

Preperitoneal Pelvic Packing versus Angioembolization for Patients with Hemodynamically Unstable Pelvic Fractures with Pelvic Bleeding: A Single-Centered Retrospective Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Data Collection
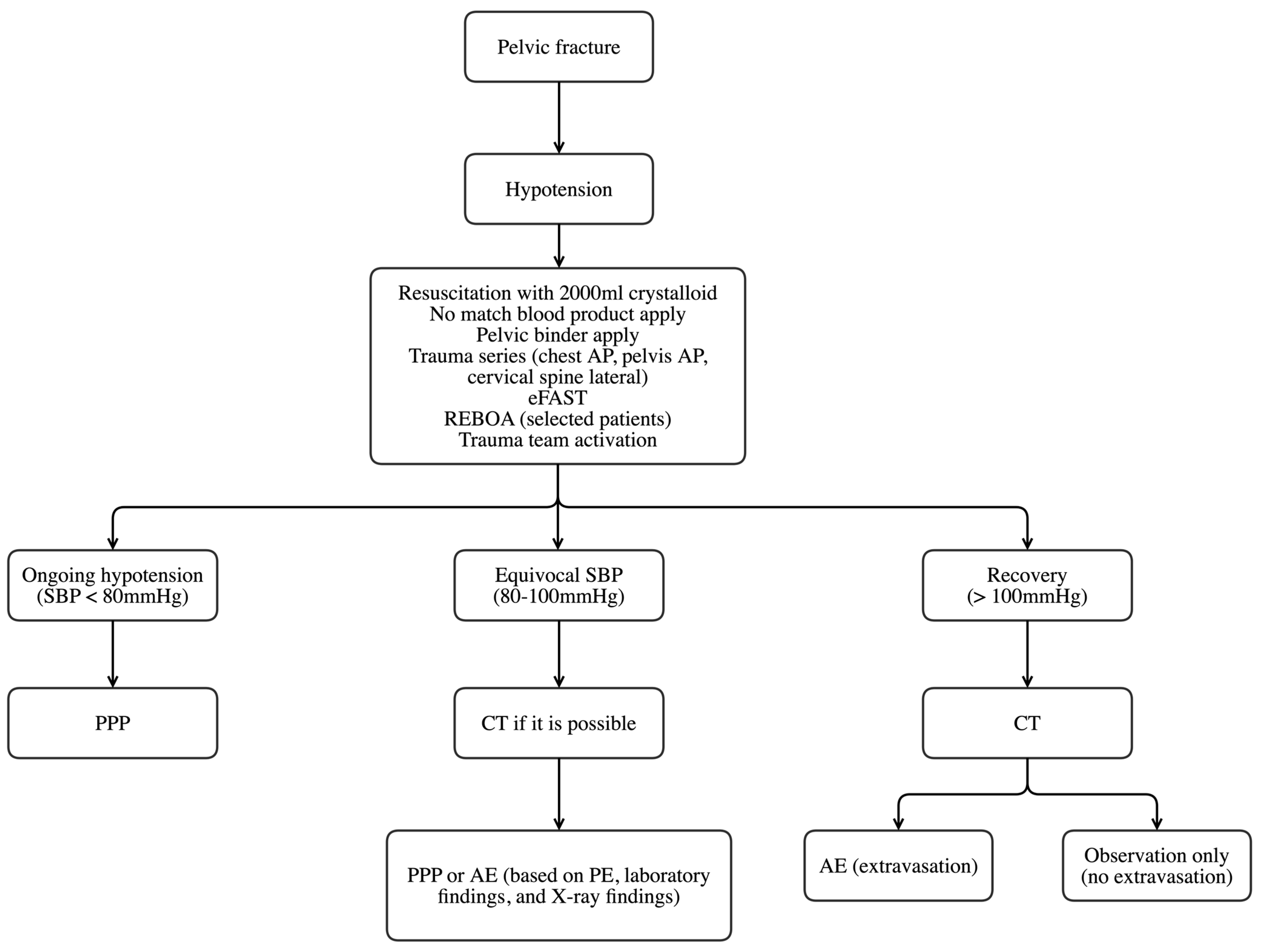
2.2. Patient Management
2.3. PPP Technique
2.4. AE
2.5. Study Setting
2.6. Statistical Analysis
3. Results
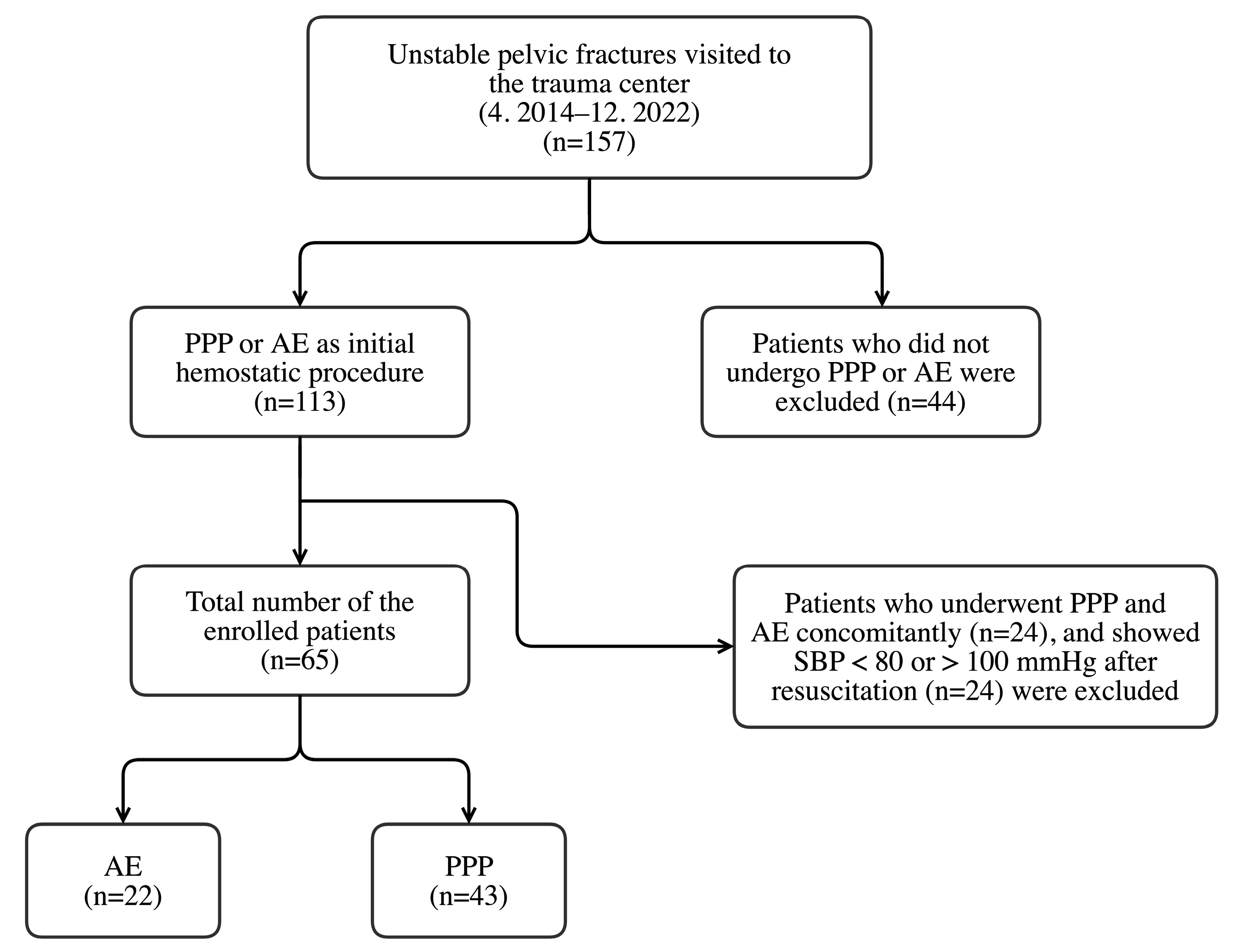
3.1. Patient Enrollment
3.2. Differences in Characteristics of the Enrolled Patients between the Two Groups
3.3. Comparison of Time Factors and Patient Outcomes
3.4. Details of Patients Who Underwent AE after REBOA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Costantini, T.W.; Coimbra, R.; Holcomb, J.B.; Podbielski, J.M.; Catalano, R.; Blackburn, A.; Scalea, T.M.; Stein, D.M.; Williams, L.; Conflitti, J.; et al. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. J. Trauma Acute Care Surg. 2016, 80, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Flint, L.; Cryer, H.G. Pelvic fracture: The last 50 years. J. Trauma 2010, 69, 483–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biffl, W.L.; Smith, W.R.; Moore, E.E.; Gonzalez, R.J.; Morgan, S.J.; Hennessey, T.; Offner, P.J.; Ray, C.E., Jr.; Franciose, R.J.; Burch, J.M. Evolution of a multidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. Ann. Surg. 2001, 233, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.M.; O’Toole, R.; Scalea, T.M. Multidisciplinary approach for patients with pelvic fractures and hemodynamic instability. Scand. J. Surg. 2007, 96, 272–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, T.L.; Brasel, K.J.; Karmy-Jones, R.; Rowell, S.; Schreiber, M.A.; Shatz, D.V.; Albrecht, R.M.; Cohen, M.J.; DeMoya, M.A.; Biffl, W.L.; et al. Western Trauma Association Critical Decisions in Trauma: Management of pelvic fracture with hemodynamic instability-2016 updates. J. Trauma Acute Care Surg. 2016, 81, 1171–1174. [Google Scholar] [CrossRef] [PubMed]
- Cullinane, D.C.; Schiller, H.J.; Zielinski, M.D.; Bilaniuk, J.W.; Collier, B.R.; Como, J.; Holevar, M.; Sabater, E.A.; Sems, S.A.; Vassy, W.M.; et al. Eastern Association for the Surgery of Trauma practice management guidelines for hemorrhage in pelvic fracture--update and systematic review. J. Trauma 2011, 71, 1850–1868. [Google Scholar] [CrossRef] [Green Version]
- Pohlemann, T.; Gänsslen, A.; Bosch, U.; Tscherne, H. The technique of packing for control of hemorrhage in complex pelvis fractures. Tech. Orthop. 1995, 9, 267–270. [Google Scholar] [CrossRef]
- Papakostidis, C.; Giannoudis, P.V. Pelvic ring injuries with haemodynamic instability: Efficacy of pelvic packing, a systematic review. Injury 2009, 40 (Suppl. S4), S53–S61. [Google Scholar] [CrossRef]
- Marzi, I.; Lustenberger, T. Management of bleeding pelvic fractures. Scand. J. Surg. 2014, 103, 104–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, T.; Smith, W.R.; Moore, E.E. Pelvic packing or angiography: Competitive or complementary? Injury 2009, 40, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.M.; Yadev, S.; Faraj, S. Controlling hemorrhage in exsanguinating pelvic fractures: Utility of extraperitoneal pelvic packing as a damage control procedure. Int. J. Crit. Illn. Inj. Sci. 2016, 6, 148–152. [Google Scholar] [CrossRef] [Green Version]
- Tai, D.K.; Li, W.H.; Lee, K.Y.; Cheng, M.; Lee, K.B.; Tang, L.F.; Lai, A.K.; Ho, H.F.; Cheung, M.T. Retroperitoneal pelvic packing in the management of hemodynamically unstable pelvic fractures: A level I trauma center experience. J. Trauma 2011, 71, E79–E86. [Google Scholar] [CrossRef]
- Hundersmarck, D.; Hietbrink, F.; Leenen, L.P.H.; Heng, M. Pelvic packing and angio-embolization after blunt pelvic trauma: A retrospective 18-year analysis. Injury 2021, 52, 946–955. [Google Scholar] [CrossRef]
- Chiara, O.; di Fratta, E.; Mariani, A.; Michaela, B.; Prestini, L.; Sammartano, F.; Cimbanassi, S. Efficacy of extra-peritoneal pelvic packing in hemodynamically unstable pelvic fractures, a Propensity Score Analysis. World J. Emerg. Surg. 2016, 11, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Dong, J.; Yang, Y.; Wang, G.; Wang, Y.; Liu, P.; Robinson, Y.; Zhou, D. Retroperitoneal packing or angioembolization for haemorrhage control of pelvic fractures--Quasi-randomized clinical trial of 56 haemodynamically unstable patients with Injury Severity Score >/=33. Injury 2016, 47, 395–401. [Google Scholar] [CrossRef]
- Osborn, P.M.; Smith, W.R.; Moore, E.E.; Cothren, C.C.; Morgan, S.J.; Williams, A.E.; Stahel, P.F. Direct retroperitoneal pelvic packing versus pelvic angiography: A comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury 2009, 40, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Zhang, Y.; Yang, Z.; Wang, J.; Jin, A.; Wang, W.; Chen, R.; Zhan, S. Incidence, temporal trend and factors associated with ventilator-associated pneumonia in mainland China: A systematic review and meta-analysis. BMC Infect. Dis. 2017, 17, 468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blot, S.; Koulenti, D.; Dimopoulos, G.; Martin, C.; Komnos, A.; Krueger, W.A.; Spina, G.; Armaganidis, A.; Rello, J.; Eu-Vap Study Investigators. Prevalence, risk factors, and mortality for ventilator-associated pneumonia in middle-aged, old, and very old critically ill patients. Crit. Care Med. 2014, 42, 601–609. [Google Scholar] [CrossRef]
- Othman, A.A.; Abdelazim, M.S. Ventilator-associated pneumonia in adult intensive care unit prevalence and complications. Egypt J. Crit. Care Med. 2017, 5, 61–63. [Google Scholar] [CrossRef]
- Petrone, P.; Rodriguez-Perdomo, M.; Perez-Jimenez, A.; Ali, F.; Brathwaite, C.E.M.; Joseph, D.K. Pre-peritoneal pelvic packing for the management of life-threatening pelvic fractures. Eur. J. Trauma Emerg. Surg. 2019, 45, 417–421. [Google Scholar] [CrossRef]
- Kato, H.; Otomo, Y.; Homma, M.; Inoue, J.; Hasegawa, E.; Henmi, H.; Kusaba, A. Gluteal soft tissue necrosis after transcatheter angiographic embolization for pelvic fracture: A report of two cases. Eur. J. Trauma Emerg. Surg. 2007, 33, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Zeeshan, M.; Sakran, J.V.; Hamidi, M.; Kulvatunyou, N.; Khan, M.; O’Keeffe, T.; Rhee, P. Nationwide analysis of resuscitative endovascular balloon occlusion of the aorta in civilian trauma. JAMA Surg. 2019, 154, 500–508. [Google Scholar] [CrossRef] [Green Version]
- Mikdad, S.; van Erp, I.A.M.; Moheb, M.E.; Fawley, J.; Saillant, N.; King, D.R.; Kaafarani, H.M.A.; Velmahos, G.; Mendoza, A.E. Pre-peritoneal pelvic packing for early hemorrhage control reduces mortality compared to resuscitative endovascular balloon occlusion of the aorta in severe blunt pelvic trauma patients: A nationwide analysis. Injury 2020, 51, 1834–1839. [Google Scholar] [CrossRef] [PubMed]
- Pieper, A.; Thony, F.; Brun, J.; Rodiere, M.; Boussat, B.; Arvieux, C.; Tonetti, J.; Payen, J.F.; Bouzat, P. Resuscitative endovascular balloon occlusion of the aorta for pelvic blunt trauma and life-threatening hemorrhage: A 20-year experience in a Level I trauma center. J. Trauma Acute Care Surg. 2018, 84, 449–453. [Google Scholar] [CrossRef]
- Harfouche, M.; Inaba, K.; Cannon, J.; Seamon, M.; Moore, E.; Scalea, T.; DuBose, J. Patterns and outcomes of zone 3 REBOA use in the management of severe pelvic fractures: Results from the AAST Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery database. J. Trauma Acute Care Surg. 2021, 90, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Burlew, C.C.; Moore, E.E.; Smith, W.R.; Johnson, J.L.; Biffl, W.L.; Barnett, C.C.; Stahel, P.F. Preperitoneal pelvic packing/external fixation with secondary angioembolization: Optimal care for life-threatening hemorrhage from unstable pelvic fractures. J. Am. Coll. Surg. 2011, 212, 628–635. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AE (n = 22) (%) | PPP (n = 43) (%) | p-Value | |
|---|---|---|---|
| Age | 58.3 ± 18.2 | 59.6 ± 18.3 | 0.782 |
| Sex (male) | 13 (59.1) | 27 (62.8) | 0.983 |
| Initial SBP | 78.8 ± 30.3 | 75.3 ± 32.6 | 0.668 |
| Worst SBP in ED | 66.3 ± 22.2 | 63.8 ± 20.9 | 0.663 |
| SBP after fluid resuscitation | 90.8 ± 7.7 | 92.1 ± 7.0 | 0.512 |
| PR (median [IQR]) | 105.5 [91.2, 121.5] | 110.0 [97.5, 126.0] | 0.637 a |
| DM | 4 (18.2) | 7 (16.3) | 1.000 b |
| Anticoagulant intake | 3 (13.6) | 4 (10.3) | 0.695 b |
| Mechanism | 0.252 b | ||
| Traffic accident | 12 (54.5) | 14 (32.6) | |
| Pedestrian accident | 4 (18.2) | 14 (32.6) | |
| Fall | 6 (27.3) | 12 (27.9) | |
| Other blunt trauma | 0 (0.0) | 3 (7.0) | |
| Associated injury (AIS ≥ 3) | 18 (81.8) | 36 (83.7) | 1.000 b |
| Abbreviated injury scale | |||
| Head and neck | 3 (13.6) | 10 (23.3) | 0.516 b |
| Face | 0 (0.0) | 2 (4.7) | 0.545 b |
| Chest | 12 (54.5) | 19 (44.2) | 0.597 |
| Abdomen | 8 (36.4) | 13 (30.2) | 0.826 |
| Extremity and pelvic girdle | 21 (95.5) | 43 (100.0) | 0.338 b |
| External | 0 (0) | 0 (0) | NA |
| ISS (median [IQR]) | 34.0 [27.5–38.0] | 38.0 [29.0–44.0] | 0.188 a |
| Initial hemoglobin level | 11.7 ± 2.4 | 10.7 ± 2.5 | 0.108 |
| Initial lactate level (median [IQR]) | 4.1 [2.8–6.4] | 5.0 [3.9–8.4] | 0.188 a |
| Young–Burgess classification | 0.282 b | ||
| LC1 | 1 (4.5) | 0 (0) | |
| LC2 | 8 (36.4) | 13 (30.2) | |
| LC3 | 8 (36.4) | 11 (25.6) | |
| APC1 | 1 (4.5) | 0 (0) | |
| APC2 | 1 (4.5) | 5 (11.6) | |
| APC3 | 1 (4.5) | 3 (7.0) | |
| VS | 2 (9.1) | 11 (25.6) | |
| Tile classification | 0.281 | ||
| B | 17 (77.3) | 26 (60.5) | |
| C | 5 (22.7) | 17 (39.5) | |
| Open fracture | 1 (4.5) | 3 (7.0) | 1.000 b |
| REBOA | 3 (13.6) | 2 (4.7) | 0.326 b |
| Hybrid room | 1 (4.5) | 6 (14.0) | 0.408 b |
| Explo-laparotomy | 3 (13.6) | 8 (18.6) | 0.737 b |
| EF | 1 (4.5) | 9 (20.9) | 0.145 b |
| ORIF | 10 (45.5) | 19 (44.2) | 1.000 |
| AE (n = 22) (Median [IQR]) | PPP (n = 43) (Median [IQR]) | p-Value | |
|---|---|---|---|
| Time from injury to ED (minutes) | 94.0 [65.8–137.2] | 146 [74.5–222.0] | 0.197 a |
| Time from ED to ICU (minutes) | 194.0 [146.2–269.0] | 157.0 [103.5–225.0] | 0.083 a |
| Time from ED to procedure (minutes) | 139.0 [95.0–155.2] | 63.0 [47.0–95.0] | <0.001 a |
| Time from ED to ORIF (days) | 8.4 ± 5.9 | 8.1 ± 5.0 | 0.876 |
| Duration of ED stay (minutes) | 124.0 [84.2–221.5] | 59.0 [43.5–96.0] | <0.001 a |
| ICU LOS (days) | 6.0 [2.2–12.8] | 9.0 [4.0–16.5] | 0.230 a |
| Hospital LOS (days) | 29.5 [4.8–49.8] | 26.0 [8.5–63.0] | 0.901 a |
| PRBC transfusion requirement within 24 h (units) | 8.5 [4.0–12.8] | 9.0 [4.0–12.5] | 0.818 a |
| Duration of mechanical ventilation (days) | 2.0 [0.2–8.0] | 6.0 [2.5–14.0] | 0.046 a |
| Complications | 10 (45.5%) | 20 (46.5%) | 1.000 |
| Infectious complications | 4 (18.2%) | 15 (34.9%) | 0.266 |
| Mortality | 7 (31.8%) | 16 (37.2%) | 0.876 |
| Mortality due to hemorrhage | 5 (22.7%) | 6 (14.0%) | 0.487 b |
| Age | Sex | Mechanism | SBP (Initial/Worst) (mmHg) | SBP Recovered After REBOA (mmHg) | PR (/min) | ISS | YB Classification | Time from REBOA Insertion to Removal | Time from REBOA Inflation to Deflation | Location of REBOA Ballooning | AE Details | Embolized Artery | Transfusion Amount ≤ 24 h (Packed RBC) | ICU Stay | HS | Complication | Mortality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 57 | M | TA | 80/68 | 95 | 102 | 38 | LC2 | 220 | 51 | Zone III | Unilateral selective | IIA branch | 8 | 10 | 52 | Pneumonia | No |
| 70 | M | TA | 64/54 | 88 | 88 | 25 | APC3 | 740 | 38 | Zone III | Bilateral selective | IIA branch | 9 | 15 | 23 | Atelectasis | No |
| 74 | F | Pedestrian accident | 81/73 | 100 | 88 | 22 | LC1 | 57 | 14 | Zone III | Bilateral selective | IIA branch | 2 | 3 | 10 | No | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gong, S.C.; Park, J.E.; Kang, S.; An, S.; Kim, M.J.; Kim, K.; Shin, I.S. Preperitoneal Pelvic Packing versus Angioembolization for Patients with Hemodynamically Unstable Pelvic Fractures with Pelvic Bleeding: A Single-Centered Retrospective Study. Healthcare 2023, 11, 1784. https://doi.org/10.3390/healthcare11121784
Gong SC, Park JE, Kang S, An S, Kim MJ, Kim K, Shin IS. Preperitoneal Pelvic Packing versus Angioembolization for Patients with Hemodynamically Unstable Pelvic Fractures with Pelvic Bleeding: A Single-Centered Retrospective Study. Healthcare. 2023; 11(12):1784. https://doi.org/10.3390/healthcare11121784
Chicago/Turabian StyleGong, Seong Chan, Ji Eun Park, Sooyeon Kang, Sanghyun An, Myoung Jun Kim, Kwangmin Kim, and In Sik Shin. 2023. "Preperitoneal Pelvic Packing versus Angioembolization for Patients with Hemodynamically Unstable Pelvic Fractures with Pelvic Bleeding: A Single-Centered Retrospective Study" Healthcare 11, no. 12: 1784. https://doi.org/10.3390/healthcare11121784