
Geospatial Analysis of Opioid Dispensing Patterns in California: A 2021 Real-World Study


Abstract
:1. Introduction
2. Methods
2.1. Data
2.2. Measures
2.3. Method
2.4. Statistical Analyses
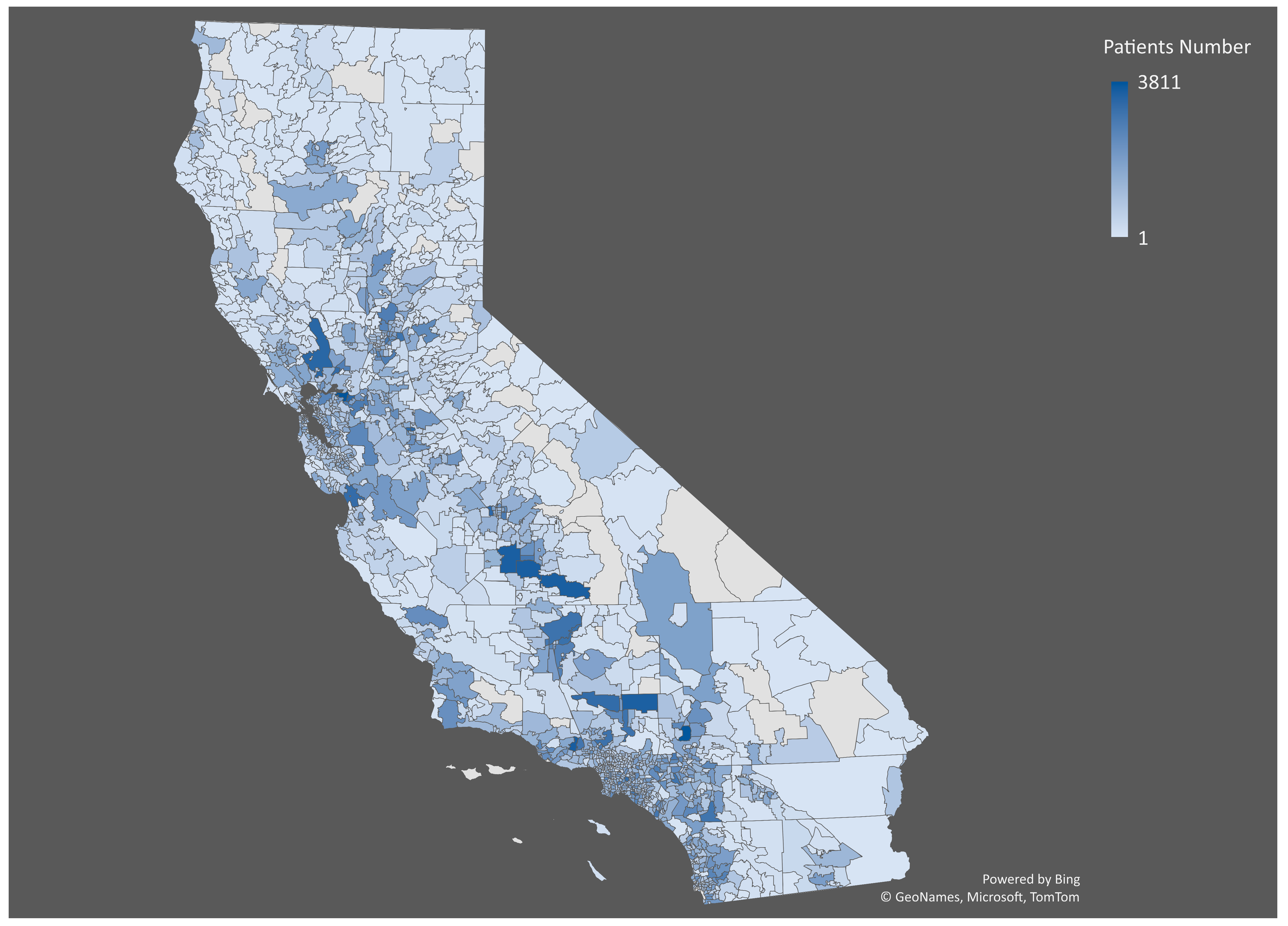
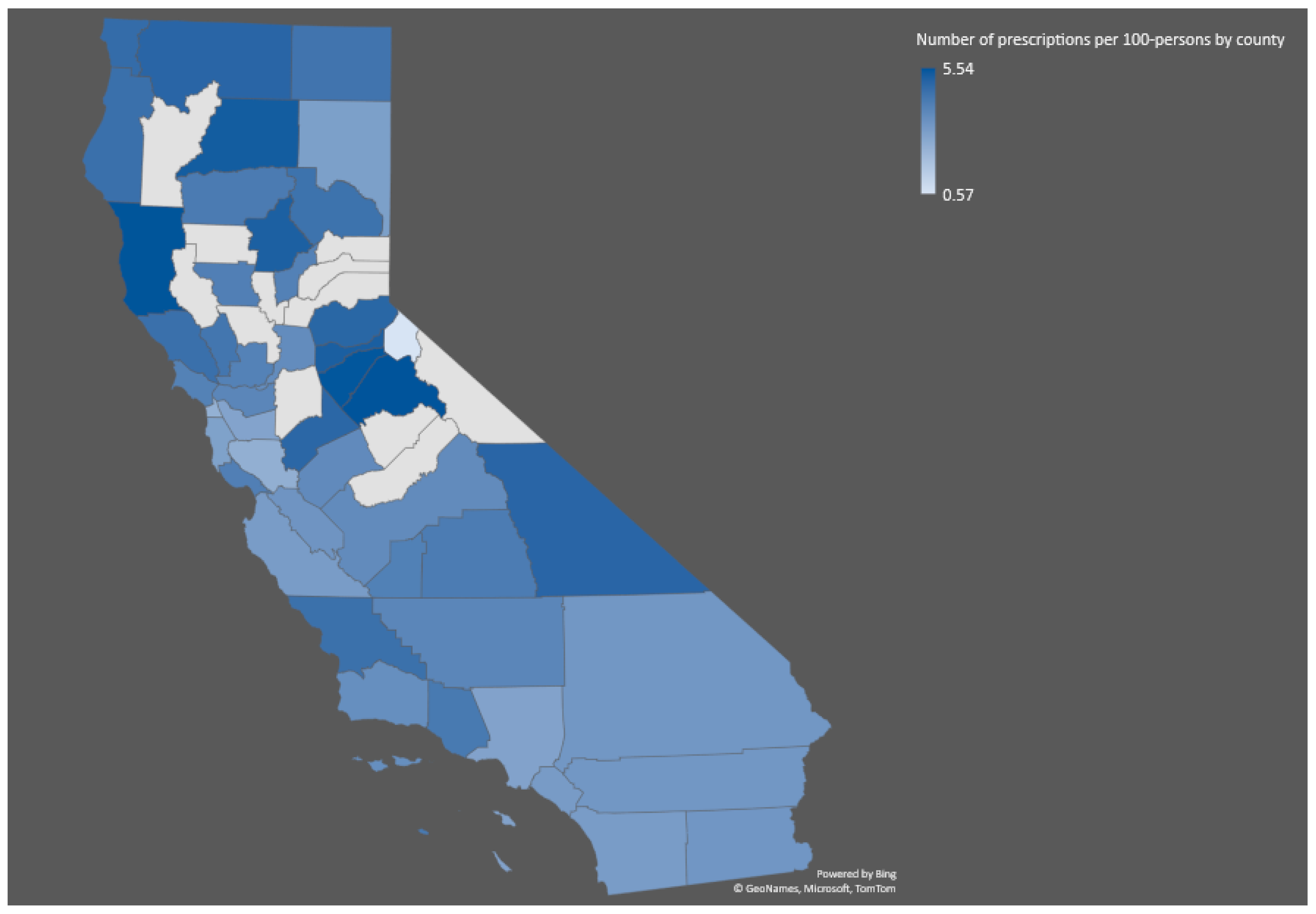
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anderson, J.A.; Demeter, N.; Wirtz, S. Using the CA Opioid Overdose Surveillance Dashboard to track opioid overdose deaths. Online J Public Health Inform. 2019, 11, e449. [Google Scholar] [CrossRef]
- Friedman, J.; Kim, D.; Schneberk, T.; Bourgois, P.; Shin, M.; Celious, A.; Schriger, D.L. Assessment of racial/ethnic and income disparities in the prescription of opioids and other controlled medications in California. JAMA Intern. Med. 2019, 179, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Rudd, R.A.; Paulozzi, L.J.; Bauer, M.J.; Burleson, R.W.; Carlson, R.E.; Dao, D.; Davis, J.W.; Dudek, J.; Eichler, B.A.; Fernandes, J.C.; et al. Increases in heroin overdose deaths—28 states, 2010 to 2012. Morb. Mortal. Wkly. Rep. 2014, 63, 849. [Google Scholar]
- Gladden, R.M.; Martinez, P.; Seth, P. Fentanyl law enforcement submissions and increases in synthetic opioid–involved overdose deaths—27 states, 2013–2014. Morb. Mortal. Wkly. Rep. 2016, 65, 837–843. [Google Scholar] [CrossRef]
- O’Donnell, J.K.; Gladden, R.M.; Seth, P. Trends in deaths involving heroin and synthetic opioids excluding methadone, and law enforcement drug product reports, by census region—United States, 2006–2015. Morb. Mortal. Wkly. Rep. 2017, 66, 897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, E.; Saunders, H. A Look at Changes in Opioid Prescribing Patterns in Medicaid from 2016 to 2019. 2023. Available online: https://www.kff.org/medicaid/issue-brief/a-look-at-changes-in-opioid-prescribing-patterns-in-medicaid-from-2016-to-2019/#:~:text=Opioid%20prescriptions%20declined%20overall%20from,an%20increase%20in%20buprenorphine%20prescriptions (accessed on 21 May 2023).
- Ghose, R.; Forati, A.M.; Mantsch, J.R. Impact of the COVID-19 pandemic on opioid overdose deaths: A spatiotemporal analysis. J. Urban Health 2022, 99, 316–327. [Google Scholar] [CrossRef]
- Chua, K.P.; Brummett, C.M.; Conti, R.M.; Bohnert, A.S. Opioid prescribing to US children and young adults in 2019. Pediatrics 2021, 148, e2021051539. [Google Scholar]
- Renny, M.H.; Yin, H.S.; Jent, V.; Hadland, S.E.; Cerdá, M. Temporal trends in opioid prescribing practices in children, adolescents, and younger adults in the US from 2006 to 2018. JAMA Pediatr. 2021, 175, 1043–1052. [Google Scholar] [CrossRef]
- Gilson, A.M.; Fishman, S.M.; Wilsey, B.L.; Casamalhuapa, C.; Baxi, H. Time series analysis of California’s prescription monitoring program: Impact on prescribing and multiple provider episodes. J. Pain 2012, 13, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Franklin, G.M.; Mai, J.; Turner, J.; Sullivan, M.; Wickizer, T.; Fulton-Kehoe, D. Bending the prescription opioid dosing and mortality curves: Impact of the Washington State opioid dosing guideline. Am. J. Ind. Med. 2012, 55, 325–331. [Google Scholar] [CrossRef]
- Kolodny, A.; Courtwright, D.T.; Hwang, C.S.; Kreiner, P.; Eadie, J.L.; Clark, T.W.; Alexander, G.C. The prescription opioid and heroin crisis: A public health approach to an epidemic of addiction. Annu. Rev. Public Health 2015, 36, 559–574. [Google Scholar] [CrossRef]
- California Department of Public Health (CDPH) CD of HCA and I. California Overdose Surveillance Dashboard. 2021. Available online: https://skylab.cdph.ca.gov/ODdash/?tab=CTY (accessed on 15 April 2023).
- US Center for Disease Control and Prevention. U.S. County Opioid Dispensing Rates, 2020. Available online: https://www.cdc.gov/drugoverdose/rxrate-maps/county2020.html (accessed on 15 April 2023).
- White, A.G.; Birnbaum, H.G.; Schiller, M.; Tang, J.; Katz, N.P. Analytic models to identify patients at risk for prescription opioid abuse. Am. J. Manag. Care 2009, 15, 897–906. [Google Scholar]
- Haffajee, R.L.; Lin, L.A.; Bohnert, A.S.B.; Goldstick, J.E. Characteristics of US counties with high opioid overdose mortality and low capacity to deliver medications for opioid use disorder. JAMA Netw. Open 2019, 2, e196373. [Google Scholar] [CrossRef] [Green Version]
- Schell, R.C.; Allen, B.; Goedel, W.C.; Hallowell, B.D.; Scagos, R.; Li, Y.; Krieger, M.S.; Neill, D.B.; Marshall, B.D.L.; Cerda, M.; et al. Identifying predictors of opioid overdose death at a neighborhood level with machine learning. Am. J. Epidemiol. 2022, 191, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Rushovich, T.; Arwady, M.A.; Salisbury-Afshar, E.; Arunkumar, P.; Aks, S.; Prachand, N. Opioid-related overdose deaths by race and neighborhood economic hardship in Chicago. J. Ethn. Subst. Abuse 2022, 21, 22–35. [Google Scholar] [CrossRef]
- Ford, J.A.; Sacra, S.A.; Yohros, A. Neighborhood characteristics and prescription drug misuse among adolescents: The importance of social disorganization and social capital. Int. J. Drug Policy 2017, 46, 47–53. [Google Scholar] [CrossRef]
- State of California Department of Justice. Controlled Substance Utilization Review and Evaluation System-California’s Prescription Drug Monitoring Program. 2022. Available online: https://oag.ca.gov/cures#:~:text=California’s%20Prescription%20Drug%20Monitoring%20Program&text=CURES%20is%20committed%20to%20the,and%20security%20laws%20and%20regulations (accessed on 15 April 2023).
- Centers for Disease Control and Prevention. Opioid National Drug Code and Oral MME Conversion File Update. 2022. Available online: https://www.cdc.gov/opioids/data-resources/index.html (accessed on 15 April 2023).
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. JAMA 2016, 315, 1624–1645. [Google Scholar] [CrossRef] [Green Version]
- Rutkow, L.; Chang, H.Y.; Daubresse, M.; Webster, D.W.; Stuart, E.A.; Alexander, G.C. Effect of Florida’s prescription drug monitoring program and pill mill laws on opioid prescribing and use. JAMA Intern. Med. 2015, 175, 1642–1649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piper, B.J.; Shah, D.T.; Simoyan, O.M.; McCall, K.L.; Nichols, S.D. Trends in medical use of opioids in the US, 2006–2016. Am. J. Prev. Med. 2018, 54, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Moyo, P.; Simoni-Wastila, L.; Griffin, B.A.; Onukwugha, E.; Harrington, D.; Alexander, G.C.; Palumbo, F. Impact of prescription drug monitoring programs (PDMPs) on opioid utilization among Medicare beneficiaries in 10 US States. Addiction 2017, 112, 1784–1796. [Google Scholar] [CrossRef] [PubMed]
- Seal, K.H.; Shi, Y.; Cohen, G.; Cohen, B.E.; Maguen, S.; Krebs, E.E.; Neylan, T.C. Association of mental health disorders with prescription opioids and high-risk opioid use in US veterans of Iraq and Afghanistan. JAMA 2012, 307, 940–947. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Johnson, P.; Jeng, P.J.; Reid, M.C.; Witkin, L.R.; Schackman, B.R.; Ancker, J.S.; Bao, Y. First opioid prescription and subsequent high-risk opioid use: A national study of privately insured and Medicare Advantage adults. J. Gen. Intern. Med. 2018, 33, 2156–2162. [Google Scholar] [CrossRef] [Green Version]
- Bao, Y.; Wen, K.; Johnson, P.; Jeng, P.J.; Meisel, Z.F.; Schackman, B.R. Assessing the impact of state policies for prescription drug monitoring programs on high-risk opioid prescriptions. Health Aff. 2018, 37, 1596–1604. [Google Scholar] [CrossRef] [PubMed]
- Sun, E.C.; Dixit, A.; Humphreys, K.; Darnall, B.D.; Baker, L.C.; Mackey, S. Association between concurrent use of prescription opioids and benzodiazepines and overdose: Retrospective analysis. BMJ 2017, 356, j760. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, E.J.; Malte, C.A.; Grossbard, J.R.; Saxon, A.J. Prevalence and trends of concurrent opioid analgesic and benzodiazepine use among veterans affairs patients with post-traumatic stress disorder, 2003–2011. Pain Med. 2015, 16, 1943–1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meara, E.; Horwitz, J.R.; Powell, W.; McClelland, L.; Zhou, W.; O’malley, A.J.; Morden, N.E. State legal restrictions and prescription-opioid use among disabled adults. N. Engl. J. Med. 2016, 375, 44–53. [Google Scholar] [CrossRef]
- Baumblatt, J.A.G.; Wiedeman, C.; Dunn, J.R.; Schaffner, W.; Paulozzi, L.J.; Jones, T.F. High-risk use by patients prescribed opioids for pain and its role in overdose deaths. JAMA Intern. Med. 2014, 174, 796–801. [Google Scholar] [CrossRef] [Green Version]
- Sansone, R.A.; Sansone, L.A. Doctor shopping: A phenomenon of many themes. Innov. Clin. Neurosci. 2012, 9, 42. [Google Scholar]
- Ball, S.J.; Simpson, K.; Zhang, J.; Marsden, J.; Heidari, K.; Moran, W.P.; Mauldin, P.D.; McCauley, J.L. High-Risk Opioid Prescribing Trends: Prescription Drug Monitoring Program Data from 2010–2018. J. Public Health Manag. Pract. 2021, 27, 379. [Google Scholar] [CrossRef] [PubMed]
- Schepis, T.S.; McCabe, S.E.; Teter, C.J. Sources of opioid medication for misuse in older adults: Results from a nationally representative survey. Pain 2018, 159, 1543. [Google Scholar] [CrossRef]
- Lister, J.J.; Ellis, J.D.; Yoon, M. Opioid prescribing and opioid-overdose deaths in Michigan: Urban-rural comparisons and changes across 2013–2017. Addict. Behav. Rep. 2020, 11, 100234. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics and Dispensing Outcomes (Year 2021) | |
| Number of opioid recipients | 1,300,171 |
| Number of dispensing recorders | 7,776,640 |
| Number of prescribers | 98,408 |
| Male | 548,446 (42.18%) |
| Male Age (median, mean, std) | 64, 62.40, 14.12 |
| Female | 751,725 (57.82%) |
| Female Age (median, mean, std) | 64, 63.29, 15.06 |
| The number of recipients who were exposed to opioid drugs over 180 days (n, %) | 208,454 (8.87%) |
| The Number of Recipients Who Have a High-Risk Dispensing Indicator | |
| (1) Multiple provider episodes (n, %) | 93,462 (7.2%) |
| (2) Overlapping opioid prescription for ≥7 days (n, %) | 290,351 (22.33%) |
| (3) Overlapping opioid and benzodiazepine for ≥7 days (n, %) | 104,357 (8%) |
| (4) High standardized dosage of opioid prescriptions (n, %) | 20,236 (1.56%) |
| Variable | Multiple Provider Episodes (95% CI) | Overlapping Opioid Prescription for ≥7 Days (95% CI) | Overlapping Opioid and Benzodiazepine for ≥7 Days (95% CI) | High Standardized Dosage of Opioid Prescriptions (95% CI) |
|---|---|---|---|---|
| Median Age | −5.5622 (−8.544, −2.5803) | −6.72 (−8.7449, −4.6951) | −7.7471 (−10.8811, −4.613) | −1.7757 (−2.6644, −0.887) |
| % Charitable Givers | 3.0683 (0.6167, 5.5200) | 4.0389 (2.3577, 5.72) | 10.7542 (8.3241, 13.1843) | Not Significant |
| Median Commute Time | Not Significant | Not Significant | −2.229 (−4.2921, −0.1659) | −0.422 (−0.9977, 0.1536) |
| Density | −0.0273 (−0.0348, −0.0198) | −0.0132 (−0.0182, −0.0082) | −0.0191 (−0.0267, −0.0115) | Not Significant |
| % Disabled | Not Significant | 2.0875 (−0.7391, 4.914) | 5.2299 (0.7059, 9.7539) | 1.2025 (−0.0422, 2.4472) |
| % Divorced | Not Significant | Not Significant | Not Significant | Not Significant |
| % Education Bachelors | Not Significant | −6.076 (−7.9764, −4.1755) | −9.884 (−12.8724, −6.8957) | −2.682 (−3.5967, −1.7672) |
| % Education College or Above | Not Significant | Not Significant | Not Significant | Not Significant |
| % Education Graduate | 3.2643 (−0.3551, 6.8837) | −4.2127 (−5.9054, −2.52) | −8.2961 (−10.864, −5.7282) | −1.9957 (−2.813, −1.1785) |
| % Education Highschool | 10.713 (7.6595, 13.7665) | Not Significant | Not Significant | −0.9965 (−1.8982, −0.0947) |
| % Education Less Highschool | 12.0349 (8.8476, 15.2221) | −1.4927 (−3.1816, 0.1962) | −3.906 (−6.3666, −1.4454) | Not Significant |
| % Education Some College | 10.7529 (7.5149, 13.9909) | Not Significant | Not Significant | Not Significant |
| % Family Dual Income | Not Significant | Not Significant | Not Significant | Not Significant |
| Average Family Size | Not Significant | Not Significant | Not Significant | Not Significant |
| % Farmer | −11.2116 (−18.1447, −4.2785) | −8.2954 (−12.9195, −3.6713) | −12.6309 (−19.9376, −5.3241) | −2.73 (−4.8246, −0.6355) |
| % Health Uninsured | −9.3876 (−13.6014, −5.1737) | −4.3291 (−7.1293, −1.5289) | −5.7225 (−10.238, −1.2069) | −2.3292 (−3.6186, −1.0398) |
| % Hispanic | −2.8474 (−4.1803, −1.5144) | −0.8857 (−1.7411, −0.0304) | Not Significant | −0.6315 (−0.974, −0.289) |
| % Home Ownership | 1.3882 (−0.054, 2.8304) | 0.6639 (−0.2548, 1.5827) | Not Significant | 0.468 (0.0996, 0.8364) |
| Median Home Value | −0.0001 (−0.0001, 0.0000) | 0.0000 (−0.0001, 0.0000) | Not Significant | Not Significant |
| Housing Units | 0.0574 (0.0553, 0.0594) | 0.0356 (0.0305, 0.0407) | 0.0647 (0.057, 0.0723) | 0.0145 (0.0121, 0.0168) |
| % Income Household $150 K Over | 3.7928 (0.4511, 7.1344) | 2.0254 (0.2468, 3.804) | Not Significant | 1.7441 (1.0319, 2.4563) |
| Median Household Income | 0.0016 (0.0001, 0.0031) | Not Significant | Not Significant | Not Significant |
| % Household Income Under $5 K | Not Significant | Not Significant | Not Significant | Not Significant |
| Median Individual Income | −0.0018 (−0.0039, 0.0003) | −0.0011 (−0.0024, 0.0001) | −0.0029 (−0.0047, −0.0011) | −0.0004 (−0.001, 0.0001) |
| % Labor Force Participation | Not Significant | −1.2225 (−2.7464, 0.3013) | −2.6415 (−5.0544, −0.2287) | Not Significant |
| % Limited English | Not Significant | Not Significant | Not Significant | −0.592 (−1.2068, 0.0228) |
| % Male | −7.593 (−11.4132, −3.7728) | Not Significant | −3.1298 (−7.2258, 0.9661) | Not Significant |
| % Married | −8.7214 (−12.2559, −5.187) | −4.7524 (−7.1951, −2.3097) | −5.3964 (−9.2797, −1.5131) | −1.3759 (−2.4982, −0.2535) |
| % Never Married | −8.1634 (−12.1485, −4.1783) | −5.7531 (−8.3803, −3.1259) | −6.6714 (−11.0447, −2.298) | −1.6997 (−2.8934, −0.5059) |
| Population | Not Significant | −0.0015 (−0.0031, 0.0002) | −0.0061 (−0.0085, −0.0037) | −0.0015 (−0.0022, −0.0007) |
| % Race Asian | −5.5453 (−6.6683, −4.4223) | −1.8246 (−2.9029, −0.7463) | −4.3852 (−5.5416, −3.2288) | −1.2717 (−1.6369, −0.9066) |
| % Race Black | Not Significant | Not Significant | −5.3587 (−7.3606, −3.3569) | Not Significant |
| % Race Native | −4.2608 (−8.084, −0.4376) | Not Significant | −4.8884 (−8.8992, −0.8776) | −0.994 (−2.1427, 0.1546) |
| % Race Other | −1.5957 (−3.2122, 0.0209) | Not Significant | −2.9232 (−4.4787, −1.3676) | Not Significant |
| % Race Pacific | 54.9469 (31.8808, 78.013) | 15.6273 (0.086, 31.1686) | Not Significant | 7.1838 (0.1787, 14.1889) |
| % Race White | Not Significant | 1.4252 (0.6343, 2.2162) | Not Significant | Not Significant |
| Median Rent Burden | Not Significant | −0.8263 (−1.8684, 0.2158) | −2.4403 (−4.1252, −0.7553) | Not Significant |
| Median Rent | Not Significant | Not Significant | Not Significant | Not Significant |
| % Self Employed | Not Significant | Not Significant | 4.5369 (1.1474, 7.9264) | 0.8391 (−0.1078, 1.786) |
| Unemployment Rate | −3.8167 (−7.5801, −0.0533) | Not Significant | Not Significant | Not Significant |
| % Veteran | Not Significant | Not Significant | −11.4975 (−17.6392, −5.3558) | Not Significant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, H.; Zheng, J.; Wang, Y. Geospatial Analysis of Opioid Dispensing Patterns in California: A 2021 Real-World Study. Healthcare 2023, 11, 1732. https://doi.org/10.3390/healthcare11121732
Lu H, Zheng J, Wang Y. Geospatial Analysis of Opioid Dispensing Patterns in California: A 2021 Real-World Study. Healthcare. 2023; 11(12):1732. https://doi.org/10.3390/healthcare11121732
Chicago/Turabian StyleLu, Hongxia, Jianwei Zheng, and Yun Wang. 2023. "Geospatial Analysis of Opioid Dispensing Patterns in California: A 2021 Real-World Study" Healthcare 11, no. 12: 1732. https://doi.org/10.3390/healthcare11121732