
Effects of Combined Training Programs in Individuals with Fibromyalgia: A Systematic Review
 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection and Data Collection Processes
2.4. Data Items
2.5. Study Risk-of-Bias Assessment
2.6. Certainty Assessment
3. Results
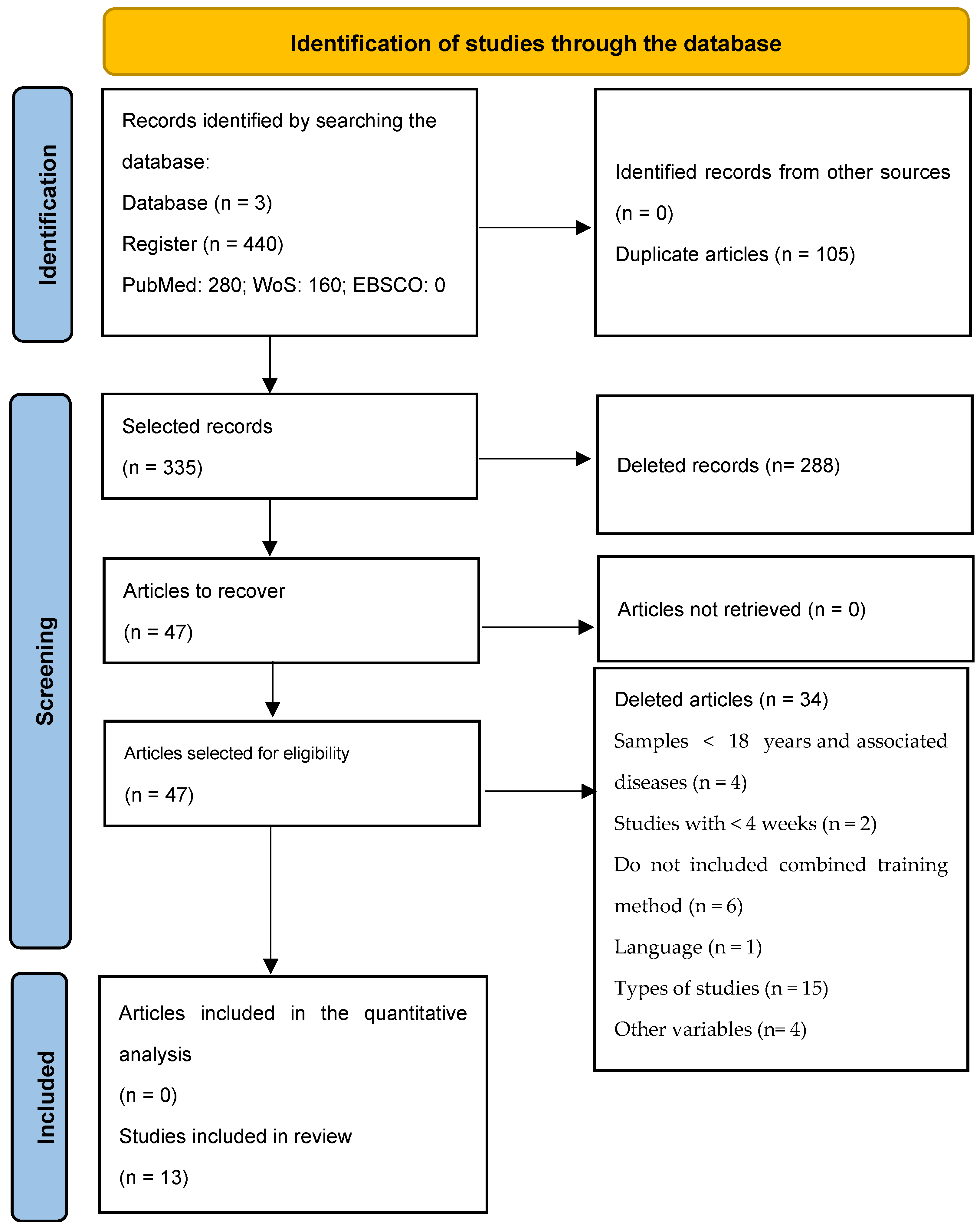
3.1. Study Identification and Selection
3.2. Study Characteristics
3.3. Risk of Bias in Studies
3.4. Intervention Characteristics
4. Discussion
5. Conclusions
- (i)
- Minimum duration of 14 weeks and never less than 6 weeks. Programs lasting 6 weeks did not have such positive effects in terms of the symptoms of the disease.
- (ii)
- Combined training programs are the most effective for this population, in order to reduce the symptoms of the disease. Training programs composed of aerobic exercises, strength training and stretching are the most indicated.
- (iii)
- Duration of sessions between 60 and 90 min, with the objective of executing the program outlined according to the limitations of each participant.
- (iv)
- Carry out the exercise program at least up to 3 times a week.
- (v)
- Aerobic exercises should be performed at 60–65% HRmax.
- (vi)
- Perform one set of exercises for large muscle groups (associated with pain points), consisting of 8 exercises and performing 8–10 repetitions in an initial phase, progressing to 15 repetitions. Rest at least 1–2 min between exercises.
- (vii)
- Perform static stretching exercises lasting 30–60 s for pain points.
- (viii)
- The intensity of the program should be light to moderate, following the ACSM guidelines for aerobic exercise.
6. Future Lines of Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atan, T.; Karavelioğlu, Y. Effectiveness of High-Intensity Interval Training vs Moderate-Intensity Continuous Training in Patients With Fibromyalgia: A Pilot Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2020, 101, 1865–1876. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, T.; Maguire, S.; Mockler, D.; Durcan, L.; Wilson, F. Behaviour Change Interventions Targeting Physical Activity in Adults with Fibromyalgia: A Systematic Review. Rheumatol. Int. 2019, 39, 805–817. [Google Scholar] [CrossRef]
- Chica, A.; Gonzalez-Guirval, F.; Reigal, R.E.; Carranque, G.; Hernandez-Mendo, A. Efectos de un programa de danza española en mujeres con fibromialgia. Cuad. Psicol. Deporte 2019, 1, 52–69. [Google Scholar] [CrossRef] [Green Version]
- Norouzi, E.; Hosseini, F.S.; Vaezmosavi, M.; Gerber, M.; Pühse, U.; Brand, S. Zumba Dancing and Aerobic Exercise Can Improve Working Memory, Motor Function, and Depressive Symptoms in Female Patients with Fibromyalgia. Eur. J. Sport Sci. 2020, 20, 981–991. [Google Scholar] [CrossRef]
- Chafer, S.; Hamilton, F. Efficacy of Physical Exercise Therapy as a Treatment for Fibromyalgia Patients. J. Phys. Ther. Health Promot. 2015, 3, 1–10. [Google Scholar] [CrossRef]
- Busch, A.J.; Webber, S.C.; Brachaniec, M.; Bidonde, J.; Bello-Haas, V.D.; Danyliw, A.D.; Overend, T.J.; Richards, R.S.; Sawant, A.; Schachter, C.L. Exercise Therapy for Fibromyalgia. Curr. Pain Headache Rep. 2011, 15, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.V.; Hung, C.H.; Sun, W.Z.; Wu, W.T.; Lai, C.L.; Han, D.S.; Chen, C.C. Evaluating Soreness Symptoms of Fibromyalgia: Establishment and Validation of the Revised Fibromyalgia Impact Questionnaire with Integration of Soreness Assessment. J. Formos. Med. Assoc. 2020, 119, 1211–1218. [Google Scholar] [CrossRef]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, Epidemiologic Profiles and Economic Costs. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef]
- Marques, A.P.; Santo, A.; de Sousa do Espírito Santo, A.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of Fibromyalgia: Literature Review Update. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Branco, J.C.; Rodrigues, A.M.; Gouveia, N.; Eusébio, M.; Ramiro, S.; Machado, P.M.; Pereira Da Costa, L.; Mourão, A.F.; Silva, I.; Laires, P.; et al. Prevalence of rheumatic and musculoskeletal diseases and their impact on health-related quality of life, physical function and mental health in Portugal: Results from EpiReumaPt—A national health survey. RMD Open 2016, 2, e000166. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F.; Allen, M.; Bennett, R.M.; Bombardier, C.; Broadhurst, N.; Cameron, R.S.; Carette, S.; Chalmers, A.; Cohen, M.; Crook, J.; et al. The Fibromyalgia Syndrome: A Consensus Report on Fibromyalgia and Disability. J. Rheumatol. 1996, 23, 534–539. [Google Scholar]
- Sarac, A.J.; Gur, A. Complementary and Alternative Medical Therapies in Fibromyalgia. Curr. Pharm. Des. 2006, 12, 47–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, J.M.; Mendonça, V.A.; Ribeiro, V.G.C.; Tossige-Gomes, R.; Fonseca, S.F.; Prates, A.C.N.; Flor, J.; Oliveira, A.C.C.; Martins, J.B.; Garcia, B.C.C.; et al. Does Whole Body Vibration Exercise Improve Oxidative Stress Markers in Women with Fibromyalgia? Braz. J. Med. Biol. Res. 2019, 52. [Google Scholar] [CrossRef] [Green Version]
- Mannerkorpi, K.; Nordeman, L.; Cider, Å.; Jonsson, G. Does moderate-to-high intensity Nordic walking improve functional capacity and pain in fibromyalgia? A prospective randomized controlled trial. Arthritis Res. Ther. 2010, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celenay, S.; Anaforoglu Kulunkoglu, B.; Yasa, M.E.; Sahbaz Pirincci, C.; Un Yildirim, N.; Kucuksahin, O.; Ugurlu, F.G.; Akkus, S. A Comparison of the Effects of Exercises plus Connective Tissue Massage to Exercises Alone in Women with Fibromyalgia Syndrome: A Randomized Controlled Trial. Rheumatol. Int. 2017, 37, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Bonnabesse, A.; Cabon, M.; L’Heveder, G.; Kermarrec, A.; Quinio, B.; Woda, A.; Marchand, S.; Dubois, A.; Giroux-Metges, M.A.; Rannou, F.; et al. Impact of a Specific Training Programme on the Neuromodulation of Pain in Female Patient with Fibromyalgia (DouFiSport): A 24-Month, Controlled, Randomised, Double-Blind Protocol. BMJ Open 2019, 9, e023742. [Google Scholar] [CrossRef]
- Wang, C.; Schmid, C.H.; Fielding, R.A.; Harvey, W.F.; Reid, K.F.; Price, L.L.; Driban, J.B.; Kalish, R.; Rones, R.; McAlindon, T. Effect of Tai Chi versus Aerobic Exercise for Fibromyalgia: Comparative Effectiveness Randomized Controlled Trial. BMJ 2018, 360, k851. [Google Scholar] [CrossRef] [Green Version]
- Pescatello, L.S.; Riebe, D.; Arena, R. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2014. [Google Scholar]
- Gómez-Hernández, M.; Gallego-Izquierdo, T.; Martínez-Merinero, P.; Pecos-Martín, D.; Ferragut-Garcías, A.; Hita-Contreras, F.; Martínez-Amat, A.; Montañez-Aguilera, F.J.; Achalandabaso Ochoa, A. Benefits of Adding Stretching to a Moderate-Intensity Aerobic Exercise Programme in Women with Fibromyalgia: A Randomized Controlled Trial. Clin. Rehabil. 2020, 34, 242–251. [Google Scholar] [CrossRef]
- De Souza, E.O.; Tricoli, V.; Roschel, H.; Brum, P.C.; Bacurau, A.V.N.; Ferreira, J.C.B.; Aoki, M.S.; Neves-Jr, M.; Aihara, A.Y.; Da Rocha Correa Fernandes, A.; et al. Molecular Adaptations to Concurrent Training. Int. J. Sports Med. 2013, 34, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Murlasits, Z.; Kneffel, Z.; Thalib, L. The Physiological Effects of Concurrent Strength and Endurance Training Sequence: A Systematic Review and Meta-Analysis. J. Sports Sci. 2018, 36, 1212–1219. [Google Scholar] [CrossRef]
- Worrel, L.M.; Krahn, L.E.; Sletten, C.D.; Pond, G.R. Treating Fibromyalgia with a Brief Interdisciplinary Program: Initial Outcomes and Predictors of Response. Mayo Clin. Proc. 2001, 76, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Valkeinen, H.; Alén, M.; Häkkinen, A.; Hannonen, P.; Kukkonen-Harjula, K.; Häkkinen, K. Effects of Concurrent Strength and Endurance Training on Physical Fitness and Symptoms in Postmenopausal Women With Fibromyalgia: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2008, 89, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.; Palstam, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Gerdle, B.; Kosek, E.; Mannerkorpi, K. Resistance Exercise Improves Muscle Strength, Health Status and Pain Intensity in Fibromyalgia-a Randomized Controlled Trial. Arthritis Res. Ther. 2015, 17, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triñanes, Y.; González-Villar, A.; Gómez-Perretta, C.; Carrillo-de-la-Peña, M.T. Profiles in Fibromyalgia: Algometry, Auditory Evoked Potentials and Clinical Characterization of Different Subtypes. Rheumatol. Int. 2014, 34, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, M.; Alvarez, M.; Monteiro, D.; Esteves, D.; Neiva, H. Exercise: Physical, Physiological and Psychological Benefits; Nova Science Publishers: New York, NY, USA, 2021. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88. [Google Scholar] [CrossRef] [PubMed]
- Rico-González, M.; Pino-Ortega, J.; Clemente, F.M.; Arcos, A.L. Guidelines for Performing Systematic Reviews in Sports Science. Biol. Sport 2022, 39, 463–471. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated Method Guidelines for Systematic Reviews in the Cochrane Collaboration Back Review Group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [Green Version]
- Kollen, B.J.; Lennon, S.; Lyons, B.; Wheatley-Smith, L.; Scheper, M.; Buurke, J.H.; Halfens, J.; Geurts, A.C.H.; Kwakkel, G. The Effectiveness of the Bobath Concept in Stroke Rehabilitation What Is the Evidence? Stroke 2009, 40, e89–e97. [Google Scholar] [CrossRef] [Green Version]
- Vaughan-Graham, J.; Cott, C.; Wright, F.V. The Bobath (NDT) Concept in Adult Neurological Rehabilitation: What Is the State of the Knowledge? A Scoping Review. Part II: Intervention Studies Perspectives. Disabil. Rehabil. 2015, 37, 1909–1928. [Google Scholar] [CrossRef]
- Gulsen, C.; Soke, F.; Eldemir, K.; Apaydin, Y.; Ozkul, C.; Guclu-Gunduz, A.; Akcali, D.T. Effect of Fully Immersive Virtual Reality Treatment Combined with Exercise in Fibromyalgia Patients: A Randomized Controlled Trial. Assist. Technol. 2020, 34, 256–263. [Google Scholar] [CrossRef]
- Sañudo, B.; Carrasco, L.; de Hoyo, M.; Oliva-Pascual-vaca, Á.; Rodríguez-Blanco, C. Changes in Body Balance and Functional Performance Following Whole-Body Vibration Training in Patients with Fibromyalgia Syndrome: A Randomized Controlled Trial. J. Rehabil. Med. 2013, 45, 678–684. [Google Scholar] [CrossRef] [Green Version]
- Sañudo, B.; de Hoyo, M.; Carrasco, L.; Rodríguez-Blanco, C.; Oliva-Pascual-Vaca, Á.; McVeigh, J.G. Effect of Whole-Body Vibration Exercise on Balance in Women with Fibromyalgia Syndrome: A Randomized Controlled Trial. J. Altern. Complement. Med. 2012, 18, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Romero-Zurita, A.; Carbonell-Baeza, A.; Aparicio, V.A.; Ruiz, J.R.; Tercedor, P.; Delgado-Fernández, M. Effectiveness of a Tai-Chi Training and Detraining on Functional Capacity, Symptomatology and Psychological Outcomes in Women with Fibromyalgia. Evid.-Based Complement. Altern. Med. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Corrales, B.S.; Galiano, D.; Carrasco, L.; de Hoyo, M.; McVeigh, J.G. Effects of a Prolonged Exercise Programe on Key Health Outcomes in Women with Fibromyalgia: A Randomized Controlled Trial. J. Rehabil. Med. 2011, 43, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Sañudo, B.; Galiano, D.; Carrasco, L.; Blagojevic, M.; de Hoyo, M.; Saxton, J. Aerobic Exercise versus Combined Exercise Therapy in Women with Fibromyalgia Syndrome: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2010, 91, 1838–1843. [Google Scholar] [CrossRef]
- Carbonell-Baeza, A.; Aparicio, V.A.; Ortega, F.B.; Cuevas, A.M.; Alvarez, I.C.; Ruiz, J.R.; Delgado-Fernandez, M. Does a 3-Month Multidisciplinary Intervention Improve Pain, Body Composition and Physical Fi Tness in Women with Fibromyalgia? Br. J. Sports Med. 2011, 45, 1189–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, S.J.; Wessel, J.; Bhambhani, Y.; Sholter, D.; Maksymowych, W. The effects of exercise and education, individually or combined, in women with fibromyalgia. J. Rheumatol. 2002, 29, 2620–2627. [Google Scholar] [PubMed]
- Mannerkorpi, K. Pool Exercise Combined with an Education Program for Patients with Fibromyalgia Syndrome. A Prospective, Randomized Study The al-Andalus Project View Project. J. Rheumatol. 2000, 27, 2473–2481. [Google Scholar]
- Doerr, J.M.; Fischer, S.; Nater, U.M.; Strahler, J. Influence of Stress Systems and Physical Activity on Different Dimensions of Fatigue in Female Fibromyalgia Patients. J. Psychosom. Res. 2016, 93, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Overend, T.J.; Kim, S.Y.; Góes, S.M.; Boden, C.; Foulds, H.J.A. Aerobic Exercise Training for Adults with Fibromyalgia. Cochrane Datab. Syst. Rev. 2017, 6. [Google Scholar] [CrossRef]
- Häuser, W.; Klose, P.; Langhorst, J.; Moradi, B.; Steinbach, M.; Schiltenwolf, M.; Busch, A. Efficacy of Different Types of Aerobic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Arthritis Res. Ther. 2010, 12, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalá, P.; Peñacoba, C.; López-Roig, S.; Pastor-Mira, M.A. Effects of Walking as Physical Exercise on Functional Limitation through Pain in Patients with Fibromyalgia—How Does Catastrophic Thinking Contribute? Int. J. Environ. Res. Public Health 2023, 20, 190. [Google Scholar] [CrossRef] [PubMed]
- Okifuji, A.; Gao, J.; Bokat, C.; Hare, B.D. Management of Fibromyalgia Syndrome in 2016. Pain Manag. 2016, 6, 383–400. [Google Scholar] [CrossRef] [Green Version]
- Busch, A.J.; Barber, K.; Schachter, C.L.; Overend, T.J.; Peloso, P.M. Exercise for Fibromyalgia: A Systematic Review. J. Rheumatol. 2008, 35, 1130–1144. [Google Scholar] [PubMed]
- Dupree Jones, K. A Randomized Controlled Trial of Muscle Strengthening versus Flexibility Training in Fibromyalgia [Microform]. J. Rheumatol. 2002, 29, 1041–1048. [Google Scholar]
- Matsutani, L.A.; Marques, A.P.; Ferreira, E.A.G.; Assumpção, A.; Lage, L.V.; Casarotto, R.A.; Pereira, C.A.B.; Matsutani, L.A.; Marques, A.P.; Ferreira, E.A.G.; et al. Effectiveness of Muscle Stretching Exercises with and without Laser Therapy at Tender Points for Patients with Fibromyalgia Stretching Exercises and Laser Therapy for FM Patients/L.A. Matsutani et al. Clin. Exp. Rheumatol. 2007, 25, 410–415. [Google Scholar]
- Singleton, O.; Hölzel, B.K.; Vangel, M.; Brach, N.; Carmody, J.; Lazar, S.W. Change in Brainstem Gray Matter Concentration Following a Mindfulness-Based Intervention Is Correlated with Improvement in Psychological Well-Being. Front. Hum. Neurosci. 2014, 8, 33. [Google Scholar] [CrossRef] [Green Version]
- Nutt, D.J. The Neuropharmacology of Serotonin and Noradrenaline in Depression. Int. Clin. Psychopharmacol. 2002, 17 (Suppl. S1), S1–S12. [Google Scholar] [CrossRef]
- Montgomery, S. Reboxetine: Additional Benefits to the Depressed Patient. J. Psychopharmacol. 1997, 11 (Suppl. S4), S9–S15. [Google Scholar]
- Alarab, A.; Taqatqa, N. Resistance Exercises for Musculoskeletal Disorders. In Resistance Training; InTech: London, UK, 2023. [Google Scholar] [CrossRef]
- Winkelmann, A.; Bork, H.; Brückle, W.; Dexl, C.; Heldmann, P.; Henningsen, P.; Krumbein, L.; Pullwitt, V.; Schiltenwolf, M.; Häuser, W. Physiotherapy, Occupational Therapy and Physical Therapy in Fibromyalgia Syndrome: Updated Guidelines 2017 and Overview of Systematic Review Articles. Schmerz 2017, 31, 255–265. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Flub, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR Revised Recommendations for the Management of Fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Zamunér, A.R.; Andrade, C.P.; Arca, E.A.; Avila, M.A. Impact of Water Therapy on Pain Management in Patients with Fibromyalgia: Current Perspectives. J. Pain Res. 2019, 12, 1971–2007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Mansilla, J.; Mejías-Gil, A.; Garrido-Ardila, E.M.; Jiménez-Palomares, M.; Montanero-Fernández, J.; González-López-arza, M.V. Effects of Non-Pharmacological Treatment on Pain, Flexibility, Balance and Quality of Life in Women with Fibromyalgia: A Randomised Clinical Trial. J. Clin. Med. 2021, 10, 3826. [Google Scholar] [CrossRef] [PubMed]
- Leon-Llamas, J.L.; Villafaina, S.; Murillo-Garcia, A.; Collado-Mateo, D.; Domínguez-Muñoz, F.J.; Sánchez-Gómez, J.; Gusi, N. Strength Assessment under Dual Task Conditions in Women with Fibromyalgia: A Test–Retest Reliability Study. Int. J. Environ. Res. Public Health 2019, 16, 4971. [Google Scholar] [CrossRef] [Green Version]
- Paolucci, T.; Baldari, C.; Di Franco, M.; Didona, D.; Reis, V.; Vetrano, M.; Iosa, M.; Trifoglio, D.; Zangrando, F.; Spadini, E.; et al. A New Rehabilitation Tool in Fibromyalgia: The Effects of Perceptive Rehabilitation on Pain and Function in a Clinical Randomized Controlled Trial. Evid.-Based Complement. Altern. Med. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, A.; Webber, S.; Richards, R.; Bidonde, J.; Schacter, C.; Schafer, L.; Danylwin, A.; Sawant, A.; Dal Bello-Haas, V.; Rander, T.; et al. Resistance exercise training for fibromyalgia. Cochrane Datab. Syst. Rev. 2013, 12, CD010884. [Google Scholar] [CrossRef] [PubMed]
- Liguori, G.; Feito, Y.; Fountaine, C.F.; Roy, B.A. ACSM’S Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]


{kind=link}
| Database | Specificities of the Databases | Search Strategy | Number of Articles in Automatic Research |
|---|---|---|---|
| PubMed | Search for title and abstract also includes keywords | (“fibromyalgia”) AND (“concurrent training” OR “combined training” OR “cross training” | 280 |
| Web of Science | Search for title and abstract also includes keywords | (“fibromyalgia”) AND (“concurrent training” OR “combined training” OR “cross training” | 160 |
| EBSCO | Search for title and abstract also includes keywords | (“fibromyalgia”) AND (“concurrent training” OR “combined training” OR “cross training” | 0 |
| Author (Year) | Country | Objectives | Participants by Gender (N) | Age (M ± SD) | Years of Diagnosis | Instruments/Tests/Evaluation Tools and Variables |
|---|---|---|---|---|---|---|
| Gulsen et al., 2020 [33] | Turkey | To evaluate the effects of training combined with immersive virtual reality | N = 16; EG = 8 EG + Immersive Virtual Reality = 8 | EG = 38.5 (29.5–50.0) EG + Immersive Virtual Reality = 46.5 (36.5–49.5) | EG = 4 (2–7.5) EG + Immersive Virtual Reality = 4 (2.5–8) | VAS: Pain Biodex Balance System (Shirley, NY, USA): Balance FIQ: Impact of FM Questionnaire IPAQ: Levels of PA Questionnaire 6-MWT: Aerobic Capacity SF-36: Health status of population Questionnaire |
| Atan and Karavelioglu et al., 2020 [1] | Turkey | To compare high-intensity interval training versus a combined training of continuous moderate intensity and strength plus stretching exercises | N = 45 HIIT Group = 19 MICT Group = 19 CG = 17 | HIIT Group = 46.5 ± 9.4 MICT Group = 47.3 ± 8.0 CG = 52.7 ± 8.9 | HIIT Group = 3.1 MICT Group = 2.0 CG = 2.3 | FIQ VAS: Pain SF-36: Health status of population Questionnaire Maximal Cardiopulmonary Exercise Test InBody 720, Biospace: Body composition (Weight, waist circumference and BMI) |
| Wang et al., 2018 [17] | United States of America | To evaluate the effects of Tai Chi protocol versus aerobic exercise | N = 226 Tai Chi Group = 151 1 × 12 weeks = 39 2 × 12 weeks = 37 1 × 24 weeks = 39 2 × 24 weeks = 36 AEG 2 × 24 weeks = 75 | Tai Chi Group: 1 × 12 weeks = 53 ± 12.6; 2 × 12 weeks = 52,1 ± 10.3; 1 × 24 weeks = 50.8 ± 11.8; 2 × 24weeks = 52.1 ± 13.3 AEG 2 × 24 weeks = 50.9 ± 12.5 | Tai Chi Group: 1 × 12 weeks = 11.1 ± 8.6; 2 × 12 weeks = 12.6 ± 12.1; 1 × 24 weeks = 12 ± 8.3; 2 × 24 weeks = 13.8 ± 10.4; AEG 2 × 24 weeks M = 11.3 ± 8.7 | FIQ VAS: Pain Depression and Anxiety Questionnaire Pittsburgh Sleep Quality Questionnaire BDI-II: Depression and behavioural manifestations Questionnaire |
| Celenay et al., 2017 [15] | Germany | To compare the effectiveness of a 6-week combined exercise program with and without CMT on pain, fatigue, sleep problems, health status and quality of life | N = 20 EG N = 20 EG + connective tissue massage = 20 | EG = 39.9 ± 9.5 = 42.5 ± 8.3 | ND | IPAQ-7: Levels of PA Questionnaire VAS: Pain Sleep: Quality of sleep Questionnaire FIQ: Impact of FM Questionnaire SF-36: Health Status population Questionnaire |
| Sañudo et al., 2013 [34] | Spain | To determine the effect of body balance and dynamic strength of an exercise program complemented with WBV | N = 46 EG + WBV (WBVEX) = 15 EG = 15 CG = 16 | EG + WBV = 57.1 ± 6.8 EG = 62.2 ± 9.8 CG = 55.5 ± 7.9 | EG + WBV = 8.5 ± 7.4 EG = 9.2 ± 8.3 CG = 8.8 ± 8.2 | Biodex F1C Stability System (BSS; Biodex, Inc. Shirley, NY, USA): Body Balance and Lower Limb Dynamic Strength |
| Sañudo et al., 2012 [35] | Spain | To analyse the effects of balance and strength through an exercise training program combined with WBV | N = 30 EG + WBV = 15 EG = 15 CG = 16 | = 59 ± 7.9 | ND | Biodex Stability System (BSS, Biodex, Inc., Shirley, NY): Body Balance The Galileo Fitness Platform (Novotech, Germany): Evaluation of knee extensor muscle strength |
| Romero-Zurita et al., 2012 [36] | Spain | To analyse the effects of Tai Chi training in women | N = 23 | = 51.4 ± 6.8 | ND | Body composition and anthropometric measurements: Weight, Waist Circumference, BMI FIQ SF-36: Health Status population Questionnaire Depression and Anxiety Questionnaire Vanderbiet Pain Management Inventory: Copping strategies Rosenbery Self-Esteem Scale: global self esteem General Self-Efficacy Scale: Beliefs in her/his own capabilities to attain aims |
| Sañudo et al., 2011 [37] | Spain | To analyse the effects on perceived health status, functional capacity and depression of a long-term exercise program versus usual care | N = 42 EG = 21 Usual Care CG = 21 | EG = 55.4 ± 7.1 Usual Care CG = 56.1 ± 8.4 | ND | FIQ SF-36: Health Status Population Questionnaire BDI: Attitudes and symptoms of stress Questionnaire |
| Sañudo et al., 2010 [38] | Spain | To determine the effects of supervised aerobic exercise and a supervised exercise program combined with aerobic exercise, strength and flexibility | N = 64 AEG2 CTG = 21 CG N = 21 | AE group = 55.9 ± 1.6; CTG M = 55.9 ± 1.7; CG = 29.7 ± 1.1 | ND | FIQ SF-36: Health Status Population Questionnaire BDI: Attitudes and symptoms of stress Questionnaire 6-MWT: Aerobic Capacity Hand-grip strength: Measure of muscular strength or the maximum force/tension by forearm muscles Flexion and extension (shoulders and hips): degrees |
| Carbonell-Balza et al., 2010 [39] | Spain | To analyse the effects on pain, body composition and physical fitness of a multidisciplinary intervention in women. | N = 75 EG = 41 CG = 34 | EG = 50 ± 7.3 CG = 51.4 ± 7.3 | ND | InBody 720; Biospace, Gateshead, UK: Body fat and muscle mass Functional Fitness Test Battery: lower and upper body strength and flexibility |
| Valkeineu et al., 2008 [23] | Finland | To determine the effects on muscle strength, aerobic and functional performance on postmenopausal symptoms of a combined strength and resistance training in women | N = 26 EG = 15 CG = 11 | EG = 59 ± 3 CG = 58 3 | ND | Health Assessment Questionnaire: Self-report functional status (disability) measures VO2 peak: Maximum oxygen carrying capacity with a bicycle ergometer test |
| King et al., 2002 [40] | Canada | To examine the effectiveness of a supervised aerobic exercise program, a self-management education program, and an exercise and education program for women | N = 152 EG = 46 Education group = 48 Exercise and Education Group = 37 CG = 39 | EG = 45.2 ± 9.4 Education group = 44.9 ± 10.0 Exercise and Education Group = 47.4 ± 9.0 CG = 47.3 ± 7.3 | EG= 7.8 ± 6.1 Education group= 10.9 ± 10.7 Exercise and Education Group = 8.9 ± 7.3 CG = 9.6 ± 7.9 | FIQ 6-MWT: Aerobic Capacity |
| Mannerkorpi et al., 2000 [41] | Sweden | To determine the effects of a pool-based exercise training program combined with an education program | N = 69 EG = 37 CG = 32 | EG = 45 ± 8.0 CG = 47 ± 11.6 | EG = 8.9 ± 7.2 CG = 8.4 ± 6.0 | FIQ 6 MW: Aerobic Capacity SF-36: Health Status population Questionnaire Arthritis Self Efficacy Scales: Pain and activities of daily living Questionnaire Arthritis Impact Measures Scales: Weight-bearing, posture and antigravity movement Questionnaire Quality of Life Questionnaire: Individual’s physical, psychological and social well-being Questionnaire |
| Study | PEDro Scale | Total Score | Methodological Quality | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 | C11 | |||
| Gulsen et al. [33] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 5 | Moderate |
| Atan and Karavelioglu et al. [1] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 | Good |
| Wang et al. [17] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 7 | Good |
| Celenay et al. [15] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 5 | Moderate |
| Sañudo et al. [34] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 | Good |
| Sañudo et e al. [35] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 6 | Good |
| Romero-Zurita et al. [36] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 8 | Good |
| Sañudo et al. [37] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 8 | Good |
| Sañudo et al. [38] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 | Good |
| Carbonell-Balza et al. [39] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 | Excellent |
| Valkeineu et al. [23] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 6 | Good |
| King et al. [40] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 6 | Good |
| Mannerkorpi et al. [41] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 5 | moderate |
| Author (Year) | Exercises | Frequency Program Length and Duration of Sessions | Intensity | Sets (N); Reps (N); Rest | Results |
|---|---|---|---|---|---|
| Gulsen et al., 2020 [33] | AEG: Treadmill; Pilates and IVR | Frequency: 2 × week Program length: 8 weeks Session duration: 80 min | AE = 60–80% HRmax | Non-Described | After the intervention, there were significant improvements in the exercise and Immersive Virtual Reality groups in pain, balance, impact of FM, fatigue, level of PA, functional exercise capacity and quality of life (p < 0.05). Exercise + IVR groups showed more improvements than exercise group in pain, fatigue, PA level, mental component and quality of life (p < 0.05). |
| Atan and Karavelioglu et al., 2020 [1] | HIIT—Cycle Ergometer MICT—Shoulder press with dumbbells or on machine; shoulder raises; bicep curl; squats; standing hip flexion and extension. | Frequency: 5 × week Program length: 6 weeks Time of the HIIT session— 35 min; MICT—55 min Control Group—without exercise | HIIT: 4 min sets at 80–95% of peak HR interspersed with three 3 min of active recovery intervals at 70% of peak HR and 5 min of return to calm at 50% of peak HR; MICT: 45 min of ST performed for the main muscle groups. | MICT: 1 set, 8–10 reps; HIIT: 4 sets of 4 min with 3 sets of 3 min of active recovery intervals and 5 min cool down period cycling | Group-time interactions were significant for the FIQ between interventions and control (p < 0.001). There were significant group-time interactions for the pain, SF-36 and cardiopulmonary exercise test parameters between treatments and control (all, p < 0.05). Body weight, fat percentage, fat-mass and BMI improved significantly (all, p < 0.05) only in MICT group after treatment. |
| Wang et al., 2018 [15] | Tai Chi: choreographed AE | Frequency: 1 or 2× week (Tai Chi and EA) Program: 52 weeks Session duration: 60 min | AE: 20 min of AE 50–60% HRmax and 11–13 on the RPE. From the 10th session, AE progressed to 60–70% of HRmax | Non-Described | Tai Chi groups improved significantly more than AEG in FIQ, anxiety and self-efficacy at 24 weeks either training 1 or 2 times per week (all, p < 0.05). Tai Chi groups compared with AE administered with the same intensity and duration (24 weeks, 2 times per week group) had greater benefits in FIQ p < 0.001. The groups who received Tai Chi for 24 weeks showed greater improvements in FIQ than Tai Chi Group of 12 weeks (p = 0.007). |
| Celenay et al., 2017 [15] | AE: walk on the treadmill for 20 min; ST: Deep neck muscles; deltoid; latissimus dorsi; pectoralis; scapular retractor muscles; external rotators of the shoulder; erector spinae; abdominals; and gluteus muscles. | Frequency: 2 × week Program duration: 6 weeks Session duration: 60 min | AE: 65–70% HRmax and then 75–80% HRmax; ST: Light/medium band and progress to a strong band | 1 set ST: 10 reps with a progression to 15 reps; | In the Exercise + connective tissue massage group, pain, fatigue and sleep problems decreased; health status and quality of life improved (p < 0.05). Exercises with connective tissue massage were superior in improving pain, fatigue, sleep problems and role limitations due to physical health compared to exercise alone. General health perceptions parameters related to quality of life improved in the Exercise group than in the connective tissue massage group (p < 0.05). |
| Sañudo et al., 2013 [34] | Exercise Group: 10–15 min of AE. This is followed by 15–20 min of ST. Exercise Group + WBV: stood on the platform on both legs, with both knees in isometric 120° flexion. Exercises such as unilateral static squats were used. | AE: 65–70% HRmax WBV: Vibration frequency of 30 Hz and at a peak-to-peak displacement of 4 mm (71.1 m/s−2 ≈ 7.2 g). | ST: 1 set; 8–10 reps. WBV: 6 sets in the exercises in which the participants stand on the platform and 4 sets in the isometric 30 s exercises with 45 s of recovery. | There were no between-group differences in any outcome measures (all p-values > 0.05), except for MLMD with open eyes between both experimental groups (p = 0.02). The 8-week intervention of exercises and WBV resulted in a statistically significant improvement in MLS I, and significant differences for the WBVEX over the EX group (p = 0.014) and over the CG (p = 0.029). | |
| Sañudo et e al., 2012 [35] | Exercise Group: combination of AE and ST. 10–15 min of AE; 15–20 min of ST Galileo Fitness_platform: stand up with both knees in isometric flexion plus unilateral static squats. | Frequency: 2 × week + 3 additional WBV sessions Program duration: 6 weeks Session duration: 45 min | Exercise Group: AE 65–70% HRmaxGalileo Fitness_platform: frequency of 20 Hz and variable amplitude of 2–3 mm. | ST: 1 set; 8 exercises; 8–10 reps; Galileo Fitness_platform: 3 sets of 45 s with a recovery of 120 s between sets and 4 sets of 15 s. The participants completed 15 s of the exercise on the right leg and then immediately completed 15 s on the left leg, and this was considered a set. | Exercise Groups of Medio-Lateral Stability Index improved balance when participants were assessed with eyes open and closed (all, p < 0.05). |
| Romero-Zurita et al., 2012 [36] | Yang style Tai-Chi forms, | Frequency: 3 × week Program: 28 weeks Session duration: 60 min | The average RPE value was 11 ± 1. | 8 forms of Tai-Chi, Yang style | Patients showed improvements in pain threshold and total number of tender points (all, p < 0.001). Tai-Chi group improved the FIQ total score (p < 0.001) and six subscales: stiffness (p = 0.005), pain, fatigue, morning tiredness, anxiety and depression (all, p < 0.001). The intervention was also effective in six SF-36 subscales: bodily pain (p = 0.003), vitality (p = 0.018), physical functioning, physical role, general health and mental health (all, p < 0.001) |
| Sañudo et al., 2011 [37] | Exercise Group: muscle-strengthening exercises, consisting of a circuit of 8 exercise stations (shoulder press; shoulder raises; biceps curl; squats; hip flexion and extension; and standing abductors). | Frequency: 2 × week Program: 24 weeks Session duration: 60 min | AE: 65–70% HRmax | ST: 1 set, at each station 8–10 reps with dumbbells 1–3 kg; | Improvements in the Medio–Lateral Stability Index and Medio–Lateral Mean Deflection with open eyes were found in the whole-body vibration exercise group compared with the control group (p = 0.02). |
| Sañudo et al., 2010 [38] | AE: 15–20 min continuous walking with arm movements, aerobic dancing and jogging Combined exercise: 10–15 min AE; jogging; 15–20 min of muscle strengthening for 8 muscle groups: deltoids, biceps, neck, hips, back and chest. | Frequency: 2 × week Program: 24 weeks Session duration: 60 min | AEG: between 60% and 65% HRmax Combined Exercise: AE 65–70% HRmax | EA Group: 1 series for muscle strengthening and flexibility exercises. 6 exercises of 1.5 min of AE Combined Exercise: 1 series for muscle strengthening and flexibility exercises. Muscle strengthening consisting of 8–10 reps with a load between 1 and 3 kg and flexibility: 3 reps for 8–9 exercises, holding the static position for 30 s. | An improvement from baseline in total FIQ score was observed in the exercise groups (p < 0.002) and it was accompanied by decreases in BDI scores of 8.5 (p < 0.001) and 6.4 (p < 0.001) points in the AE and CE groups, respectively. Relative to non-exercising controls, CE evoked improvements in the SF-36 physical functioning (p = 0.003) and bodily pain (p = 0.003) domains and it was more effective than AE for evoking improvements in the vitality (p = 0.002) and mental health (p = 0.04) domains. Greater improvements were observed in shoulder/hip range of motion and handgrip strength in the CE group. |
| Carbonell-Balza et al., 2010 [39] | 1st session, pool resistance exercises developed at a slow pace using water and aquatic materials as a means of resistance; 2nd session, pool-balance-oriented activities: position changes, walking backwards, coordination through aquatic exercises and dance exercises; 3rd session: land-based AE and coordination through an exercise circuit and 90 min of psychological follow-up. | Frequency: 3 × week Program: 12 weeks Session duration: 45 min of physical exercise classes; 90 min of psychological support | The average RPE was 12–13 AU. | Non-Described | A significant groupxtime effect for the left (L) and right (R) side of the anterior cervical (p < 0.001) and the lateral epicondyle R (p = 0.001) tender point. Pain threshold increased in the intervention group (positive) in the anterior cervical R (p < 0.001) and L (p = 0.012), and in the lateral epicondyle R (p = 0.010), whereas it decreased (negative) in the anterior cervical R (p < 0.001) and L (p = 0.002) in the usual care group. |
| Valkeineu et al., 2008 [23] | Concurrent training: in the 1st week, participants performed 2 strength training sessions and 1 endurance training session and in the 2nd week, 1 strength training and 2 endurance training sessions, and vice versa on alternate weeks. Strength training included isometric leg extension, concentric leg extension, elbow flexion and trunk flexion and extension. | Frequency: 3 × week Program: 21 weeks of combined training (strength and endurance training) Session duration: 60–90 min | Bicycle: 50 W with a load progression of 20 W until exhaustion Strength: 1 RM. | Bicycle: 3 min of heating with an intensity of 50 W and the load was increased to 20 W until exhaustion ST: 3 sets of exercises for legs, hips and knees and elbow flexors. Re-accelerate to maximum force for 3 to 5 s/1 min rest between exercises. | The concurrent training showed higher values in Wmax (p = 0.001), work time (p = 0.001), concentric leg extension force (p = 0.043), walking (p = 0.001), stair-climbing (p < 0.001) time and fatigue (p = 0.038) than strength training. The training led to an increase of 10% (p = 0.004) in Wmax and 13% (p = 0.004) than control group. |
| King et al., 2002 [40] | Education Group was based on self-management principles, where information was given about FM and individual goals and strategies for dealing with pain or other symptoms were established, guiding the participants toward a balanced and active life. Exercise Group included AE walking in deep or shallow water or low-impact AE such as walking outdoors. Education + EG was a combination of the previous protocols. | Frequency: 3 × week Program: 12 weeks Session duration: Exercise Group: 40 min Education Group: 60 min | AE: 60–75% HRmax | Non-Described | Only Exercise Group showed higher distance in the Six-Minute-Walk test (p = 0.04) when compared with Education Group. |
| Mannerkorpi et al., 2000 [41] | Exercise program in a heated pool and included resistance, flexibility, coordination and relaxation exercises. | Frequency: 1 × week Program: 24 weeks Session duration: 35 min | ND | Non-Described | Significant differences between the treatment group and the control group were found for the FIQ total score (p = 0.017) and the 6 min walk test (p < 0.001). Significant differences were also found for physical function, grip strength, pain severity, social functioning, psychological distress and quality of life for the treatment group. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, M.; Oliveira, R.; Brito, J.P.; Martins, A.D.; Moutão, J.; Alves, S. Effects of Combined Training Programs in Individuals with Fibromyalgia: A Systematic Review. Healthcare 2023, 11, 1708. https://doi.org/10.3390/healthcare11121708
Sousa M, Oliveira R, Brito JP, Martins AD, Moutão J, Alves S. Effects of Combined Training Programs in Individuals with Fibromyalgia: A Systematic Review. Healthcare. 2023; 11(12):1708. https://doi.org/10.3390/healthcare11121708
Chicago/Turabian StyleSousa, Mónica, Rafael Oliveira, João Paulo Brito, Alexandre Duarte Martins, João Moutão, and Susana Alves. 2023. "Effects of Combined Training Programs in Individuals with Fibromyalgia: A Systematic Review" Healthcare 11, no. 12: 1708. https://doi.org/10.3390/healthcare11121708