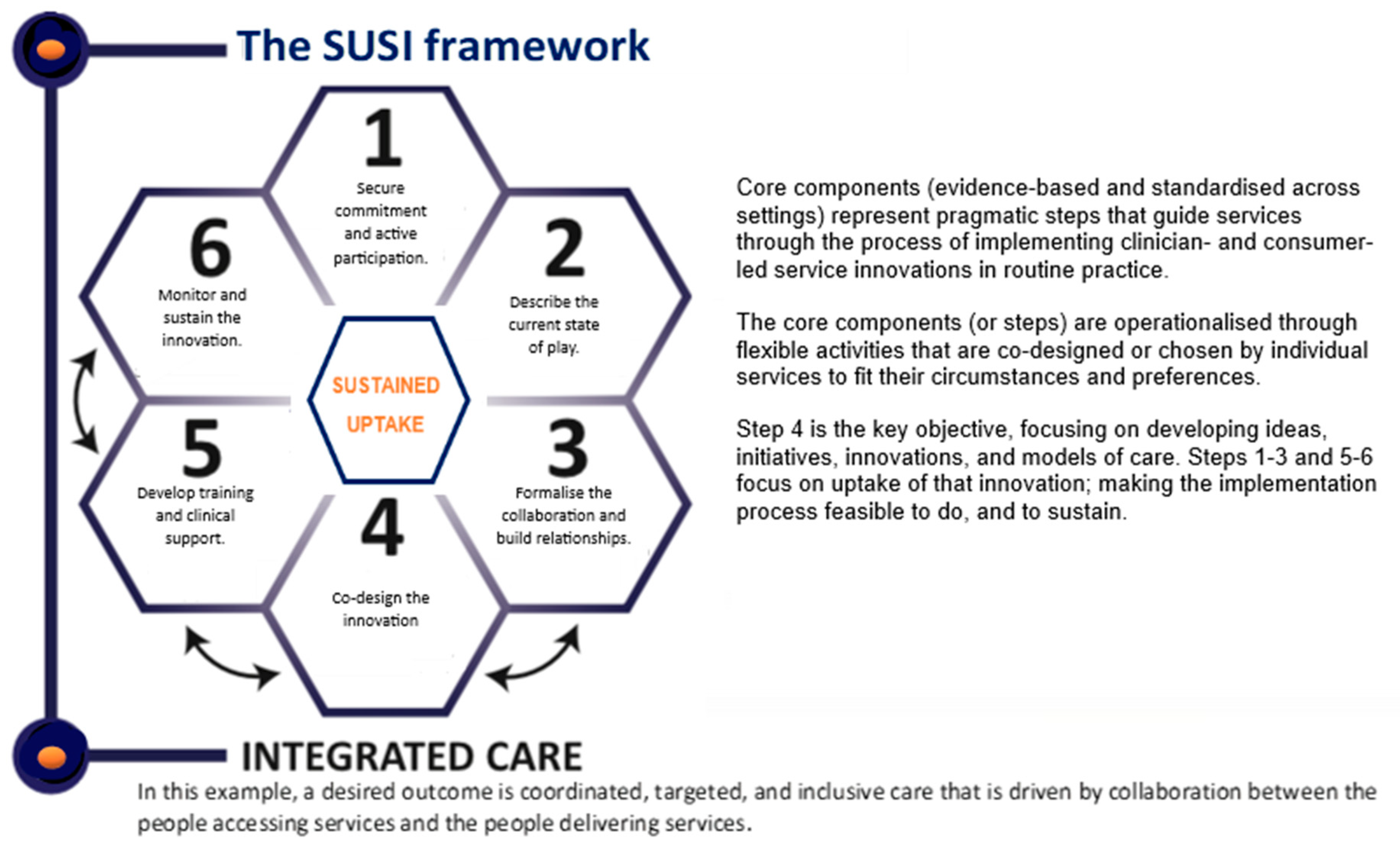
The Core Components of the SUSI Framework and Their Operationalisation
- Core component 1. Secure Commitment and Active Participation.
- Service managers and clinical leads. Clinicians are unlikely to engage in collaboration and practice change if their line supervisor is not actively supportive of the process. Clinical leads and service managers can ensure effective service planning and delivery, and they are well-positioned to lead and/or support innovations with staff and consumers. Participation at this level establishes IC as a priority and demonstrates to the staff that their involvement is valued and taken seriously. Involvement is also required from executive (or senior) managers, however, to ensure the clinical managers’ role expectations are met and their decisions are supported, for example, by allocating time for staff to take part in co-designed activities. If securing commitment and participation from clinical/service managers is successful, the process of securing a commitment from senior managers can then be taken appropriately and optimised for success.
- Senior (Executive) managers. Sustainable change requires a commitment to system-level change. For example, allocating designated leaders to drive the shift to IC increased the services’ capacity to maintain momentum in the change process whilst also allowing time to develop sustainability mechanisms, such as strategically identified Performance Indicators. Without input from the executive level about how to create and support designated leaders on the frontline, however, known barriers (e.g., competing clinical priorities, staff shortages, and organisational changes) are likely to prevent a successful change transition. This step acknowledges and draws upon expertise from the executive level, creates opportunities for access to other initiatives and resources, and ensures the proposed innovation aligns with the health services’ priorities and limitations.
- Clinicians and frontline staff. This step establishes staff confidence and interest in delivering IC and works to secure active participation from clinicians to drive the co-design and co-implementation process. Once participation is established, the implementation can draw on the clinical expertise that already exists within the workforce to improve staff confidence and capability. This step enables the development of practices that staff are more likely to adopt.
- Clients of the participating health service (consumers, people with lived experience). Consumer participation is key to designing care that meets the needs of the people most likely to seek that care. Navigating complex systems can be difficult, but involvement from consumers from the design phase onward can help services to identify those difficulties as well as strategies to reduce their occurrence or impact. This step enables the development of practices that are acceptable and relevant to consumers and are, therefore, more likely to be used.
- Core component 2. Describe the Current State of Play.
- Core component 3. Formalise Collaboration and Build Relationships.
- Core component 4. Co-design the Innovation.
- Core component 5. Develop Training & Clinical Support (for delivering new procedures).
- Core component 6. Monitor and Sustain the Innovation.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Samokhvalov, A.; Awan, S.; George, T.; Irving, J.; Le Foll, B.; Perrotta, S.; Probst, C.; Voore, P.; Rehm, J. Integrated care pathway for cooccurring major depressive and alcohol use disorders: Outcomes of the first two years. Am. J. Addict. 2017, 26, 602–609. [Google Scholar] [CrossRef]
- Minkoff, K.; Covell, N.H. Recommendations for integrated systems and services for people with co-occurring mental health and substance use conditions. Psychiatr. Serv. 2022, 73, 686–689. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration (SAMHSA). Treating Concurrent Substance Use among Adults; SAMHSA Publication No. PEP21-06-02-002; National Mental Health and Substance Use Policy Laboratory, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2021. Available online: https://store.samhsa.gov/sites/default/files/pep21-06-02-002.pdf (accessed on 12 October 2022).
- National Institute for Health and Care Excellence. Coexisting Severe Mental Illness and Substance Misuse: Community Health and Social Care Services; NICE Guideline [NG58]; National Institute for Health and Care Excellence: London, UK, 2016; Available online: https://www.nice.org.uk/guidance/ng58 (accessed on 10 November 2021).
- NSW Mental Health Commission. Living Well: A Strategic Plan for Mental Health in NSW 2014–2024; NSW Mental Health Commission: Sydney, Australia, 2014; Available online: https://www.nswmentalhealthcommission.com.au/report/living-well-strategic-plan-mental-health-nsw-2014-2024 (accessed on 10 November 2021).
- Hakobyan, S.; Vazirian, S.; Lee-Cheong, S.; Krausz, M.; Honer, W.G.; Schutz, C.G. Concurrent Disorder Management Guidelines. Systematic Review. J. Clin. Med. 2020, 9, 2406. [Google Scholar] [CrossRef] [PubMed]
- Baxter, S.; Johnson, M.; Chambers, D.; Sutton, A.; Goyder, E.; Booth, A. The effects of integrated care: A systematic review of UK and international evidence. BMC Health Serv. Res. 2018, 18, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lappin, J.M. Comorbid substance use in psychosis: Someone else’s problem? Aust. N. Z. J. Psychiatry 2022, 56, 5–7. [Google Scholar] [CrossRef]
- Fantuzzi, C.; Mezzina, R. Dual diagnosis: A systematic review of the organization of community health services. Int. J. Soc. Psychiatry 2020, 66, 300–310. [Google Scholar] [CrossRef]
- McGinty, E.E.; Daumit, G.L. Integrating Mental Health and Addiction Treatment into General Medical Care: The Role of Policy. Psychiatr. Serv. 2020, 71, 1163–1169. [Google Scholar] [CrossRef]
- Hartzler, B. Integration of Substance Use Services in Mental Health Settings; Alcohol & Drug Abuse Institute, University of Washington: Seattle, WA, USA, 2017; Available online: http://adai.uw.edu/pubs/pdf/2017susmentalhealth.pdf (accessed on 10 November 2021).
- Addiction and Mental Health Collaborative Project Steering Committee. Collaboration for Addiction and Mental Health Care: Best Advice; Canadian Centre on Substance Abuse: Ottawa, ON, Canada, 2015; Available online: https://www.ccsa.ca/collaboration-addiction-and-mental-health-care-best-advice-report (accessed on 12 October 2022).
- Australian Health Ministers’ Advisory Council. A National Framework for Recovery-Oriented Mental Health Services: Guide for Practitioners and Providers; Department of Health and Ageing, Ed.; Commonwealth of Australia: Canberra, Australia, 2013. Available online: https://www.health.gov.au/resources/publications/a-national-framework-for-recovery-oriented-mental-health-services-guide-for-practitioners-and-providers (accessed on 12 October 2022).
- Australian Commission on Safety and Quality in Health Care. Patient-Centred Care: Improving Quality and Safety through Partnerships with Patients and Consumers; ACSQHC, Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2011. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/PCC_Paper_August.pdf (accessed on 12 October 2022).
- The Senate Select Committee on Mental Health. A National Approach to Mental Health—From Crisis to Community First Report; Commonwealth of Australia: Canberra, Australia, 2006. Available online: https://www.aph.gov.au/Parliamentary_Business/Committees/Senate/Former_Committees/mentalhealth/report02/index (accessed on 10 November 2021).
- NSW Department of Health. NSW Clinical Guidelines for the Care of Persons with Comorbid Mental Illness and Substance Use Disorders in Acute Care Settings; Department of Health: Sydney, Australia, 2009. Available online: https://www.health.nsw.gov.au/aod/resources/Publications/comorbidity-report.pdf (accessed on 14 September 2022).
- Marel, C.; Siedlecka, E.; Fisher, A.; Gournay, K.; Deady, M.; Baker, A.; Kay-Lambkin, F.; Teesson, M.; Baillie, A.; Mills, K.L. Guidelines on the Management of Co-Occurring Alcohol and Other Drug and Mental Health Conditions in Alcohol and Other Drug Treatment Settings, 3rd ed.; Matilda Centre for Research in Mental Health and Substance Use, the University of Sydney: Sydney, Australia, 2022; Available online: https://comorbidityguidelines.org.au/pdf/comorbidity-guideline.pdf (accessed on 31 January 2023).
- Skinner, W.J.; O’Grady, C.P.; Bartha, C.; Parker, C. Best Practices: Concurrent Mental Health and Substance Use Disorders; Canadian Centre for Addiction and Mental Health: Ottawa, ON, Canada, 2012; Available online: https://www.camh.ca/-/media/files/guides-and-publications/concurrent-disorders-guide-en.pdf (accessed on 14 September 2022).
- Kleber, H.; Weiss, R.; Anton, R.; George, T.; Greenfield, S.; Kosten, T.; O’Brien, C.; Rounsaville, B.; Strain, E.; Ziedonis, D.; et al. Practice guideline for the treatment of patients with substance use disorders. Am. J. Psychiatry 2007, 164, 5–123. [Google Scholar] [CrossRef]
- Public Health England. Better Care for People with Co-Occurring Mental Health and Alcohol/Drug Use Conditions. A Guide for Commissioners and Service Providers; PHE Publication Gateway Number: 2017119; Public Health England: London, UK, 2017. Available online: https://www.gov.uk/government/publications/people-with-co-occurring-conditions-commission-and-provide-services (accessed on 14 September 2022).
- Deady, M.; Barrett, E.; Mills, K.; Kay-Lambkin, F.; Haber, P.; Shand, F.; Baker, A.; Baillie, A.; Christensen, H.; Manns, L.; et al. Effective Models of Care for Comorbid Mental Illness and Illicit Substance Use: Evidence Check Review; NSW Ministry of Health: Sydney, Australia, 2015. Available online: https://www.health.nsw.gov.au/mentalhealth/resources/Publications/comorbid-mental-care-review.pdf (accessed on 14 September 2022).
- Alsuhaibani, R.; Smith, D.C.; Lowrie, R.; Aljhani, S.; Paudyal, V. Scope, quality and inclusivity of international clinical guidelines on mental health and substance abuse in relation to dual diagnosis, social and community outcomes: A systematic review. BMC Psychiatry 2021, 21, 209. [Google Scholar] [CrossRef]
- Hunt, G.E.; Siegfried, N.; Morley, K.; Brooke-Sumner, C.; Cleary, M. Psychosocial interventions for people with both severe mental illness and substance misuse. CDSR 2019, I12, CD001088. [Google Scholar] [CrossRef] [Green Version]
- Hesse, M. Integrated psychological treatment for substance use and co-morbid anxiety or depression vs. treatment for substance use alone. A systematic review of the published literature. BMC Psychiatry 2009, 20, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, M.N.; Levin, C.J.; Levin, F.R. Treatment for substance use disorder with co-occurring mental illness. Focus 2019, 17, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Collings, S.; Allan, J.; Munro, A. Improving treatment for people with cognitive impairment and substance misuse issues: Lessons from an inclusive residential treatment program pilot in Australia. Disabil. Health J. 2022, 15, 101295. [Google Scholar] [CrossRef]
- Hobbs, J.D.; Kushner, M.G.; Lee, S.S.; Reardon, S.M.; Maurer, E.W. Meta-analysis of supplemental treatment for depressive and anxiety disorders in patients being treated for alcohol dependence. Am. J. Addict. 2011, 20, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, G.; Robertson, J.; Pallis, S.; Segal, J. The dual diagnosis clinician shared care model—A clinical mental health dual diagnosis integrated treatment initiative. Adv. Dual. Diagn. 2022, 15, 165–176. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration (SAMHSA). Integrated Treatment for Co-Occurring Disorders Evidence-Based Practices (EBP) KIT. 2010. Available online: https://store.samhsa.gov/product/Integrated-Treatment-for-Co-Occurring-Disorders-Evidence-Based-Practices-EBP-KIT/SMA08-4367 (accessed on 14 September 2022).
- Hussain, S.T.; Lei, S.; Akram, T.; Haider, M.J.; Hussain, S.H.; Ali, M. Kurt Lewin’s change model: A critical review of the role of leadership and employee involvement in organizational change. J. Innov. Knowl. 2022, 3, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Appelbaum, S.H.; Habashy, S.; Malo, J.-L.; Shafiq, H. Back to the future: Revisiting Kotter’s 1996 change model. J. Manag. Dev. 2012, 31, 764–782. [Google Scholar] [CrossRef]
- Rosenbaum, D.; More, E.; Steane, P. Planned organisational change management: Forward to the past? An exploratory literature review. J. Org. Chang. Manag. 2018, 31, 286–303. [Google Scholar] [CrossRef]
- Langley, G.L.; Moen, R.; Nolan, K.M.; Nolan, T.W.; Norman, C.L.; Provost, L.P. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance, 2nd ed.; Jossey-Bass Publishers: San Francisco, CA, USA, 2009. [Google Scholar]
- Foley, C.; Allan, J.; Lappin, J.; Courtney, R.; Baker, S.; Hickman, C.; Gibbons, R.; Duncanson, K.; Farnbach, S.; Henderson, A.; et al. “The driving force here is that it’s better for our clients”. From independent to integrated care in rural Australian mental health and addiction services: A mixed methods study of a clinician-led process of change. J. Subst. Abuse Treat. 2023. submitted. [Google Scholar]
- Schmidt, D. What a great idea! Someone should evaluate that. Aust. Health Rev. 2016, 40, 270–272. [Google Scholar] [CrossRef]
- Sackett, D.L.; Rosenberg, W.M.; Muir-Gray, J.A.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Substance Abuse and Mental Health Services Administration (SAMHSA). Adapting Evidence-Based Practices for Under-Resourced Populations; SAMHSA Publication No. PEP22-06-02-004; National Mental Health and Substance Use Policy Laboratory, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2022. Available online: https://store.samhsa.gov/sites/default/files/SAMHSA_Digital_Download/PEP22-06-02-004.pdf (accessed on 31 January 2023).
- de Groot, M.; van der Wouden, J.M.; van Hell, E.A.; Nieweg, M.B. Evidence-based practice for individuals or groups: Let’s make a difference. Perspect. Med. Educ. 2013, 2, 216–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murata, R.M.; Moss, M.E.; Wright, W.; Pardi, V. Knowledge to action: Integrating evidence-based practice into online PBL cases during COVID-19. J. Dent. Educ. 2021, 85 (Suppl. S3), 1938–1939. [Google Scholar] [CrossRef] [PubMed]
- Farnbach, S.; Allan, J.; Wallace, R.; Aiken, A.; Shakeshaft, A. Formative process evaluation of a guideline-driven process for improving the cultural responsiveness of alcohol and drug treatment services. BMC Health Serv. Res. 2021, 21, 352. [Google Scholar] [CrossRef]
- Snijder, M.; Wagemakers, A.; Calabria, B.; Byrne, B.; O’Neill, J.; Babblett, R.; Munro, A.; Shakeshaft, A. ‘We walked side by side through the whole thing’: A mixed-methods study of key elements of community-based participatory research partnerships between rural Aboriginal communities and researchers. AJRH 2020, 28, 338–350. [Google Scholar] [CrossRef]
- Shakeshaft, A.; Can We Improve Processes for Engaging Communities and Services in Research. Drug and Alcohol Research Connections. 2018. Available online: http://www.connections.edu.au/opinion/can-we-improve-processes-engaging-communities-and-services-research (accessed on 31 January 2023).
- Knight, A.; Maple, M.; Shakeshaft, A.; Shakeshaft, B.; Pearce, T. Improving the evidence base for services working with youth at-risk of involvement in the criminal justice system: Developing a standardised program approach. Health Justice 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Munro, A.; Shakeshaft, A.; Clifford, A. The development of a healing model of care for an Indigenous drug and alcohol residential rehabilitation service: A community-based participatory research approach. Health Justice 2017, 5, 12. [Google Scholar] [CrossRef]
- Foley, C. Development of a Standardised but Flexible Process for the Sustained Uptake of Integrated Care in Mental Health and Drug and Alcohol Services. Ph.D. Thesis, University of NSW, Sydney, Australia, 15 May 2019. [Google Scholar]
- Bhandari, P. Triangulation in Research|Guide, Types, Examples. Available online: https://www.scribbr.co.uk/research-methods/triangulation-in-research/ (accessed on 31 January 2023).
- Foley, C.; Lappin, J.; Allan, J.; Courtney, R.; Young, C.; Farnbach, S.; Henderson, A.; Shakeshaft, A. How do you make it work in practice? Co-designing a pragmatic model of integrated care for psychiatric and addiction services. Adv. Dual. Diagn. 2023. submitted. [Google Scholar]


{kind=link}
| Step | Description | Activity Undertaken |
|---|---|---|
| 1 | ASK a searchable question | Identified by clinicians and brought to researchers. Development of a PAR study. Question: How do you make IC work in practice across diverse clinical settings? |
| 2 | ACQUIRE information | Reviewed the literature [45] and conducted the PAR study [34] |
| 3 | APPRAISE the search results |
|
| 4 | APPLY the evidence in practice.
|
|
| 5 | ASSESS the provided care | Results of testing will be published separately. |
| Core Components | Change Enablers | Flexible Activities (Examples) |
|---|---|---|
| 1. Secure commitment and active participation. Identify relevant stakeholders at all levels of the organisation and form an alliance, starting with service managers and clinical leads. | The innovation is actively driven by frontline managers, and workers (bottom-up leadership) alongside executive sponsors and managers (top-down permission and participation). |
|
| 2. Describe the current state. Understand existing processes, strengths, and gaps. Establish a baseline. | The innovation is monitored for acceptability and effectiveness from commencement and ongoing, by the people delivering and/or receiving clinical care. |
|
| 3. Formalise collaboration, build relationships. Establish collaboration processes and a shared vision. | There is sufficient time for genuine professional relationships to develop, and a shared goal to emerge rather than be imposed. |
|
| 4. Co-design the innovation. E.g., design a new model of IC or tailor an existing model to the needs of your service. | Buy-in and ownership are optimised through equitable & meaningful contribution to development of clinical procedures, and opportunities to devise own activities. |
|
| 5. Develop training and clinical support. Co-design training and processes to support clinicians to deliver new procedures. | Training and clinical supports are relevant and productive and are delivered in a flexible and feasible way. |
|
| 6. Monitor and sustain the innovation. Embed measures and continue to build staff confidence via clinical supervision and supports. | The innovation is embedded in routine practice and clinicians have confidence to deliver the new procedures. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foley, C.; Allan, J.; Lappin, J.; Courtney, R.; Farnbach, S.; Henderson, A.; Shakeshaft, A. Utilising the Implementation of Integrated Care to Develop a Pragmatic Framework for the Sustained Uptake of Service Innovations (SUSI). Healthcare 2023, 11, 1786. https://doi.org/10.3390/healthcare11121786
Foley C, Allan J, Lappin J, Courtney R, Farnbach S, Henderson A, Shakeshaft A. Utilising the Implementation of Integrated Care to Develop a Pragmatic Framework for the Sustained Uptake of Service Innovations (SUSI). Healthcare. 2023; 11(12):1786. https://doi.org/10.3390/healthcare11121786
Chicago/Turabian StyleFoley, Catherine, Julaine Allan, Julia Lappin, Ryan Courtney, Sara Farnbach, Alexandra Henderson, and Anthony Shakeshaft. 2023. "Utilising the Implementation of Integrated Care to Develop a Pragmatic Framework for the Sustained Uptake of Service Innovations (SUSI)" Healthcare 11, no. 12: 1786. https://doi.org/10.3390/healthcare11121786