
Development and Implementation of an Antimicrobial Stewardship Checklist in Sub-Saharan Africa: A Co-Creation Consensus Approach

 , , , , , , , , , , , and
, , , , , , , , , , , and
Abstract
:1. Introduction
- (1)
- Our focus on Sub-Saharan Africa (specifically Tanzania, Zambia, Uganda, and Ghana) offers a further local adaptation of the materials.
- (2)
- Our unique methodological approach uses elements of co-creation through the strong involvement of local hospital representatives during a Delphi consensus procedure.
- (3)
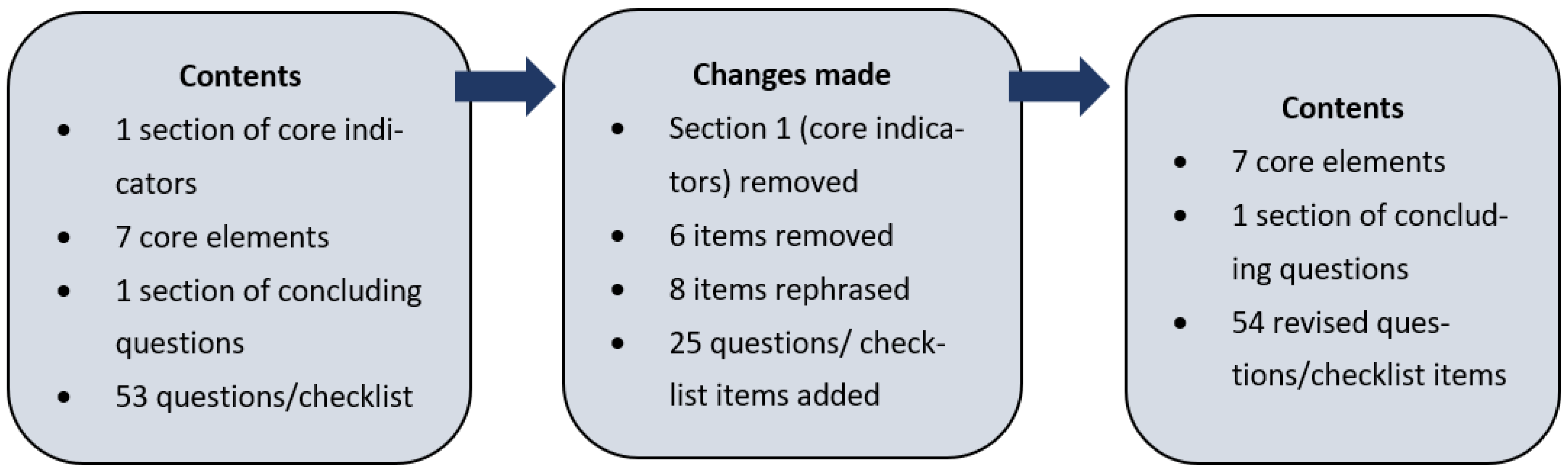
- We extended the number of checklist items to capture the more nuanced differences in the AMS elements. Additionally, we incorporate open-ended questions within the AMS checklist to allow for more reporting flexibility.
- (4)
- We provide an initial evaluation of the checklist’s effectiveness by using it to measure the outcomes of an AMS intervention programme.
2. Materials and Methods
2.1. Checklist Development
2.2. AMS Checklist Implementation across 19 Hospitals
2.3. Demographics of Study Sites
3. Results
3.1. Checklist Implementation
Quantitative Improvements Following the AMS Intervention
3.2. Development and Review of Guidelines/Policies
3.3. Raising Awareness of WHO AWaRe Categories
3.4. Other AMS Activities
3.5. Barriers to AMS Implementation
3.6. Unique Contribution of Implementing the AMS Checklist
4. Discussion
4.1. Development of the AMS Checklist
4.2. AMS Checklist Implementation
4.3. Barriers to and Opportunities for AMS Implementation
4.4. Strengths and Limitations
- (1)
- Our narrow focus on Sub-Saharan Africa (specifically Tanzania, Zambia, Uganda, and Ghana) allows for further local adaptation of the materials.
- (2)
- Our unique methodological approach uses elements of co-creation through the strong involvement of local hospital representatives during a Delphi consensus procedure.
- (3)
- We extended the number of checklist items to capture the more nuanced differences in the AMS elements. Additionally, we incorporate open-ended questions within the AMS checklist to allow for more reporting flexibility.
- (4)
- We provide an initial evaluation of the checklist’s effectiveness by using it to measure the outcomes of an AMS intervention programme.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015; Available online: http://www.who.int/antimicrobial-resistance/publications/global-action-plan/en/ (accessed on 20 December 2021).
- Davey, P.; A Marwick, C.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2017, CD003543. [Google Scholar] [CrossRef]
- Charani, E.; Holmes, A.H. Antimicrobial stewardship programmes: The need for wider engagement. BMJ Qual. Saf. 2013, 22, 885–887. [Google Scholar] [PubMed]
- Charani, E.; Holmes, A. Antibiotic Stewardship—Twenty Years in the Making. Antibiotics 2019, 8, 7. [Google Scholar]
- CDC. Core Elements of Hospital Antibiotic Stewardship Programs|Get Smart for Healthcare|CDC. Centers for Disease Control and Prevention. 2016; pp. 1–25. Available online: https://www.cdc.gov/antibiotic-use/healthcare/implementation/core-elements.html (accessed on 20 December 2021).
- GOV.UK. Tackling Antimicrobial Resistance 2019–2024: The UK’s Five-Year National Action Plan. 2019. Available online: https://www.gov.uk/government/publications/uk-5-year-action-plan-for-antimicrobial-resistance-2019-to-2024 (accessed on 20 December 2021).
- Goff, D.A.; Ashiru-Oredope, D.; Cairns, K.A.; Eljaaly, K.; Gauthier, T.P.; Langford, B.J.; Mahmoud, S.F.; Messina, A.P.; Michael, U.C.; Saad, T.; et al. Global contributions of pharmacists during the COVID-19 pandemic. J. Am. Coll. Clin. Pharm. 2020, 3, 1480–1492. [Google Scholar] [CrossRef] [PubMed]
- Kerr, F.; Sefah, I.; Essah, D.; Cockburn, A.; Afriyie, D.; Mahungu, J.; Mirfenderesky, M.; Ankrah, D.; Aggor, A.; Barrett, S.; et al. Practical Pharmacist-Led Interventions to Improve Antimicrobial Stewardship in Ghana, Tanzania, Uganda and Zambia. Pharmacy 2021, 9, 124. [Google Scholar] [CrossRef]
- Brandish, C.; Garraghan, F.; Ng, B.; Russell-Hobbs, K.; Olaoye, O.; Ashiru-Oredope, D. Assessing the Impact of a Global Health Fellowship on Pharmacists’ Leadership Skills and Consideration of Benefits to the National Health Service (NHS) in the United Kingdom. Healthcare 2021, 9, 890. [Google Scholar] [CrossRef]
- Kpokiri, E.E.; Ladva, M.; Dodoo, C.C.; Orman, E.; Aku, T.A.; Mensah, A.; Jato, J.; Mfoafo, K.A.; Folitse, I.; Hutton-Nyameaye, A.; et al. Knowledge awareness and practice with antimicrobial stewardship programmes among healthcare providers in a Ghanaian Tertiary Hospital. Antibiotics 2021, 11, 6. [Google Scholar] [CrossRef]
- Pulcini, C.; Binda, F.; Lamkang, A.S.; Trett, A.; Charani, E.; Goff, D.A.; Harbarth, S.; Hinrichsen, S.L.; Levy-Hara, G.; Mendelson, M.; et al. Developing core elements and checklist items for global hospital antimicrobial stewardship programmes: A consensus approach. Clin. Microbiol. Infect. 2019, 25, 20. [Google Scholar]
- World Health Organization. Antimicrobial Stewardship Programmes in Health-Care Facilities in Low- and Middle-Income Countries: A WHO Practical Toolkit; License: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/handle/10665/329404 (accessed on 20 December 2021).
- The Fleming Fund. Commonwealth Health Partnerships to Improve Antimicrobial Stewardship Announced! 2019. Available online: https://www.flemingfund.org/publications/commonwealth-health-partnerships-to-improve-antimicrobial-stewardship-announced/ (accessed on 20 December 2021).
- THET Partnerships for Global Health. Commonwealth Partnerships for Antimicrobial Stewardship Scheme. 2019. Available online: https://www.thet.org/our-work/grants/cwpams/ (accessed on 20 December 2021).
- Commonwealth Pharmacists Association. Commonwealth Partnerships for Antimicrobial Stewardship. 2019. Available online: https://commonwealthpharmacy.org/commonwealth-partnerships-for-antimicrobial-stewardship/ (accessed on 20 December 2021).
- GOV.UK. Funding for Commonwealth Partnerships to Improve Antimicrobial Stewardship. 2019. Available online: https://www.gov.uk/government/news/funding-for-commonwealth-partnerships-to-improve-antimicrobial-stewardship (accessed on 20 December 2021).
- McKnight, J.; Maina, M.; Zosi, M.; Kimemia, G.; Onyango, T.; Schultsz, C.; English, M.; Tosas-Auguet, O. Evaluating hospital performance in antibiotic stewardship to guide action at national and local levels in a lower-middle income setting. Glob. Health Action 2019, 12, 1761657. [Google Scholar] [CrossRef]
- Charani, E.; Castro-Sanchéz, E.; Bradley, S.; Nathwani, D.; Holmes, A.H.; Davey, P. Implementation of antibiotic stewardship in different settings–results of an international survey. Antimicrob. Resist. Infect. Control 2019, 8, 34. [Google Scholar] [CrossRef]
- Charani, E.; Castro-Sánchez, E.; Sevdalis, N.; Kyratsis, Y.; Drumright, L.; Shah, N.; Holmes, A. Understanding the determinants of antimicrobial prescribing within hospitals: The role of “Prescribing etiquete”. Clin. Infect. Dis. 2013, 57, 188–196. [Google Scholar] [CrossRef] [PubMed]
- CDC. Core Elements of Hospital Antibiotic Stewardship Programs; US Department of Health and Human Services; CDC: Atlanta, GA, USA, 2019. Available online: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html (accessed on 20 December 2021).
- Olaoye, O.; Tuck, C.; Khor, W.P.; McMenamin, R.; Hudson, L.; Northall, M.; Panford-Quainoo, E.; Asima, D.M.; Ashiru-Oredope, D. Improving Access to Antimicrobial Prescribing Guidelines in 4 African Countries: Development and Pilot Implementation of an App and Cross-Sectional Assessment of Attitudes and Behaviour Survey of Healthcare Workers and Patients. Antibiotics 2020, 9, 555. [Google Scholar] [CrossRef] [PubMed]
- Musoke, D.; Kitutu, F.; Mugisha, L.; Amir, S.; Brandish, C.; Ikhile, D.; Kajumbula, H.; Kizito, I.; Lubega, G.; Niyongabo, F.; et al. A One Health Approach to Strengthening Antimicrobial Stewardship in Wakiso District, Uganda. Antibiotics 2020, 9, 764. [Google Scholar] [CrossRef]
- Afriyie, D.K.; Sefah, I.A.; Sneddon, J.; Malcolm, W.; McKinney, R.; Cooper, L.; Kurdi, A.; Godman, B.; Seaton, R.A. Antimicrobial point prevalence surveys in two Ghanaian hospitals: Opportunities for antimicrobial stewardship. JAC-Antimicrob. Resist. 2020, 2, dlaa001. [Google Scholar] [CrossRef] [PubMed]
- Ankrah, D.; Owusu, H.; Aggor, A.; Osei, A.; Ampomah, A.; Harrison, M.; Nelson, F.; Aboagye, G.O.; Ekpale, P.; Laryea, J.; et al. Point Prevalence Survey of Antimicrobial Utilization in Ghana’s Premier Hospital: Implications for Antimicrobial Stewardship. Antibiotics 2021, 10, 1528. [Google Scholar] [CrossRef]
- D’Arcy, N.; Ashiru-Oredope, D.; Olaoye, O.; Afriyie, D.; Akello, Z.; Ankrah, D.; Asima, D.M.; Banda, D.C.; Barrett, S.; Brandish, C.; et al. Antibiotic Prescribing Patterns in Ghana, Uganda, Zambia and Tanzania Hospitals: Results from the Global Point Prevalence Survey (G-PPS) on Antimicrobial Use and Stewardship Interventions Implemented. Antibiotics 2021, 10, 1122. [Google Scholar] [CrossRef]
- Ghebrehewet, S.; Shepherd, W.; Panford-Quainoo, E.; Shantikumar, S.; Decraene, V.; Rajendran, R.; Kaushal, M.; Akuffo, A.; Ayerh, D.; Amofah, G. Implementation of a Delayed Prescribing Model to Reduce Antibiotic Prescribing for Suspected Upper Respiratory Tract Infections in a Hospital Outpatient Department, Ghana. Antibiotics 2020, 9, 773. [Google Scholar] [CrossRef]
- Kalungia, A.; Jones, A.S.C.; Lippett, S.; May, C. UK and Zambian Pharmacists Working Together: Improving Antimicrobial Stewardship and Pharmaceutical Education; International Pharmaceutical Federation (FIP) Congress: Abu Dhabi, UAE, 2019. [Google Scholar]
- Ashiru-Oredope, D.; Chan, A.H.Y.; Olaoye, O.; Rutter, V.; Babar, Z.-U.; Anderson, C.; Anderson, R.; Halai, M.; Matuluko, A.; Nambatya, W.; et al. Needs assessment and impact of COVID-19 on pharmacy professionals in 31 commonwealth countries. J. Pharm. Policy Pract. 2020, 13, 72. [Google Scholar]
- Kubai, K.D. Implementation and Barriers to Antimicrobial Stewardship Activities in Private Hospitals in Kampala, Uganda; A Case of Antimicrobial Stewardship Programmes. Ph.D. Thesis, Makerere University, Kampala, Uganda, 2021. [Google Scholar]
- Ackers, L.; Ackers-Johnson, G.; Seekles, M.; Odur, J.; Opio, S. Opportunities and challenges for improving anti-microbial stewardship in low-and middle-income countries; lessons learnt from the maternal sepsis intervention in Western Uganda. Antibiotics 2020, 9, 315. [Google Scholar] [CrossRef]
- Yevutsey, S.K.; Buabeng, K.O.; Aikins, M.; Anto, B.P.; Biritwum, R.B.; Frimodt-Møller, N.; Gyansa-Lutterodt, M. Situational analysis of antibiotic use and resistance in Ghana: Policy and regulation. BMC Public Health 2017, 17, 896. [Google Scholar] [CrossRef]
- Haldeman, M.S.; Kishimbo, P.; Seddon, M.; Sangare, A.; Mwasomola, D.; Hall, J.; Shaffer, M.; Leclair, R.; Caulder, C.; Bookstaver, P.B.; et al. Evaluation of Antimicrobial Utilization and Concordance with National Guidelines at a Tertiary Hospital in the Southern Highlands Zone of Tanzania. Am. J. Trop. Med. Hyg. 2020, 102, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Nambasa, V.; Ndagije, H.; Serwanga, A.; Manirakiza, L.; Atuhaire, J.; Nakitto, D.; Kiguba, R.; Figueras, A. Prescription of Levofloxacin and Moxifloxacin in Select Hospitals in Uganda: A Pilot Study to Assess Guideline Concordance. Antibiotics 2020, 9, 439. [Google Scholar] [CrossRef]
- Thriemer, K.; Katuala, Y.; Batoko, B.; Alworonga, J.-P.; Devlieger, H.; Van Geet, C.; Ngbonda, D.; Jacobs, J. Antibiotic prescribing in DR Congo: A knowledge, attitude and practice survey among medical doctors and students. PLoS ONE 2013, 8, e55495. [Google Scholar] [CrossRef] [Green Version]
- Quet, F.; Vlieghe, E.; Leyer, C.; Buisson, Y.; Newton, P.; Naphayvong, P.; Keoluangkhot, V.; Chomarat, M.; Longuet, C.; Steenkeste, N.; et al. Antibiotic prescription behaviours in Lao People’s Democratic Republic: A knowledge, attitude and practice survey. Bull. World Health Organ. 2015, 93, 219–227. [Google Scholar] [CrossRef]
- Tadeg, H.; Berhane, Y. Substandard and counterfeit antimicrobials: Recent trends and implications to key public health interventions in developing countries. East Afr. J. Public Health 2012, 9, 85–89. [Google Scholar]
- Kinfu, Y.; Dal Poz, M.R.; Mercer, H.; Evans, D.B. The health worker shortage in Africa: Are enough physicians and nurses being trained? Bull. World Health Organ. 2009, 87, 225–230. [Google Scholar] [CrossRef]
- Beiderbeck, D.; Frevel, N.; von der Gracht, H.A.; Schmidt, S.L.; Schweitzer, V.M. Preparing, conducting, and analyzing Delphi surveys: Cross-disciplinary practices, new directions, and advancements. MethodsX 2021, 8, 101401. [Google Scholar] [CrossRef]
- Förster, B.; von der Gracht, H. Assessing Delphi panel composition for strategic foresight—A comparison of panels based on company-internal and external participants. Technol. Forecast. Soc. Change 2013, 84, 215–229. [Google Scholar] [CrossRef]


{kind=link}
| Pre-AMS Intervention N = 14 | Post-AMS Intervention N = 14 | Percentage Difference | |||
|---|---|---|---|---|---|
| Has your hospital management formally identified AMS as a priority objective for the institution and included it in its key performance indicators? | 2 | 14% | 10 | 71% | +57% |
| Is there dedicated, sustainable and sufficient budgeted financial support for AMS activities (e.g., support for salary, training, or IT (information technology) support)? | 1 | 7% | 3 | 21% | +14% |
| Does your hospital have a formal organisational multidisciplinary structure responsible for AMS? | 3 | 21% | 14 | 100% | +79% |
| Does your hospital have a dedicated committee focussed on antimicrobial use? | 2 | 14% | 8 | 57% | +43% |
| Is there a healthcare professional identified as a leader for AMS activities at your hospital and responsible for implementing the programme? | 4 | 29% | 12 | 86% | +57% |
| Is a multidisciplinary AMS team available at your hospital (e.g., greater than one trained staff member supporting clinical decisions to ensure appropriate antimicrobial use) to implement your stewardship strategy? | 1 | 7% | 10 | 71% | +64% |
| Are clinicians, nurses or pharmacists, other than those part of the AMS team (e.g., from the ICU, Internal Medicine and Surgery) involved in the AMS committee? | 1 | 7% | 9 | 64% | +57% |
| Do you have access to laboratory/imaging services to be able to support the diagnosis of the most common infections at your hospital? | 8 | 57% | 9 | 64% | +7% |
| Are the results available in a timely manner to be able to support diagnosis of most common infections? | 3 | 21% | 6 | 43% | +22% |
| In your hospital are there, or do you have access to healthcare professionals in infection management and stewardship willing to constitute an antimicrobial stewardship team? | 9 | 64% | 12 | 86% | +22% |
| Does your hospital offer access to educational resources to support staff training on how to optimise antimicrobial prescribing? | 2 | 14% | 6 | 43% | +29% |
| Does your hospital monitor the quantity of antimicrobials prescribed/dispensed/purchased at the unit and/or hospital wide level? | 5 | 36% | 9 | 64% | +28% |
| Does your stewardship programme monitor compliance with one or more of the specific interventions put in place by the stewardship team (e.g., indication captured in the medical record for all antimicrobial prescriptions, or antibiotic prescribed follows hospital guidelines)? | 1 | 7% | 7 | 50% | +43% |
| Has your hospital conducted a point prevalence survey (PPS) for antimicrobial use in the last year? | 1 | 7% | 11 | 79% | +72% |
| Are hospital-specific reports on the quantity of antimicrobials prescribed/dispensed/purchased shared with/fed back to prescribers? | 3 | 21% | 7 | 50% | +29% |
| Does your stewardship programme share facility-specific reports on antibiotic susceptibility rates with prescribers? | 3 | 21% | 5 | 36% | +15% |
| Are results of audits/reviews of the quality/appropriateness of antimicrobial use communicated directly with prescribers? | 1 | 7% | 7 | 50% | +43% |
| Does your hospital have available and up-to-date recommendations for infection management (diagnosis, prevention and treatment)? | 7 | 50% | 10 | 71% | +21% |
| Do you have any published AMS protocols e.g., restricted antimicrobial list, IV to oral policy (that have been ratified for use within your organisation)? | 0 | 0% | 5 | 36% | +36% |
| Do you have any published Infection Prevention and Control protocols e.g., hand hygiene, WASH (that have been ratified for use in your health institution)? | 7 | 50% | 12 | 86% | +36% |
| Are there regular infection and antimicrobial prescribing focused ward rounds in specific departments in your hospital? | 0 | 0% | 3 | 21% | +21% |
| Does the organisation have local/hospital specific antimicrobial prescribing guidelines? This may be included as part of a wider drug formulary. | 3 | 21% | 7 | 50% | +29% |
| AMS Team Members | Pre-AMS Intervention | Post-AMS Intervention | Total Increase Post-Intervention |
|---|---|---|---|
| Pharmacists | 3 | 13 | 10 |
| Nurses | 3 | 14 | 11 |
| Clinicians | 3 | 11 | 8 |
| Infectious Disease doctors | 2 | 6 | 4 |
| Surgeons | 0 | 6 | 6 |
| Clinical microbiologists | 1 | 2 | 1 |
| Laboratory microbiologists | 0 | 9 | 9 |
| ITU consultants | 0 | 0 | 0 |
| Data analysts | 1 | 3 | 2 |
| Infection control staff | 2 | 7 | 5 |
| Priority | Top 5 Barriers to AMS Selected by Participants Pre- and Post-CwPAMS Intervention (Pre-AMS Intervention) |
|---|---|
| 1 | Lack of funding |
| 2 | Insufficient microbiology lab capacity |
| 3 | Qualified personnel do not have enough time to perform stewardship |
| 4 | Inadequate use of the microbiology laboratory |
| 5 | Lack of motivated or engaged staff |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashiru-Oredope, D.; Garraghan, F.; Olaoye, O.; Krockow, E.M.; Matuluko, A.; Nambatya, W.; Babigumira, P.A.; Tuck, C.; Amofah, G.; Ankrah, D.; et al. Development and Implementation of an Antimicrobial Stewardship Checklist in Sub-Saharan Africa: A Co-Creation Consensus Approach. Healthcare 2022, 10, 1706. https://doi.org/10.3390/healthcare10091706
Ashiru-Oredope D, Garraghan F, Olaoye O, Krockow EM, Matuluko A, Nambatya W, Babigumira PA, Tuck C, Amofah G, Ankrah D, et al. Development and Implementation of an Antimicrobial Stewardship Checklist in Sub-Saharan Africa: A Co-Creation Consensus Approach. Healthcare. 2022; 10(9):1706. https://doi.org/10.3390/healthcare10091706
Chicago/Turabian StyleAshiru-Oredope, Diane, Frances Garraghan, Omotayo Olaoye, Eva M. Krockow, Ayodeji Matuluko, Winnie Nambatya, Peter Ahabwe Babigumira, Chloe Tuck, George Amofah, Daniel Ankrah, and et al. 2022. "Development and Implementation of an Antimicrobial Stewardship Checklist in Sub-Saharan Africa: A Co-Creation Consensus Approach" Healthcare 10, no. 9: 1706. https://doi.org/10.3390/healthcare10091706