
Distinct Clinical Presentations and Outcomes of Hospitalized Adults with the SARS-CoV-2 Infection Occurring during the Omicron Variant Surge

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection
2.3. Outcome Measures and Definitions
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iuliano, A.D.; Brunkard, J.M.; Boehmer, T.K.; Peterson, E.; Adjei, S.; Binder, A.M.; Cobb, S.; Graff, P.; Hidalgo, P.; Panaggio, M.J.; et al. Trends in Disease Severity and Health Care Utilization During the Early Omicron Variant Period Compared with Previous SARS-CoV-2 High Transmission Periods-United States, December 2020-January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.; Whitaker, M.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Chai, S.J.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; et al. COVID-19-Associated Hospitalizations Among Adults During SARS-CoV-2 Delta and Omicron Variant Predominance, by Race/Ethnicity and Vaccination Status-COVID-NET, 14 States, July 2021-January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 466–473. [Google Scholar] [CrossRef]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; de Villiers, T.; Van der Walt, Z.; et al. Decreased severity of disease during the first global omicron variant covid-19 outbreak in a large hospital in tshwane, south africa. Int. J. Infect. Dis. 2022, 116, 38–42. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef] [PubMed]
- Collie, S.; Champion, J.; Moultrie, H.; Bekker, L.G.; Gray, G. Effectiveness of BNT162b2 Vaccine against Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 494–496. [Google Scholar] [CrossRef]
- Maslo, C.; Friedland, R.; Toubkin, M.; Laubscher, A.; Akaloo, T.; Kama, B. Characteristics and Outcomes of Hospitalized Patients in South Africa During the COVID-19 Omicron Wave Compared With Previous Waves. JAMA 2022, 327, 583–584. [Google Scholar] [CrossRef]
- Cegolon, L.; Ronchese, F.; Ricci, F.; Negro, C.; Larese-Filon, F. SARS-CoV-2 Infection in Health Care Workers of Trieste (North-Eastern Italy), 1 October 2020-7 February 2022: Occupational Risk and the Impact of the Omicron Variant. Viruses 2022, 14, 1663. [Google Scholar] [CrossRef] [PubMed]
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef]
- Schmidt, F.; Muecksch, F.; Weisblum, Y.; Da Silva, J.; Bednarski, E.; Cho, A.; Wang, Z.; Gaebler, C.; Caskey, M.; Nussenzweig, M.C.; et al. Plasma Neutralization of the SARS-CoV-2 Omicron Variant. N. Engl. J. Med. 2022, 386, 599–601. [Google Scholar] [CrossRef]
- Klann, J.G.; Strasser, Z.H.; Hutch, M.R.; Kennedy, C.J.; Marwaha, J.S.; Morris, M.; Samayamuthu, M.J.; Pfaff, A.C.; Estiri, H.; South, A.M.; et al. Distinguishing Admissions Specifically for COVID-19 From Incidental SARS-CoV-2 Admissions: National Retrospective Electronic Health Record Study. J. Med. Internet Res. 2022, 24, e37931. [Google Scholar] [CrossRef] [PubMed]
- Khullar, D. Do the Omicron Numbers Mean What We Think They Mean. The New Yorker, 16 January 2022; p. 1. [Google Scholar]
- Havers, F.P.; Patel, K.; Whitaker, M.; Milucky, J.; Reingold, A.; Armistead, I.; Meek, J.; Anderson, E.J.; Weigel, A.; Reeg, L.; et al. Laboratory-Confirmed COVID-19-Associated Hospitalizations Among Adults During SARS-CoV-2 Omicron BA.2 Variant Predominance-COVID-19-Associated Hospitalization Surveillance Network, 14 States, June 20, 2021-May 31, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1085–1091. [Google Scholar] [CrossRef]
- Voor In ’t Holt, A.F.; Haanappel, C.P.; Rahamat-Langendoen, J.; Molenkamp, R.; van Nood, E.; van den Toorn, L.M.; Peeters, R.P.; van Rossum, A.M.C.; Severin, J.A. Admissions to a large tertiary care hospital and Omicron BA.1 and BA.2 SARS-CoV-2 polymerase chain reaction positivity: Primary, contributing, or incidental COVID-19. Int. J. Infect. Dis. 2022, 122, 665–668. [Google Scholar] [CrossRef]
- Viana, R.; Moyo, S.; Amoako, D.G.; Tegally, H.; Scheepers, C.; Althaus, C.L.; Anyaneji, U.J.; Bester, P.A.; Boni, M.F.; Chand, M.; et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature 2022, 603, 679–686. [Google Scholar] [CrossRef]
- Esper, F.P.; Adhikari, T.M.; Tu, Z.J.; Cheng, Y.W.; El-Haddad, K.; Farkas, D.H.; Bosler, D.; Rhoads, D.; Procop, G.W.; Ko, J.S.; et al. Alpha to Omicron: Disease Severity and Clinical Outcomes of Major SARS-CoV-2 Variants. J. Infect. Dis. 2022, 227, 344–352. [Google Scholar] [CrossRef]
- de Prost, N.; Audureau, E.; Heming, N.; Gault, E.; Pham, T.; Chaghouri, A.; de Montmollin, N.; Voiriot, G.; Morand-Joubert, L.; Joseph, A.; et al. Clinical phenotypes and outcomes associated with SARS-CoV-2 variant Omicron in critically ill French patients with COVID-19. Nat. Commun. 2022, 13, 6025. [Google Scholar] [CrossRef]
- Hodgson, I.; Mower, L. First Omicron COVID Cases Detected in Florida, One at a Tampa VA Hospital. Available online: https://www.tampabay.com/news/health/2021/12/07/first-omicron-cases-detected-in-florida-one-at-a-tampa-va-hospital/ (accessed on 24 May 2023).
- Scobie, H.M.; Johnson, A.G.; Suthar, A.B.; Severson, R.; Alden, N.B.; Balter, S.; Bertolino, D.; Blythe, D.; Brady, S.; Cadwell, B.; et al. Monitoring Incidence of COVID-19 Cases, Hospitalizations, and Deaths, by Vaccination Status-13 U.S. Jurisdictions, April 4-July 17, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.W. Omicron Variant (B.1.1.529): Infectivity, Vaccine Breakthrough, and Antibody Resistance. J. Chem. Inf. Model. 2022, 62, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Lippi, G.; Nocini, R.; Henry, B.M. Analysis of online search trends suggests that SARS-CoV-2 Omicron (B.1.1.529) variant causes different symptoms. J. Infect. 2022, 84, e76–e77. [Google Scholar] [CrossRef]
- Carazo, S.; Skowronski, D.M.; Brisson, M.; Barkati, S.; Sauvageau, C.; Brousseau, N.; Gilca, R.; Fafard, J.; Talbot, D.; Ouakki, M.; et al. Protection against omicron (B.1.1.529) BA.2 reinfection conferred by primary omicron BA.1 or pre-omicron SARS-CoV-2 infection among health-care workers with and without mRNA vaccination: A test-negative case-control study. Lancet Infect. Dis. 2023, 23, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Self, W.H.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; McNeal, T.; et al. Effectiveness of mRNA Vaccination in Preventing COVID-19-Associated Invasive Mechanical Ventilation and Death-United States, March 2021-January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Accorsi, E.K.; Britton, A.; Fleming-Dutra, K.E.; Smith, Z.R.; Shang, N.; Derado, G.; Miller, J.; Schrag, S.J.; Verani, J.R. Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants. JAMA 2022, 327, 639–651. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. Covid-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Pulliam, J.R.C.; van Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022, 376, eabn4947. [Google Scholar] [CrossRef] [PubMed]
- Molani, S.; Hernandez, P.V.; Roper, R.T.; Duvvuri, V.R.; Baumgartner, A.M.; Goldman, J.D.; Ertekin-Taner, N.; Funk, C.C.; Price, N.D.; Rappaport, N.; et al. Risk factors for severe COVID-19 differ by age for hospitalized adults. Sci. Rep. 2022, 12, 6568. [Google Scholar] [CrossRef]
- Booth, A.; Reed, A.B.; Ponzo, S.; Yassaee, A.; Aral, M.; Plans, D.; Labrique, A.; Mohan, D. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef]
- Tsai, J.; Traub, E.; Aoki, K.; Oyong, K.; Sato, H.; Rizik-Baer, D.; Gounder, P. Incidentally Detected SARS-COV-2 Among Hospitalized Patients in Los Angeles County, August to October 2020. J. Hosp. Med. 2021, 16, 480–483. [Google Scholar] [CrossRef]
- Juthani, P.V.; Gupta, A.; Borges, K.A.; Price, C.C.; Lee, A.I.; Won, C.H.; Chun, H.J. Hospitalisation among vaccine breakthrough COVID-19 infections. Lancet Infect. Dis. 2021, 21, 1485–1486. [Google Scholar] [CrossRef] [PubMed]
- Moffa, M.A.; Shively, N.R.; Carr, D.R.; Bremmer, D.N.; Buchanan, C.; Trienski, T.L.; Jacobs, M.W.; Saini, V.; Walsh, T.L. Description of Hospitalizations due to the Severe Acute Respiratory Syndrome Coronavirus 2 Omicron Variant Based on Vaccination Status. Open Forum Infect. Dis. 2022, 9, ofac438. [Google Scholar] [CrossRef]
- Niu, J.; Sareli, C.; Mayer, D.; Visbal, A.; Sareli, A. Lymphopenia as a Predictor for Adverse Clinical Outcomes in Hospitalized Patients with COVID-19: A Single Center Retrospective Study of 4485 Cases. J. Clin. Med. 2022, 11, 700. [Google Scholar] [CrossRef] [PubMed]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and outcomes of COVID-19 hospitalisations: Systematic review and meta-analysis. BMJ Evid.-Based Med. 2021, 26, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Alimohamadi, Y.; Yekta, E.M.; Sepandi, M.; Sharafoddin, M.; Arshadi, M.; Hesari, E. Hospital length of stay for COVID-19 patients: A systematic review and meta-analysis. Multidiscip. Respir. Med. 2022, 17, 856. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
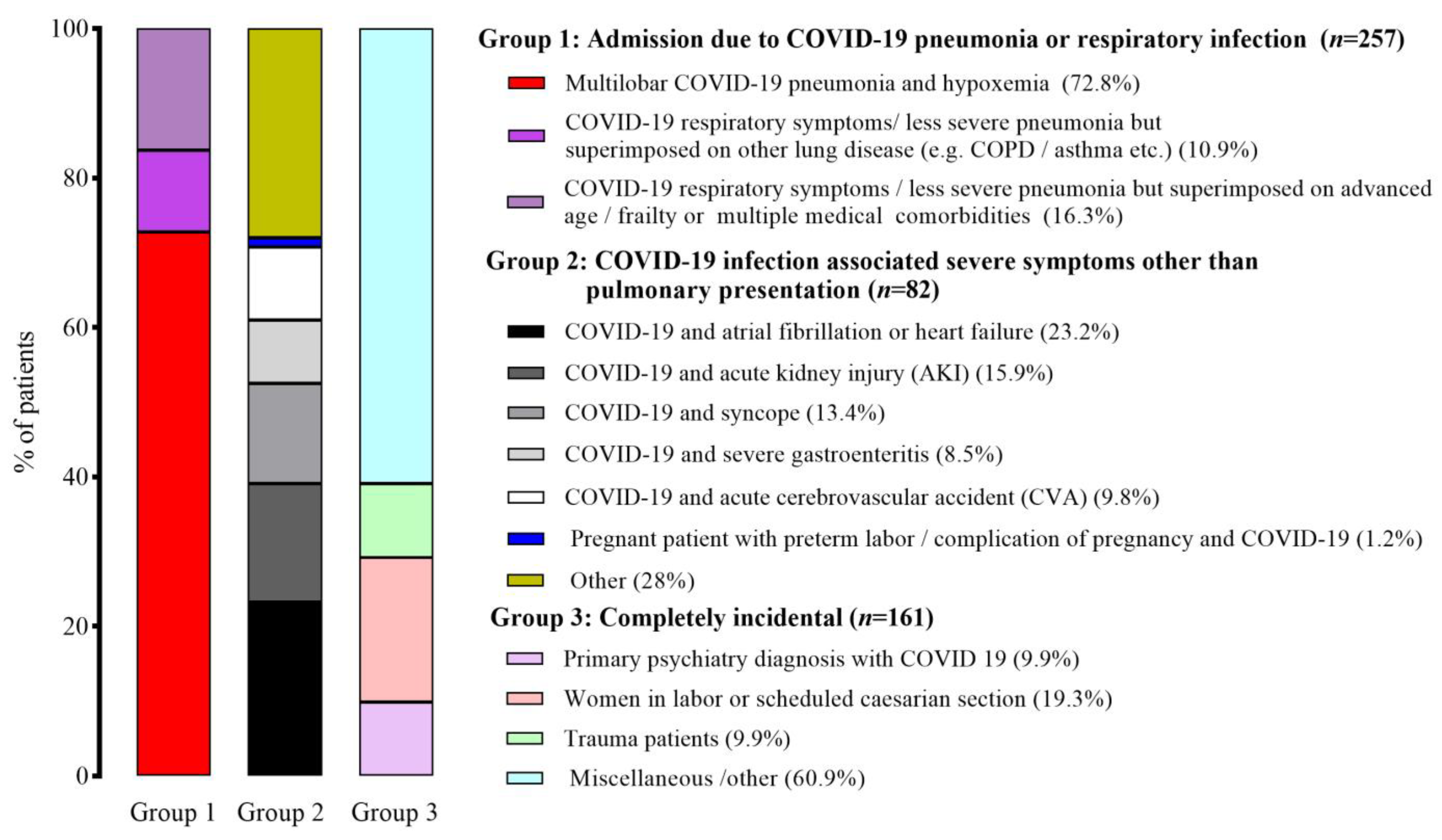
| Classification | Definition |
|---|---|
| Group 1: Primary COVID-19 | COVID-19 is the main cause for hospitalization. |
| (a) Multilobar COVID-19 pneumonia and hypoxemia. | |
| (b) COVID-19 respiratory symptoms/less severe pneumonia but on top of other lung disease (COPD/asthma, etc.). | |
| (c) COVID-19 respiratory symptoms/less severe pneumonia but on top of advanced age/frailty or multiple medical comorbidities. | |
| Group 2: Extrapulmonary manifestations of COVID-19 | COVID-19 is associated severe symptoms other than pulmonary presentation. |
| (a) COVID-19 with atrial fibrillation or heart failure. | |
| (b) COVID-19 with acute kidney injury. | |
| (c) COVID-19 with syncope. | |
| (d) COVID-19 with severe gastroenteritis. | |
| (e) COVID-19 and acute cerebrovascular accident. | |
| (f) COVID-19 with preterm labor/complication of pregnancy. | |
| (g) Other. | |
| Group 3: Incidental COVID-19 | COVID-19 is not the cause for hospitalization, and patient does not have any medical treatment related to COVID-19. |
| (a) Psychiatric patients with COVID-19. | |
| (b) Women in labor or scheduled for caesarean. | |
| (c) Trauma patients. | |
| (d) Miscellaneous/Other. |
| Group 1 | Group 2 | Group 3 | p-Value | p-Value | p-Value | |
|---|---|---|---|---|---|---|
| (n = 257) | (n = 82) | (n = 161) | Group 1 vs. Group 2 | Group 1 vs. Group 3 | Group 2 vs. Group 3 | |
| Age, years, median (IQR) | 73 (61–82) | 74 (62–81) | 58 (32–74) | 0.965 | <0.001 | <0.001 |
| Male sex | 123 (48.2) | 44 (53.7) | 62 (38.5) | 0.361 | 0.061 | 0.024 |
| Race | 0.654 | 0.005 | 0.287 | |||
| White | 176 (68.4) | 52 (63.4) | 85 (52.8) | |||
| Black | 74 (28.8) | 28 (34.1) | 71 (44.1) | |||
| Other | 7 (2.7) | 2 (2.4) | 5 (3.1) | |||
| Pre-existing health conditions | ||||||
| Hypertension | 186 (72.4) | 58 (70.7) | 82 (50.9) | 0.778 | <0.001 | 0.004 |
| Diabetes | 103 (40.1) | 37 (45.1) | 46 (28.6) | 0.804 | 0.021 | 0.015 |
| COPD/asthma | 48 (18.6) | 12 (14.6) | 18 (11.2) | 0.506 | 0.536 | 0.053 |
| Chronic kidney disease | 59 (19.4) | 29 (35.3) | 32 (19.8) | 0.030 | 0.543 | 0.012 |
| Coronary heart disease | 51 (19.8) | 27 (32.9) | 22 (13.7) | 0.016 | 0.113 | <0.001 |
| Cerebrovascular disease | 23 (8.9) | 9 (10.9) | 16 (9.9) | 0.664 | 0.732 | 0.825 |
| Heart failure | 32 (12.5) | 14 (17.1) | 12 (7.5) | 0.353 | 0.139 | 0.028 |
| Cardiac arrythmias | 47 (18.2) | 23 (28) | 12 (7.5) | 0.062 | 0.002 | <0.001 |
| Active malignancy | 14 (5.4) | 8 (9.8) | 9 (5.6) | 0.197 | >0.999 | 0.287 |
| History of malignancy | 30 (11.7) | 9 (10.9) | 13 (8.1) | >0.999 | 0.252 | 0.483 |
| Solid organ transplantation | 4 (1.6) | 4 (4.9) | 2 (1.2) | 0.100 | >0.999 | 0.183 |
| Bone marrow transplantation | 1 (0.4) | 2 (2.4) | 0 (0) | 0.146 | >0.999 | 0.112 |
| HIV infection | 2 (0.8) | 1 (1.2) | 3 (1.9) | 0.565 | 0.377 | >0.999 |
| Smoking | 93 (36.9) | 27 (32.9) | 30 (18.6) | 0.691 | <0.001 | 0.016 |
| Obesity | 111/254 (43.7) | 30/81 (37.0) | 38/130 (29.2) | 0.304 | 0.007 | 0.289 |
| Previous COVID-19 infection | 13/252 (5.2) | 4/77 (5.2) | 15/149 (10.1) | >0.999 | 0.070 | 0.312 |
| COVID-19 vaccination status | 0.306 | 0.192 | 0.056 | |||
| Fully vaccinated | 137 (53.3) | 48 (58.5) | 75 (46.5) | |||
| Unvaccinated | 120 (46.7) | 34 (41.5) | 86 (53.5) | |||
| Hospital LOS, days, median (IQR) | 6 (3–9) | 5 (4–8) | 3 (2–6) | >0.999 | <0.001 | 0.002 |
| ICU LOS, days, median (IQR) | 10 (3.5–16) | 10 (2–18) | 2.5 (1.3–3.0) | >0.999 | 0.055 | 0.189 |
| Age Status | Number of Patients, n (%) | Admission to ICU | p-Value | In-Hospital Death | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Yes, n (%) | Adjusted OR (95% CI) | Yes, n (%) | Adjusted OR (95% CI) | |||||
| Overall | <65 years | 205 (41) | 24 (11.7) | Reference | 10 (4.9) | Reference | ||
| ≥65 years | 295 (59) | 30 (10.2) | 0.85 (0.49–1.52) | 0.586 | 38 (12.9) | 2.24 (1.10–4.98) | 0.047 | |
| Subgroup analyses by age group | ||||||||
| Age < 65 years | Group 1 | 83 (40.5) | 19 (22.9) | 39.78 (1.13–308.17) | <0.001 | 8 (9.6) | Infinity (2.18–infinity) | 0.002 |
| Group 2 | 22 (10.7) | 3 (13.6) | 12.02 (1.07–135.08) | 0.044 | 2 (9.1) | Infinity (2.16–infinity) | 0.034 | |
| Group 3 | 100 (48.8) | 2 (2.0) | Reference | 0 (0.0) | Reference | |||
| Age ≥ 65 years | Group 1 | 179 (60.7) | 22 (12.3) | 4.91 (0.98–24.48) | 0.052 | 32 (17.9) | 25.62 (2.32–283.12) | 0.008 |
| Group 2 | 61 (20.7) | 6 (9.8) | 3.60 (0.61–21.19) | 0.156 | 5 (8.2) | 7.67 (0.57–103.31) | 0.124 | |
| Group 3 | 55 (18.6) | 2 (3.6) | Reference | 1 (1.8) | Reference | |||
| Vaccination Status | Number of Patients, n (%) | Admission to ICU | p-Value | In-Hospital Death | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Yes, n (%) | Adjusted OR (95% CI) | Yes, n (%) | Adjusted OR (95% CI) | |||||
| Overall | Unvaccinated | 240 (48) | 23 (9.6) | Reference | 19 (7.9) | Reference | ||
| Fully vaccinated | 260 (52) | 31 (11.9) | 1.17 (0.66–2.08) | 0.600 | 29 (11.2) | 1.12 (0.55–2.26) | 0.760 | |
| Subgroup analyses by number of doses of COVID-19 vaccine received | ||||||||
| 1 dose | Unvaccinated | 187 (77.9) | 15 (8.0) | Reference | 12 (6.4) | Reference | ||
| One dose | 53 (22.1) | 8 (15.1) | 1.15 (0.41–3.28) | 0.790 | 7 (13.2) | 2.13 (0.67–6.77) | 0.197 | |
| 2 doses | Unvaccinated | 187 (58.4) | 15 (8.0) | Reference | 12 (6.4) | Reference | ||
| Two doses | 190 (41.6) | 19 (10.0) | 1.39 (0.68–2.87) | 0.366 | 16 (8.4) | 1.67 (0.77–3.63) | 0.194 | |
| 3 doses | Unvaccinated | 187 (72.8) | 15 (8.0) | Reference | 12 (6.4) | Reference | ||
| Three doses | 70 (27.2) | 4 (5.7) | 0.45 (0.14–1.53) | 0.205 | 4 (5.7) | 0.88 (0.28–2.73) | 0.833 | |
| Comparison analyses by number of doses of COVID-19 vaccine received | ||||||||
| Number of doses of COVID-19 vaccine | One dose | 53 (16.9) | 8 (15.1) | Reference | 7 (13.2) | Reference | ||
| Two doses | 190 (60.7) | 19 (10.0) | 0.89 (0.37–2.16) | 0.893 | 16 (8.4) | 0.54 (0.25–2.91) | 0.788 | |
| Three doses | 70 (22.4) | 4 (5.7) | 0.37 (0.09–1.43) | 0.150 | 4 (5.7) | 0.38 (0.07–1.94) | 0.245 | |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age (years) | ||||
| ≥65 years | 2.21 (1.50–3.26) | <0.001 | 1.72 (1.07–2.77) | 0.025 |
| <65 years | 1.00 | 1.00 | ||
| Sex | ||||
| Male | 1.04 (0.71–1.53) | 0.834 | - | - |
| Female | 1.00 | |||
| Race | ||||
| Black | 0.82 (0.55–1.23) | 0.335 | - | - |
| Other | 1.21 (0.12–11.79) | 0.869 | - | - |
| White | 1.00 | |||
| BMI (kg/m2) | ||||
| >30 | 1.18 (0.78–1.79) | 0.433 | - | - |
| ≤30 | 1.00 | |||
| Diabetes | 1.32 (0.89–1.98) | 0.166 | - | - |
| Hypertension | 1.17 (0.79–1.74) | 0.444 | 0.51 (0.31–0.86) | 0.012 |
| COPD/asthma | 1.31 (0.64–2.67) | 0.456 | - | - |
| Chronic kidney disease | 1.09 (0.69–1.72) | 0.696 | - | - |
| Coronary heart disease | 1.51 (0.91–2.51) | 0.108 | - | - |
| Cerebrovascular disease | 0.97 (0.51–1.84) | 0.918 | - | - |
| Chronic liver disease | 1.68 (0.55–5.16) | 0.362 | - | - |
| Heart failure | 1.02 (0.58–1.82) | 0.935 | - | - |
| Cardiac arrythmias | 1.56 (0.90–2.72) | 0.112 | - | - |
| Active malignancy | 1.08 (0.49–2.41) | 0.845 | - | - |
| History of malignancy | 1.73 (0.86–3.46) | 0.122 | - | - |
| History of solid organ transplantation | 4.97 (0.64–38.89) | 0.126 | - | - |
| History of bone marrow transplantation | 0.88 (0.08–9.79) | 0.918 | - | - |
| HIV infection | 0.44 (0.09–2.18) | 0.313 | - | - |
| Previous COVID-19 infection | 0.92 (0.42–1.98) | 0.813 | - | - |
| COVID-19 vaccination | 1.37 (0.22–1.44) | 0.118 | - | - |
| Smoking | 0.78 (0.43–1.87) | 0.781 | - | - |
| Type of COVID-19 hospitalizations | ||||
| Group 1 | 3.63 (2.36–5.57) | <0.001 | 2.76 (1.72–4.42) | <0.001 |
| Group 2 | 3.51 (1.92–6.45) | <0.001 | 2.62 (1.36–5.04) | 0.004 |
| Group 3 | 1.00 | 1.00 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niu, J.; Kim, M.; Jalal, A.T.; Goldberg, J.E.; Acevedo Martinez, E.M.; Suarez Moscoso, N.P.; Rubio-Gomez, H.; Mayer, D.; Visbal, A.; Sareli, C.; et al. Distinct Clinical Presentations and Outcomes of Hospitalized Adults with the SARS-CoV-2 Infection Occurring during the Omicron Variant Surge. Healthcare 2023, 11, 1703. https://doi.org/10.3390/healthcare11121703
Niu J, Kim M, Jalal AT, Goldberg JE, Acevedo Martinez EM, Suarez Moscoso NP, Rubio-Gomez H, Mayer D, Visbal A, Sareli C, et al. Distinct Clinical Presentations and Outcomes of Hospitalized Adults with the SARS-CoV-2 Infection Occurring during the Omicron Variant Surge. Healthcare. 2023; 11(12):1703. https://doi.org/10.3390/healthcare11121703
Chicago/Turabian StyleNiu, Jianli, Myeongji Kim, Ayesha T. Jalal, Jessica E. Goldberg, Elsa M. Acevedo Martinez, Nathalie P. Suarez Moscoso, Heysu Rubio-Gomez, Daniel Mayer, Alvaro Visbal, Candice Sareli, and et al. 2023. "Distinct Clinical Presentations and Outcomes of Hospitalized Adults with the SARS-CoV-2 Infection Occurring during the Omicron Variant Surge" Healthcare 11, no. 12: 1703. https://doi.org/10.3390/healthcare11121703