Attitudes toward Medical Ethics among Obstetricians and Gynecologists in Saudi Arabia: An Exploratory Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Study Design and Setting
2.3. Statistical Methods
2.4. Ethical Considerations
3. Results
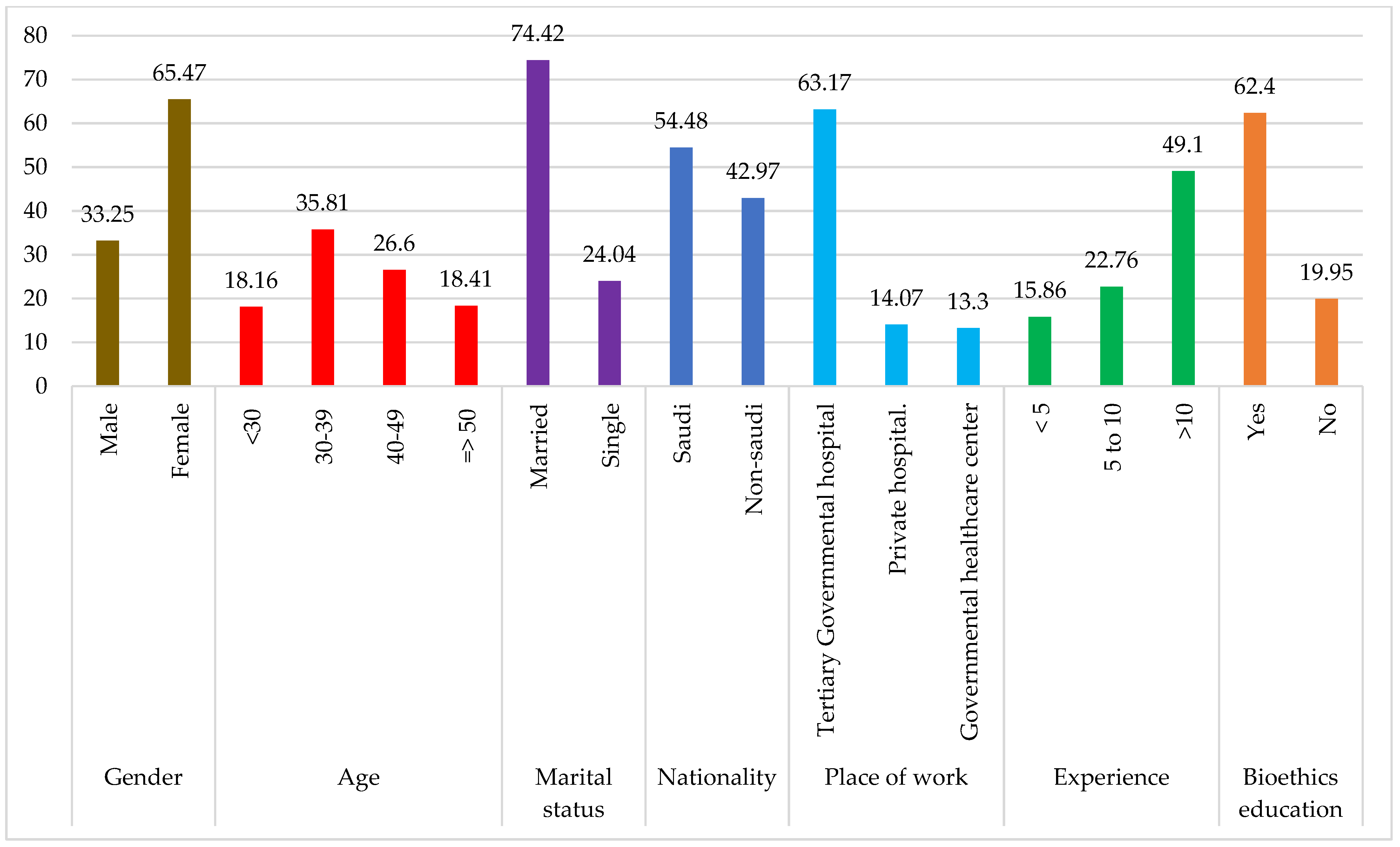
3.1. Demographic Characteristics of Respondents
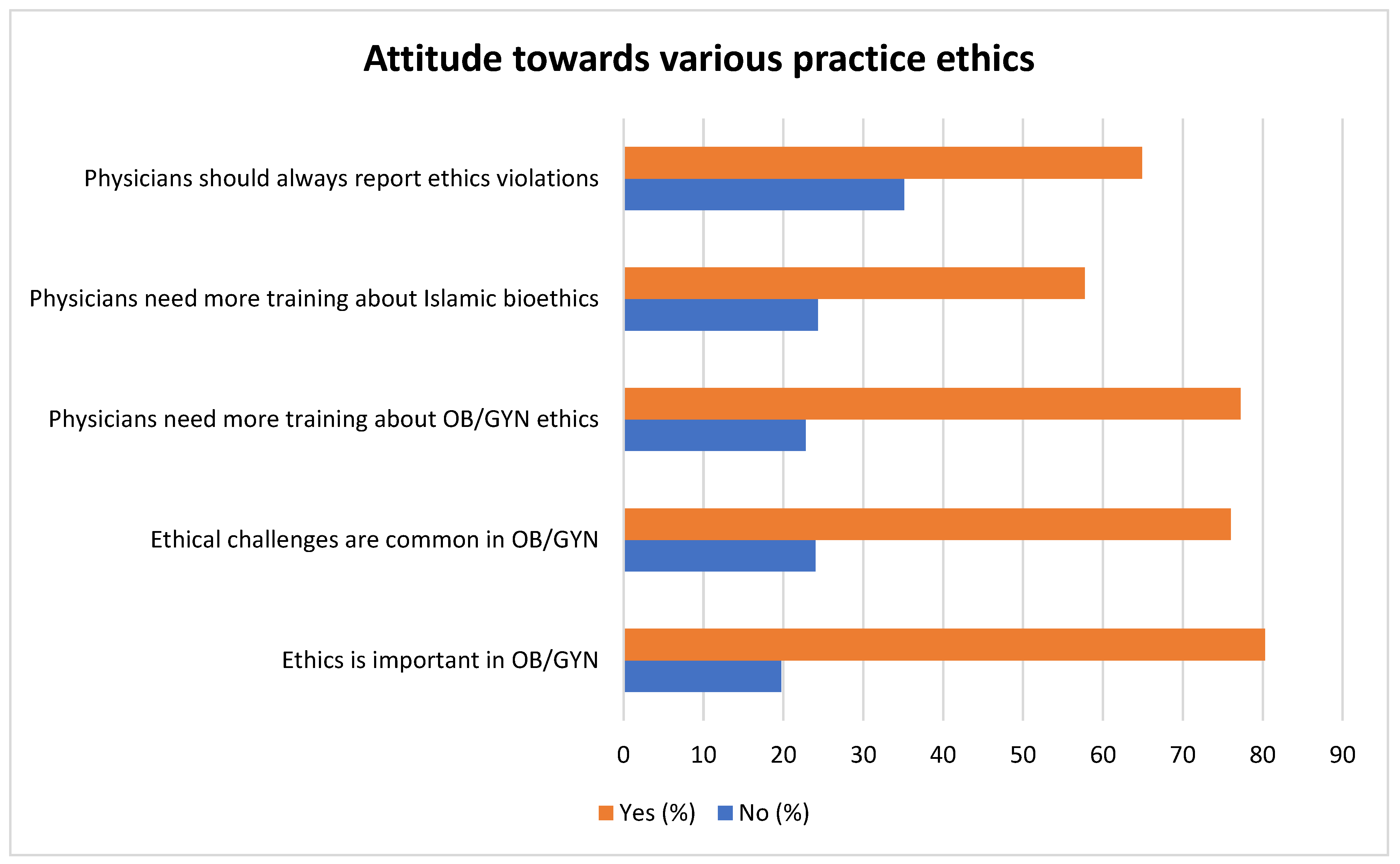
3.2. Attitude towards Various Practice Ethics
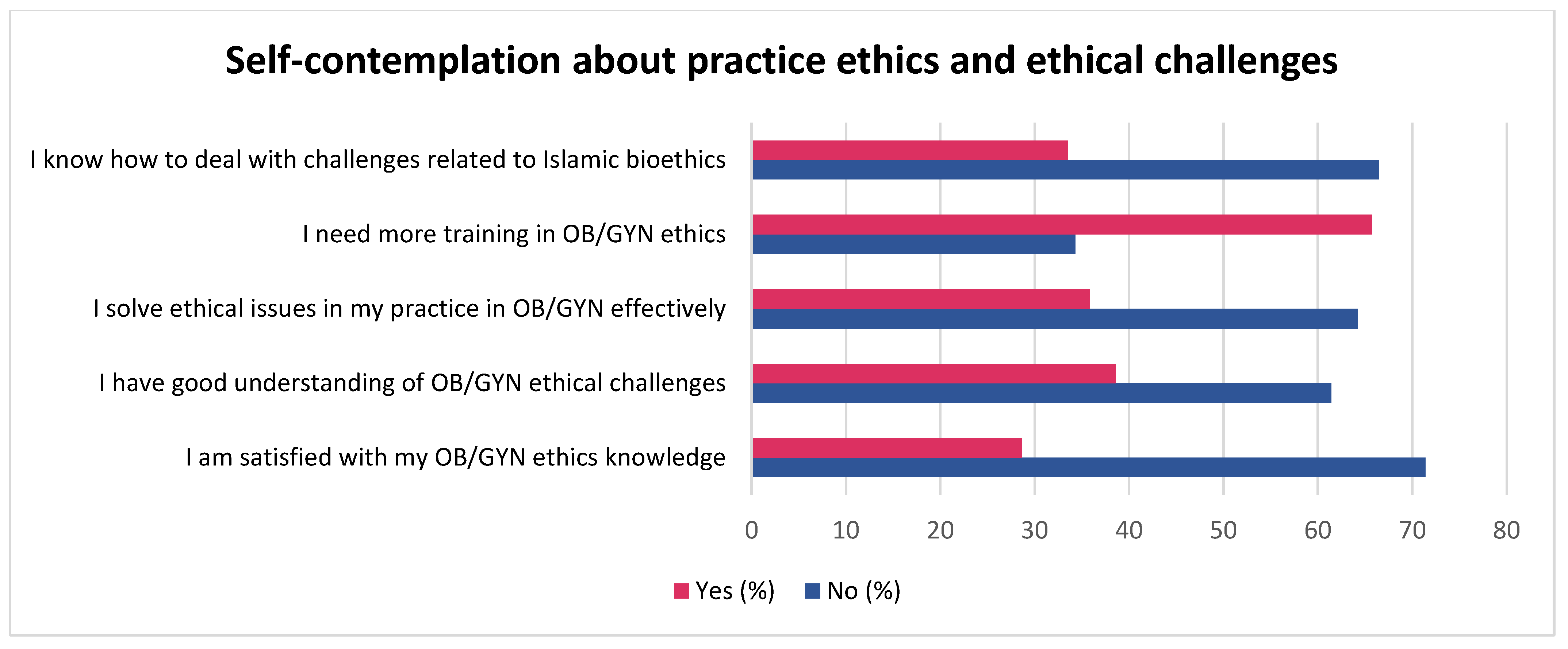
3.3. Self-Contemplation about Practice Ethics and Ethical Challenges
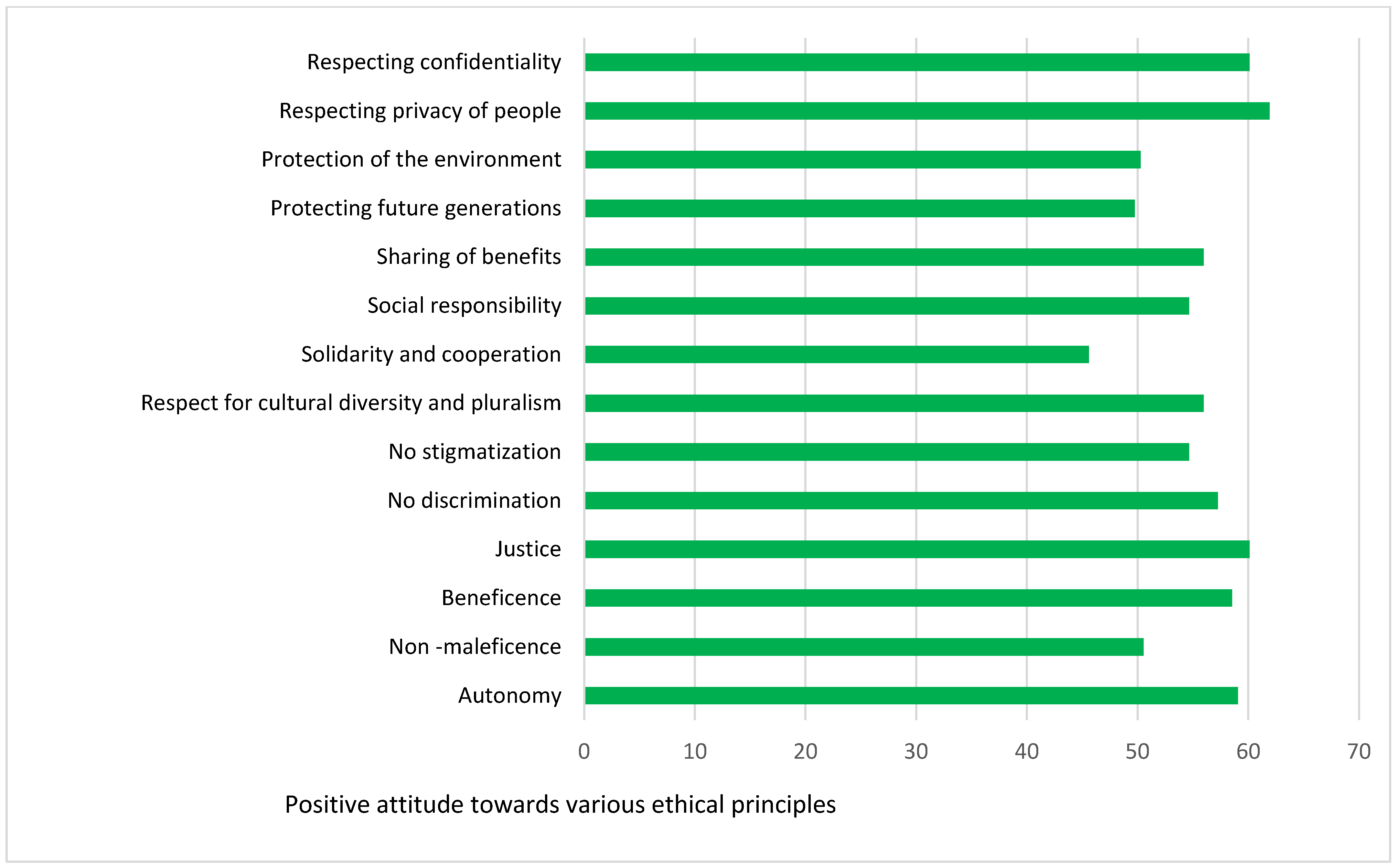
3.4. Attitude towards Primary and Secondary Ethical Principles
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hemberg, J.; Hemberg, H. Ethical competence in a profession: Healthcare professionals’ views. Nurs. Open 2020, 7, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Chervenak, F.A.; McCullough, L.B. The Professional Responsibility Model of Obstetric Ethics in Clinical Practice. Glob. Libr. Women’s Med. 2015, 27, 153–164. [Google Scholar] [CrossRef]
- Beachamp, T.; Childress, J. Principles of Biomedical Ethics: Marking Its Fortieth Anniversary. Am. J. Bioeth. 2019, 19, 9–12. [Google Scholar] [CrossRef]
- Serour, G.I. Global work of the International Federation of Gynecology and Obstetrics (FIGO). Facts Views Vis. ObGyn 2012, 4, 3. [Google Scholar]
- Zaami, S.; Orrico, A.; Signore, F.; Cavaliere, A.F.; Mazzi, M.; Marinelli, E. Ethical, Legal and Social Issues (ELSI) Associated with Non-Invasive Prenatal Testing: Reflections on the Evolution of Prenatal Diagnosis and Procreative Choices. Genes 2021, 12, 204. [Google Scholar] [CrossRef]
- Carvajal, B.; White, H.; Brooks, J.; Thomson, A.M.; Cooke, A. Experiences of midwives and nurses when implementing abortion policies: A systematic integrative review. Midwifery 2022, 111, 103363. [Google Scholar] [CrossRef]
- Gammon, B.; Kraft, S.; Michie, M.; Allyse, M. “I think we’ve got too many tests!”: Prenatal providers’ reflections on ethical and clinical challenges in the practice integration of cell-free DNA screening. Ethics Med. Public Health 2016, 2, 334–342. [Google Scholar] [CrossRef]
- American College of Obstetrics and Gynecology. ACOG Committee Opinion No. 390, December 2007. Ethical Decision Making in Obstetrics and Gynecology. Obstet. Gynecol. 2007, 110, 1479–1487. [Google Scholar] [CrossRef]
- McCullough, L.B.; Chervenak, F.A.; Coverdale, J.H. Professional Ethics in Obstetrics and Gynecology; Cambridge University Press: Cambridge, NY, USA, 2019; 248p. [Google Scholar] [CrossRef]
- Chamsi-Pasha, H.; Albar, M.A. Western and Islamic bioethics: How close is the gap? Avicenna J. Med. 2013, 3, 8–14. [Google Scholar] [CrossRef]
- Alahmad, G. The Saudi Law of Ethics of Research on Living Creatures and its Implementing Regulations. Dev. World Bioeth. 2016, 17, 63–69. [Google Scholar] [CrossRef]
- Laher, S. Islamic Medical Jurisprudence; Saudi Society for Studies in Medical Jurisprudence, Imam Muhammad Ibn Saud Islamic University, Ministry of Higher Education, Kingdom of Saudi Arabia: Riyadh, Saudi Arabia, 2009; ISBN 978-603-505-278-8. [Google Scholar]
- Alahmad, G. National Guidelines Regarding Research Ethics in Saudi Arabia. In Research Ethics in the Arab Region. Research Ethics Forum; Silverman, H., Ed.; Springer: Cham, Switzerland, 2017; Volume 5. [Google Scholar] [CrossRef]
- Law of Practicing Healthcare Professions. The Council of Ministers, Kingdom of Saudi Arabia. 2005. Available online: https://laws.boe.gov.sa/BoeLaws/Laws/LawDetails/f1de206c-eef4-4a76-904a-a9a700f2899a/2 (accessed on 7 May 2023).
- Alahmad, G.; Dierickx, K. What do Islamic institutional fatwas say about medical and research confidentiality and breach of confidentiality? Dev. World Bioeth. 2012, 12, 104–112. [Google Scholar] [CrossRef]
- Zuk, M. Medical Waste and Environmental Protection in Developing Countries. 2020. Available online: https://www.researchgate.net/publication/340661311_Mateusz_Zuk_Medical_waste_and_coronavirus_The_lessons_for_environment_protection_and_new_horizons_for_international_development (accessed on 7 May 2023).
- Al-Zahrani, M.; I Fakhri, Z.; A Al-Shanshouri, M.; Al-Ayed, M.H. Healthcare risk waste in Saudi Arabia. Rate of generation. Saudi Med. J. 2000, 21, 245–250. [Google Scholar] [PubMed]
- Al Naemi, H.; Izuka, K.; Edquibal, C.; Al-Korbi, N.; Al Kuwari, N.; Al Homaid, M. Quantitative Assessment of Medical Waste Management in Hamad Medical Corporation—Qatar. Occup. Dis. Environ. Med. 2021, 9, 112–126. [Google Scholar] [CrossRef]
- Pop Dual-Physician Marriages: Understanding the Challenges and Rewards. Cutis 2022, 110, E14–E16. [CrossRef]
- Byrne, J.; Straub, H.; DiGiovanni, L.; Chor, J. Evaluation of ethics education in obstetrics and gynecology residency programs. Am. J. Obstet. Gynecol. 2015, 212, 397.e1–397.e8. [Google Scholar] [CrossRef] [PubMed]
- Byrne, J.; Holmquist, S.; Derby, K.; Chor, J. Ethics Education in Obstetrics and Gynecology: A Survey of Resident Physicians. Med. Sci. Educ. 2017, 27, 345–351. [Google Scholar] [CrossRef]
- Alardan, A.; Alshammari, S.A.; Alruwaili, M. Knowledge, Attitude, and Practice of Family Medicine Trainees in Saudi Training Programs towards Medical Ethics, in Riyadh. J. Evol. Med. Dent. Sci. 2021, 10, 968–975. [Google Scholar] [CrossRef]
- Farrow, V.A.; Leddy, M.A.; Lawrence, H.; Schulkin, J. Ethical Concerns and Career Satisfaction in Obstetrics and Gynecology: A Review of Recent Findings From the Collaborative Ambulatory Research Network. Obstet. Gynecol. Surv. 2011, 66, 572–579. [Google Scholar] [CrossRef]
- Glynou, A.; Frysira, E.; Christakakou-Fotiadi, K.; Eleftheriadis, M.; Sarella, A.; Stergiotou, I.; Koukaki, M.; Chasalevri, E.; Galatis, D.; Salakos, N. The Cognitive Approach to Bioethical Issues in Perinatal Care in Greece. Cureus 2022, 14, e22760. [Google Scholar] [CrossRef]
- Al-Matary, A.; Ali, J. Controversies and considerations regarding the termination of pregnancy for Foetal Anomalies in Islam. BMC Med. Ethics 2014, 15, 10. [Google Scholar] [CrossRef]
- Negro, F.; Varone, M.C.; Del Rio, A.; Marinelli, S.; Basile, G. Conscientious objection to abortion: How to strike a legal and ethical balance between conflicting rights? Acta Biomed. 2022, 93, e2022279. [Google Scholar] [CrossRef] [PubMed]
- ITALY. Law No. 194 of 22 May 1978 on the Social Protection of Motherhood and the Voluntary Termination of Pregnancy. (Gazzetta Ufficiale della Repubblica Italiana, Part I, 2 May 1978, No. 140, pp. 3642–3646). Available online: http://www.columbia.edu/itc/history/degrazia/courseworks/legge_194.pdf (accessed on 7 May 2023).
- Zaręba, K.; La Rosa, V.L.; Kołb-Sielecka, E.; Ciebiera, M.; Ragusa, R.; Gierus, J.; Commodari, E.; Jakiel, G. Attitudes and Opinions of Young Gynecologists on Pregnancy Termination: Results of a Cross-Sectional Survey in Poland. Int. J. Environ. Res. Public Health 2020, 17, 3895. [Google Scholar] [CrossRef] [PubMed]
- Adinma, J. Litigations and the obstetrician in clinical practice. Ann. Med. Health Sci. Res. 2016, 6, 74–79. [Google Scholar] [CrossRef]
- AlDakhil, L.O. Obstetric and gynecologic malpractice claims in Saudi Arabia: Incidence and cause. J. Forensic Leg. Med. 2016, 40, 8–11. [Google Scholar] [CrossRef] [PubMed]
- SAUDI ARABIA. Basic Law of Governance, Royal Decree No. A/90 2 March 1992. (Official Translation Department). Available online: https://laws.boe.gov.sa/Files/Download/?attId=ed4842e1-9543-40b9-973b-ada200d4ed10 (accessed on 7 May 2023).
- Eleftheriades, A.; Tsagkaris, C.; Gozderesi, Y.; Panagopoulos, P. Making obstetrics more environmentally sustainable during and beyond the COVID-19 pandemic. Int. J. Health Plan. Manag. 2022, 37, 2992–2996. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Total No. of Respondents Who Completed the Questionnaire | Total Percentage of Respondents Who Completed the Questionnaire across Various Factors | ||
|---|---|---|---|---|
| N | % | % | ||
| Gender | Male | 130 | 33.25 | 98.72 |
| Female | 256 | 65.47 | ||
| Age | <30 | 71 | 18.16 | 98.98 |
| 30–39 | 140 | 35.81 | ||
| 40–49 | 104 | 26.60 | ||
| ≥50 | 72 | 18.41 | ||
| Marital status | Married | 291 | 74.42 | 98.47 |
| Single | 94 | 24.04 | ||
| Nationality | Saudi | 213 | 54.48 | 97.44 |
| Non-Saudi | 168 | 42.97 | ||
| Place of work | Tertiary governmental hospital | 247 | 63.17 | 90.54 |
| Private hospital | 55 | 14.07 | ||
| Governmental healthcare center | 52 | 13.30 | ||
| Experience | <5 | 62 | 15.86 | 87.72 |
| 5–10 | 89 | 22.76 | ||
| >10 | 192 | 49.10 | ||
| Bioethics education | Yes | 244 | 62.40 | 82.35 |
| No | 78 | 19.95 | ||
| Demographic Characteristics | Ethics is Important in OB/GYN | Ethical Challenges Are Common in OB/GYN | Physicians Need More Training about OB/GYN Ethics | Physicians Need More Training about Islamic Bioethics | Physicians Should Always Report Ethics Violations | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | ||
| Total | 314 | 80.3 | 297 | 76.0 | 302 | 77.2 | 296 | 57.7 | 254 | 64.9 | |
| Sex | M | 98 | 75.40 | 93 | 71.50 | 92 | 70.80 | 91 | 70.00 | 84 | 64.60 |
| F | 214 | 83.30 | 202 | 78.60 | 208 | 80.90 | 203 | 79.00 | 165 | 64.20 | |
| p = 0.064 | p = 0.123 | p = 0.024 | p = 0.051 | p = 0.936 | |||||||
| Age (years) | <30 | 51 | 71.80 | 51 | 71.80 | 50 | 70.40 | 48 | 67.60 | 42 | 59.20 |
| 30–39 | 119 | 85.00 | 111 | 79.30 | 115 | 82.10 | 111 | 79.30 | 89 | 63.60 | |
| 39–49 | 86 | 82.70 | 82 | 78.80 | 82 | 78.80 | 81 | 77.90 | 71 | 68.30 | |
| >49 | 57 | 79.20 | 52 | 72.20 | 54 | 75.00 | 55 | 76.40 | 49 | 68.10 | |
| p = 0.130 | p = 0.472 | p = 0.245 | p = 0.285 | p = 0.579 | |||||||
| Married | Yes | 234 | 80.40 | 220 | 75.60 | 224 | 77.00 | 220 | 75.60 | 182 | 62.50 |
| No | 76 | 80.10 | 73 | 77.70 | 75 | 79.80 | 73 | 77.40 | 65 | 69.10 | |
| p = 0.163 | p = 0.392 | p = 0.116 | p = 0.063 | p = 0.408 | |||||||
| Nationality | Saudi | 174 | 81.70 | 170 | 79.80 | 170 | 79.80 | 164 | 77.00 | 150 | 70.40 |
| Others | 135 | 80.40 | 123 | 73.20 | 127 | 75.60 | 127 | 75.60 | 97 | 57.70 | |
| p = 0.741 | p = 0.129 | p = 0.324 | p = 0.749 | p = 0.010 * | |||||||
| Workplace | Tertiary govern. hospital | 224 | 90.70 | 216 | 87.40 | 213 | 86.20 | 208 | 84.20 | 187 | 75.70 |
| Private hospital | 51 | 92.70 | 48 | 87.30 | 50 | 90.90 | 49 | 89.10 | 37 | 67.30 | |
| Govern. healthcare center | 39 | 75.00 | 33 | 63.50 | 39 | 75.00 | 39 | 75.00 | 27 | 51.90 | |
| p = 0.003 * | p = 0.000 * | p = 0.074 | p = 0.165 | p = 0.003 * | |||||||
| Bioethics education | Yes | 237 | 97.18 | 223 | 91.17 | 228 | 93.62 | 225 | 92.45 | 188 | 77.78 |
| No | 73 | 93.60 | 70 | 89.7 | 70 | 89.7 | 68 | 87.2 | 59 | 75.6 | |
| p = 0.066 | p = 0.093 | p = 0.043 * | p = 0.024 * | p = 0.057 | |||||||
| Years of experience | <5 | 52 | 83.90 | 49 | 79.00 | 50 | 80.60 | 48 | 77.40 | 37 | 59.70 |
| 5–10 | 81 | 91.00 | 77 | 86.50 | 79 | 88.80 | 76 | 85.40 | 61 | 68.50 | |
| >10 | 175 | 91.10 | 165 | 85.90 | 166 | 86.50 | 165 | 85.90 | 146 | 76.00 | |
| p = 0.234 | p = 0.368 | p = 0.354 | p = 0.262 | p = 0.039 * | |||||||
| Demographic Characteristics | I Am Satisfied with My OB/GYN Ethics Knowledge | I Have Good Understanding of OB/GYN Ethical Challenges | I Solve Ethical Issues in My Practice in OB/GYN Effectively | I Need More Training in OB/GYN Ethics | I Know How to Deal with Challenges Related to Islamic Bioethics | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | ||
| Total | 112 | 28.6 | 151 | 38.6 | 140 | 35.8 | 257 | 65.7 | 131 | 33.5 | |
| Sex | M | 48 | 36.90 | 66 | 50.80 | 61 | 46.90 | 76 | 58.50 | 55 | 42.30 |
| F | 64 | 24.90 | 83 | 32.30 | 77 | 30.00 | 179 | 69.60 | 75 | 29.20 | |
| p = 0.000 * | p = 0.000 * | p = 0.001 * | p = 0.028 * | p = 0.010 * | |||||||
| Age (years) | <30 | 8 | 11.30 | 10 | 14.10 | 46 | 64.80 | 10 | 14.10 | 13 | 18.30 |
| 30–39 | 36 | 25.70 | 50 | 35.70 | 45 | 32.10 | 106 | 75.70 | 43 | 30.70 | |
| 39–49 | 37 | 35.60 | 51 | 49.00 | 49 | 47.10 | 67 | 64.40 | 40 | 38.50 | |
| >49 | 31 | 43.10 | 39 | 54.20 | 36 | 50.00 | 37 | 51.40 | 34 | 47.20 | |
| p = 0.000 * | p = 0.000 * | p = 0.000 * | p = 0.005 * | p = 0.002 * | |||||||
| Married | Yes | 99 | 34.00 | 133 | 45.70 | 124 | 42.60 | 183 | 62.90 | 110 | 37.80 |
| No | 10 | 10.60 | 15 | 16.00 | 14 | 14.90 | 72 | 76.60 | 20 | 21.30 | |
| p = 0.000 * | p = 0.000 * | p = 0.000 * | p = 0.000 * | p = 0.013 * | |||||||
| Nationality | Saudi | 53 | 24.90 | 71 | 33.30 | 68 | 31.90 | 142 | 66.70 | 61 | 28.60 |
| Non-Saudi | 57 | 33.90 | 77 | 45.80 | 70 | 41.70 | 111 | 66.10 | 68 | 40.50 | |
| p = 0.05 * | p = 0.013 * | p = 0.049 * | p = 0.903 | p = 0.015 * | |||||||
| Workplace | Tertiary govern. hospital | 72 | 29.10 | 102 | 41.30 | 91 | 36.80 | 182 | 73.70 | 84 | 34.00 |
| Private hospital | 29 | 52.70 | 32 | 58.20 | 30 | 54.50 | 39 | 70.90 | 29 | 52.70 | |
| Govern. healthcare center | 11 | 21.20 | 17 | 32.70 | 19 | 36.50 | 36 | 69.20 | 18 | 34.60 | |
| p = 0.000 * | p = 0.001 * | p = 0.001 * | p = 0.755 | p = 0.069 | |||||||
| Bioethics education | Yes | 89 | 37.17 | 118 | 48.32 | 102 | 41.97 | 195 | 80.04 | 102 | 42.83 |
| No | 21 | 26.9 | 30 | 38.5 | 35 | 44.9 | 59 | 75.6 | 28 | 35.90 | |
| p = 0.171 | p = 0.506 | p = 0.808 | p = 0.549 | p = 0.167 | |||||||
| Years of experience | <5 | 12 | 19.40 | 14 | 22.60 | 17 | 27.40 | 46 | 74.20 | 12 | 19.40 |
| 5–10 | 20 | 22.50 | 31 | 34.80 | 26 | 29.20 | 74 | 83.10 | 28 | 31.50 | |
| >10 | 80 | 41.70 | 103 | 53.60 | 93 | 48.40 | 132 | 68.80 | 87 | 45.30 | |
| p = 0.000 * | p = 0.000 * | p = 0.001 * | p = 0.039 * | p = 0.001 * | |||||||
| Characteristics | Autonomy | Non-Maleficence | Beneficence | Justice | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | ||
| Sex | M | 76 | 58.46 | 66 | 50.77 | 73 | 56.15 | 80 | 61.54 |
| F | 152 | 59.38 | 129 | 50.39 | 153 | 59.77 | 182 | 71.09 | |
| p value | 0.897 | 0.915 | 0.524 | 0.65 | |||||
| Age (years) | <30 | 42 | 59.15 | 37 | 52.11 | 47 | 66.20 | 44 | 61.97 |
| 30–39 | 86 | 61.43 | 77 | 55.00 | 85 | 60.71 | 88 | 62.86 | |
| 39–49 | 62 | 59.62 | 52 | 50.00 | 61 | 58.65 | 64 | 61.54 | |
| >49 | 39 | 54.17 | 30 | 41.67 | 35 | 48.61 | 37 | 51.39 | |
| p value | 0.717 | 0.279 | 0.144 | 0.357 | |||||
| Married | Yes | 170 | 58.42 | 144 | 49.48 | 165 | 56.70 | 176 | 60.48 |
| No | 55 | 58.51 | 47 | 50.00 | 58 | 61.70 | 54 | 57.45 | |
| p value | 0.938 | 0.525 | 0.561 | 0.784 | |||||
| Nationality | Saudi | 134 | 62.91 | 115 | 53.99 | 133 | 62.44 | 132 | 61.97 |
| Others | 93 | 55.36 | 80 | 47.62 | 94 | 55.95 | 99 | 58.93 | |
| p value | 0.136 | 0.217 | 0.2 | 0.546 | |||||
| Workplace | Tertiary govern. hospital | 152 | 61.54 | 128 | 51.82 | 151 | 61.13 | 151 | 61.13 |
| Private hospital | 32 | 58.18 | 29 | 52.73 | 33 | 60.00 | 34 | 61.82 | |
| Govern. healthcare center | 24 | 46.15 | 20 | 38.46 | 22 | 42.31 | 24 | 46.15 | |
| p value | 0.027 * | 0.013 * | 0.008 * | 0.013 * | |||||
| Bioethics education | Yes | 142 | 58.20 | 127 | 52.05 | 142 | 58.20 | 145 | 59.43 |
| No | 50 | 64.10 | 37 | 47.44 | 48 | 61.54 | 47 | 60.26 | |
| p value | 0.628 | 0.594 | 0.878 | 0.714 | |||||
| Years of experience | <5 | 36 | 58.06 | 33 | 53.23 | 38 | 61.29 | 41 | 66.13 |
| 5–10 | 56 | 62.92 | 50 | 56.18 | 57 | 64.04 | 53 | 59.55 | |
| >10 | 110 | 57.29 | 90 | 46.88 | 105 | 54.69 | 109 | 56.77 | |
| p value | 0.655 | 0.278 | 0.26 | 0.375 | |||||
| Characteristics | No Discrimination | No Stigmatization | Respect for Cultural Diversity and Pluralism | Solidarity and Cooperation | Social Responsibility | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | ||
| Sex | M | 72 | 55.4 | 71 | 54.6 | 74 | 56.9 | 60 | 46.2 | 73 | 56.2 |
| F | 149 | 58.2 | 140 | 54.7 | 142 | 55.5 | 116 | 45.3 | 138 | 53.9 | |
| p value | 0.627 | 0.979 | 0.755 | 0.849 | 0.647 | ||||||
| Age (years) | <30 | 41 | 57.8 | 38 | 53.5 | 40 | 56.3 | 35 | 49.3 | 42 | 59.2 |
| 30–39 | 87 | 62.1 | 81 | 57.9 | 79 | 56.4 | 65 | 46.4 | 77 | 55 | |
| 39–49 | 60 | 57.7 | 61 | 58.7 | 63 | 60.6 | 51 | 49 | 57 | 54.8 | |
| >49 | 34 | 47.2 | 32 | 44.4 | 35 | 48.6 | 26 | 36.1 | 36 | 50 | |
| p value | 0.207 | 0.26 | 0.503 | 0.29 | 0.641 | ||||||
| Married | Yes | 165 | 56.7 | 158 | 54.3 | 162 | 55.7 | 127 | 43.6 | 154 | 52.9 |
| No | 53 | 56.4 | 51 | 54.3 | 53 | 56.4 | 47 | 50 | 56 | 59.6 | |
| p value | 0.786 | 0.832 | 0.749 | 0.349 | 0.438 | ||||||
| Nationality | Saudi | 124 | 58.2 | 120 | 56.3 | 124 | 58.2 | 104 | 48.8 | 125 | 58.7 |
| Others | 95 | 56.6 | 91 | 54.2 | 92 | 54.8 | 72 | 42.9 | 85 | 50.6 | |
| p value | 0.744 | 0.672 | 0.499 | 0.246 | 0.115 | ||||||
| Workplace | Tertiary govern. hospital | 148 | 59.9 | 142 | 57.5 | 146 | 59.1 | 119 | 48.2 | 141 | 57.1 |
| Private hospital | 34 | 61.8 | 33 | 60 | 31 | 56.4 | 23 | 41.8 | 30 | 54.6 | |
| Govern. healthcare center | 21 | 40.4 | 19 | 36.5 | 19 | 36.5 | 16 | 30.8 | 21 | 40.4 | |
| p value | 0.014 * | 0.007 * | 0.006 * | 0.032 * | 0.024 * | ||||||
| Bioethics education | Yes | 143 | 58.6 | 137 | 56.2 | 138 | 56.6 | 114 | 46.7 | 131 | 53.7 |
| No | 46 | 59 | 45 | 57.7 | 46 | 59 | 36 | 46.2 | 48 | 61.5 | |
| p value | 0.976 | 0.954 | 0.909 | 0.908 | 0.551 | ||||||
| Years of experience | <5 | 38 | 61.3 | 36 | 58.1 | 34 | 54.8 | 27 | 43.6 | 33 | 53.2 |
| 5–10 | 52 | 58.4 | 49 | 55.1 | 50 | 56.2 | 41 | 46.1 | 48 | 53.9 | |
| >10 | 108 | 56.3 | 104 | 54.2 | 106 | 55.2 | 84 | 43.8 | 104 | 54.2 | |
| p value | 0.702 | 0.807 | 0.982 | 0.917 | 0.971 | ||||||
| Characteristics | Sharing of Benefits | Protecting Future Generations | Protection of the Environment | Respecting Privacy of People | Respecting Confidentiality | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | ||
| Sex | M | 76 | 58.5 | 72 | 55.4 | 71 | 54.6 | 82 | 63.1 | 80 | 61.5 |
| F | 140 | 54.7 | 120 | 46.9 | 123 | 48.1 | 157 | 61.3 | 152 | 59.4 | |
| p value | 0.456 | 0.106 | 0.209 | 0.704 | 0.65 | ||||||
| Age (years) | <30 | 42 | 59.2 | 35 | 49.3 | 40 | 56.3 | 46 | 64.8 | 46 | 64.8 |
| 30–39 | 80 | 57.1 | 72 | 51.4 | 69 | 49.3 | 91 | 65 | 86 | 61.4 | |
| 39–49 | 58 | 55.8 | 53 | 51 | 55 | 52.9 | 65 | 62.5 | 61 | 58.7 | |
| >49 | 37 | 51.4 | 33 | 45.8 | 31 | 43.1 | 38 | 52.8 | 40 | 55.6 | |
| p value | 0.691 | 0.832 | 0.367 | 0.286 | 0.575 | ||||||
| Married | Yes | 160 | 55 | 140 | 48.1 | 140 | 48.1 | 176 | 60.5 | 171 | 58.8 |
| No | 55 | 58.5 | 51 | 54.3 | 53 | 56.4 | 60 | 63.8 | 58 | 61.7 | |
| p value | 0.763 | 0.417 | 0.325 | 0.752 | 0.74 | ||||||
| Nationality | Saudi | 130 | 61 | 113 | 53.1 | 112 | 52.6 | 144 | 67.6 | 136 | 63.9 |
| Others | 85 | 50.6 | 79 | 47 | 82 | 48.8 | 94 | 56 | 96 | 57.1 | |
| p value | 0.041 * | 0.243 | 0.465 | 0.02 * | 0.183 | ||||||
| Workplace | Tertiary govern. hospital | 143 | 57.9 | 128 | 51.8 | 131 | 53 | 160 | 64.8 | 154 | 62.4 |
| Private hospital | 31 | 56.4 | 26 | 47.3 | 26 | 47.3 | 36 | 65.5 | 35 | 63.6 | |
| Govern. healthcare center | 23 | 44.2 | 20 | 38.5 | 19 | 36.5 | 24 | 46.2 | 25 | 48.1 | |
| p value | 0.045 * | 0.126 | 0.012 * | 0.007 * | 0.048 * | ||||||
| Bioethics education | Yes | 137 | 56.2 | 121 | 49.6 | 121 | 49.6 | 152 | 62.3 | 146 | 59.8 |
| No | 47 | 60.3 | 42 | 53.9 | 42 | 53.9 | 51 | 65.4 | 51 | 65.4 | |
| p value | 0.806 | 0.717 | 0.47 | 0.929 | 0.77 | ||||||
| Years of experience | < 5 | 35 | 56.5 | 28 | 45.2 | 31 | 50 | 39 | 62.9 | 40 | 64.5 |
| 5–10 | 48 | 53.9 | 45 | 50.6 | 45 | 50.6 | 56 | 62.9 | 54 | 60.7 | |
| >10 | 107 | 55.7 | 95 | 49.5 | 93 | 48.4 | 117 | 60.9 | 113 | 58.9 | |
| p value | 0.949 | 0.768 | 0.892 | 0.879 | 0.66 | ||||||
| Characteristics | Attitude towards Ethical Issues in OB/GYN | Satisfaction towards Ethical Issues in OB/GYN | Attitude towards Ethical Principles in OB/GYN | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | p | Mean | SD | p | Mean | SD | p | ||
| Gender | Male | 56 | 36.7 | 0.367 | 43.7 | 32.7 | 0.001 * | 58.2 | 27.6 | 0.612 |
| Female | 59.4 | 31.8 | 29.3 | 31.6 | 56.7 | 27 | ||||
| Age | <30 | 51.1 | 36.4 | 0.191 | 18.6 | 24.7 | 0.001 * | 59.2 | 26.2 | 0.171 |
| 30–39 | 59.6 | 31.7 | 29.7 | 29.7 | 59.2 | 27.1 | ||||
| 40–49 | 61.9 | 32.3 | 41.2 | 35 | 58 | 27.9 | ||||
| ≥50 | 57.6 | 34.6 | 48.6 | 33.7 | 51 | 26.9 | ||||
| Marital status | Married | 57.7 | 33.2 | 0.053 | 39.5 | 32.9 | 0.001 * | 56.3 | 27 | 0.476 |
| Not married | 59.4 | 33.7 | 17.2 | 24.8 | 59.2 | 28.1 | ||||
| Current workplace | Tertiary govern. hospital | 64.8 | 28.1 | 0.002 * | 33.5 | 33.3 | 0.001 * | 58.8 | 26.6 | 0.007 * |
| Private hospital | 71.3 | 27.5 | 49.5 | 35 | 58.5 | 27.8 | ||||
| Govern. healthcare center | 52.3 | 33.2 | 31.2 | 30 | 48.5 | 26.7 | ||||
| Nationality | Saudi | 58.6 | 33.1 | 0.984 | 30.4 | 31.4 | 0.009 * | 59.2 | 27.1 | 0.203 |
| Non-Saudi | 58.6 | 33.7 | 39.2 | 33.6 | 55.6 | 27.3 | ||||
| Bioethics education | Yes | 71.3 | 21.8 | 0.001 * | 37.6 | 35.3 | 0.861 | 58.4 | 27.6 | 0.696 |
| No | 63.7 | 23.6 | 34.1 | 34.1 | 57.4 | 26 | ||||
| Experience | <5 | 52.9 | 29.8 | 0.001 * | 22.9 | 30.5 | 0.001 * | 58 | 27 | 0.798 |
| 5–10 | 64.5 | 27.8 | 27 | 29.9 | 58.7 | 27.2 | ||||
| >10 | 68.7 | 28 | 44.1 | 34.9 | 56.5 | 27.3 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alahmad, G.; Althagafi, N.A. Attitudes toward Medical Ethics among Obstetricians and Gynecologists in Saudi Arabia: An Exploratory Survey. Healthcare 2023, 11, 1394. https://doi.org/10.3390/healthcare11101394
Alahmad G, Althagafi NA. Attitudes toward Medical Ethics among Obstetricians and Gynecologists in Saudi Arabia: An Exploratory Survey. Healthcare. 2023; 11(10):1394. https://doi.org/10.3390/healthcare11101394
Chicago/Turabian StyleAlahmad, Ghiath, and Nuha Abed Althagafi. 2023. "Attitudes toward Medical Ethics among Obstetricians and Gynecologists in Saudi Arabia: An Exploratory Survey" Healthcare 11, no. 10: 1394. https://doi.org/10.3390/healthcare11101394