

Readmission of Patients to Acute Psychiatric Hospitals: Influential Factors and Interventions to Reduce Psychiatric Readmission Rates

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Stage 1: Developing the Research Question
2.2. Stage 2: Identifying the Relevant Studies
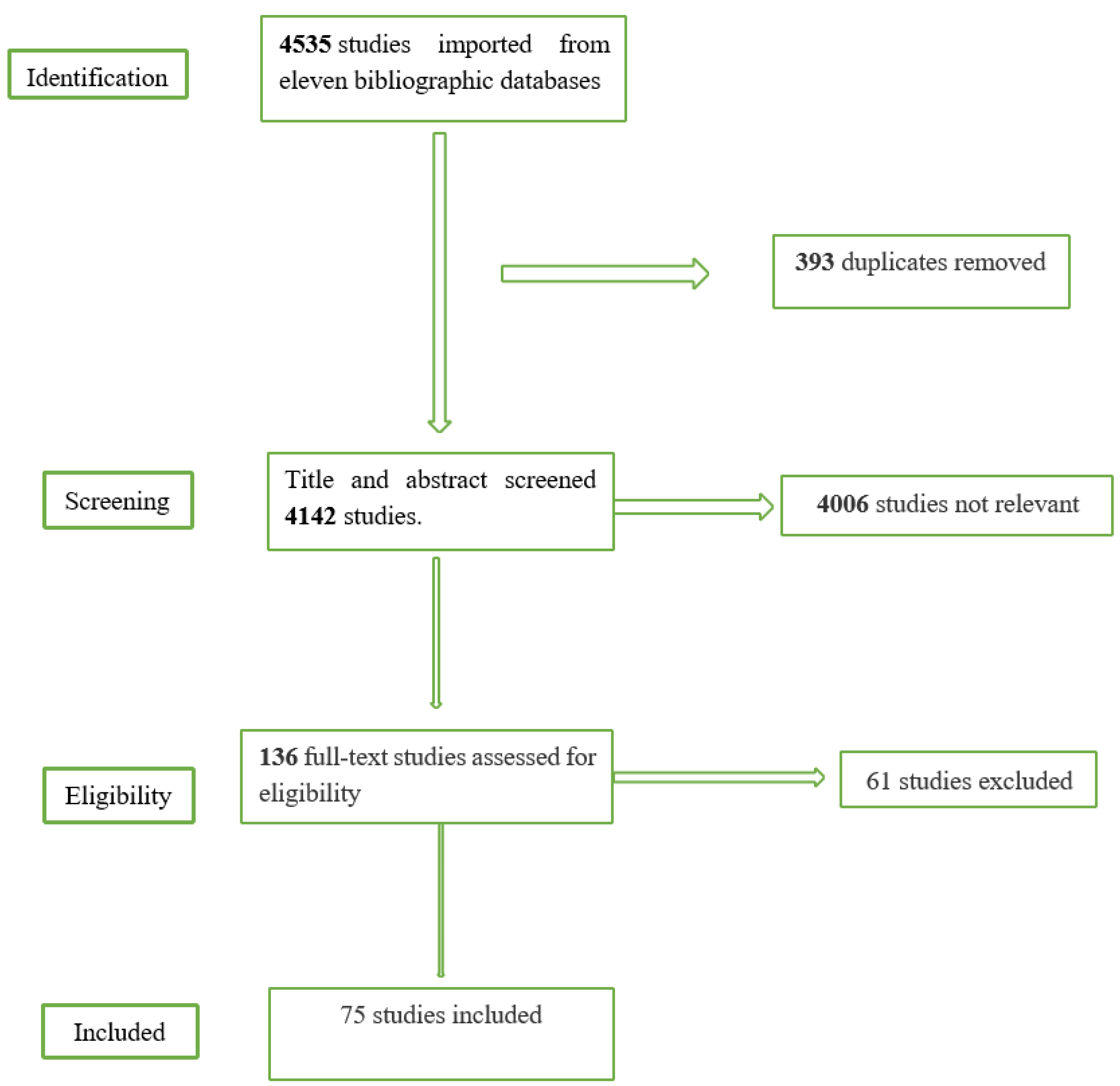
2.3. Stage 3: Article Selection
2.4. Stage 4: Data Charting and Data Extraction
2.5. Stage 5: Collating, Summarizing, and Reporting the Results
3. Result
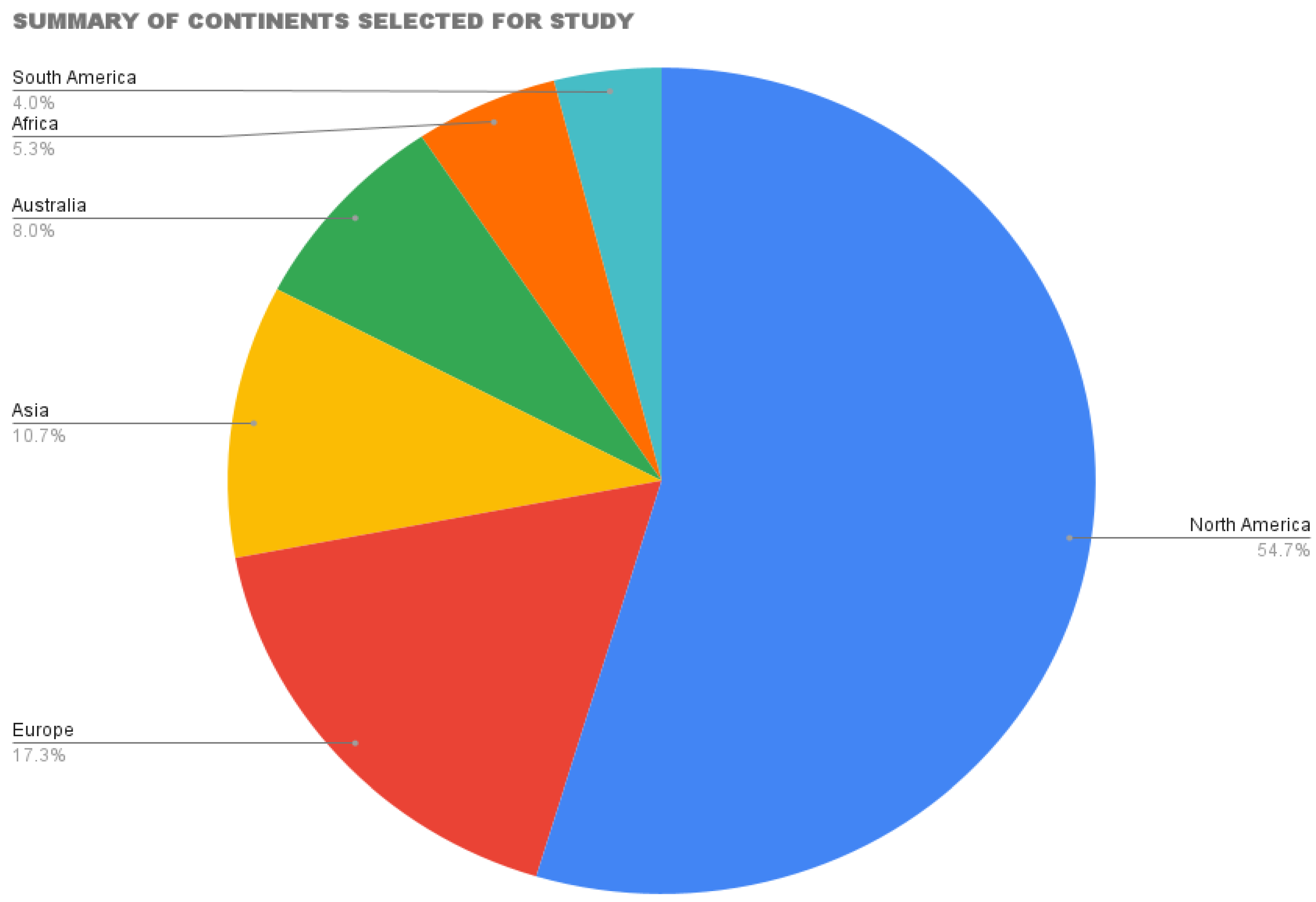
3.1. Characteristics of the Studies Included
3.2. Influential Factors for the Readmission of Psychiatric Patients
3.2.1. Length of Hospitalization for First Admitted Psychiatric Patients
3.2.2. Patients with a Previous Diagnosis of Chronic Psychiatric Disorders
3.2.3. Presence of Learning Disability, Developmental Delay, and Personality Disorder
3.3. Alcohol, Drugs, and Substance Abuse
3.4. Non-Medication Adherence
3.5. Suicidal Ideation
3.6. Interventions to Reduce Psychiatric Patients’ Readmission Rates
3.6.1. Residential Treatment Services
3.6.2. Rendering Sufficient Inpatient Care
3.6.3. Adequate Discharge Plan
3.6.4. Strengthen Focus on Staff Training
3.6.5. Focus on Care Coordination and Transitional Efforts
3.6.6. Promoting Psychological Support
3.6.7. Adherence to Medication
4. Discussion
5. Limitations
6. Conclusions, Implications for Policy and Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pow, J.L.; Baumeister, A.A.; Hawkins, M.F.; Cohen, A.S.; Garand, J.C. Deinstitutionalization of American public hospitals for the mentally ill before and after the introduction of antipsychotic medications. Harv. Rev. Psychiatry 2015, 23, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.E.; Donzé, J.; Schnipper, J.L. Contribution of psychiatric illness and substance abuse to 30-day readmission risk. J. Hosp. Med. 2013, 8, 450–455. [Google Scholar] [CrossRef]
- Montgomery, P.; Kirkpatrick, H. Understanding those who seek frequent psychiatric hospitalizations. Arch. Psychiatr. Nurs. 2002, 16, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Arnold, E.M.; Goldston, D.B.; Ruggiero, A.; Reboussin, B.A.; Daniel, S.S.; Hickman, E.A. Rates and predictors of rehospitalization among formerly hospitalized adolescents. Psychiatr. Serv. 2003, 54, 994–998. [Google Scholar] [CrossRef] [PubMed]
- Barekatain, M.; Maracy, M.R.; Hassannejad, R.; Hosseini, R. Factors associated with readmission of patients at a university hospital psychiatric ward in Iran. Psychiatry J. 2013, 2013, 685625. [Google Scholar] [CrossRef]
- Rosca, P.; Bauer, A.; Grinshpoon, A.; Khawaled, R.; Mester, R.; Ponizovsky, A.M. Rehospitalizations among psychiatric patients whose first admission was involuntary: A 10-year follow-up. Isr. J. Psychiatry Relat. Sci. 2006, 43, 57. [Google Scholar]
- Fisher, S.; Stevens, R.F. Subgroups of frequent users of an inpatient mental health program at a community hospital in Canada. Psychiatr. Serv. 1999, 50, 244–247. [Google Scholar] [CrossRef]
- Burke, R.E.; Whitfield, E.A.; Hittle, D.; Min, S.J.; Levy, C.; Prochazka, A.V.; Coleman, E.A.; Schwartz, R.; Ginde, A.A. Hospital readmission from post-acute care facilities: Risk factors, timing, and outcomes. J. Am. Med. Dir. Assoc. 2016, 17, 249–255. [Google Scholar] [CrossRef]
- Goldstein, A.B.; Frosch, E.; Davarya, S.; Leaf, P.J. Factors associated with a six-month return to emergency services among child and adolescent psychiatric patients. Psychiatr. Serv. 2007, 58, 1489–1492. [Google Scholar] [CrossRef]
- Bobo, W.V.; Hoge, C.W.; Messina, M.A.; Pavlovcic, F.; Levandowski, D.; Grieger, T. Characteristics of repeat users of an inpatient psychiatry service at a large military tertiary care hospital. Mil. Med. 2004, 169, 648–653. [Google Scholar] [CrossRef]
- Rothbard, A.B.; Kuno, E.; Schinnar, A.P.; Hadley, T.R.; Turk, R. Service utilization and cost of community care for discharged state hospital patients: A 3-year follow-up study. Am. J. Psychiatry 1999, 156, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Durbin, J.; Lin, E.; Layne, C.; Teed, M. Is readmission a valid indicator of the quality of inpatient psychiatric care? J. Behav. Health Serv. Res. 2007, 34, 137–150. [Google Scholar] [CrossRef]
- Rumball-Smith, J.; Hider, P. The validity of readmission rate as a marker of the quality of hospital care, and a recommendation for its definition. N. Z. Med. J. 2009, 122, 63–70. [Google Scholar]
- Lana, F.; Martin, M.; Vinue, J. Variability in psychiatric medical practice evaluated by studying short-term psychiatric rehospitalization. Actas Esp. Psiquiatr. 2004, 32, 340. [Google Scholar]
- Roick, C.; Heider, D.; Kilian, R.; Matschinger, H.; Toumi, M.; Angermeyer, M.C. Factors contributing to frequent use of psychiatric inpatient services by schizophrenia patients. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.E.; Neighbors, H.W.; Munday, C.; Trierweiler, S. Length of stay, referral to aftercare, and rehospitalization among psychiatric inpatients. Psychiatr. Serv. 2003, 55, 1271–1276. [Google Scholar] [CrossRef]
- Niehaus, D.J.; Koen, L.; Galal, U.; Dhansay, K.; Oosthuizen, P.P.; Emsley, R.A.; Jordaan, E. Crisis discharges and readmission risk in acute psychiatric male inpatients. BMC Psychiatry 2008, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Yussuf, A.D.; Kuranga, S.A.; Balogun, O.R.; Ajiboyed, P.O.; Issa, B.A.; Adegunloye, O. Predictors of psychiatric readmissions to the psychiatric unit of a tertiary health facility in a Nigerian city-a 5-year study. Afr. J. Psychiatry 2008, 11, 187–190. [Google Scholar] [CrossRef]
- Haywood, T.W.; Kravitz, H.M.; Grossman, L.S.; Cavanaugh, J.L.; Davis, J.M.; Lewis, D.A. Predicting the “revolving door” phenomenon among patients with schizophrenic, schizoaffective, and affective disorders. Am. J. Psychiatry 1995, 152, 856–861. [Google Scholar] [PubMed]
- Romansky, J.B.; Lyons, J.S.; Lehner, R.K.; West, C.M. Factors related to psychiatric hospital readmission among children and adolescents in state custody. Psychiatr. Serv. 2003, 54, 356–362. [Google Scholar] [CrossRef]
- Bobier, C.; Bobier, C.; Warwick, M. Factors associated with readmission to adolescent psychiatric care. Aust. N. Z. J. Psychiatry 2005, 39, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Fontanella, C.A. The influence of clinical, treatment, and healthcare system characteristics on psychiatric readmission of adolescents. Am. J. Orthopsychiatry 2008, 78, 187–198. [Google Scholar] [CrossRef]
- Cheng, C.; Chan, C.W.; Gula, C.A.; Parker, M.D. Effects of outpatient aftercare on psychiatric rehospitalization among children and emerging adults in Alberta, Canada. Psychiatr. Serv. 2017, 68, 696–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Elhassan, N.M.; Elhusein, B.; Al Abdulla, M.; Saad, T.A.; Kumar, R. Sociodemographic and clinical characteristics of patients with recurrent psychiatric readmissions in Qatar. J. Int. Med. Res. 2020, 48, 0300060520977382. [Google Scholar] [CrossRef]
- Maestri, T.J.; Mican, L.M.; Rozea, H.; Barner, J.C. Do long-acting injectable antipsychotics prevent or delay hospital readmission? Psychopharmacol. Bull. 2018, 48, 8. [Google Scholar]
- Barros, R.E.M.; de Azevedo Marques, J.M.; Santos, J.L.F.; Zuardi, A.W.; Del-Ben, C.M. Impact of length of stay for first psychiatric admissions on the ratio of readmissions in subsequent years in a large Brazilian catchment area. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.P.; Favarato, G.; Lamb, D.; Harper, T.; Johnson, S.; Lloyd-Evans, B.; Marston, L.; Pinfold, V.; Smith, D.; Kirkbride, J.B.; et al. Readmission after discharge from acute mental healthcare among 231,988 people in England: Cohort study exploring predictors of readmission including availability of acute day units in local areas. BJPsych Open 2021, 7, e136. [Google Scholar] [CrossRef]
- Tedeschi, F.; Donisi, V.; Salazzari, D.; Cresswell-Smith, J.; Wahlbeck, K.; Amaddeo, F. Clinical and organizational factors predicting readmission for mental health patients across Italy. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 187–196. [Google Scholar] [CrossRef]
- Serrani, D.; Galfetti, G.; Rodríguez, C. Factors associated with length of stay and the risk of readmission in an acute psychiatric inpatient facility: A retrospective study. Vertex (Buenos Aires Argent.) 2017, 28, 260–270. [Google Scholar]
- Trask, E.V.; Fawley-King, K.; Garland, A.F.; Aarons, G.A. Do aftercare mental health services reduce risk of psychiatric rehospitalization for children? Psychol. Serv. 2016, 13, 127. [Google Scholar] [CrossRef]
- Munley, P.H.; Hyer, L.A. Demographic and clinical characteristics as predictors of readmission: A one-year follow-up. J. Clin. Psychol. 1978, 34, 833–838. [Google Scholar] [CrossRef]
- Joyce, P.R. Changing trends in first admissions and readmissions for mania and schizophrenia in New Zealand, 1974 to 1984. Aust. N. Z. J. Psychiatry 1987, 21, 82–86. [Google Scholar] [CrossRef] [PubMed]
- MacEwan, J.P.; Kamat, S.A.; Duffy, R.A.; Seabury, S.; Chou, J.W.; Legacy, S.N.; Hartry, A.; Eramo, A.; Karson, C. Hospital readmission rates among patients with schizophrenia treated with long-acting injectables or oral antipsychotics. Psychiatr. Serv. 2016, 67, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- La Vonne, A.D.; Zun, L.S. Reasons for readmissions: What are the reasons for 90-day readmissions of psychiatric patients from the ED? Am. J. Emerg. Med. 2015, 33, 1489–1491. [Google Scholar]
- Guzman-Parra, J.; Moreno-Küstner, B.; Rivas, F.; Alba-Vallejo, M.; Hernandez-Pedrosa, J.; Mayoral-Cleries, F. Needs, perceived support, and hospital readmissions in patients with severe mental illness. Community Ment. Health J. 2018, 54, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.C.; Bassani, D.G.; Palazzo, L.S. A case-control study of factors associated with multiple psychiatric readmissions. Psychiatr. Serv. 2009, 60, 786–791. [Google Scholar] [CrossRef]
- Manu, P.; Khan, S.; Radhakrishnan, R.; Russ, M.J.; Kane, J.M.; Correll, C.U. Body mass index identified as an independent predictor of psychiatric readmission. J. Clin. Psychiatry 2014, 75, e573–e577. [Google Scholar] [CrossRef]
- McNeill, D.N.; Stevenson, J.; Longabaugh, R.H. Short-term inpatient care and readmission rates: The CMHC approach versus the private approach. Hosp. Community Psychiatry 1980, 31, 751–755. [Google Scholar] [CrossRef]
- Wani, R.J.; Kathe, N.J.; Klepser, D.G. Predictors of Cost and Incidence of 30-Day Readmissions Following Hospitalizations for Schizophrenia and Psychotic Disorders: A Nationwide Analysis. Qual. Manag. Health Care 2019, 28, 130–138. [Google Scholar] [CrossRef]
- Soyka, M. Alcohol-induced psychotic disorders—A diagnostic entity of its own? Nervenarzt 2014, 85, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Soyka, M.; Helten, B.; Cleves, M.; Schmidt, P. High rehospitalization rate in alcohol-induced psychotic disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.L.; Fanaian, M.; Kotze, B.; Grenyer, B.F. Mental health presentations to acute psychiatric services: 3-year study of prevalence and readmission risk for personality disorders compared with psychotic, affective, substance or other disorders. BJPsych Open 2019, 5, e1. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, R.E.; Lewis, M.; Boardman, A.P. Prediction of readmission to acute psychiatric units. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 304–309. [Google Scholar] [CrossRef]
- Behr, G.M.; Christie, C.; Soderlund, N.; Lee, T. Patterns and determinants of acute psychiatric readmissions. South Afr. J. Psychiatry 2002, 8, 71–77. [Google Scholar] [CrossRef]
- Barros, R.E.M.; Del-Ben, C.M. Rates of psychiatric readmission and public mental health policies. Rev. Bras. Psiquiatr. 2012, 34, 352–355. [Google Scholar] [CrossRef]
- Mellesdal, L.; Mehlum, L.; Wentzel-Larsen, T.; Kroken, R.; Arild Jørgensen, H. Suicide risk and acute psychiatric readmissions: A prospective cohort study. Psychiatr. Serv. 2010, 61, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Yedlapati, S.H.; Stewart, S.H. Predictors of alcohol withdrawal readmissions. Alcohol Alcohol. 2018, 53, 448–452. [Google Scholar] [CrossRef]
- Di Giovanni, P.; Di Martino, G.; Zecca, I.A.L.; Porfilio, I.; Romano, F.; Staniscia, T. The revolving door phenomenon: Psychiatric hospitalization and risk of readmission among drug-addicted patients. Clin. Ter. 2020, 171, e421–e424. [Google Scholar]
- Moos, R.H.; Pettit, B.; Gruber, V. Longer episodes of community residential care reduce substance abuse patients’ readmission rates. J. Stud. Alcohol 1995, 56, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Moos, R.H.; Mertens, J.R.; Brennan, P.L. Rates and predictors of four-year readmission among late-middle-aged and older substance abuse patients. J. Stud. Alcohol 1994, 55, 561–570. [Google Scholar] [CrossRef]
- Verdoux, H.; Lengronne, J.; Liraud, F.; Gonzales, B.; Assens, F.; Abalan, F.; Os, J.V. Medication adherence in psychosis: Predictors and impact on outcome. A 2-year follow-up of first-admitted subjects. Acta Psychiatr. Scand. 2000, 102, 203–210. [Google Scholar] [CrossRef]
- Xu, K.Y.; Rossi, K.C.; Kim, A.M.; Jetté, N.; Yoo, J.Y.; Hung, K.; Dhamoon, M.S. Risk of readmission for suicide attempt after epilepsy hospitalization. Epilepsy Behav. 2018, 83, 124–130. [Google Scholar] [CrossRef]
- Barnett, B.S.; Kusunzi, V.; Magola, L.; Borba, C.P.; Udedi, M.; Kulisewa, K.; Hosseinipour, M.C. Risk factors for readmission among a cohort of psychiatric inpatients in Lilongwe, Malawi. Int. J. Psychiatry Clin. Pract. 2020, 24, 25–30. [Google Scholar] [CrossRef]
- Czyz, E.K.; Berona, J.; King, C.A. Rehospitalization of suicidal adolescents in relation to course of suicidal ideation and future suicide attempts. Psychiatr. Serv. 2016, 67, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Lakin, B.L.; Brambila, A.D.; Sigda, K.B. Behavioral managed care and its effects in the readmission to a children’s residential treatment center. Resid. Treat. Child. Youth 2008, 24, 315–326. [Google Scholar] [CrossRef]
- Chiesa, M.; Fonagy, P.; Holmes, J.; Drahorad, C. Residential versus community treatment of personality disorders: A comparative study of three treatment programs. Am. J. Psychiatry 2004, 161, 1463–1470. [Google Scholar] [CrossRef] [Green Version]
- Reif, S.; Acevedo, A.; Garnick, D.W.; Fullerton, C.A. Reducing behavioral health inpatient readmissions for people with substance use disorders: Do follow-up services matter? Psychiatr. Serv. 2017, 68, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Csipke, E.; Rose, D.; Koeser, L.; McCrone, P.; Tulloch, A.D.; Salaminios, G.; Wykes, T.; Craig, T. Efficacy of a triage system to reduce length of hospital stay. Br. J. Psychiatry 2014, 204, 480–485. [Google Scholar] [CrossRef]
- Markley, J.; Andow, V.; Sabharwal, K.; Wang, Z.; Fennell, E.; Dusek, R. A project to reengineer discharges reduces 30-day readmission rates. AJN Am. J. Nurs. 2013, 113, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Vigod, S.N.; Kurdyak, P.A.; Dennis, C.L.; Leszcz, T.; Taylor, V.H.; Blumberger, D.M.; Seitz, D.P. Transitional interventions to reduce early psychiatric readmissions in adults: Systematic review. Br. J. Psychiatry 2013, 202, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Cloonan, P.; Wood, J.; Riley, J.B. Reducing 30-day readmissions: Health literacy strategies. JONA J. Nurs. Adm. 2013, 43, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Arendts, G.; MacKenzie, J.; Lee, J.K. Discharge planning and patient satisfaction in an emergency short-stay unit. Emerg. Med. Australas. 2006, 18, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.K.; Orav, E.J.; Epstein, A.M. Public reporting of discharge planning and rates of readmissions. N. Engl. J. Med. 2009, 361, 2637–2645. [Google Scholar] [CrossRef]
- Shaffer, S.L.; Hutchison, S.L.; Ayers, A.M.; Goldberg, R.W.; Herman, D.; Duch, D.A.; Kogan, J.N.; Terhorst, L. Brief critical time intervention to reduce psychiatric rehospitalization. Psychiatr. Serv. 2015, 66, 1155–1161. [Google Scholar] [CrossRef]
- Doering, S.; Müller, E.; Köpcke, W.; Pietzcher, A.; Gaebel, W.; Linden, M.; Müller, P.; Müller-Spahn, F.; Tegeler, J.; Schüssler, G. Predictors of relapse and rehospitalization in schizophrenia and schizoaffective disorder. Schizophr. Bull. 1998, 24, 87–98. [Google Scholar] [CrossRef]
- Vasilevskis, E.E.; Ouslander, J.G.; Mixon, A.S.; Bell, S.P.; Jacobsen, J.M.L.; Saraf, A.A.; Markley, D.; Sponsler, K.C.; Shutes, J.; Long, E.A.; et al. Potentially avoidable readmissions of patients discharged to post-acute care: Perspectives of hospital and skilled nursing facility staff. J. Am. Geriatr. Soc. 2017, 65, 269–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, L.D. Medication refusal and the rehospitalized mentally ill inmate. Hosp. Community Psychiatry 1989, 40, 491–496. [Google Scholar] [CrossRef]
- Lewis, T.; Joyce, P.R. The new revolving-door patients: Results from a national cohort of first admissions. Acta Psychiatr. Scand. 1990, 82, 130–135. [Google Scholar] [CrossRef]
- Rosen, O.Z.; Fridman, R.; Rosen, B.T.; Shane, R.; Pevnick, J.M. Medication adherence as a predictor of 30-day hospital readmissions. Patient Prefer. Adherence 2017, 11, 801. [Google Scholar] [CrossRef]
- Hochhalter, A.K.; Basu, R.; Prasla, K.; Jo, C. Retrospective cohort study of medication adherence and risk for 30-day hospital readmission in a Medicare Cost Plan. Manag. Care 2014, 23, 43–47. [Google Scholar]
- Kim, H.M.; Pfeiffer, P.; Ganoczy, D.; Valenstein, M. Intensity of outpatient monitoring after discharge and psychiatric rehospitalization of veterans with depression. Psychiatr. Serv. 2011, 62, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Zeff, K.N.; Armstrong, S.C.; Folen, R.A. Characteristics associated with psychiatric readmission. Hosp. Community Psychiatry 1990, 41, 91–93. [Google Scholar] [PubMed]
- Gunnell, D.; Hawton, K.; Ho, D.; Evans, J.; O’Connor, S.; Potokar, J.; Donovan, J.; Kapur, N. Hospital admissions for self harm after discharge from psychiatric inpatient care: Cohort study. BMJ 2008, 337, a2278. [Google Scholar] [CrossRef] [PubMed]
- Clements, K.M.; Murphy, J.M.; Eisen, S.V.; Normand, S.L.T. Comparison of self-report and clinician-rated measures of psychiatric symptoms and functioning in predicting 1-year hospital readmission. Adm. Policy Ment. Health Ment. Health Serv. Res. 2006, 33, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Madi, N.; Zhao, H.; Li, J.F. Hospital readmissions for patients with mental illness in Canada. Healthc Q 2007, 10, 30–32. [Google Scholar] [CrossRef]
- Heslin, K.C.; Weiss, A.J. Hospital Readmissions Involving Psychiatric Disorders, 2012: Statistical Brief# 189; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2015. [Google Scholar]
- Linehan, M.M.; Rizvi, S.L.; Welch, S.S.; Page, B. Psychiatric aspects of suicidal behaviour: Personality disorders. In The International Handbook of Suicide and Attempted Suicide; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2008; pp. 147–178. [Google Scholar]
- Bodén, R.; Brandt, L.; Kieler, H.; Andersen, M.; Reutfors, J. Early non-adherence to medication and other risk factors for rehospitalization in schizophrenia and schizoaffective disorder. Schizophr. Res. 2011, 133, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Steffen, S.; Koesters, M.; Becker, T.; Puschner, B. Discharge planning in mental health care: A systematic review of the recent literature. Acta Psychiatr. Scand. 2009, 120, 1–9. [Google Scholar] [CrossRef]
- Moos, R.H.; Mertens, J.R.; Brennan, P.L. Program characteristics and readmission among older substance abuse patients: Comparisons with middle-aged and younger patients. J. Ment. Health Adm. 1995, 22, 332–345. [Google Scholar] [CrossRef]
- Brennan, P.L.; Kagay, C.R.; Geppert, J.J.; Moos, R.H. Elderly Medicare inpatients with substance use disorders: Characteristics and predictors of hospital readmissions over a four-year interval. J. Stud. Alcohol 2000, 61, 891–895. [Google Scholar] [CrossRef]
- Davidson, L.; Guy, K. Peer support among persons with severe mental illnesses: A review of evidence and experience. World Psychiatry 2012, 11, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Lamb, D.; Marston, L.; Osborn, D.; Mason, O.; Henderson, C.; Ambler, G.; Milton, A.; Davidson, M.; Christoforou, M.; et al. Peer-supported self-management for people discharged from a mental health crisis team: A randomised controlled trial. Lancet 2018, 392, 409–418. [Google Scholar] [CrossRef]
- Agyapong, V.I.; Hrabok, M.; Shalaby, R.; Vuong, W.; Noble, J.M.; Gusnowski, A.; Mrklas, K.; Li, D.; Urichuck, L.; Snaterse, M.; et al. Text4Hope: Receiving daily supportive text messages for 3 months during the COVID-19 pandemic reduces stress, anxiety, and depression. Disaster Med. Public Health Prep. 2021, 16, 1326–1330. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.; Mrklas, K.; Juhás, M.; Omeje, J.; Ohinmaa, A.; Dursun, S.M. Cross-sectional survey evaluating Text4Mood: Mobile health program to reduce psychological treatment gap in mental healthcare in Alberta through daily supportive text messages. BMC Psychiatry 2016, 16, 378. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Mrklas, K.; Suen, V.Y.M.; Rose, M.S.; Jahn, M.; Gladue, I.; Kozak, J.; Leslie, M.; Dursun, S.; Ohinmaa, A.; et al. Supportive text messages to reduce mood symptoms and problem drinking in patients with primary depression or alcohol use disorder: Protocol for an implementation research study. JMIR Res. Protoc. 2015, 4, e4371. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Hrabok, M.; Shalaby, R.; Mrklas, K.; Vuong, W.; Gusnowski, A.; Surood, S.; Greenshaw, A.J.; Nkire, N. Closing the COVID-19 psychological treatment gap for cancer patients in Alberta: Protocol for the implementation and evaluation of Text4Hope-Cancer Care. JMIR Res. Protoc. 2020, 9, e20240. [Google Scholar] [CrossRef]
- IO Agyapong, V.; Farren, C.K.; McLoughlin, D.M. Mobile phone text message interventions in psychiatry-what are the possibilities? Curr. Psychiatry Rev. 2011, 7, 50–56. [Google Scholar] [CrossRef]
- Agyapong, V.I.; Juhás, M.; Mrklas, K.; Hrabok, M.; Omeje, J.; Gladue, I.; Kozak, J.; Leslie, M.; Chue, P.; Greenshaw, A.J. Randomized controlled pilot trial of supportive text messaging for alcohol use disorder patients. J. Subst. Abus. Treat. 2018, 94, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Hrabok, M.; Vuong, W.; Gusnowski, A.; Shalaby, R.; Mrklas, K.; Li, D.; Urichuk, L.; Snaterse, M.; Surood, S.; et al. Closing the psychological treatment gap during the COVID-19 pandemic with a supportive text messaging program: Protocol for implementation and evaluation. JMIR Res. Protoc. 2020, 9, e19292. [Google Scholar] [CrossRef]
- Agyapong, V.I.; Shalaby, R.; Hrabok, M.; Vuong, W.; Noble, J.M.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; et al. Mental health outreach via supportive text messages during the COVID-19 pandemic: Improved mental health and reduced suicidal ideation after six weeks in subscribers of Text4Hope compared to a control population. Int. J. Environ. Res. Public Health 2021, 18, 2157. [Google Scholar] [CrossRef]
- Eboreime, E.; Shalaby, R.; Mao, W.; Owusu, E.; Vuong, W.; Surood, S.; Agyapong, V.I.O. Reducing readmission rates for individuals discharged from acute psychiatric care in Alberta using peer and text message support: Protocol for an innovative supportive program. BMC Health Serv. Res. 2022, 22, 332. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors | Country | Study Type | Sample Size | Age Range | Medical Conditions | Study Findings |
|---|---|---|---|---|---|---|
| Albrecht et al., 2012 | USA | Retrospective cohort study | 26,878 | 58 years | Severe mental illness/diabetes | No significant association between Serious mental illness (SMI) and 30-day hospital readmission was found in any group. |
| Bach et al., 2002 | USA | Retrospective comparative study | 35 | 39.2 years | Schizophrenia, depression, and bipolar disorder | Four sessions of an individual acceptance intervention reduced the rate of hospitalization over four months by 50% in a chronic group of hospitalized patients experiencing positive symptoms of psychosis. |
| Bardach et al., 2020 | USA | Chart review | 22,844 | 6–17 years | Depression, bipolar disorder, psychosis, and anxiety | The readmission rates were 62% for 7-day, and 82.3% for 30-days. Acute care readmission rates were 22.4% within 30 days and 54.8% within six months. |
| Barker et al., 2018 | Canada | Retrospective chart review | 65,789 | 46 years | Psychiatric diagnosis | The 30-day readmission rates were 9.3% and 9.1% for women and men, respectively. Predictors were personality disorders and positive symptoms for women and self-care problems at admission and discharge and mild anxiety for men. |
| Barnett et al., 2020 | Malawi | Retrospective chart review | 419 | 10–74 years | All patients on admission | Ten percent were readmitted at least once during the study period. The predictor was the intentional medication non-adherence at home. |
| Batalla et al., 2013 | Spain | Retrospective chart review | 58 | 18–29 | Substance use disorder | Cocaine and cannabis use disorders were predictors for readmission. |
| Behr et al., 2002 | South Africa | Retrospective cohort study (analytical and descriptive) | 180 | 21–50 years | All psychiatric diagnoses | The rate of readmission within the 90 days post-discharge was 21%. Being married or co-habiting was found to be a protective factor for readmission. |
| Boag et al., 2021 | USA | Retrospective cohort design | 5076 | 45.2 years | Psychiatric diagnosis | The 180 days readmission rate was 23%. Prediction models incorporating topics derived from Latent Dirichlet Allocation in addition to simpler bag-of-words features performed comparably to, or better than, the models relying solely on bag-of-words or coded data. |
| Botha et al., 2018 | South Africa | Randomized, non-blinded clinical trial | 100 | 18–59 years | Schizoaffective disorder or bipolar disorder | The rate of readmissions over the 12 months was 34%. Participants in the facilitated care group (FCG) appeared to be more likely to have more than one readmission (18%) compared to the treatment as usual group (TUG) participants (7%). |
| Callaly et al., 2010 | Australia | Retrospective cross-sectional study | 115 | Adult | All psychiatric conditions | Predictors for readmission were being admitted in the previous year, receiving the Disability Support Pension, not having a discharge plan and being unemployed. The rates for readmission were 45% within seven days, 68% within 14 days and 91% within 21 days. |
| Carlisle et al., 2012 | Canada | Population-based cohort analysis | 4472 | 16.9 years | Psychiatric diagnosis | No aftercare in the month post-discharge increased the risk of readmission but not emergency department visits. |
| Cheng et al., 2017 | Canada | Retrospective analysis | 15,628 | 5–24 years | Psychiatric conditions | Fourteen percent (14%) were readmitted within 90 days. Readmission predictions were prior service use, more extended hospital stays, higher income, specific diagnoses, female sex, and comorbid mental health conditions. Aftercare reduced the risk of readmission by 32%. |
| Conley et al., 1999 | USA | Retrospective cross-sectional study | 2024 | 41.6 years | Schizophrenia and other mental conditions | The predictor for readmission was schizophrenia. The readmission rate for risperidone-treated patients appeared to be steady up to 24 months. At 24 months, 87% of the clozapine-treated patients and 66% of the risperidone-treated patients remained in the community. |
| Czyz et al., 2016 | USA | Prospective cross-sectional study | 373 | 13–17 years | Substance use disorder with risk of suicide | The 90 days readmission rate was 21%. Youths with a history of multiple suicide attempts were the predictors. |
| Di Giovanni et al., 2020 | Italy | Retrospective observational study | 325 | 36.5 years | Drug addiction | Overall, 80.8% of readmissions occurred during the first year and 88.2% during the first two years. The critical predictor was drug-addicted patients. |
| Doering et al., 1998 | Germany | Retrospective chart review | 354 | 18–55 years | Schizophrenia and schizoaffective disorder | Readmission predictors were neuroleptic treatment, onset and previous course, psychopathology, social adjustment (marital status, employment, intensity of life), previous life experiences and biology (gender, age). |
| Downey et al., 2015 | USA | Retrospective chart review | 350 | 30–49 years | Depression, schizophrenia, schizoaffective disorder, bipolar disorder, and psychosis | The predictors for readmission were depression, schizophrenia, schizoaffective disorder, bipolar disorder, and psychosis. |
| Guzman-Parra et al., 2018 | USA | Longitudinal observational study | 780 | 18–78 years | Psychiatric conditions | The rate of readmission within one year was 36.28%. The overall rates of readmissions within 30, 90 days, and one year after discharge were 21.21, 40.40, and 61.61%, respectively. Predictors were previous readmissions and informal help for psychological distress. |
| Haddad et al., 2020 | Lebanon | Retrospective observational study | 158 | 43.7 years | Acute mania | Predictors for readmission were male gender, taking anticholinergic drugs, and having a family history of psychiatric disorders. |
| Hamilton et al., 2015 | USA | Retrospective chart review | 588 | 18–71 years | Schizophrenia, bipolar, and depression | Lack of engagement in post-discharge aftercare services was a key predictor for readmission. |
| Hodgson et al., 2001 | UK | Retrospective chart review | 3404 | 16–64 years | Psychiatric disorders | Predictors for readmission were being unmarried and having a psychosis diagnosis. The readmission rate was 49% for patients with affective disorders, 42% for schizophrenia, and 39% for personality disorders. |
| Hung et al., 2017 | Taiwan | Retrospective chart review study | 138 | 38.73 years | Schizophrenia and schizoaffective disorder | The one-year and 3-months readmission rates were 33.3% and 15.2%, respectively. Predictors were an unmarried status, previous history of involuntary admission, longer involuntary admission days, and shorter total admission days. |
| Joanna et al., 2016 | USA | Retrospective cohort analysis | 1450 | 18–64 years | Schizophrenia | The rate of readmission within the 60-day post-discharge period was 25%. Long-acting injections (LAIs) were found to significantly reduce the risk of readmission by 16% compared to oral antipsychotics. |
| John et al., 1997 | USA | Observational study | 255 | 30.8 years | Psychiatric conditions | Predictors for readmission were patients with more significant impairment in self-care, more severe symptoms, and more persistent illnesses. |
| Joyce et al., 2019 | USA | Retrospective cross-sectional study | 783 | 12–17 years | Psychiatric conditions | The readmission rate was 26% at two years post-discharge, 22% at one year, 18% at 180 days, 12% at 90 days, and 6% at 30 days. Predicting factors were a diagnosis of PTSD, severe lifetime SI, and lack of treatment alliance. |
| Lee et al., 2017 | Malaysia | Observational study | 149 | 37.8 years | Psychotic disorder, bipolar disorder, major depression disorder, mental sub-normality and substance abuse | Patients were readmitted within three months of their last discharge. Predictors were male, single, unemployed, taken care of by family, and achieved secondary education level with a mean age of 37.89 years. |
| Lewis et al., 2019 | Australia | Comparative study | 2833 | 42.08 years | Personality disorder | Readmission was within 28 days after discharge. Predictors were a personality disorder diagnosis and psychotic disorders. |
| Lorine et al., 2015 | USA | Retrospective chart review | 207 | 18–65+ years | Schizophrenia, MDD, seasonal affective disorder (SAD), and psychosis | Risk factors for readmission within 15 days were diagnosis of schizophrenia and or seasonal affective disorder (SAD). |
| Maali et al., 2018 | Australia | Case study | 62,255 | 16–75 years | Psychiatric and medical diagnosis | Predictors for readmission were the previous history of healthcare utilization, the urgency of the index admission, old age, comorbidities related to cancer, psychosis, drug abuse, abnormal pathology results at discharge, and being unmarried and a public patient. |
| Manu et al., 2014 | USA | Cohort | 945 | 41.5 years | Schizophrenia spectrum disorders, bipolar disorder, and depressive disorder. | The one year readmission rate was 24%. Higher BMI, diagnosis of schizophrenia and schizoaffective disorder, shorter length of stay, and treatment with clozapine were key predictors of readmission. |
| Maples et al., 2012 | USA | Observational study | 345 | 36.3 years | Schizophrenia, bipolar, and depression | The use of hospital and crisis or emergency services reduced significantly within the 30 days of discharge. |
| Marcus et al., 2017 | USA | Retrospective longitudinal cohort analyses | 71,776 | 18–64 years | Schizophrenia and bipolar disorder | Outpatient visits 30 days after discharge were associated with a lower hospital readmission risk during the following 90 days. Assertive hospital discharge planning to secure outpatient visits after hospital discharge is needed for these patient populations. |
| Mark et al., 2013 | USA | Retrospective cross-sectional study | 121,275 | 18–65 years | Substance use disorder | The annual readmission rate was 11%. The hospital-level factors that reduced readmission rates were patients with follow-up at a community mental health center (CMHC), and longer lengths of stay. Prior to the inpatient stay, psychotic illness, substance use disorders, and medical comorbidities were predicted. |
| Mellesdal et al., 2010 | Norway | Prospective cohort study | 1245 | 41.6 | Psychiatric diagnosis | Fifty-four percent (54%) of the index admissions and 62% of the readmissions were related to suicide risk. Other predictors were substance use disorders, personality disorders, prior psychiatric hospitalization, unemployment, and receipt of social benefits. |
| Mgutshini et al., 2010 | USA | An explorative study | 59 | 18–74 years | Psychiatric diagnosis | The predictor of readmission was non-adherence with prescribed medication. |
| Miller et al., 2020 | Canada | Retrospective cross-section study | 3825 | 3–19 years | All psychiatric conditions | The rate of readmission within 90 days following discharge was 57.3%. Predictors were older age, being male, higher socioeconomic status (SES), referral to care by a medical practitioner, discharge to another health facility, psychosis, and previous psychiatric admission. |
| Moos et al., 1994 | USA | Cross-sectional Study | 85 | 56 | Substance abuse | Predictors of readmission were being married, diagnoses of alcoholic psychosis and treatment in the index episode, and discharge against medical advice (AMA). |
| Moos et al., 1998 | USA | Retrospective chart review and file analysis | 16,066 | 61.3 years | Substance abuse | Four-year readmission rates ranged from 57% to 70%. Predictors for readmission were younger age, unmarried status, more prior service use, alcohol psychosis or psychiatric diagnoses, treatment in a psychiatric unit, and shorter hospital stay. |
| Munley et al., 1978 | USA | Retrospective cohort study | 202 | 39.8 years | Substance abuse | Predictors for readmission were the number of prior psychiatric hospitalizations and diagnosis of depression upon admission. |
| Nagata et al., 2019 | Japan | Retrospective chart review | 526 | 48 years | Substance abuse | Following discharge, the cumulative admission rate to local psychiatric hospitals was 21.8% after six months and 37.6% after one year. Predicting factor was patients who had been discharged from their Medical Treatment and Supervision Act [MTSA] order but transferred to a general psychiatric hospital. |
| Nahid et al., 2020 | Qatar | Retrospective chart review | 380 | 1–64 years | All psychiatric conditions | Eleven percent (11%) were readmitted within 30 days of discharge. The predictors were single, male and unemployed, and poor or no compliance to medication after discharge. |
| Olfson et al., 1999 | USA | Retrospective cross-sectional study | 316 | 18–64 years | Schizophrenia and schizoaffective disorder | The rate of readmission was 24.4% within three months of hospital discharge. Predictors were male subjects, persons who had never married, and individuals with relatively low levels of formal education. |
| Ortiz et al., 2019 | USA | Retrospective chart review and file analysis | 60,254 | 38 years | Psychiatric diagnosis | Eight percent (8%) of discharges were readmitted to the same hospital within 30 days of discharge. Factors predicting readmission were white, non-Hispanic, not married, voluntarily admitted, with the length of stay, LOS 8–31 days, LOS 32–92 days, and schizophrenia or other psychotic disorders or personality disorder. |
| Osborn et al., 2021 | England | Cohort study | 231,998 | 16–54 years | Severe psychosis | The rate of readmission was 21.4% within six months. Predictors were female, older, single, from black or mixed ethnic groups, or more deprived areas. Clinical predictors included shorter index admission, psychosis and being an inpatient at baseline. |
| Owen et al., 1997 | Australia | Observational study | 135 | 35.2 years | Schizophrenia, schizoaffective disorder, bipolar, and depression | In the follow-up period, 5% of patients had been admitted to a drug and alcohol admission unit, and 3% had gone to jail. There was no relationship between patient demography, diagnosis, level of symptoms or functioning at discharge, patient attitude to follow-up or patient “likeability” and rehospitalization prediction. |
| Pablo et al., 1986 | Canada | Retrospective chart review and file analysis | 150 | 17–65 years | Schizophrenia, affective disorders | Only 3% of the patients had any readmissions after their 1981 readmission. The average number of readmissions per patient was only 0.63. |
| Patricia et al., 2002 | USA | Randomized control trial | 80 | 39.2 | Psychosis | The readmission rate was reduced by 50% over a 4-month period in patients with positive symptoms of psychosis. |
| Payne et al., 2009 | Scotland | Retrospective cross-sectional study | 50,891 | 15–65 years | Self-poisoning | The 1-year readmission rate was 12.2%. Predictor factors were previous psychiatric hospital treatment and diagnosis of personality disorder. |
| Phillips et al., 2020 | USA | Retrospective cohort study | 6797 | 6–17 years | Mood disorders | Publicly insured, mood disordered, and psychiatrically hospitalized youth were predictors for readmissions within six months of the initial hospital discharge with a readmission rate of 13.8%. |
| Pieterse et al., 2016 | South Africa | Retrospective cohort study | 99 | 12–19 years | Schizophrenia, spectrum bipolar type 1, and substance-induced psychotic disorder | Thirty-six percent (36%) were readmitted during the study period. The predictor factor was having a prior admission. No association was seen between the type of diagnosis and readmission. |
| Popiolek et al., 2018 | Denmark | Population based study | 1255 | 52.2 | Bipolar disorder | The rates for readmission were 29%, 41%, and 52% at 3, 6, and 12 months, respectively, post-discharge. Predictors were a history of multiple psychiatric admissions, lower age, and post-discharge treatment with antipsychotics or benzodiazepines. |
| Puntis et al., 2016 | UK | Retrospective chart review | 323 | 18–65 years | Psychosis | Patients who had a higher proportion of clinical correspondence copied to them spent fewer days in the hospital. |
| Regis et al., 2016 | Brazil | Survey | 6261 | 1–60 years | Psychiatric patients | Within 90 days after discharge, the readmission rate ranged from 16.1 to 20.9%. The predictors for early readmission included the diagnosis of depressive, bipolar, psychotic, and non-alcohol-related disorders, younger ages, and unemployment. |
| Roaldset et al., 2014 | Norway | Prospective observational study | 196 | 38–46 years | Psychiatric diagnosis | Patients exhibiting three or more deliberate self-harm (DSH) related rehospitalizations (repeated DSH, DSH-R) constituted 24% of the total sample of DSH patients and 9% of all patients but accounted for 83% of DSH-related rehospitalizations and 44% of all rehospitalizations. |
| Romansky et al., 2003 | USA | Randomized case study | 500 | 3 to 21 years | Childhood severity of psychiatric illness (CSPI) | Twenty-one percent of the girls and 22% of the boys were readmitted. Learning disability and mental retardation were crucial predictors for readmission. |
| Romer et al., 2018 | Denmark | Record-linkage study | 634 | 34.6 years | Schizophrenia, psychosis, and substance use disorder | Of all patients, 78.7% were readmitted for schizophrenia within 12 months of discharge. Predictors were the use of amphetamine and cannabis, a history of schizophrenia and drug use disorder (DUD). |
| Rylander et al., 2016 | USA | Retrospective chart review | 693 | 38 years | Psychiatric diagnosis | Predictors for readmission were male gender with suicidal ideation on admission, a diagnosis of a psychotic disorder with a prior medical admission, and suicidal ideation with a comorbid personality disorder. |
| Schmutte et al., 2010 | USA | Matched-control survival analysis | 150 | 42.2 years | Psychiatric diagnosis | Thirty percent (30%) were rehospitalized during the 12-month observation period. Predictors were unemployment and living in supervised residential facilities. |
| Shadmi et al., 2018 | Israel | Cohort study | 2842 | 46.9years | Schizophrenia | Quality of life (QoL) was a significant predictor for future hospitalization within six months, and self-report of the impact of symptoms on functioning significantly predicted 12-month hospitalization. |
| Shaffer et al., 2015 | USA | Retrospective comparative study | 149 | 38.8 years | Anxiety disorder, bipolar disorder, schizophrenia, and depression | Longer-term readmission rates were lower in the brief critical time intervention (BCTI) cohort but were not significantly different from the comparison cohort (44% versus 52%). Brief critical time intervention (BCTI) decreased early psychiatric hospital readmission rates for individuals at high risk of readmission. |
| Silva et al., 2009 | Brazil | Case-control study | 307 | 18–69 years | Psychiatric conditions | Individuals referred to community psychosocial support units after their most recent discharge had about a 20% lower risk of multiple readmissions than those referred to usual outpatient care. Predictors of readmission were diagnosis of schizophrenia or psychotic symptoms, younger age at first admission and a more significant number of previous admissions. |
| Silva et al., 2020 | Portugal | Retrospective cross-sectional study | 3872 | 65+ years | Psychiatric diagnosis | Retired, psychotic, and patients with compulsory admission are predicted to have more than one admission within a year. Older age and having a secondary or higher education reduced the risk of admissions. |
| Smith et al., 2015 | USA | Quasi-experimental | 164,544 | 17–65 years | Mental health and substance abuse conditions | The readmission rate for mental health and substance abuse (MHSA) diagnoses was 16.4% within the 12 months after discharge. Predictors were alcohol or drug dependence, dementia, psychotic disorders, autism, impulse control disorders, and personality disorders. |
| Soni et al., 1994 | UK | Case study | 88 | 47.6 years | Chronic schizophrenia | Predictors for readmission were early age of onset of illness, the severity of positive and affective symptoms, current neuroleptic dose and total Involuntary Movement Scale (AIMS) score. |
| Soyka et al., 2013 | Germany | Retrospective cross-sectional study | 5,300,000 | 49 years | Alcohol-induced psychotic disorder | The readmission rate for four years is 62.4%. The key predictors were chronic schizophrenia and mental or behavioral disorders. |
| Tedeschi et al., 2019 | Italy | Comparative study | 63,419 | 18–65 years | Psychiatric diagnosis | The 1-year readmission rate was 43.0%. Predictors for readmission were: admission in the same local health districts (LHDs) as a residence, psychotic disorder, greater length of stay (LoS), and higher rate of public beds in the LHD. |
| Thomas et al., 2018 | USA | Retrospective observational study | 240 | 18–65 years | Schizophrenia, schizoaffective disorder, or bipolar disorder | The rate of readmissions for those who received the LAI and those who did not were 43.1% and 56.95, respectively. Patients who received the LAI at a frequency of one month or longer had a significant longer survival time without readmission compared to those with a shorter administration frequency (mean 307.9 and 245.0 days). |
| Trask et al., 2016 | USA | Retrospective chart study | 569 | 6–18 years | Childhood psychiatric disorders | Seventy percent (70%) of youths with a psychiatric hospitalization received aftercare and 28% were rehospitalized within six months of discharge. Predictors were having a diagnosis of schizophrenia and receiving more days of day treatment reduced the risk of rehospitalization. |
| van Alphen et al., 2017 | USA | Retrospective observational study | 165 | 13–19 years | Depression | Overall, 12.1% of patients were rehospitalized within the period. The predictor was frequent self-injurious behaviors in the month prior to hospitalization. |
| Volpe et al., 2018 | Brazil | Retrospective cross-section study | 19,723 | 37.4 years | All psychiatric conditions | The rates for readmissions were 5.7% for less than seven days, 5.9% for 8–30 days, and 18.9% for 31–365 days. Young male patients and those residing outside the capital were predictors for readmission. Psychotic disorders, mood disorders, and neurotic disorders were protective factors for readmission. |
| Xu et al., 2018 | USA | 973,078 | 52–70 years | Epilepsy | Less than one percent were readmitted. Predictors were psychiatric comorbidities, epilepsy, and risk of suicide. | |
| Yedlapati et al., 2018 | USA | Cross-sectional and retrospective analyses | 163,143 | 50.4 years | Alcohol withdrawal | The yearly readmission rate was 60%. Predictors for 30-day readmission and multiple readmissions were discharged against medical advice (AMA), comorbid psychosis and low socioeconomic status. |
| Yussuf et al., 2008 | Nigeria | Retrospective record study | 502 | 21–40 years | Psychiatric patients | Within the study period, 41.4% were readmitted. Predictors for readmission were a young age, a longer length of stay, multiple admissions, and a diagnosis of schizophrenia. |
| Zhang et al., 2011 | Australia | Retrospective study | 249 | 39 years | Psychotic illness | Predictors for readmission were a history of previous frequent admissions, a risk to others at the index admission and alcohol intoxication. More active and assertive treatment in the community post-discharge decreased the risk of readmission. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owusu, E.; Oluwasina, F.; Nkire, N.; Lawal, M.A.; Agyapong, V.I.O. Readmission of Patients to Acute Psychiatric Hospitals: Influential Factors and Interventions to Reduce Psychiatric Readmission Rates. Healthcare 2022, 10, 1808. https://doi.org/10.3390/healthcare10091808
Owusu E, Oluwasina F, Nkire N, Lawal MA, Agyapong VIO. Readmission of Patients to Acute Psychiatric Hospitals: Influential Factors and Interventions to Reduce Psychiatric Readmission Rates. Healthcare. 2022; 10(9):1808. https://doi.org/10.3390/healthcare10091808
Chicago/Turabian StyleOwusu, Ernest, Folajinmi Oluwasina, Nnamdi Nkire, Mobolaji A. Lawal, and Vincent I. O. Agyapong. 2022. "Readmission of Patients to Acute Psychiatric Hospitals: Influential Factors and Interventions to Reduce Psychiatric Readmission Rates" Healthcare 10, no. 9: 1808. https://doi.org/10.3390/healthcare10091808