
Telerehabilitation as a Form of Pulmonary Rehabilitation in Chronic Lung Disease: A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Literature Search and Selection
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction and Analysis
2.5. Risk of Bias
3. Results
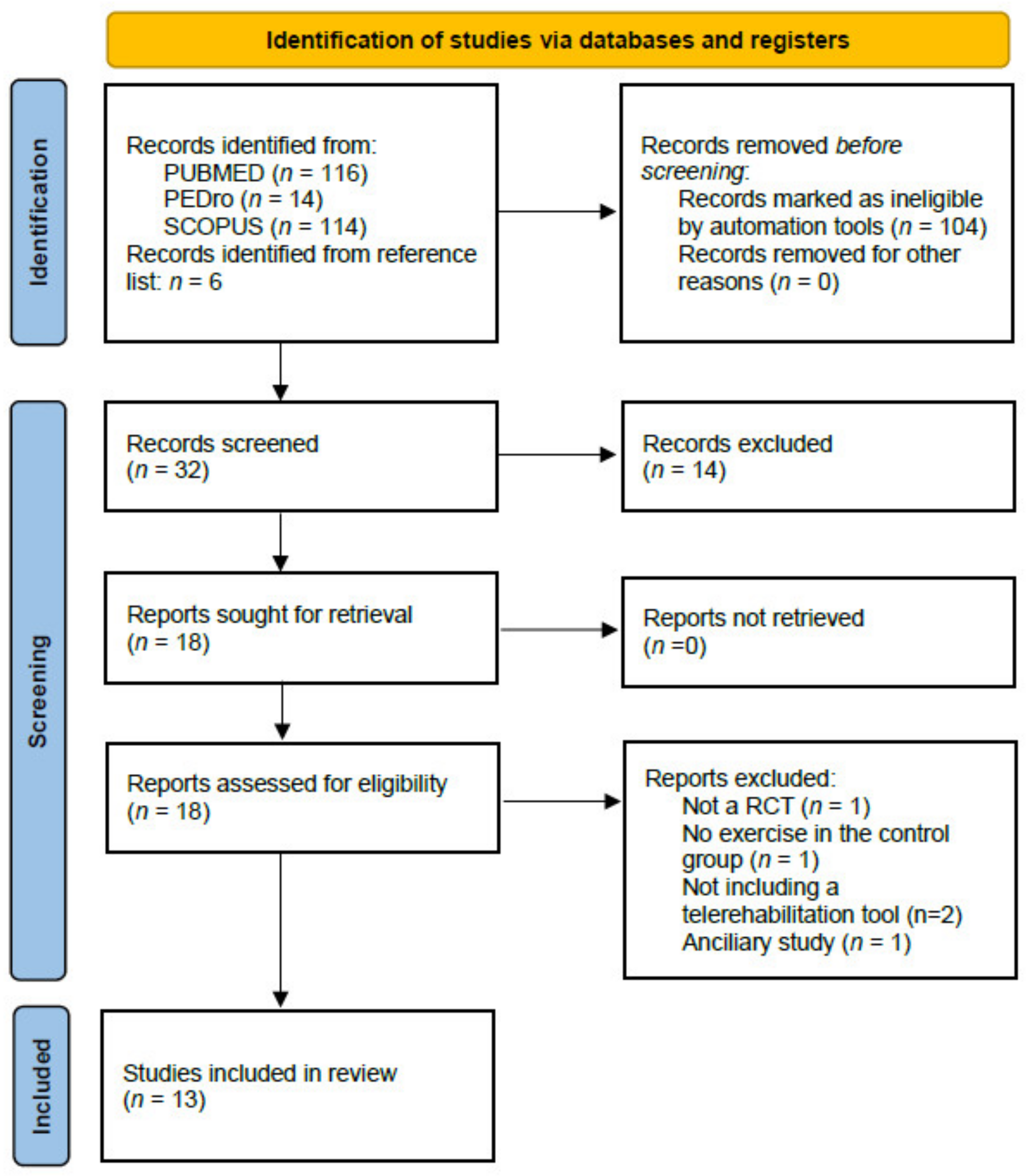
3.1. Study Selection
3.2. Study Characteristics
3.3. Participants
3.4. Intervention Characteristics
3.5. Quality of Studies
3.6. Outcome Measures
3.7. Effects of Intervention
3.7.1. Effects on Functional Exercise Capacity
3.7.2. Effects on Dyspnoea
3.7.3. Effects on Quality of Life
3.8. Adherence and Adverse Events Related to Telerehabilitation
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.C.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Wuytack, F.; Devane, D.; Stovold, E.; McDonnell, M.; Casey, M.; McDonnell, T.J.; Gillespie, P.; Raymakers, A.; Lacasse, Y.; McCarthy, B. Comparison of outpatient and home-based exercise training programmes for COPD: A systematic review and meta-analysis. Respirology 2018, 23, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Cox, N.S.; Oliveira, C.C.; Lahham, A.; Holland, A.E. Pulmonary rehabilitation referral and participation are commonly influenced by environment, knowledge, and beliefs about consequences: A systematic review using the Theoretical Domains Framework. J. Physiother. 2017, 63, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Augustine, A.; Bhat, A.; Vaishali, K.; Magazine, R. Barriers to pulmonary rehabilitation—A narrative review and perspectives from a few stakeholders. Lung 2021, 38, 59–63. [Google Scholar]
- Sami, R.; Salehi, K.; Hashemi, M.; Atashi, V. Exploring the barriers to pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: A qualitative study. BMC Health Serv. Res. 2021, 21, 828. [Google Scholar] [CrossRef]
- Ozden, F.; Sari, Z.; Karaman, O.N.; Aydogmus, H. The effect of video exercise-based telerehabilitation on clinical outcomes, expectation, satisfaction, and motivation in patients with chronic low back pain. Ir. J. Med. Sci. 2021, 191, 1229–1239. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Bernocchi, P.; Vitacca, M.; La Rovere, M.T.; Volterrani, M.; Galli, T.; Baratti, D.; Paneroni, M.; Campolongo, G.; Sposato, B.; Scalvini, S. Home-based telerehabilitation in older patients with chronic obstructive pulmonary disease and heart failure: A randomised controlled trial. Age Ageing 2018, 47, 82–88. [Google Scholar] [CrossRef]
- Kwon, H.; Lee, S.; Jung, E.J.; Kim, S.; Lee, J.K.; Kim, D.K.; Kim, T.H.; Lee, S.H.; Lee, M.K.; Song, S.; et al. An mHealth Management Platform for Patients with Chronic Obstructive Pulmonary Disease (efil breath): Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e10502. [Google Scholar] [CrossRef]
- Knox, L.; Dunning, M.; Davies, C.A.; Mills-Bennet, R.; Sion, T.W.; Phipps, K.; Stevenson, V.; Hurlin, C.; Lewis, K. Safety, feasibility, and effectiveness of virtual pulmonary rehabilitation in the real world. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 775–780. [Google Scholar] [CrossRef]
- Chaplin, E.; Hewitt, S.; Apps, L.; Bankart, J.; Pulikottil-Jacob, R.; Boyce, S.; Morgan, M.; Williams, J.; Singh, S. Interactive web-based pulmonary rehabilitation programme: A randomised controlled feasibility trial. BMJ Open 2017, 7, e013682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourne, S.; DeVos, R.; North, M.; Chauhan, A.; Green, B.; Brown, T.; Cornelius, V.; Wilkinson, T. Online versus face-to-face pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: Randomised controlled trial. BMJ Open 2017, 7, e014580. [Google Scholar] [CrossRef] [PubMed]
- Cerdán-de-Las-Heras, J.; Balbino, F.; Løkke, A.; Catalán-Matamoros, D.; Hilberg, O.; Bendstrup, E. Tele-Rehabilitation Program in Idiopathic Pulmonary Fibrosis-A Single-Center Randomized Trial. Int. J. Environ. Res. Public Health 2021, 18, 10016. [Google Scholar] [CrossRef]
- Hansen, H.; Bieler, T.; Beyer, N.; Kallemose, T.; Wilcke, J.T.; Østergaard, L.M.; Andeassen, H.F.; Martinez, G.; Lavesen, M.; Frølich, A.; et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: A randomised multicentre trial. Thorax 2020, 75, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Tabak, M.; Vollenbroek-Hutten, M.M.; van der Valk, P.D.; van der Palen, J.; Hermens, H.J. A telerehabilitation intervention for patients with Chronic Obstructive Pulmonary Disease: A randomized controlled pilot trial. Clin. Rehabil. 2014, 28, 582–591. [Google Scholar] [CrossRef]
- Tsai, L.L.; McNamara, R.J.; Moddel, C.; Alison, J.A.; McKenzie, D.K.; McKeough, Z.J. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: The randomized controlled TeleR Study. Respirology 2017, 22, 699–707. [Google Scholar] [CrossRef]
- Vasilopoulou, M.; Papaioannou, A.I.; Kaltsakas, G.; Louvaris, Z.; Chynkiamis, N.; Spetsioti, S.; Kortianou, E.; Genimata, S.A.; Palamidas, A.; Kostikas, K.; et al. Home-based maintenance tele-rehabilitation reduces the risk for acute exacerbations of COPD, hospitalisations and emergency department visits. Eur. Respir. J. 2017, 49, 602129. [Google Scholar] [CrossRef]
- Yuen, H.K.; Lowman, J.D.; Oster, R.A.; de Andrade, J.A. Home-Based Pulmonary Rehabilitation for Patients with Idiopathic Pulmonary Fibrosis: A Pilot Study. J. Cardiopulm. Rehabil. Prev. 2019, 39, 281–284. [Google Scholar] [CrossRef]
- Franke, K.J.; Domanski, U.; Schroeder, M.; Jansen, V.; Artmann, F.; Weber, U.; Ettler, R.; Nilius, G. Telemonitoring of home exercise cycle training in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2821–2829. [Google Scholar] [CrossRef]
- Galdiz, J.B.; Gómez, A.; Rodriguez, D.; Guell, R.; Cebollero, P.; Hueto, J.; Cejudo, P.; Ortega, F.; Sayago, I.; Chic, S.; et al. Telerehabilitation Programme as a Maintenance Strategy for COPD Patients: A 12-Month Randomized Clinical Trial. Arch. Bronconeumol. 2021, 57, 195–204. [Google Scholar] [CrossRef]
- Ibeggazene, S.; Turner, R.; Rosario, D.; Bourke, L. Remote interventions to improve exercise behaviour in sedentary people living with and beyond cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 308. [Google Scholar] [CrossRef] [PubMed]
- Zasadzka, E.; Trzmiel, T.; Pieczynska, A.; Hojan, K. Modern Technologies in the Rehabilitation of Patients with Multiple Sclerosis and Their Potential Application in Times of COVID-19. Medicina 2021, 57, 549. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Cox, N.S.; Houchen-Wolloff, L.; Rochester, C.L.; Garvey, C.; ZuWallack, R.; Nici, L.; Limberg, T.; Lareau, S.C.; Yawn, B.P.; et al. Defining Modern Pulmonary Rehabilitation. An Official American Thoracic Society Workshop Report. Ann. Am. Thorac. Soc. 2021, 18, e12–e29. [Google Scholar] [CrossRef] [PubMed]
- Pang, L.; Liu, Z.; Lin, S.; Liu, Z.; Liu, H.; Mai, Z.; Liu, Z.; Chen, C.; Zhao, Q. The effects of telemedicine on the quality of life of patients with lung cancer: A systematic review and meta-analysis. Ther. Adv. Chronic Dis. 2020, 11, 2040622320961597. [Google Scholar] [CrossRef]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef]
- Parshall, M.B.; Schwartzstein, R.M.; Adams, L.; Banzett, R.B.; Manning, H.L.; Bourbeau, J.; Calverley, P.M.; Gift, A.G.; Harver, A.; Lareau, S.C.; et al. An official American Thoracic Society statement: Update on the mechanisms, assessment, and management of dyspnoea. Am. J. Respir. Crit. Care Med. 2012, 185, 435–452. [Google Scholar] [CrossRef]
- Keating, A.; Lee, A.L.; Holland, A.E. Lack of perceived benefit and inadequate transport influence uptake and completion of pulmonary rehabilitation in people with chronic obstructive pulmonary disease: A qualitative study. J. Physiother. 2011, 57, 183–190. [Google Scholar] [CrossRef]
- Piraux, E.; Caty, G.; Renard, L.; Vancraeynest, D.; Tombal, B.; Geets, X.; Reychler, G. Effects of high-intensity interval training compared with resistance training in prostate cancer patients undergoing radiotherapy: A randomized controlled trial. Prostate Cancer Prostatic Dis. 2021, 24, 156–165. [Google Scholar] [CrossRef]
- Spruit, M.A.; Singh, S.J. Maintenance programs after pulmonary rehabilitation: How may we advance this field? Chest 2013, 144, 1091–1093. [Google Scholar] [CrossRef]


{kind=link}
| Authors, Year | Disease (s) | Group | Sample (n) | Age (Year) | Gender (M/F) | FEV1 (%) | BMI (kg/m2) | Drop-Out |
|---|---|---|---|---|---|---|---|---|
| Tabak 2014 [15] | COPD | IG | 14 | 65.2 ± 9.0 | 8/6 | 48.7 ± 16.7 | 28.4 ± 7.8 | 0 |
| CG | 16 | 67.9 ± 5.7 | 11/5 | 56.4 ± 10.6 | 29.2 ± 4.7 | 0 | ||
| Chaplin 2017 [11] | COPD | IG | 51 | 66.4 ± 10.1 | 38/14 | 58.7 ± 29.1 | 27.9 ± 6.4 | 29 |
| CG | 52 | 66.1 ± 8.1 | 33/19 | 55.0 ± 20.5 | 29.3 ± 6.3 | 12 | ||
| Franke 2016 [19] | COPD | IG-CG | 23 | 63.3 ± 7.8 | 20/24 | 47.5 ± 15.8 | 24.3 ± 5.2 | 5 |
| CG-IG | 21 | 2 | ||||||
| Bourne 2017 [12] | COPD | IG | 64 | 69.1 ± 7.9 | 18/8 | 58.0 ± 23.6 | NR | 7 |
| CG | 26 | 71.4 ± 8.6 | 41/23 | 60.5 ± 20.1 | NR | 5 | ||
| Tsai 2017 [16] | COPD | IG | 20 | 73 ± 8 | 12/7 | 60 ± 23 | 28 ± 4 | 1 (unrelated) |
| CG | 17 | 75 ± 9 | 6/11 | 68 ± 19 | 28 ± 5 | 0 | ||
| Vasilopoulou 2017 [17] | COPD | IG | 47 | 66.9 ± 9.6 | 44/3 | 49.6 ± 21.9 | 28.0 ± 5.3 | 0 |
| CG1 | 50 | 66.7 ± 7.3 | 38/12 | 51.8 ± 17.3 | 27.5 ± 5.0 | 0 | ||
| CG2 | 50 | 64.0 ± 8.0 | 37/13 | 51.7 ± 21.0 | 26.4 ± 5.0 | 0 | ||
| Bernocchi 2018 [8] | COPD + CHF | IG | 56 | 71 ± 9 | 50/6 | 66.6 ± 18.6 | 28.5 ± 5.8 | 11 |
| CG | 56 | 70 ± 9.5 | 42/14 | 66.1 ± 16.4 | 27.7 ± 5.4 | 21 | ||
| Kwon 2018 [9] | COPD | IG1 | 27 | 64 ± 8 | 23/4 | 58.6 ± 15.8 | 23.6 ± 3.7 | 11 |
| IG2 | 30 | 65 ± 7 | 26/4 | 57.1 ± 16.8 | 22.6 ± 3.0 | 6 | ||
| CG | 28 | 64 ± 8 | 21/7 | 55.8 ± 15.5 | 24.3 ± 3.9 | 6 | ||
| Knox 2019 [10] | COPD + CLD | IG | 21 | 70.1 ± 10.8 | 14/7 | NR | NR | 0 |
| CG | 24 | 68.6 ± 12.8 | 10/14 | NR | NR | 1 | ||
| Yuen 2019 [18] | IPF | IG | 10 | 67.4 ± 7.4 | 5/5 | 65 ± 15 | 28.0 ± 4.6 | 3 |
| CG | 10 | 72.2 ± 8.4 | 8/2 | 86 ± 18 | 28.4 ± 4.3 | 0 | ||
| Hansen 2020 [14] | COPD | IG | 67 | 68.4 ± 8.7 | 32/35 | 32.6 ± 10.3 | 25.5 ± 5.0 | 10 |
| CG | 67 | 68.2 ± 9.4 | 28/39 | 33.7 ± 8.4 | 25.9 ± 6.4 | 14 | ||
| Galdiz 2021 [20] | COPD | IG | 41 | 63.0 ± 6.6 | 27/14 | 42.1 ± 14.6 | 26.5 ± 5.2 | 2 |
| CG | 40 | 62.3 ± 8.2 | 27/13 | 45.9 ± 17.2 | 27.7 ± 5.1 | 2 | ||
| Cerdan 2021 [13] | IPF | IG | 15 | 70.1 ± 8.8 | 13/2 | NR | NR | 5 |
| CG | 14 | 72.4 ± 7.6 | 8/6 | NR | NR | 3 |
| Authors, Year | Group | Setting, Supervision | Length of Intervention | Frequency Duration | Exercise Intervention | Follow-Up | Adherence (A) Adverse Events (AE) | PEDro |
|---|---|---|---|---|---|---|---|---|
| (A) Studies using usual care as control group | ||||||||
| Tabak 2014 [15] | IG | Accelerometer Smartphone Web diary No | 4 w | >4/w | Feedback text messages (awareness and extra motivation) based on the difference between the activity and the reference Advice on how to improve or maintain the activity behaviour | - | A: 54% AE: NR | 5 |
| CG | UC | 4 w | Medication and physiotherapy (training session) | - | A: NR AE: NR | |||
| Tsai 2017 [16] | IG | Videoconference Lower limb cycloergometer Oximeter Yes | 8 w | 3/w 55 min | Lower limb cycle ergometer, walking training and strengthening exercises | - | A: 92% AE: no | 8 |
| CG | UC | Optimal pharmacological intervention Action plan | - | A: NR | ||||
| Vasilopoulou 2017 [17] | IG | Video Psychological support Weekly contact Multimodal apparatus (pedometer) Tablet Call centre No | 2 m PR + 12 m Maintenance TelePR (144 sessions) No | 3/w NR | Exercise (arm and leg exercises and walking drills) Action plan | - | A: 93% AE: no | 5 |
| CG1 | PR Yes | 2 m PR + 12 m PR (96 sessions) | 2/w NR | Exercise | - | A: 91% AE: no | ||
| CG2 | UC No | 2 m PR + 12 m UC | Optimal pharmacological treatment | - | A: NR | |||
| Kwon 2018 [9] | IG1 | TelePR Non-interactive App Monitoring website Oximeter (connected) No | 12 w (fixed) | Walking (fixed program) (6 levels of distance, automatic increment) | - | A: 59% AE: NR | 3 | |
| IG2 | TelePR Interactive App Monitoring website Oximeter (connected) Yes | 6 w (fixed) + 6 w (Interactive) | Walking (interactive program) (12 levels and automatic adaptation based on the Borg scale) | - | A: 80% AE: NR | |||
| CG | UC | - | A: 79% | |||||
| Bernocchi 2018 [8] | IG | TelePR kit (ergometer, pedometer) Phone call Oximeter + ECG No | 4 m No | From 3/w + 2/w to 3 to 7/w From 45–55 min to 30 to 45 min | Initial level Ergometer without load (3/w) Walking (2/w) Final level Ergometer (from 0 to 60 W) Muscle reinforcement (0.5 kg) Pedometer | 2 m | A: <60% AE: no | 4 |
| CG | UC | Pharmacological treatment PTE | 2 m | |||||
| Galdiz 2021 [20] | IG | TelePR kit (phone, oximeter) No | 8 w PR + 12 m Maintenance TelePR | 3/w 60 min | 30 min weightlifting 30 min on cycle ergometer 4 sessions of PTE | 3, 9, 12 m | A: 60% AE:no | 7 |
| CG | UC No | 8 w PR + 12 m UC | Advice: 1 h walking/d | 3, 9, 12 m | A: NR AE: NR | |||
| Cerdan 2021 [13] | IG | TelePR Video Chat Oximeter Tablet No | 12 w | 3–5/w 10–20 min | Exercise E-learning | 3, 6 m | A: 64% AE: NR | |
| CG | UC No | 12 w | Pharmacological treatment | |||||
| (B) Studies using exercise or PR as control group | ||||||||
| Chaplin 2017 [11] | IG | TelePR Weekly phone call No | 6/8 w | Target weekly work | Exercise (aerobic and upper/lower limb resistance training) PTE | - | A: NR AE: 20% | 5 |
| CG | PR Yes | 7 w | 2/w 120 min | Exercise (aerobic and upper/lower limb resistance training) (60 min) PTE (60 min) | - | A: NR AE: 5% | ||
| Franke 2016 [19] | IG | Ergometer with data transmission Phone call No | 3 m | 7/w 30 min | Ergometer with motivational phone call every week | - | A: 69% AE: NR | 4 |
| CG | Ergometer No | 3 m | 7/w 30 min | Ergometer without motivational phone call | A: 61% AE: NR | |||
| Bourne 2017 [12] | IG | TelePR No | 6 w | 2 to 5/w 10 min to 35 min | 10 exercises (Biceps curls, squats, push-ups against a wall, leg extensions in a sitting position, upright row with weights, sit-to-stand, arm swings with a stick, leg kicks to the side, arm punches with weights and step-ups) PTE | - | A: 62% AE: 2 | 8 |
| CG | PR Yes | 6 w | 2/w (PR) 3/w (home) NR | 10 exercises (Biceps curls, squats, push-ups against a wall, leg extensions in a sitting position, upright row with weights, sit-to-stand, arm swings with a stick, leg kicks to the side, arm punches with weights and step-ups. PTE | - | A: 72% AE: 3 | ||
| Vasilopoulou 2017 [17] | IG | Video Psychological support Weekly contact Multimodal apparatus (pedometer) Tablet Call centre No | 2 m PR + 12 m Maintenance TelePR (144 sessions) No | 3/w NR | Exercise (arm and leg exercises, and walking drills) Action plan | - | A: 93% AE: no | 5 |
| CG1 | PR Yes | 2 m PR + 12 m PR (96 sessions) | 2/w NR | Exercise | - | A: 91% AE: no | ||
| CG2 | UC No | 2 m PR + 12 m UC | Optimal pharmacological treatment | - | A: NR | |||
| Knox 2019 [10] | IG | TelePR Videoconference Yes | 7 w | 2/w 60–90 min + 20–40 min (spoke site) | Exercise PTE | - | A: 61.9% AE: 0 | 0 |
| CG | PR Yes | 7 w | 2/w 60–90 min + 20–40 min (hub site) | Exercise PTE | - | A: 54.6% AE: 1 | ||
| Yuen 2019 [18] | IG | Wii U console Balance Board Wii Fit game Phone call No | 12 w | 3/w 30 min | Exergame | - | A: 39% AE: 0 | 7 |
| CG | Nintendo Wii U console Traditional video game Phone call No | 12 w | 3/w 30 min | Video game | - | A: NR AE: 0 | ||
| Hansen 2020 [14] | IG | TelePR Videoconference Yes | 10 w | 3/w 35 min | High repetitive muscle exercise PTE | 3, 12 m | A: 83% AE: 2 | 7 |
| CG | PR Yes | 10 w | 2/w 60 min | Exercise PTE | A: 80% AE: 0 | |||
| Authors, Year | Functional Exercise Capacity | Dyspnoea | HRQoL Anxiety-Depression |
|---|---|---|---|
| Studies using usual care as control group | |||
| Tabak 2014 [15] | Accelerometer IG: 5766 ± 965–6106 ± 965–6271 ± 959–5603 ± 964 CG: 5256 ± 865–4853 ± 865–4590 ± 865–4617 ± 865 p = 0.482 | MRC IG: 2.0 ± 0.9 (Δ: −0.3 ± 0.7) CG: 2.3 ± 1.4 (Δ: −0.2 ± 0.9) | CCQ IG: 2.0 ± 0.8 (Δ: −0.3 ± 0.5) CG: 1.8 ± 1.0 (Δ: 0.0 ± 0.6) |
| Tsai 2017 [16] | 6MWT (m) IG: 363 (66)–403 (82) (+40 (1/80)) CG: 383 (93)–374 (136) (−9 (−62/44) IG vs. CG: 45 (−18/108) ISWT (m) IG: 260 (106)–275 (132) (+12 (−12/36)) CG: 298 (114)–306 (118) (+8 (−8/24)) IG vs. CG: 6 (−23/35) ESWT (s) IG: 410 (253)–693 (357) (283 (107/460)) CG: 361 (155)–316 (182) (−31 (−76/14)) IG vs. CG: 340 (153/526) | Borg IG: 4 (2)–3 (2) (+1 (0/2)) CG: 4 (2)–4 (2) (0 (−1/1)) IG vs. CG: +4 (−7/16) | CRDQ IG: 90 (18)–99 (16) (+9 (2/16) CG: 88 (23)–90 (18) (+2 (−5/10) IG vs. CG: +8 (−1/16) CAT IG: 16 (7)–15 (7) (−1 (−4/2) CG: 15 (6)–18 (6) (+3 (1/5) IG vs. CG: −3 (−7/0) HADS-A IG: 5 (4)–4 (4) (−2 (−3/−0.3) CG: 6 (4)–6 (3) (−1 (−2/1) IG vs. CG: −1 (−3/0) HADS-D IG: 5 (3)–4 (3) (−1.4 (−2/−0.4) CG: 5 (3)–6 (3) (+1(0/3)) IG vs. CG: −3 (−4/−1) |
| Vasilopoulou 2017 [17] | 6MWT (m) IG: 389.1 ± 91.3–422.1 ± 70.5–420.2 ± 74.9 (NS) CG1: 385.1 ± 80.3–423.0 ± 70.5–427.5 ± 63.0 (NS) CG2: 384.8 ± 80.2–382.4 ± 80.3–339.9 ± 110.1 (NS) IG et CG1 vs. CG2: S | mMRC IG: 1.8 ± 0.9–1.6 ± 1.0 CG1: 1.5 ± 0.9–1.3 ± 0.9 CG2: 2.5 ± 1.0–3.1 ± 0.8 IG vs. CG1 vs. CG2: S | SGRQ IG: 42.2 ± 19.2–38.4 ± 20.5 CG1: 35.4 ± 15.7–33.6 ± 16.5 CG2: 44.7 ± 16.9–50.2 ± 17.7 IG vs. CG1 vs. CG2: S CAT IG: 12.9 ± 7.5–13.0 ± 7.3 CG: 13.2 ± 5.8–11.8 ± 5.6 CG2: 16.1 ± 6.2–20.9 ± 6.7 IG vs. CG1 vs. CG2: S |
| Kwon 2018 [9] | 6MWT (m) IG1: NS IG2: NS CG: NS | MRC IG1: NS IG2: NS CG: NS | CAT IG1: p = 0.01 (6 w), NS (6 w) IG2: p = 0.06 (6 w), NS (6 w) |
| Bernocchi 2018 [8] | 6MWT (m) IG: +60 (22.2/97.8) CG: −15 (−40.3/9.8) IG vs. CG: p = 0.004 | MRC IG: −0.17 (−0.3/−0.02) CG: 0.07 (−0.1/0.3) IG vs. CG: p = 0.05 | CAT IG: −5.3 (−6.9/−3.7) CG: +1.6 (−0.4/3.5) IG vs. CG: p < 0.001 |
| Galdiz 2021 [20] | 6MWT (m) IG: 445 m (102)–436 (113)–432 (117)–441 (106) CG: 449 m (92)–447 (95)–423 (117)–423 (101) IG vs. CG: 19.9 m (−4.1/43.8)(p = 0.10) | BODE IG vs. CG: 0.0 (−0.6/0.6) (p = 0.89) CRQ-D IG: 5.2 (1.2)–5.2 (1.1)–4.9 (1.2)–4.8 (1.5) CG: 5.2 (1.5)–4.7 (1.5)–4.8 (1.3)–5.0 (1.3) IG vs. CG: NR | CRQ-F IG: 4.7 (1.1)–4.7 (1.0)–4.5 (1.2)–4.5 (1.3) CG: 4.8 (1.3)–4.2 (1.4)–4.1 (1.2)–4.3 (1.5) IG vs. CG: +0.3 (−0.2/0.8) (p = 0.20) CRQ-E IG: 5.1 (1.2)–5.3 (1.0)–5.1 (1.2)–5.1 (1.2) CG: 5.2 (1.3)–4.6 (1.4)–4.7 (1.3)–4.8 (1.3 IG vs. CG: +0.4 (0.0/0.8) (p = 0.067) CRQ-M IG: 5.2 (1.5)–5.5 (1.2)–5.2 (1.5)–5.1 (1.4) CG: 5.3 (1.5)–4.9 (1.5)–5.0 (1.5)–5.0 (1.5) IG vs. CG: +0.2 (−0.4/0.7) (p = 0.55) |
| Cerdan 2021 [13] | 6MWT (m) IG: 461.5 ± 115–470 ± 115 (S)–469 ± 136 (S)–448 ± 133 CG: 446 ± 63.6–421 ± 70–423 ± 76–390 ± 85 IG vs. CG: NR–+39.5 (p = 0.03)–+34.3 (p = 0.02)–+40.0 (p = 0.15). | SGRQ-I IG: 49.8 ± 14.9–51.2 ± 17.8–48.3 ± 13.3–43.9 ± 19.4 CG: 47.7 ± 16.7–43.3 ± 16.4–49.7 ± 22.2–45.9 ± 16.6 IG vs. CG: NS GAD7 IG: 1.63 ± 2.5–3.27 ± 3.9–2.9 ± 3.1–2.1 ± 3.2 CG: 2.36 ± 3.9–2.55 ± 3.3–0.8 ± 1.7–4.6 ± 3.7 IG vs. CG: NS | |
| Studies using exercise or PR as control group | |||
| Chaplin 2017 [11] | ESWT (s) IG: +189 ± 211.1 CG: +184.5 ± 247.4 IG vs. CG: NS | CRQ-D IG: +0.7 ± 1.2 CG: +0.8 ± 1.0 IG vs. CG: NS | CAT: NR (NS) HADS: NR (NS) |
| Franke 2016 [19] | Training time (min) IG: 24.2 ± 9.4 CG: 19.6 ± 10.3 IG vs. CG: p < 0.001 IGt1: 26.7 ± 8.4 IGt2: 21.5 ± 9.9 IGt1 vs. IGt2: p = 0.066 | CAT IG: 15.3 ± 7.6 (p = 0.006) CG: 15.7 ± 7.3 (p = 0.03) IG vs. CG: p = 0.03 | |
| Bourne 2017 [12] | 6MWT (m) IG: 416.5 ± 118.3–445.1 ± 124.9 CG: 388.7 ± 104.4–433.6 ± 102.9 IG vs. CG: p = 0.10 | mMRC IG: 2.0 (1-2)–1.5 (1-2) CG: 2 (1-3)–1 (1-2) IG vs. CG: p = 0.91 | SGRQ IG: 37.7 ± 17.2–39.3 ± 18.5 CG: 42.4 ± 18.6–39.3 ± 18.5 IG vs. CG: p = 0.30 CAT IG: 17.3 ± 6.7–16.2 ± 6.7 CG: 18.1 ± 7.9–14.9 ± 7.0 IG vs. CG: p = 0.37 HADS IG: 10.0 (6-18)–10.5 (5-13) CG: 10.0 (6-16.5)–7 (4-15) IG vs. CG: p = 0.26 |
| Vasilopoulou 2017 [17] | 6MWT (m) IG: 389.1 ± 91.3–422.1 ± 70.5–420.2 ± 74.9 (NS) CG1: 385.1 ± 80.3–423.0 ± 70.5–427.5 ± 63.0 (NS) CG2: 384.8 ± 80.2–382.4 ± 80.3–339.9 ± 110.1 (NS) IG et CG1 vs. CG2: S | mMRC IG: 1.8 ± 0.9–1.6 ± 1.0 CG1: 1.5 ± 0.9–1.3 ± 0.9 CG2: 2.5 ± 1.0–3.1 ± 0.8 IG vs. CG1 vs. CG2: NR | SGRQ IG: 42.2 ± 19.2–38.4 ± 20.5 CG1: 35.4 ± 15.7–33.6 ± 16.5 CG2: 44.7 ± 16.9–50.2 ± 17.7 IG vs. CG1 vs. CG2: NR CAT IG: 12.9 ± 7.5–13.0 ± 7.3 CG: 13.2 ± 5.8–11.8 ± 5.6 CG2: 16.1 ± 6.2–20.9 ± 6.7 IG vs. CG1 vs. CG2: NR |
| Knox 2019 [10] | ISWT (m) IG: +137 (S) CG: +66 (S) IG vs. CG: p = 0.025 | MRC IG: 3.3 ± 0.8–−0.75 ± 0.86 (p = 0.003) CG: 3.5 ± 0.9–−0.48 ± 0.60 (p = 0.002) IG vs. CG: p = 0.26 | CAT IG: 24.0 ± 6.2 (S) CG: 25.2 ± 6.6 (S) IG vs. CG: p = 0.51 HADS-A IG: 7.6 ± 4.2 (S) CG: 8.2 ± 3.5 IG vs. CG: p = 0.18 HADS-D IG: 7.05 ± 2.60 CG: 6.50 ± 2.70 IG vs. CG: p = 0.07 |
| Yuen 2019 [18] | 6MWT (m) IG: 321 ± 88–305 ± 108 (p = 0.27) CG: 408 ± 103–372 ± 125 (p = 0.17) IG vs. CG: p = 0.29 | Borg IG: 2.4 ± 1.3–3.4 ± 1.6 (p = 0.02) CG: 1.65 ± 1.3–1.4 ± 1.2 (p = 0.54) IG vs. CG: p = 0.99 | SGRQ IG: 44 ± 12–47 ± 15 (p = 0.30) CG: 32 ± 10–33 ± 17 (p = 0.70) IG vs. CG: p = 0.63 |
| Hansen 2020 [14] | 6MWT (m) IG: 17.2 (5.8/28.5)(S) − 22.0 (5.0/39.1)(S) CG: 23.5 (12.1/35.0)(S) − 11.0 (−5.2/27.2) IG vs. CG (end–12 m): 8.3 (−7.7/24.3) − −3.9 (−27.9/19.9) 30sSTST IG: 1.3 (0.4/2.0)(S)–1.1 (0.1/2.0)(S) CG: 1.7 (0.9/2.5)(S)–1.5 (0.5/2.3)(S) IG vs. CG (end–12 m): 0.5 (−0.6/1.5)–0.5 (−0.6/1.6) | CCQ IG: −0.3 (−0.4/−0.1)(S)−0.0 (−0.2/0.2) CG: −0.1 (−0.3/0.1)−0.1 (−0.2/0.3) IG vs. CG (end–12 m): 0.2 (−0.1/0.5) − 0.1 (−0.1/0.4) EQ5D-VAS IG: 3.2 (−1.2/7.6)−3.5 (−1.2/8.2) CG: 2.9 (−1.4/7.2)−4.2 (−0.4/9.0) IG vs. CG (end–12 m): −0.2 (−6.2/5.9) − 1.6 (−5.1/8.3) CAT IG: −1.7 (−3.2/−0.2)(S)–−0.5 (−1.9/1.1) CG: −0.3 (−1.8/1.2)–−1.0 (−2.5/0.6) IG vs. CG (end–12 m): 1.6 (0.1/3.3)(S)–−0.2 (−2.1/1.8) HADS-A IG: −1.0 (−1.7/−0.2)(S)–−0.5 (−1.4/0.5) CG: 0.1 (−0.6/0.8)–−0.3 (−1.2/0.7) IG vs. CG (end–12 m): 1.2 (0.2/2.3)(S)−0.4 (−0.8/1.6) HADS-D IG: −0.4 (−1.1/0.3)−0.5 (−0.4/1.5) CG: 0.3 (−0.4/1.0)−0.3 (−0.6/1.4) IG vs. CG (end–12 m): 0.9 (0.1/1.7)(S) –−0.2 (−1.3/1.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reychler, G.; Piraux, E.; Beaumont, M.; Caty, G.; Liistro, G. Telerehabilitation as a Form of Pulmonary Rehabilitation in Chronic Lung Disease: A Systematic Review. Healthcare 2022, 10, 1795. https://doi.org/10.3390/healthcare10091795
Reychler G, Piraux E, Beaumont M, Caty G, Liistro G. Telerehabilitation as a Form of Pulmonary Rehabilitation in Chronic Lung Disease: A Systematic Review. Healthcare. 2022; 10(9):1795. https://doi.org/10.3390/healthcare10091795
Chicago/Turabian StyleReychler, Gregory, Elise Piraux, Marc Beaumont, Gilles Caty, and Giuseppe Liistro. 2022. "Telerehabilitation as a Form of Pulmonary Rehabilitation in Chronic Lung Disease: A Systematic Review" Healthcare 10, no. 9: 1795. https://doi.org/10.3390/healthcare10091795