
Implementation of an In-House 3D Manufacturing Unit in a Public Hospital’s Radiology Department
 , , , and
, , , and
Abstract
:1. Introduction
1.1. Clinical Utility and Indication
1.2. Economic Issues
1.3. “In-House”/Point-of-Care Manufacturing
1.4. Leading Digital Transformation
2. Materials and Methods
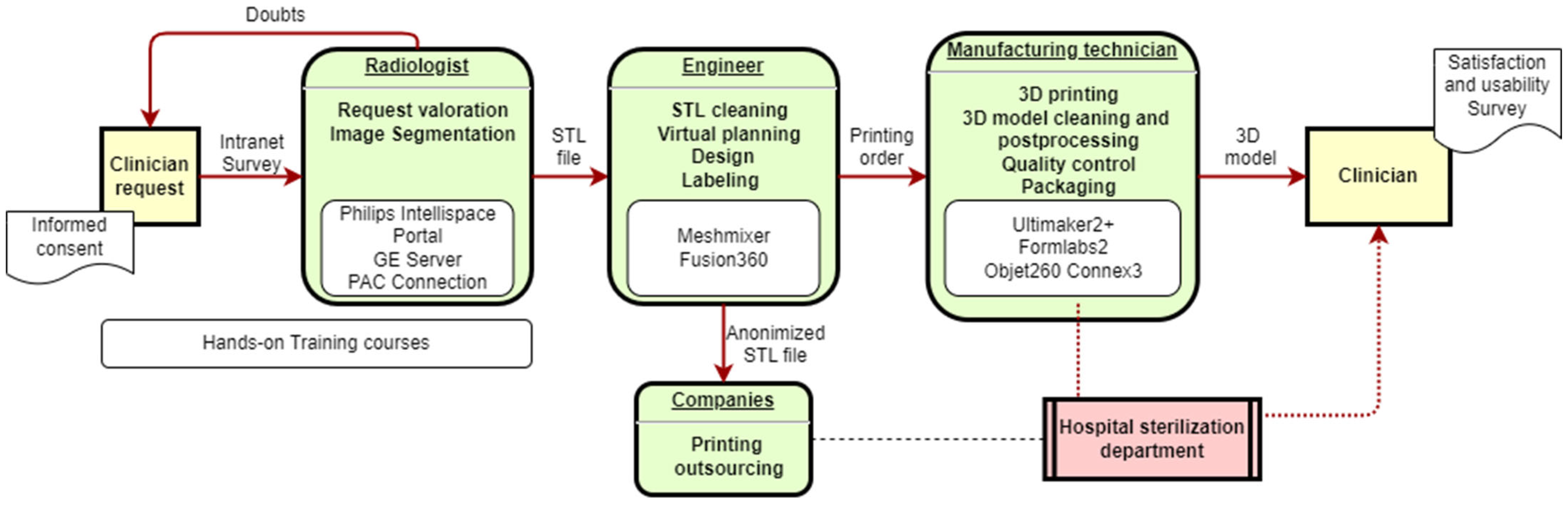
2.1. Workflow Definition
2.2. Human Resources
2.3. Segmentation Software
2.4. Online Application System
2.5. Additive Manufacturing
2.6. Quality Processes
- (i)
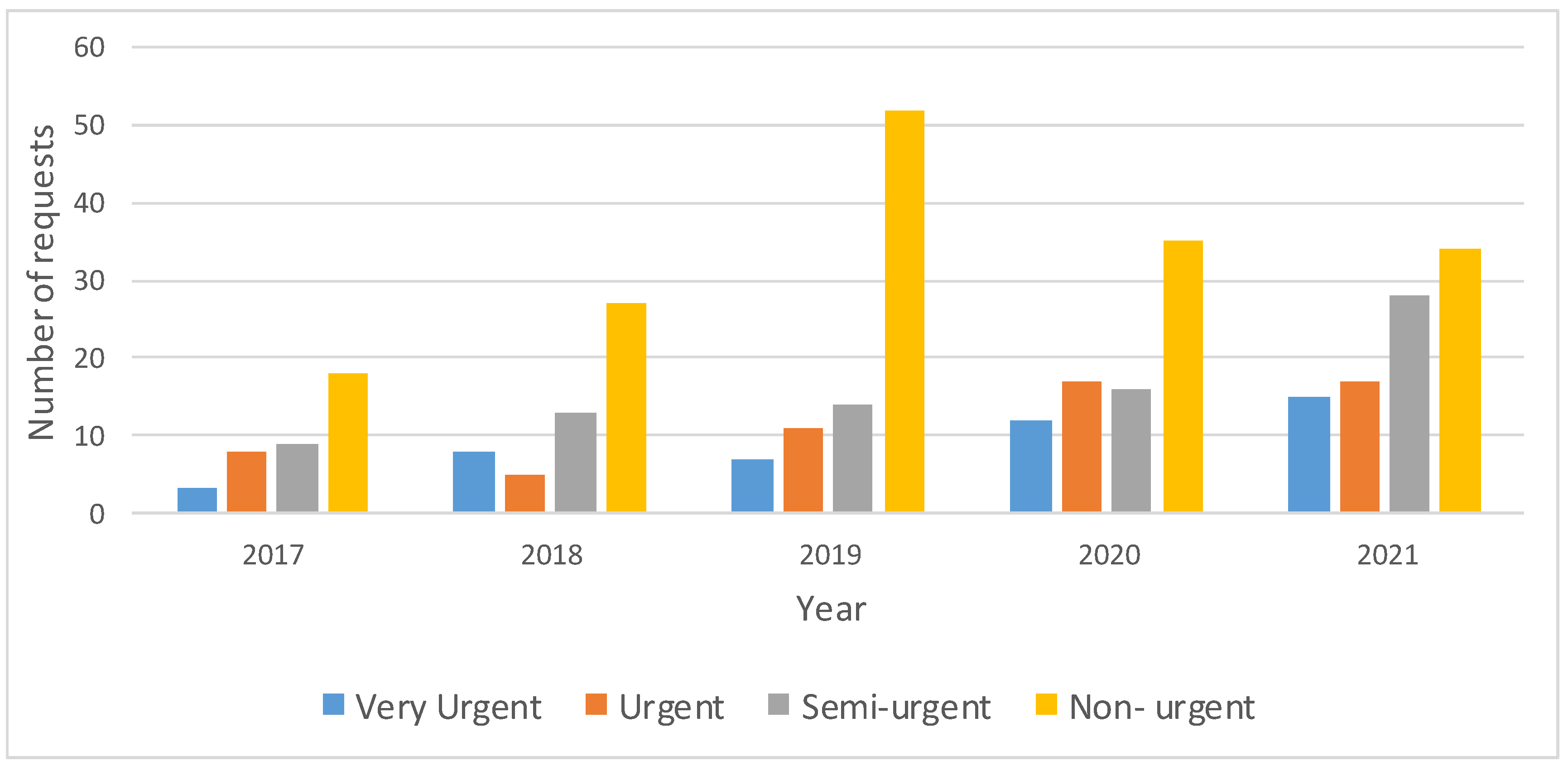
- The speed of response of the service: To analyze urgency and responsiveness, the request date, the delivery requirement date and the final delivery date were recorded.
- (ii)
- The technical quality of the products manufactured, or errors made in 3D printing: For the manufactured quality, we measured the absolute error between the physical model and the unprocessed virtual model or STL file. For each manufactured model, we took 6 dimensions (3 for each Cartesian coordinate) in both the physical model (with a digital Vernier caliper) and the virtual model (with the ®Meshmixer software; version 3.5.474, 2017 Autodesk, Inc., San Rafael, CA, USA).
2.7. Satisfaction and Usability Surveys
2.8. Costs
3. Examples of Applications
- a.
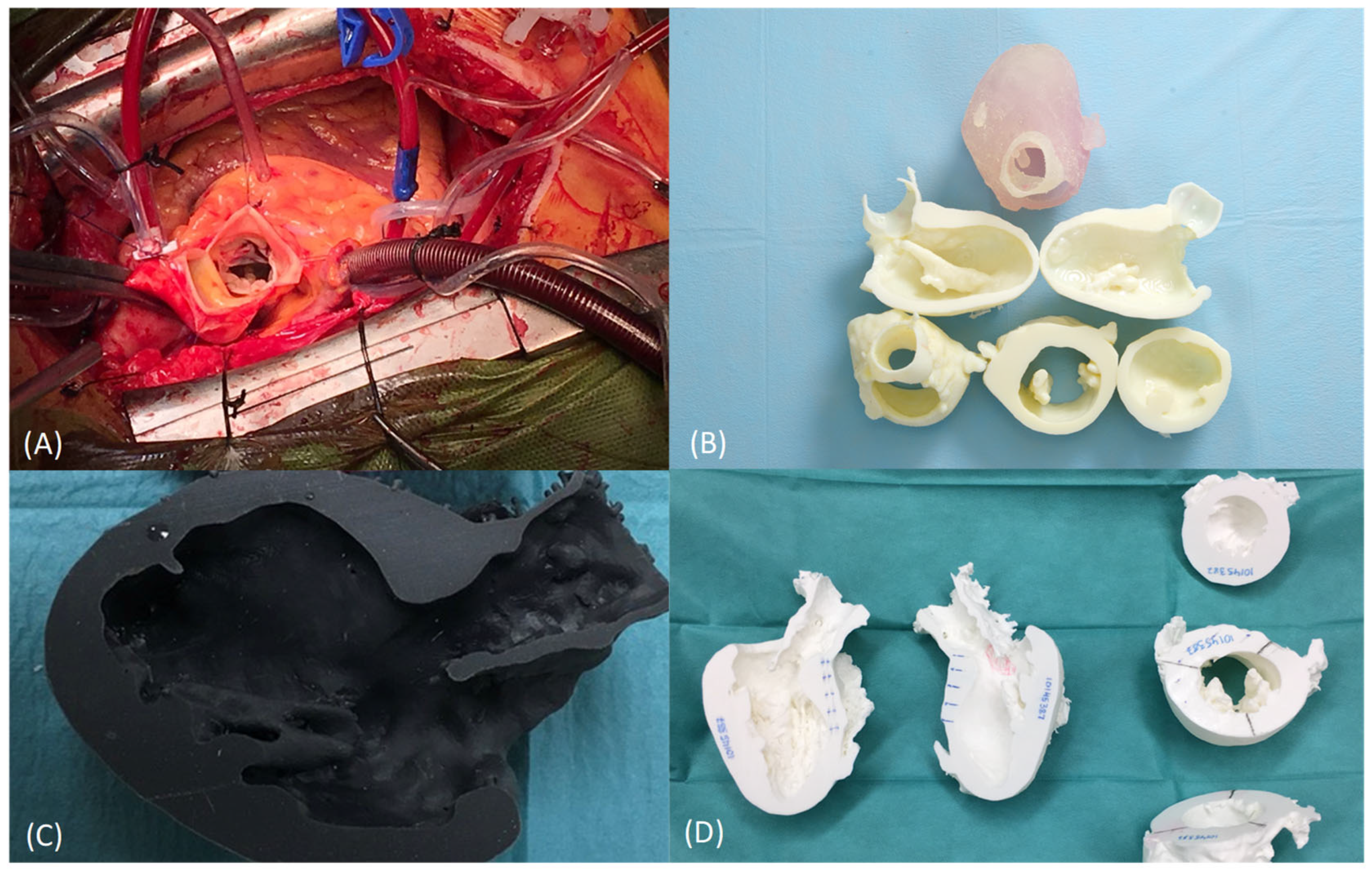
- Anatomical model for planning, training, teaching and patient communication of obstructive hypertrophic cardiomyopathy (cardiovascular surgery)
- b.
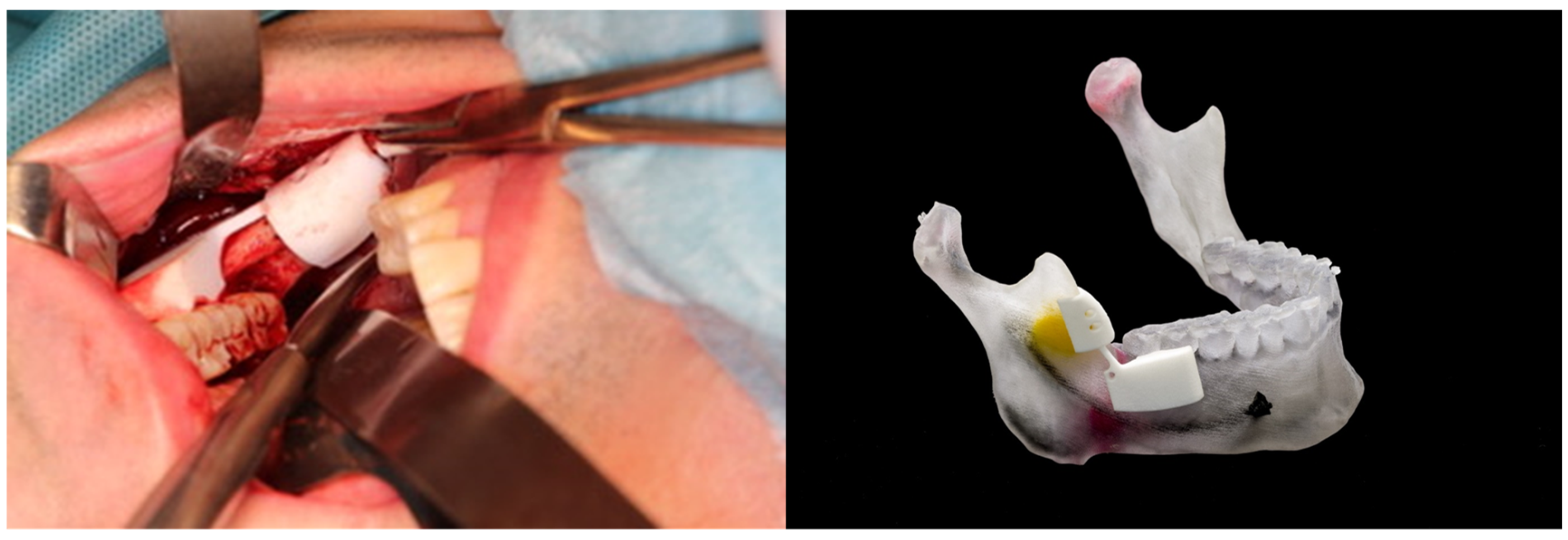
- Anatomical model and cutting guides for surgical treatment of a complex benign neoplasm (maxillofacial surgery)
- c.
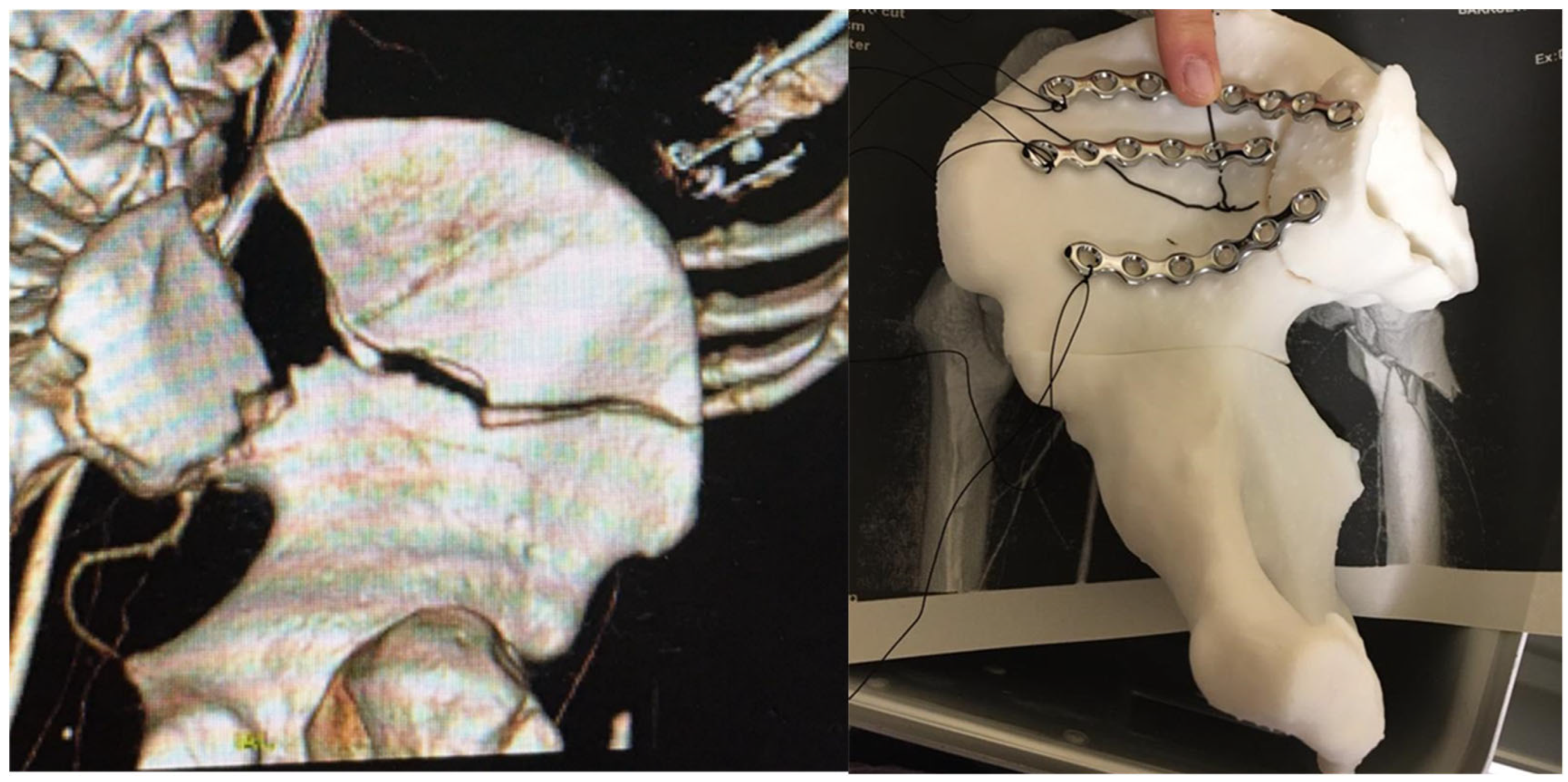
- Anatomical model for pre-modeling synthesis plates for surgical treatment of acetabular fractures (traumatological surgery)
4. Results
4.1. Training Courses
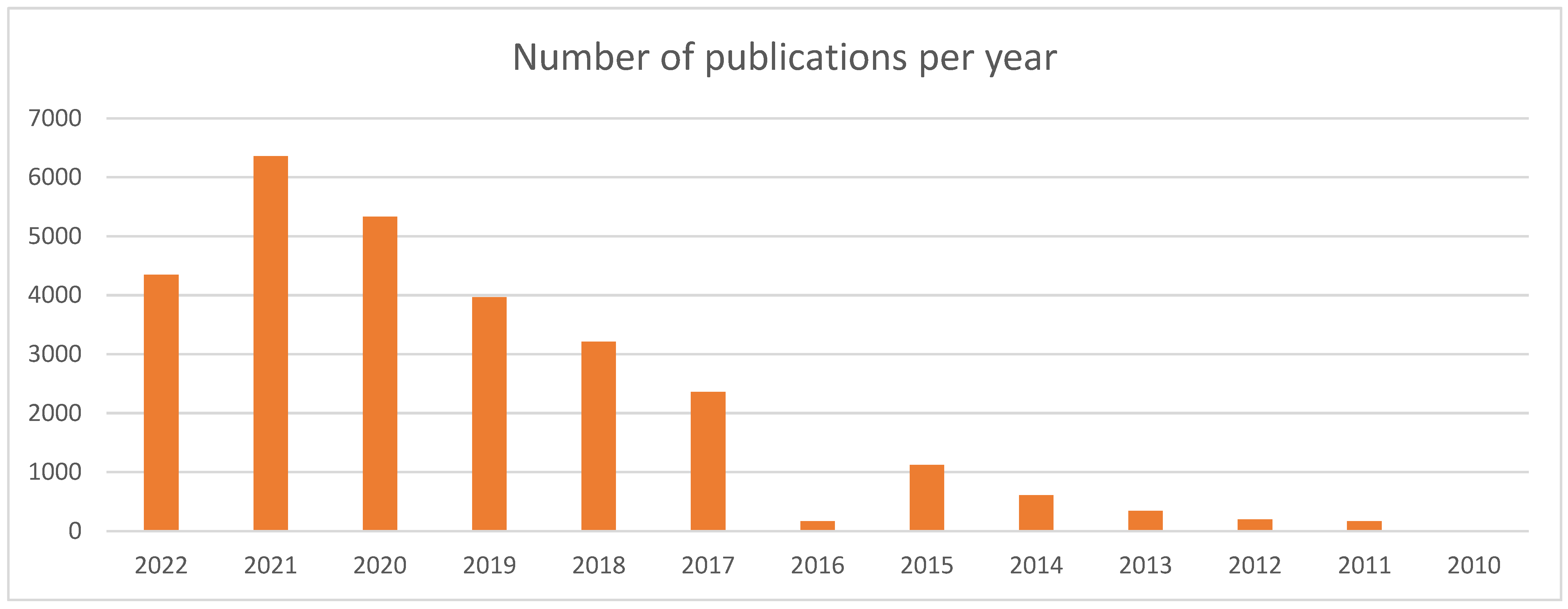
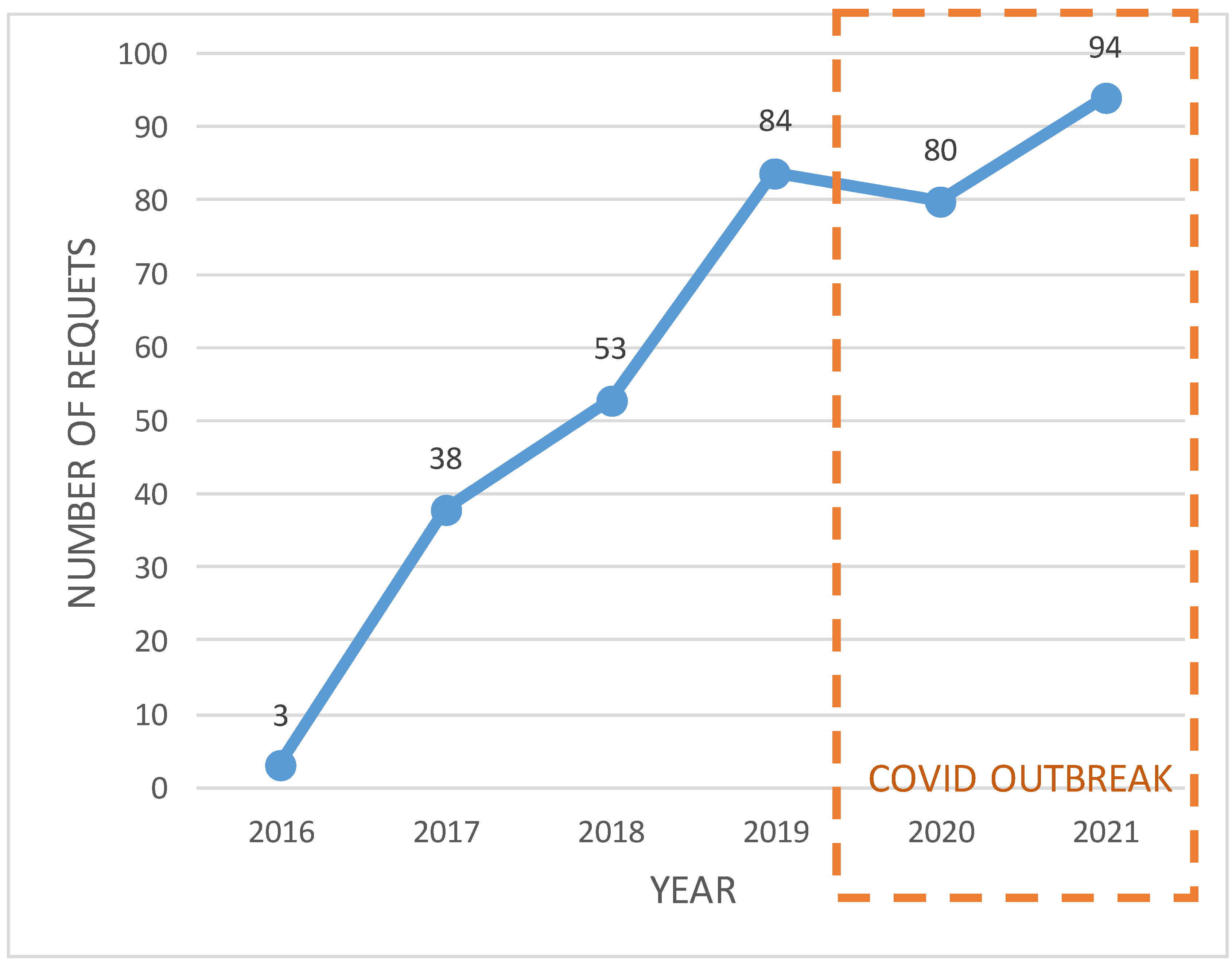
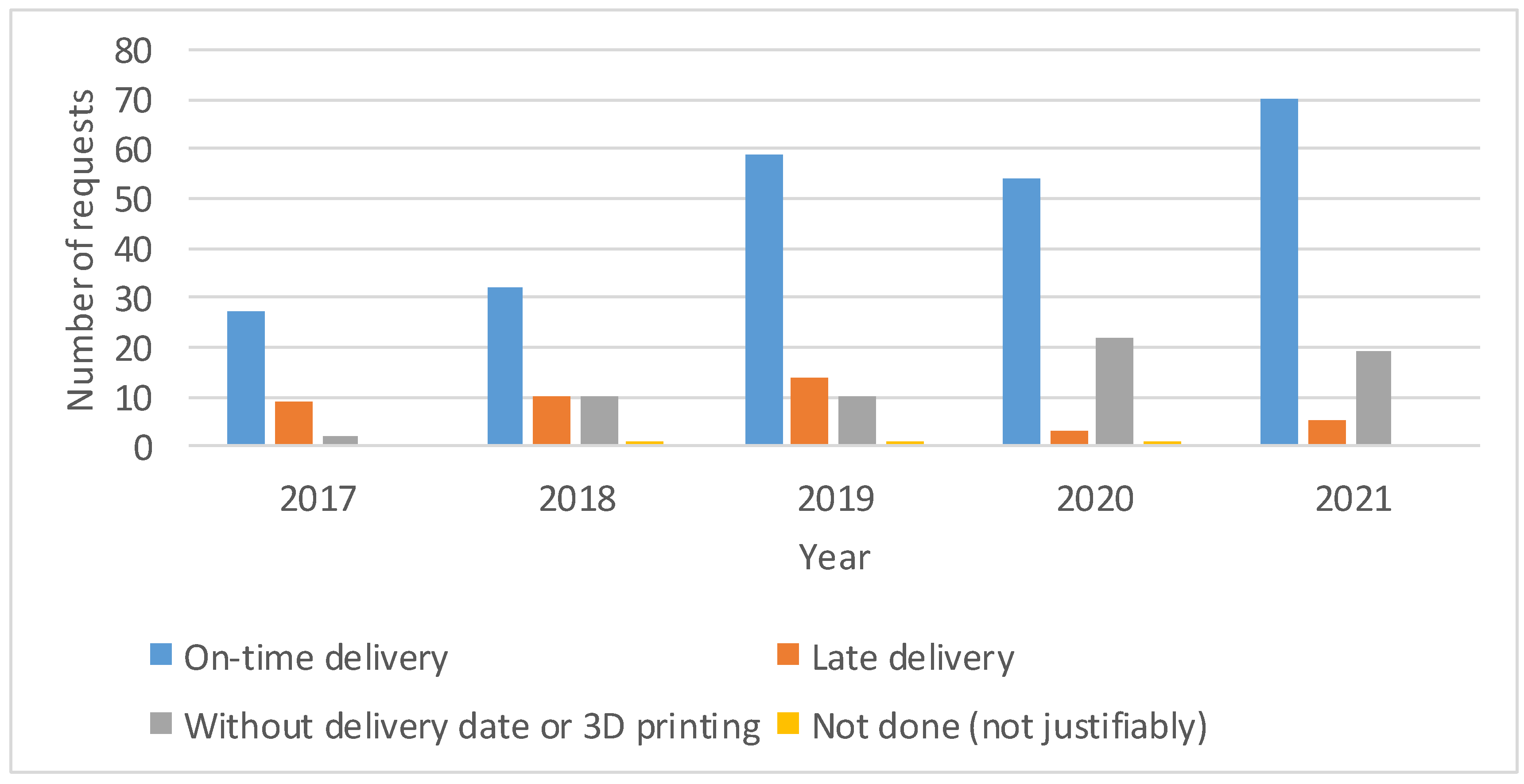
4.2. Evolution of Requests
4.3. Quality Control
4.4. Cost
4.5. Questionnaires
5. Discussion and Conclusions
5.1. Clinical Indication
5.2. In-House/Point-of-Care Manufacturing Decision
5.3. Leading Digital Transformation
5.4. Technology Investment and Cost-Effectiveness
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yang, T.; Lin, S.; Tan, T.; Yang, J.; Pan, J.; Hu, C.; Li, J.; Zou, Y. Impact of 3D Printing Technology on Comprehension of Surgical Anatomy of Retroperitoneal Tumor. World J. Surg. 2018, 42, 2339–2343. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Szary, J.; Luis, M.S.; Mikulski, S.; Patel, A.; Schulz, F.; Tretiakow, D.; Fercho, J.; Jaguszewska, K.; Frankiewicz, M.; Pawłowska, E.; et al. The Role of 3D Printing in Planning Complex Medical Procedures and Training of Medical Professionals-Cross-Sectional Multispecialty Review. Int. J. Environ. Res. Public Health 2022, 19, 3331. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Liu, D. A systematic review of clinical value of three-dimensional printing in renal disease. Quant. Imaging Med. Surg. 2018, 8, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Ballard, D.H.; Mills, P.; Duszak, R.; Weisman, J.A.; Rybicki, F.J.; Woodard, P.K. Medical 3D Printing Cost-Savings in Orthopedic and Maxillofacial Surgery: Cost Analysis of Operating Room Time Saved with 3D Printed Anatomic Models and Surgical Guides. Acad. Radiol. 2019, 27, 1103–1113. [Google Scholar] [CrossRef]
- Raza, M.; Murphy, D.; Gelfer, Y. The effect of three-dimensional (3D) printing on quantitative and qualitative outcomes in paediatric orthopaedic osteotomies: A systematic review. EFORT Open Rev. 2021, 6, 130–138. [Google Scholar] [CrossRef]
- Marconi, S.; Pugliese, L.; Botti, M.; Peri, A.; Cavazzi, E.; Latteri, S.; Auricchio, F.; Pietrabissa, A. Value of 3D printing for the comprehension of surgical anatomy. Surg. Endosc. 2017, 31, 4102–4110. [Google Scholar] [CrossRef]
- Langridge, B.; Momin, S.; Coumbe, B.; Woin, E.; Griffin, M.; Butler, P. Systematic Review of the Use of 3-Dimensional Printing in Surgical Teaching and Assessment. J. Surg. Educ. 2018, 75, 209–221. [Google Scholar] [CrossRef]
- Ryan, J.; Gregg, C.; Frakes, D.; Pophal, S. Three-dimensional printing: Changing clinical care or just a passing fad? Curr. Opin. Cardiol. 2017, 32, 86–92. [Google Scholar] [CrossRef]
- Jiang, M.; Chen, G.; Coles-Black, J.; Chuen, J.; Hardidge, A. Three-dimensional printing in orthopaedic preoperative planning improves intraoperative metrics: A systematic review. ANZ J. Surg. 2020, 90, 243–250. [Google Scholar] [CrossRef]
- Witowski, J.; Sitkowski, M.; Zuzak, T.; Coles-Black, J.; Chuen, J.; Major, P.; Pdziwiatr, M. From ideas to long-term studies: 3D printing clinical trials review. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 1473–1478. [Google Scholar] [CrossRef] [Green Version]
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H.M. Clinical efficacy and effectiveness of 3D printing: A systematic review. BMJ Open 2017, 7, e016891. [Google Scholar] [CrossRef] [PubMed]
- Chepelev, L.; Wake, N.; Ryan, J.; Althobaity, W.; Gupta, A.; Arribas, E.; Santiago, L.; Ballard, D.H.; Wang, K.C.; Weadock, W.; et al. Radiological Society of North America (RSNA) 3D printing Special Interest Group (SIG): Guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print. Med. 2018, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Am, W.P.O.C. Considerations for Point of Care (POC) 3D Printing|Thought Leadership|Knowledge|Exponent. 2019; 8–10. [Google Scholar]
- Medical Manufacturing Innovations. Physicians as Manufacturers: The Rise of Point-of-Care Manufacturing; SME: Southfield, MI, USA, 2018; p. 20. [Google Scholar]
- Christensen, A.; Rybicki, F.J. Maintaining safety and efficacy for 3D printing in medicine. 3D Print. Med. 2017, 3, 1–10. [Google Scholar] [CrossRef]
- Kim, G.B.; Lee, S.; Kim, H.; Yang, D.H.; Kim, Y.H.; Kyung, Y.S.; Kim, C.S.; Choi, S.H.; Kim, B.J.; Ha, H.; et al. Three-dimensional printing: Basic principles and applications in medicine and radiology. Korean J. Radiol. 2016, 17, 182–197. [Google Scholar] [CrossRef]
- Hoang, D.; Perrault, D.; Stevanovic, M.; Ghiassi, A. Surgical applications of three-dimensional printing: A review of the current literature & how to get started. Ann. Transl. Med. 2016, 4, 456. [Google Scholar] [CrossRef]
- Martelli, N.; Serrano, C.; Van Den Brink, H.; Pineau, J.; Prognon, P.; Borget, I.; El Batti, S. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016, 159, 1485–1500. [Google Scholar] [CrossRef]
- Bastawrous, S.; Wu, L.; Liacouras, P.C.; Levin, D.B.; Ahmed, M.T.; Strzelecki, B.; Amendola, M.F.; Lee, J.T.; Coburn, J.; Ripley, B. Establishing 3D Printing at the Point of Care: Basic Principles and Tools for Success. Radiographics 2022, 42, 451–468. [Google Scholar] [CrossRef]
- Serrano, C.; Fontenay, S.; Van Den Brink, H.; Pineau, J.; Prognon, P.; Martelli, N. Evaluation of 3D printing costs in surgery: A systematic review. Int. J. Technol. Assess. Health Care 2020, 36, 349–355. [Google Scholar] [CrossRef]
- Bongo, M.; Abellana, D.P.; Caballes, S.A.; Ancheta, R.; Himang, C.; Obiso, J.J.; Ocampo, L.; Deocaris, C. Critical success factors in implementing Industry 4.0 from an organisational point of view: A literature analysis. Int. J. Adv. Oper. Manag. 2020, 12, 273–301. [Google Scholar] [CrossRef]
- Chaudhuri, A.; Naseraldin, H.; Søberg, P.V.; Kroll, E.; Librus, M. Should hospitals invest in customised on-demand 3D printing for surgeries? Int. J. Oper. Prod. Manag. 2020, 41, 55–62. [Google Scholar] [CrossRef]
- Hatamleh, M.M.; Ong, J.; Hatamleh, Z.M.; Watson, J.; Huppa, C. Developing an In-house Interdisciplinary Three-Dimensional Service. J. Craniofac. Surg. 2018, 29, 1. [Google Scholar] [CrossRef]
- Pugliese, L.; Marconi, S.; Negrello, E.; Mauri, V.; Peri, A.; Gallo, V.; Auricchio, F.; Pietrabissa, A. The clinical use of 3D printing in surgery. Updates Surg. 2018, 70, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Beitler, B.G.; Abraham, P.F.; Glennon, A.R.; Tommasini, S.M.; Lattanza, L.L.; Morris, J.M.; Wiznia, D.H. Interpretation of regulatory factors for 3D printing at hospitals and medical centers, or at the point of care. 3D Print Med. 2022, 8, 7. [Google Scholar] [CrossRef]
- Venchiarutti, R.L.; Clark AM, J.R.; Dusseldorp, J.R.; Cheng, K.; Howes, D.; Fleming, S.; Maddern, G.J.; Mukherjee, P. New regulatory changes in 3D printing: Implementation in surgery and research at the point of care. ANZ J. Surg. 2021, 91, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Tino, R.; Yeo, A.; Leary, M.; Brandt, M.; Kron, T. A systematic review on 3D-Printed imaging and dosimetry phantoms in radiation therapy. Technol. Cancer Res. Treat. 2019, 18, 1–14. [Google Scholar] [CrossRef]
- Waterson, P.; Hoonakker, P.L.T.; Carayon, P. Special issue on human factors and the implementation of health information technology (HIT): Comparing approaches across nations. Int. J. Med. Inform. 2013, 82, 277–280. [Google Scholar] [CrossRef]
- Sligo, J.; Gauld, R.; Roberts, V.; Villa, L. A literature review for large-scale health information system project planning, implementation and evaluation. Int. J. Med. Inform. 2017, 97, 86–97. [Google Scholar] [CrossRef]
- Matsumoto, J.S.; Morris, J.M.; Foley, T.A.; Williamson, E.E.; Leng, S.; McGee, K.P.; Kuhlmann, J.L.; Nesberg, L.E.; Vrtiska, T.J. Three-dimensional Physical Modeling: Applications and Experience at Mayo Clinic. RadioGraphics 2015, 35, 1989–2006. [Google Scholar] [CrossRef]
- Powell, B.J.; Waltz, T.J.; Chinman, M.J.; Damschroder, L.J.; Smith, J.L.; Matthieu, M.M.; Proctor, E.K.; Kirchner, J.A.E. A refined compilation of implementation strategies: Results from the Expert Recommendations for Implementing Change (ERIC) project. Implement. Sci. 2015, 10, 1–14. [Google Scholar] [CrossRef]
- Sampietro-Colom, L.; Lach, K.; Pasternack, I.; Wasserfallen, J.B.; Cicchetti, A.; Marchetti, M.; Kidholm, K.; Arentz-Hansen, H.; Rosenmöller, M.; Wild, C.; et al. Guiding principles for good practices in hospital-based health technology assessment units. Int. J. Technol. Assess. Health Care 2016, 31, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Hirst, A.; Philippou, Y.; Blazeby, J.; Campbell, B.; Campbell, M.; Feinberg, J.; Rovers, M.; Blencowe, N.; Pennell, C.; Quinn, T.; et al. No Surgical Innovation Without Evaluation: Evolution and Further Development of the IDEAL Framework and Recommendations. Ann. Surg. 2019, 269, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Technical Considerations for Additive Manufactured Medical Devices: Guidance for Industry and Food and Drug Administration Staff Document; Food and Drug Administration: Rockville, MD, USA, 2017; ISBN 9788578110796.
- Zheng, Y.X.; Yu, D.F.; Zhao, J.G.; Wu, Y.L.; Zheng, B. 3D Printout Models vs. 3D-Rendered Images: Which Is Better for Preoperative Planning? J. Surg. Educ. 2016, 73, 518–523. [Google Scholar] [CrossRef]
- Bagaria, V.; Chaudhary, K. A paradigm shift in surgical planning and simulation using 3Dgraphy: Experience of first 50 surgeries done using 3D-printed biomodels. Injury 2017, 48, 2501–2508. [Google Scholar] [CrossRef]
- Guo, H.C.; Wang, Y.; Dai, J.; Ren, C.W.; Li, J.H.; Lai, Y.Q. Application of 3D printing in the surgical planning of hypertrophic obstructive cardiomyopathy and physician-patient communication: A preliminary study. J. Thorac. Dis. 2018, 10, 867–873. [Google Scholar] [CrossRef]
- Nayyer, N.V.; Macluskey, M.; Keys, W. Odontogenic cysts—An overview. Dent. Update 2015, 42, 548–555. [Google Scholar] [CrossRef]
- Ghai, S.; Sharma, Y.; Jain, N.; Satpathy, M.; Pillai, A.K. Use of 3-D printing technologies in craniomaxillofacial surgery: A review. Oral Maxillofac. Surg. 2018, 22, 249–259. [Google Scholar] [CrossRef]
- Tu, D.P.; Yu, Y.K.; Liu, Z.; Zhang, W.K.; Fan, X.; Xu, C. Three-dimensional printing combined with open reduction and internal fixation versus open reduction and internal fixation in the treatment of acetabular fractures:A systematic review and meta-analysis. Chin. J. Traumatol. 2021, 24, 159–168. [Google Scholar] [CrossRef]
- Wang, J.; Wang, X.; Wang, B.; Xie, L.; Zheng, W.; Chen, H.; Cai, L. Comparison of the feasibility of 3D printing technology in the treatment of pelvic fractures: A systematic review and meta-analysis of randomized controlled trials and prospective comparative studies. Eur. J. Trauma Emerg. Surg. 2020, 47, 1699–1712. [Google Scholar] [CrossRef]
- Beer, N.; Kaae, S.; Genina, N.; Sporrong, S.K.; Alves, T.L.; Hoebert, J.; de Bruin, M.L.; Hegger, I. Magistral Compounding with 3D Printing: A Promising Way to Achieve Personalized Medicine. Ther. Innov. Regul. Sci. 2022. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Chen, Y.; Cai, W.; Cheng, M.; Yan, W.; Huang, W. Computer-Aided Design and 3D Printing of Hemipelvic Endoprosthesis for Personalized Limb-Salvage Reconstruction after Periacetabular Tumor Resection. Bioengineering 2022, 9, 400. [Google Scholar] [CrossRef] [PubMed]
- Arce, K.; Morris, J.M.; Alexander, A.E.; Ettinger, K.S. Developing a Point-of-Care Manufacturing Program for Craniomaxillofacial Surgery. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2020, 28, 165–179. [Google Scholar] [CrossRef]
- Zarean, P.; Zarean, P.; Thieringer, F.M.; Mueller, A.A.; Kressmann, S.; Erismann, M.; Sharma, N.; Benitez, B.K. A Point-of-Care Digital Workflow for 3D Printed Passive Presurgical Orthopedic Plates in Cleft Care. Children 2022, 9, 1261. [Google Scholar] [CrossRef] [PubMed]
- Frizziero, L.; Santi, G.M.; Liverani, A.; Giuseppetti, V.; Trisolino, G.; Maredi, E.; Stilli, S. Paediatric orthopaedic surgery with 3D printing: Improvements and cost reduction. Symmetry 2019, 11, 1317. [Google Scholar] [CrossRef]
- Dorweiler, B.; Elisabeth, P.; Chaban, R.; Ghazy, A.; Salem, O. Quality Control in 3D Printing: Accuracy Analysis of 3D-Printed Models of Patient-Specific Anatomy. Materials 2021, 14, 1021. [Google Scholar] [CrossRef]
- Mitsouras, D.; Liacouras, P.; Imanzadeh, A.; Giannopoulos, A.A.; Cai, T.; Kumamaru, K.K.; George, E.; Wake, N.; Caterson, E.J.; Pomahac, B.; et al. Medical 3D Printing for the Radiologist. RadioGraphics 2015, 35, 1965–1988. [Google Scholar] [CrossRef]
- Guo, C.; Su, S.; Choo, K.K.R.; Tang, X. A Fast Nearest Neighbor Search Scheme over Outsourced Encrypted Medical Images. IEEE Trans. Ind. Inform. 2021, 17, 514–523. [Google Scholar] [CrossRef]
- Tursunbayeva, A. Human resource technology disruptions and their implications for human resources management in healthcare organizations. BMC Health Serv. Res. 2019, 19, 268. [Google Scholar] [CrossRef]
- Waqas, M.; Mokin, M.; Lim, J.; Vakharia, K.; Springer, M.E.; Meess, K.M.; Ducharme, R.W.; Ionita, C.N.; Nagesh, S.V.S.; Gutierrez, L.C.; et al. Design and physical properties of 3-dimensional printed models used for neurointervention: A systematic review of the literature. Neurosurgery 2020, 87, E445–E453. [Google Scholar] [CrossRef]
- Pamias-romero, J.; Masnou-pratdesaba, J.; Manel, S. Personalized Surgery Service in a Tertiary Hospital: A Method to Increase Effectiveness, Precision, Safety and Quality in Maxillofacial Surgery Using Custom-Made 3D Prostheses and Implants. J. Clin. Med. 2022, 11, 4791. [Google Scholar] [CrossRef] [PubMed]
- Culmone, C.; Smit, G.; Breedveld, P. Additive manufacturing of medical instruments: A state-of-the-art review. Addit. Manuf. 2019, 27, 461–473. [Google Scholar] [CrossRef]
- Zoabi, A.; Redenski, I.; Oren, D.; Kasem, A.; Zigron, A.; Daoud, S.; Moskovich, L.; Kablan, F.; Srouji, S. 3D Printing and Virtual Surgical Planning in Oral and Maxillofacial Surgery. J. Clin. Med. 2022, 11, 2385. [Google Scholar] [CrossRef] [PubMed]
- Guttridge, C.; Shannon, A.; O’Sullivan, A.; O’Sullivan, K.J.; O’Sullivan, L.W. Biocompatible 3D printing resins for medical applications: A review of marketed intended use, biocompatibility certification, and post-processing guidance. Ann. 3D Print. Med. 2022, 5, 100044. [Google Scholar] [CrossRef]
- Witowski, J.S.; Coles-Black, J.; Zuzak, T.Z.; Pȩdziwiatr, M.; Chuen, J.; Major, P.; Budzyński, A. 3D Printing in Liver Surgery: A Systematic Review. Telemed. e-Health 2017, 23, 943–947. [Google Scholar] [CrossRef]
- Ravi, P.; Burch, M.B.; Farahani, S.; Chepelev, L.L.; Yang, D.; Ali, A.; Joyce, J.R.; Wang, K.C.; Mahoney, M.C.; Kondor, S. Utility and Costs During the Initial Year of 3-D Printing in an Academic Hospital. J. Am. Coll. Radiol. 2022; in press. [Google Scholar] [CrossRef]
- Jacobs, G.; van der Zijpp, T.; van Lieshout, F.; van Dulmen, S. Research into person-centred healthcare technology: A plea for considering humanization dimensions. In Person-Centred Healthcare Research; Wiley: Hoboken, NJ, USA, 2017; pp. 61–68. [Google Scholar]
- Micallef, J.; Broekhuyse, A.; Vuyyuru, S.; Wax, R.; Sridhar, S.K.; Heath, J.; Dubrowski, A. Application of 3D Printing in Training Health Care Providers; the Development of Diverse Facial Overlays for Simulation-Based Medical Training. Cureus 2022, 14, e26637. [Google Scholar] [CrossRef]
- Sarkis, J.; Cohen, M.J.; Dewick, P.; Schröder, P. A brave new world: Lessons from the COVID-19 pandemic for transitioning to sustainable supply and production. Resour. Conserv. Recycl. 2020, 159, 104894. [Google Scholar] [CrossRef]
- Zeller, A.N.; Goetze, E.; Thiem, D.G.E.; Bartella, A.K.; Seifert, L.; Beiglboeck, F.M.; Kröplin, J.; Hoffmann, J.; Pabst, A. A survey regarding the organizational aspects and quality systems of in-house 3D printing in oral and maxillofacial surgery in Germany. Oral Maxillofac. Surg. 2022; online ahead of print. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Usage | Times | Times/Total Cases |
|---|---|---|
| Surgical Planning | 190 | 54% |
| Surgical Training | 125 | 36% |
| Premolding of osteosynthesis plates | 82 | 23% |
| Guidance/support during surgery | 91 | 26% |
| Teaching | 85 | 24% |
| Patient communication | 90 | 26% |
| Others | 65 | 18% |
| Technology | Number of Cases | Number of Measures | Error Mean ± Sd |
|---|---|---|---|
| FDM | 52 | 468 | 1.94 ± 0.05% |
| SLA | 29 | 259 | 2.88 ± 0.06% |
| MJ | 33 | 297 | 2.73 ± 0.03% |
| Anatomy | Material Costs | Machine Time | Machine Cost (Amortization) | Total Cost | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FDM | SLA | MJ | FDM | SLA | MJ | FDM | SLA | MJ | FDM | SLA | MJ | |
| Mandible | EUR 0.70 | EUR 11.60 | EUR 58.10 | 4.6 h | 5.5 h | 6.1 h | EUR 1.10 | EUR 2.37 | EUR 88.88 | EUR 1.80 | EUR 13.97 | EUR 146.98 |
| Hemipelvis | EUR 5.70 | EUR 51.90 | EUR 379 | 40.3 h | 19.8 h | 18.7 h | EUR 9.67 | EUR 8.51 | EUR 272.46 | EUR 15.37 | EUR 60.41 | EUR 651.46 |
| Heart (1 chamber) | EUR 3.30 | EUR 74.00 | EUR 183 | 20.4 h | 16.6 h | 5.2 h | EUR 4.90 | EUR 7.14 | EUR 75.76 | EUR 8.20 | EUR 81.14 | EUR 258.76 |
| Anatomy Model | Radiologist | Engineer | Manufacturing Technician | Human Resources Costs |
|---|---|---|---|---|
| Bone | 30 min | 30 min | 50 min | EUR 70.96 |
| Bone with mass | 40 min | 30 min | 50 min | EUR 81.46 |
| Visceral masses | 180 min | 30 min | 50 min | EUR 228.41 |
| Heart | 150 min | 40 min | 50 min | EUR 202.92 |
| Vascular anatomy | 45 min | 30 min | 50 min | EUR 86.70 |
| Trachea | 45 min | 30 min | 50 min | EUR 86.70 |
| Question | Mean ± SD |
|---|---|
| 1. Have you used the 3D model for pre-planning the surgery? (Y = 25) | |
| 1.1. The printed model has provided me with relevant information that the digital model had not offered me. | 4.36 ± 0.95 |
| 1.2. Surgical preparation using the model has had a positive effect on the final surgical outcome. | 4.32 ± 0.95 |
| 1.3. The surgical approach has been modified after examination of the 3D model. | 2.92 ± 1.32 |
| 1.4. The surgical instruments have been modified after examination of the 3D model. | 2.28 ± 1.46 |
| 1.5. 3D models should be part of the planning for this pathology as a “gold standard” process. | 4.04 ± 1.14 |
| 2. Have you used the 3D model as a communication support with the patient? (Y = 13) | |
| 2.1. The patient/guardian has been more receptive/collaborative after explaining the pathology with their personalized 3D model. | 4.15 ± 1.35 |
| 2.2. The patient/guardian has shown interest in keeping the 3D model. | 2.08 ± 1.49 |
| 2.3. The 3D model has contributed to a better understanding of the intervention by the patient/guardian compared to other tools or drawings. | 4.08 ± 1.31 |
| 2.4. The patient has been reassured to know that the surgery is being customized through a 3D model. | 3.69 ± 1.50 |
| 3. Have you used the model during the surgery? (Y = 15) | |
| 3.1. The 3D model has made it possible to avoid unforeseen events/complications during the operation. | 3.93 ± 1.54 |
| 3.2. The 3D model has facilitated communication with colleagues. | 4.73 ± 1.26 |
| 3.3. The 3D model has increased the confidence of the clinical team during the surgery. | 4.33 ± 1.34 |
| 3.4. Having the 3D model in the operating theatre has proved useful. | 4.60 ± 1.25 |
| 4. After the surgery I consider that: (Y = 28) | |
| 4.1. The operation time was shorter than usual for this type of pathology | 3.32 ± 1.47 |
| 4.2. The 3D model represents the anatomical area as observed during the operation. | 4.39 ± 0.99 |
| 4.3. The same model on a smaller scale would have sufficient for the same purpose. | 1.43 ± 0.88 |
| 4.4. The virtual model (3D PDF file) would have been sufficient for the same purpose. | 1.68 ± 1.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, R.I.; Jauregui, I.; del Amo, C.; Gandiaga, A.; Rodriguez, O.; Margallo, L.; Voces, R.; Martin, N.; Gallego, I.; Minguez, R.; et al. Implementation of an In-House 3D Manufacturing Unit in a Public Hospital’s Radiology Department. Healthcare 2022, 10, 1791. https://doi.org/10.3390/healthcare10091791
García RI, Jauregui I, del Amo C, Gandiaga A, Rodriguez O, Margallo L, Voces R, Martin N, Gallego I, Minguez R, et al. Implementation of an In-House 3D Manufacturing Unit in a Public Hospital’s Radiology Department. Healthcare. 2022; 10(9):1791. https://doi.org/10.3390/healthcare10091791
Chicago/Turabian StyleGarcía, Ruben I., Ines Jauregui, Cristina del Amo, Ainhoa Gandiaga, Olivia Rodriguez, Leyre Margallo, Roberto Voces, Nerea Martin, Inés Gallego, Rikardo Minguez, and et al. 2022. "Implementation of an In-House 3D Manufacturing Unit in a Public Hospital’s Radiology Department" Healthcare 10, no. 9: 1791. https://doi.org/10.3390/healthcare10091791