
Causes for Medical Errors in Obstetrics and Gynaecology

Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
3. Results
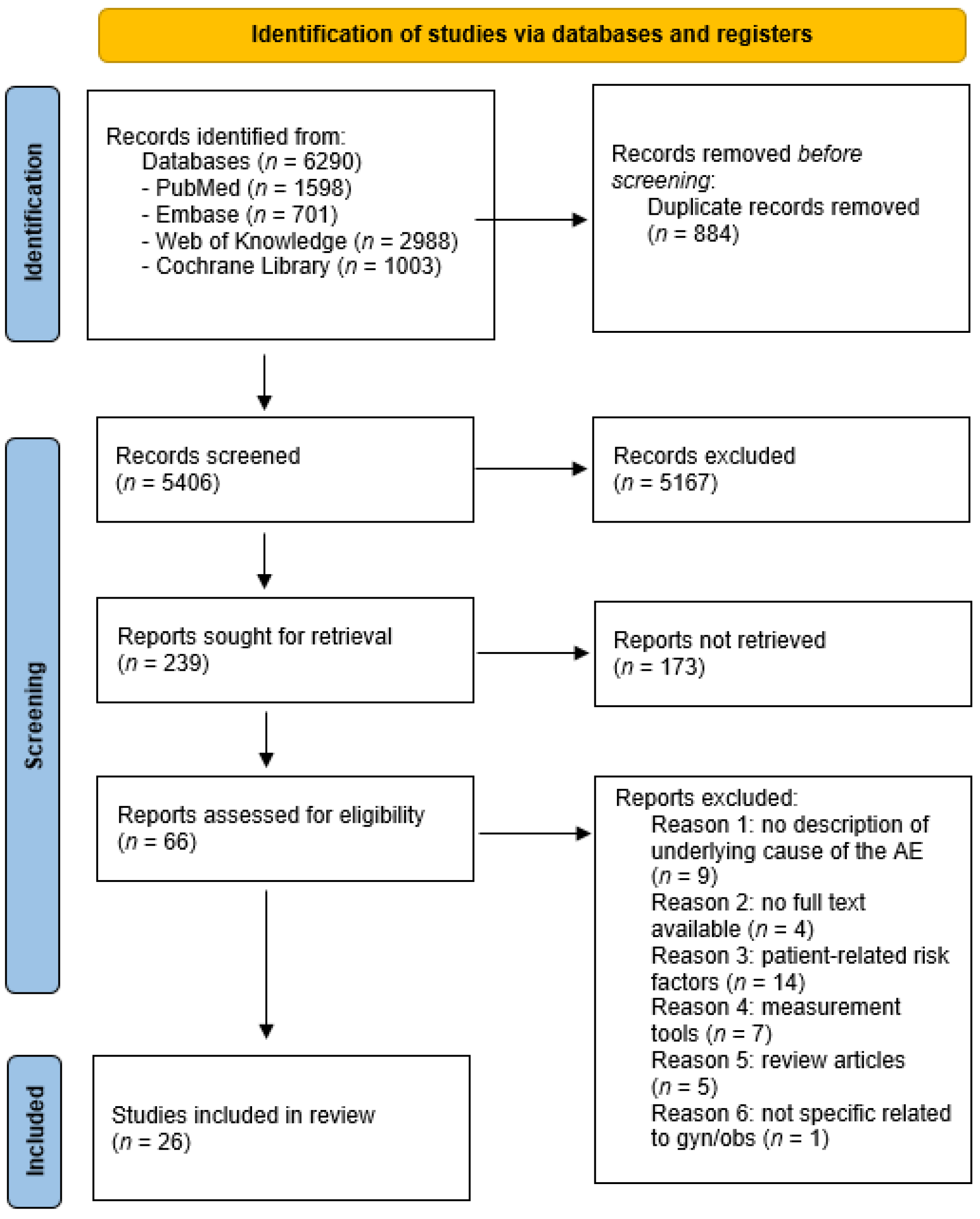
3.1. Results of the Search and Study Selection
3.2. Quality Criteria
3.3. Included Studies
3.4. Definitions
3.5. Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Search Database | Search Terms | Filters | Articles (n) |
|---|---|---|---|
| Pubmed | Medical error, medical mistake, adverse event, risk management, health care quality assessment, health care quality, access, and evaluation, gynaecology and/or obstetrics |
| 1598 |
| EMBASE | Medical error, medical mistake, adverse event, complication, risk factor, risk management, incident report, risk report, quality assurance, quality assessment, health care quality assessment, health care quality, access, and evaluation, gynaecology or obstetrics |
| 701 |
| Web of knowledge | Medical error, medical mistake, adverse event, complication, risk factor, risk management, incident report, quality assurance, quality assessment, health care quality assessment |
| 2988 |
| cocchrane library | Medical error, medical mistake, adverse event, risk management, health care quality assessment, health care quality, access and evaluation, gynaecology, obstetrics |
| 1003 |
| Total (before exclusion) | 6290 |
References
- Busse, R.P.D.; Quentin, W. Improving Healthcare Quality in Europe: Characteristics, Effectiveness and Implementation of Different Strategies; European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2019. [Google Scholar]
- Graafmans, W. EU Actions on Patient Safety and Quality of Healthcare; European Commission, Healthcare Systems Unit: Madrid, Spain, 2010. [Google Scholar]
- World Health Organization, Organisation for Economic Co-operation and Development & International Bank for Reconstruction and Development. Delivering Quality Health Services: A Global Imperative for Universal Health Coverage; World Health; World Health Organization, Organisation for Economic Co-operation and Development & International Bank for Reconstruction and Development: Geneva, Switzerland, 2018. [Google Scholar]
- OECD. Caring for Quality in Health: Lessons Learnt from 15 Reviews of Health Care Quality; OECD Publishing: Paris, France, 2017. [Google Scholar]
- Walshe, K. Adverse events in health care: Issues in measurement. Health Care Qual. 2000, 9, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Martin-Delgado, J.; Martínez-García, A.; Aranaz, J.M.; Valencia-Martín, J.L.; Mira, J.J. How Much of Root Cause Analysis Translates into Improved Patient Safety: A Systematic Review. Med. Princ. Pract. 2020, 29, 524–531. [Google Scholar] [CrossRef]
- Wilson, R.M.; Runciman, W.B.; Gibberd, R.W.; Harrison, B.T.; Newby, L.; Hamilton, J.D.; BS, F.R.M.W.M.; Fanzca, W.B.R.; Rn, R.B.T.H.; Llb, M.L.N.; et al. The Quality in Australian Health Care Study. Med. J. Aust. 1995, 163, 458–471. [Google Scholar] [CrossRef]
- Leape, L.L.; Brennan, T.A.; Laird, N.; Lawthers, A.G.; Localio, A.R.; Barnes, B.A.; Hebert, L.; Newhouse, J.P.; Weiler, P.C.; Hiatt, H. The Nature of Adverse Events in Hospitalized Patients. N. Engl. J. Med. 1991, 324, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Liu, P.; Gong, X.; Liang, F. Relating Medical Errors to Medical Specialties: A Mixed Analysis Based on Litigation Documents and Qualitative Data. Risk Manag. Health Policy 2020, 13, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar]
- Tello, J.E.; Barbazza, E.; Waddell, K. Review of 128 quality of care mechanisms: A framework and mapping for health system stewards. Health Policy 2019, 124, 12–24. [Google Scholar] [CrossRef]
- Worster, A.; Bledsoe, R.D.; Cleve, P.; Fernandes, C.M.; Upadhye, S.; Eva, K. Reassessing the Methods of Medical Record Review Studies in Emergency Medicine Research. Ann. Emerg. Med. 2005, 45, 448–451. [Google Scholar] [CrossRef]
- Aibar, L.; Rabanaque, M.J.; Aibar, C.; Aranaz, J.M.; Mozas, J. Patient safety and adverse events related with obstetric care. Arch. Gynecol. Obstet. 2014, 291, 825–830. [Google Scholar] [CrossRef]
- Aikpitanyi, J.; Ohenhen, V.; Ugbodaga, P.; Ojemhen, B.; Omo-Omorodion, B.I.; Ntoimo, L.F.; Imongan, W.; Balogun, J.; Okonofua, F.E. Maternal death review and surveillance: The case of Central Hospital, Benin City, Nigeria. PLoS ONE 2019, 14, e0226075. [Google Scholar] [CrossRef]
- Benimana, C.; Small, M.; Rulisa, S. Preventability of maternal near miss and mortality in Rwanda: A case series from the University Teaching Hospital of Kigali (CHUK). PLoS ONE 2018, 13, e0195711. [Google Scholar] [CrossRef]
- Carvalho, O.M.C.; Junior, A.B.V.; Augusto, M.C.C.; Leite, J.M.; Nobre, R.A.; Bessa, O.A.A.C.; De Castro, E.C.M.; Lopes, F.N.B.; Carvalho, F.H.C. Delays in obstetric care increase the risk of neonatal near-miss morbidity events and death: A case-control study. BMC Pregnancy Childbirth 2020, 20, 437. [Google Scholar] [CrossRef]
- David, E.; Machungo, F.; Zanconato, G.; Cavaliere, E.; Fiosse, S.; Sululu, C.; Chiluvane, B.; Bergström, S. Maternal near miss and maternal deaths in Mozambique: A cross-sectional, region-wide study of 635 consecutive cases assisted in health facilities of Maputo province. BMC Pregnancy Childbirth 2014, 14, 401. [Google Scholar] [CrossRef] [Green Version]
- Florea, A.; Caughey, S.S.; Westland, J.; Berckmans, M.; Kennelly, C.; Beach, C.; Dyer, A.; Forster, A.J.; Oppenheimer, L.W. The Ottawa Hospital Quality Incident Notification System for Capturing Adverse Events in Obstetrics. J. Obstet. Gynaecol. Can. 2010, 32, 657–662. [Google Scholar] [CrossRef]
- Habte, A.; Wondimu, M. Determinants of maternal near miss among women admitted to maternity wards of tertiary hospitals in Southern Ethiopia, 2020: A hospital-based case-control study. PLoS ONE 2021, 16, e0251826. [Google Scholar] [CrossRef]
- Haddad, S.M.; Cecatti, J.G.; Souza, J.P.; Sousa, M.H.; Parpinelli, M.A.; Costa, M.L.; Pacagnella, R.C.; Brum, I.R.; Filho, O.B.M.; Feitosa, F.E.; et al. Applying the Maternal Near Miss Approach for the Evaluation of Quality of Obstetric Care: A Worked Example from a Multicenter Surveillance Study. BioMed Res. Int. 2014, 2014, 989815. [Google Scholar] [CrossRef] [Green Version]
- Hüner, B.; Derksen, C.; Schmiedhofer, M.; Lippke, S.; Janni, W.; Scholz, C. Preventable Adverse Events in Obstetrics—Systemic Assessment of Their Incidence and Linked Risk Factors. Healthcare 2022, 10, 97. [Google Scholar] [CrossRef]
- Iwuh, I.A.; Fawcus, S.; Schoeman, L. Maternal near-miss audit in the Metro West maternity service, Cape Town, South Africa: A retrospective observational study. S. Afr. Med. J. 2018, 108, 171–175. [Google Scholar] [CrossRef] [Green Version]
- Jensen, K.R.; Hvidman, L.; Kierkegaard, O.; Gliese, H.; Manser, T.; Uldbjerg, N.; Brogaard, L. Noise as a risk factor in the delivery room: A clinical study. PLoS ONE 2019, 14, e0221860. [Google Scholar] [CrossRef] [Green Version]
- Johansen, L.T.; Braut, G.S.; Andresen, J.F.; Øian, P. An evaluation by the Norwegian Health Care Supervision Authorities of events involving death or injuries in maternity care. Acta Obstet. Gynecol. Scand. 2018, 97, 1206–1211. [Google Scholar] [CrossRef]
- Johansen, L.T.; Braut, G.S.; Acharya, G.; Andresen, J.F.; Øian, P. How common is substandard obstetric care in adverse events of birth asphyxia, shoulder dystocia and postpartum hemorrhage? Findings from an external inspection of Norwegian maternity units. Acta Obstet. Gynecol. Scand. 2020, 100, 139–146. [Google Scholar] [CrossRef]
- Kalisa, R.; Rulisa, S.; Akker, T.V.D.; Van Roosmalen, J. Maternal Near Miss and quality of care in a rural Rwandan hospital. BMC Pregnancy Childbirth 2016, 16, 324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasahun, A.W.; Wako, W.G. Predictors of maternal near miss among women admitted in Gurage zone hospitals, South Ethiopia, 2017: A case control study. BMC Pregnancy Childbirth 2018, 18, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, R.; Chauhan, S.; Daver, R.; Nandanwar, Y.; Patil, A.; Bhosale, A. Prospective observational study of near-miss obstetric events at two tertiary hospitals in Mumbai, Maharashtra, India. Int. J. Gynecol. Obstet. 2016, 132, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, M.A.; Mufidah, I.; Scroggs, S.; Siddiqui, A.R.; Raheel, H.; Wibdarminto, K.; Dirgantoro, B.; Vercruyssen, J.; Wahabi, H.A. Root-Cause Analysis of Persistently High Maternal Mortality in a Rural District of Indonesia: Role of Clinical Care Quality and Health Services Organizational Factors. BioMed. Res. Int. 2018, 2018, 3673265. [Google Scholar] [CrossRef] [Green Version]
- Mawarti, Y.; Utarini, A.; Hakimi, M. Maternal care quality in near miss and maternal mortality in an academic public tertiary hospital in Yogyakarta, Indonesia: A retrospective cohort study. BMC Pregnancy Childbirth 2017, 17, 149. [Google Scholar] [CrossRef]
- Mulongo, S.M.; Kaura, D.; Mash, B. Self-reported continuity and coordination of antenatal care and its association with obstetric near miss in Uasin Gishu county, Kenya. Afr. J. Prim. Health Care Fam. Med. 2023, 15, 8. [Google Scholar] [CrossRef]
- Nassoro, M.M.; Chiwanga, E.; Lilungulu, A.; Bintabara, D. Maternal Deaths due to Obstetric Haemorrhage in Dodoma Regional Referral Hospital, Tanzania. Obstet. Gynecol. Int. 2020, 2020, 8854498. [Google Scholar] [CrossRef]
- Neogi, S.B.; Sharma, J.; Negandhi, P.; Chauhan, M.; Reddy, S.; Sethy, G. Risk factors for stillbirths: How much can a responsive health system prevent? BMC Pregnancy Childbirth 2018, 18, 33. [Google Scholar] [CrossRef]
- Saucedo, M.; Bouvier-Colle, M.; Blondel, B.; Bonnet, M.; Deneux-Tharaux, C. Delivery Hospital Characteristics and Postpartum Maternal Mortality: A National Case-Control Study in France. Obstet. Anesth. Dig. 2020, 40, 54. [Google Scholar] [CrossRef]
- Sayinzoga, F.; Bijlmakers, L.; van Dillen, J.; Mivumbi, V.; Ngabo, F.; van der Velden, K. Maternal death audit in Rwanda 2009–2013: A nationwide facility-based retrospective cohort study. BMJ Open 2016, 6, e009734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, B.L.; Elsass, P.; Nielsen, B.B.; Massawe, S.; Nyakina, J.; Rasch, V. Substandard emergency obstetric care—A confidential enquiry into maternal deaths at a regional hospital in Tanzania. Trop. Med. Int. Health 2010, 15, 894–900. [Google Scholar] [CrossRef] [PubMed]
- Wasim, T.; Raana, G.; Wasim, M.; Mushtaq, J.; Amin, Z.; Asghar, S. Maternal near-miss, mortality and their correlates at a tertiary care hospital. J. Pak. Med. Assoc. 2021, 71, 1843–1848. [Google Scholar] [PubMed]
- Zewde, H.K. Quality and timeliness of emergency obstetric care and its association with maternal outcome in Keren Hospital, Eritrea. Sci. Rep. 2022, 12, 14614. [Google Scholar] [CrossRef] [PubMed]
- Pattinson, R.; Say, L.; Souza, J.P.; Broek, N.v.D.; Rooney, C. WHO maternal death and near-miss classifications. Bull. World Health Organ. 2009, 87, 734. [Google Scholar] [CrossRef]
- Hollnagel, E. FRAM: The Functional Resonance Analysis Method. Modelling Complex Socio-Technical Systems, 1st ed.; CRC Press: London, UK, 2012. [Google Scholar]

| Abstractors Training | Selection Criteria | Variable Definition | Abstraction Forms | Performance Monitored | Blind to Hypothesis | IRR * Mentioned | IRR * Tested | MR Identified | Sampling Method | Missing Data Management | Institutional Review Board | Total Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aibar [13] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 |
| Aikpitanyi [14] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 5 |
| Benimana [15] | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 6 |
| Carvalho [16] | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 6 |
| David [17] | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 6 |
| Florea [18] | No MRR, criteria inapplicable | ||||||||||||
| Habte [19] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 9 |
| Hadad [20] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 5 |
| Huner [21] | No MRR, criteria inapplicable | ||||||||||||
| Iwuh [22] | 0 | 1 | 1 | 1 | - | - | - | - | 1 | 1 | 0 | 0 | 5 |
| Jensen [23] | No MRR, criteria inapplicable | ||||||||||||
| Johansen [24] | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 5 |
| Johansen [25] | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Kalisa [26] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 5 |
| Kasahun [27] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 7 |
| Kulkarni [28] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 8 |
| Mahmood [29] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 4 |
| Mawarti [30] | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 4 |
| Mulongo [31] | No MRR, criteria inapplicable | ||||||||||||
| Nassoro [32] | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 3 |
| Neogi [33] | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 6 |
| Saucedo [34] | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Sayinzoga [35] | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 3 |
| Sorensen [36] | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 8 |
| Wasim [37] | No MRR, criteria inapplicable | ||||||||||||
| Zewde [38] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 8 |
| Author | Terms Used | Definition Used |
|---|---|---|
| Aibar [13] | Patient safety incident | Any event or circumstance that caused or could have caused unnecessary harm to a patient. |
| No harm incident | Any unforeseen and unexpected event recorded in the medical record that did not cause harm to the patient but which, under different circumstances, could have been an accident or an event that, if not discovered or corrected in time, could imply problems for the patient. | |
| Adverse event | Any unforeseen and unexpected accident recorded in the medical record that caused injury and/or disability and/or prolonged the hospital stay and/or led to death, which was the result of health care and not the patient’s underlying condition. | |
| Aikpitanyi [14] | Maternal death | No definition provided |
| Benimana [15] | Maternal near-miss | Refers to WHO criteria |
| Maternal deaths | Refers to WHO criteria | |
| Carvalho [16] | Three delays | Refers to WHO criteria |
| David [17] | Near-miss cases | Refers to clinical criteria for identification of near-miss (e.g., eclampsia, severe hemorrhage, severe sepsis, uterine rupture and severe malaria). |
| Florea [18] | Averse events | No definition provided |
| Incidents | No definition provided | |
| Near-misses | No definition provided | |
| Habte [19] | Maternal near-miss | Refers to WHO criteria |
| Haddad [20] | Severe maternal morbidity | Refers to WHO criteria |
| Hüner [21] | Adverse events | A catalogue of criteria or events was developed based on international research findings from scientific studies in two project meetings and interprofessional focus groups. |
| Iwuh [22] | Maternal near-miss | Refers to WHO criteria |
| Jensen [23] | Adverse health outcomes | No definition provided |
| Clinical performance | TeamOBS-PPH score | |
| Johansen [24] | Adverse events | No definition provided |
| Serious outcomes | No definition provided | |
| Serious adverse events | An injury was regarded as serious when it had serious consequences on the patient’s disease or disorder; or if it caused serious pain or reduced self-realization in the short or long term | |
| Johansen [25] | Serious adverse events | Three categories were described (birth asphyxia, shoulder dystocia and severe PPH) |
| Adequate obstetric care | Healthcare is in accordance with clinical practice based on Norwegian national and local obstetric guidelines. | |
| Kalisa [26] | Maternal near-miss | Refers to WHO criteria: a woman who almost died but survived a complication during pregnancy, childbirth or within 42 days after the termination of pregnancy. |
| Severe maternal outcome | Maternal near-miss and maternal deaths combined | |
| Kasahun [27] | Maternal near-miss/severe maternal morbidity | Refers to WHO criteria and states that the terms maternal near-miss and severe maternal morbidity are used interchangeably.Operational definition: maternal near-misses (severe maternal morbidity) is women who are admitted with either of the following obstetric diagnoses: severe preeclampsia, eclampsia, severe hemorrhage, dystocia (defined in the current study as uterine rupture, impending uterine rupture like prolonged labor with previous cesarean section, and emergency C/S delivery), severe anemia (<6), sepsis (puerperal sepsis, chorioamnionitis and septic abortion). |
| Kulkarni [28] | Near-miss obstetric event | Refers to WHO criteria. Near-miss obstetric event concerns a woman who nearly died as a result of a complication that occurred during pregnancy, childbirth or within 42 days of termination of pregnancy. Clinical criteria near-miss events were defined as any near-miss event related to a specific disease entity, while management-based near-miss events and organ-system dysfunction-based near-miss events were defined according to the near-miss approach outlined by WHO. |
| Mahmood [29] | Maternal deaths | No definition described |
| Mawarti [30] | Maternal deaths | Refers to WHO criteria |
| Maternal near-miss | Refers to WHO criteria | |
| Mulongo [31] | Maternal near-miss | Refers to WHO criteria |
| Nassoro [32] | Maternal deaths that occurred due to haemorrhage | No definition described |
| Neogi [33] | Stillbirths | Any baby born dead after the 24th week of pregnancy. |
| Saucedo [34] | Pregnancy-associated deaths | All deaths of women while pregnant or within one year of the termination of pregnancy, regardless of the cause of death. |
| Sayinzoga [35] | Maternal deaths | No definition described |
| Sorensen [36] | Maternal death | No definition described |
| Wasim [37] | Maternal deaths | Refers to WHO criteria |
| Maternal near-miss | Refers to WHO criteria | |
| Zewde [38] | Severe maternal outcome | Combination of maternal deaths and maternal near-miss |
| Maternal near-miss | Refers to WHO criteria |
| Quality of Care Mechanism | Study | Results | Percentages |
|---|---|---|---|
| Patients | Iwuh [22] | Patient education (lack of information) | 6.25 |
| Clinical practice | Aikpitanyi [14] | Delay in commencing treatment | 27.8 |
| Benimana [15] | Diagnostic delays | 41.3 | |
| Therapeutic delays | 5.8 | ||
| Florea [18] | Protocol | 5.9 | |
| Nursing resources | 0.2 | ||
| Physician resources | 1.7 | ||
| Other personnel | 0.7 | ||
| Equipment/resources | 6.9 | ||
| Records/results | 14.5 | ||
| Staff communication | 10.0 | ||
| Patient/family communication | 1.6 | ||
| Delay | 1.0 | ||
| Haddad [20] | Lack of trained staff | 5.1 | |
| Difficulty in monitoring | 8.1 | ||
| Delay in diagnosis | 5.6 | ||
| Delay in starting treatment | 6.5 | ||
| Delay in referral/transfer of the case | 5.2 | ||
| Improper management of the case | 21.8 | ||
| Iwuh [22] | Not managed at the level of care that was needed | 20.5 | |
| Clinical assessment (diagnosis), Problem recognition | 4.5 | ||
| Delay in referring | 0.9 | ||
| Managed at inappropriate level | 0.9 | ||
| Monitoring problems | 13.4 | ||
| Johansen [24] | Failure in surveillance | 36 | |
| Failure in diagnostics | 17 | ||
| Failure in operative delivery | 8 | ||
| Failure in resuscitation | 2 | ||
| Sayinzoga [35] | Lack of skilled staff | ||
| Insufficient diagnostic means | |||
| Inadequate monitoring of labour (use of partograph) | |||
| Delay in recognising the complication or administering the correct treatment | |||
| Insufficient follow-up in post-operative or postpartum period | |||
| No respect for asepsis | |||
| Not following protocol | |||
| Inadequate resuscitation | |||
| Insufficient follow-up of anaesthesia induction | |||
| Insufficient pre-operative preparation | |||
| Poor quality of antenatal care visit | |||
| Sorensen [36] | Training of staff insufficient | ||
| Habte [19] | Poor birth preparedness and poor complication readiness | 85.2 | |
| Johansen [25] | Delay in decision to operate | 8 | |
| Delay in decision to delivery time | 20 | ||
| Failure monitoring/Misinterpretation CTG | 13 | ||
| Medication error | 56.2 | ||
| Nasorro [32] | Delay in managing uterine atony | 17 | |
| Carvalho [16] | Inadequate prenatal care: improper conduct with patient | 5 neonatal near-miss/1 death | |
| Huner [21] | Peripartum therapeutic delay | 44.32 | |
| Diagnostic error | 36.36 | ||
| Inadequate birth position | 34.09 | ||
| Medication error | 2.27 | ||
| Zewde [38] | Insuffiency of medical staff | ||
| Delay in making diagnosis | |||
| Poor communication during referral | |||
| Emergency medicine | Aikpitanyi [14] | Delay in deciding to refer patients | 5.6 |
| Haddad [20] | Difficulty in communication between hospital and regulatory centre | 18.8 | |
| Delay in referral/transfer | 5.2 | ||
| Mahmood [29] | Failure in delay and emergency response | 42.9 | |
| Delay in procedures | 28.6 | ||
| Lack of policy, protocol and guidelines. | 46.4 | ||
| Delay in emergency response | 33.3 | ||
| Lacking knowledge and skills | 60 | ||
| Failure to follow best practice | 70 | ||
| Lack of recognition of seriousness. | 50 | ||
| Sayinzoga [35] | delay of the ambulance to reach the health centre | ||
| Nasorro [32] | Inadequate preparation in complete readiness | 17 | |
| Management | Aikpitanyi [14] | Lack of skilled manpower | 11.1 |
| Mahmood [29] | Inadequate access to senior clinical staff | 39.3 | |
| Failure to seek supervision or help | 43.3 | ||
| Sayinzoga [35] | Delay in referring the patient at high level | ||
| Sorensen [36] | Staff not available | ||
| Nasorro [32] | Delated referral from another facility | 26 | |
| Saucedo [34] | Lack of 24/7 on-site presence of obstetrician or anesthesiologist | 5/66 28/81 obstetrician | |
| 13/66 37/81 anesthesiologist | |||
| Zewde [38] | Unavailability of a senior obstetrician | ||
| Inappropriate management | |||
| Multiple referrals between health facilities | |||
| Health workforce | Johansen [24] | Failure in teamwork | 14 |
| Johansen [25] | Failure in cooperation between midwife and physician | 16 | |
| Pharmaceuticals and medical products | Aibar [13] | Peripheral venous catheter | 86.2 |
| Closed bladder catheter | 18.9 | ||
| Aikpitanyi [14] | Non-availability of blood products | 33.3 | |
| Lack of essential emergency drugs | 11.1 | ||
| Benimana [15] | Delayed or lacking supplies (blood and medication) | 5.8 | |
| Haddad [20] | Lack of medication | 1.8 | |
| Absence of blood products | 1.3 | ||
| Johansen [24] | Failure in administration of medication | 11.1 | |
| Sayinzoga [35] | Lack of isogroup blood | ||
| Wasim [37] | Inadequacy in blood arrangement | ||
| Zewde [38] | Lack of supplies and equipment | ||
| Health Facilities | Aikpitanyi [14] | Non-functional ICU | 11.1 |
| Carvalho [16] | Inadequate prenatal care: difficult access due to lack of specialised services | 46.5 | |
| Mulongo [31] | Lack of continuity of care and coordination | ||
| Wasim [37] | Inadequacy in overburdened ICU | ||
| Information Systems | Iwuh [22] | Incomplete registration (lack of information) | 6.3 |
| Johanssen [24] | Failure in documentation | 5 | |
| Huner [21] | Lack of documentation |
| Protocols | Delay | Equipment and Staff | Communication | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Presence of Adequate Protocol | Not Following Protocol | Delay in Referral/Transfer | Delay in Diagnostics | Delay in Decision-Making/Therapy | Lack of Equipment | Lack of (Well Trained) Staff | Verbal | Medical File | |
| Individual healthcare worker | 5.9% [18] 70% [24] | 0.9% [21] 5.2% [20] 5.6% [14] 26% [32] | 4.5% [22] 13.7% [20] 17% [25] 36.4% [21] 41.3% [15] | 5.8% [15] 6.5% [20] 27.8% [14] 28.6% [20] 33.3% [29] 44.3% [21] 46.0% [24] 48% [25] 61% [32] | 13% [32] 18.2% [21] 56% [25] 60% [29] | 1.6% [18] 6.25% [22] | 5% [24] 6.3% [22] | ||
| Teamwork | 14% [24] 39% [25] 43.3% [29] | 10% [18] | |||||||
| System | 46.4% [29] | 42.9% [29] | 6.9% [18] 55.5% [14] 5.8% [15] 3.1% [20] | 2.6% [18] 5.1% [20] 11.1% [14] 28% [34] 39.3% [29] | 18.8% [20] | 14.5% [18] | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klemann, D.; Rijkx, M.; Mertens, H.; van Merode, F.; Klein, D. Causes for Medical Errors in Obstetrics and Gynaecology. Healthcare 2023, 11, 1636. https://doi.org/10.3390/healthcare11111636
Klemann D, Rijkx M, Mertens H, van Merode F, Klein D. Causes for Medical Errors in Obstetrics and Gynaecology. Healthcare. 2023; 11(11):1636. https://doi.org/10.3390/healthcare11111636
Chicago/Turabian StyleKlemann, Désirée, Maud Rijkx, Helen Mertens, Frits van Merode, and Dorthe Klein. 2023. "Causes for Medical Errors in Obstetrics and Gynaecology" Healthcare 11, no. 11: 1636. https://doi.org/10.3390/healthcare11111636