


Association between Alexithymia and Depression among King Khalid University Medical Students: An Analytical Cross-Sectional Study


Abstract
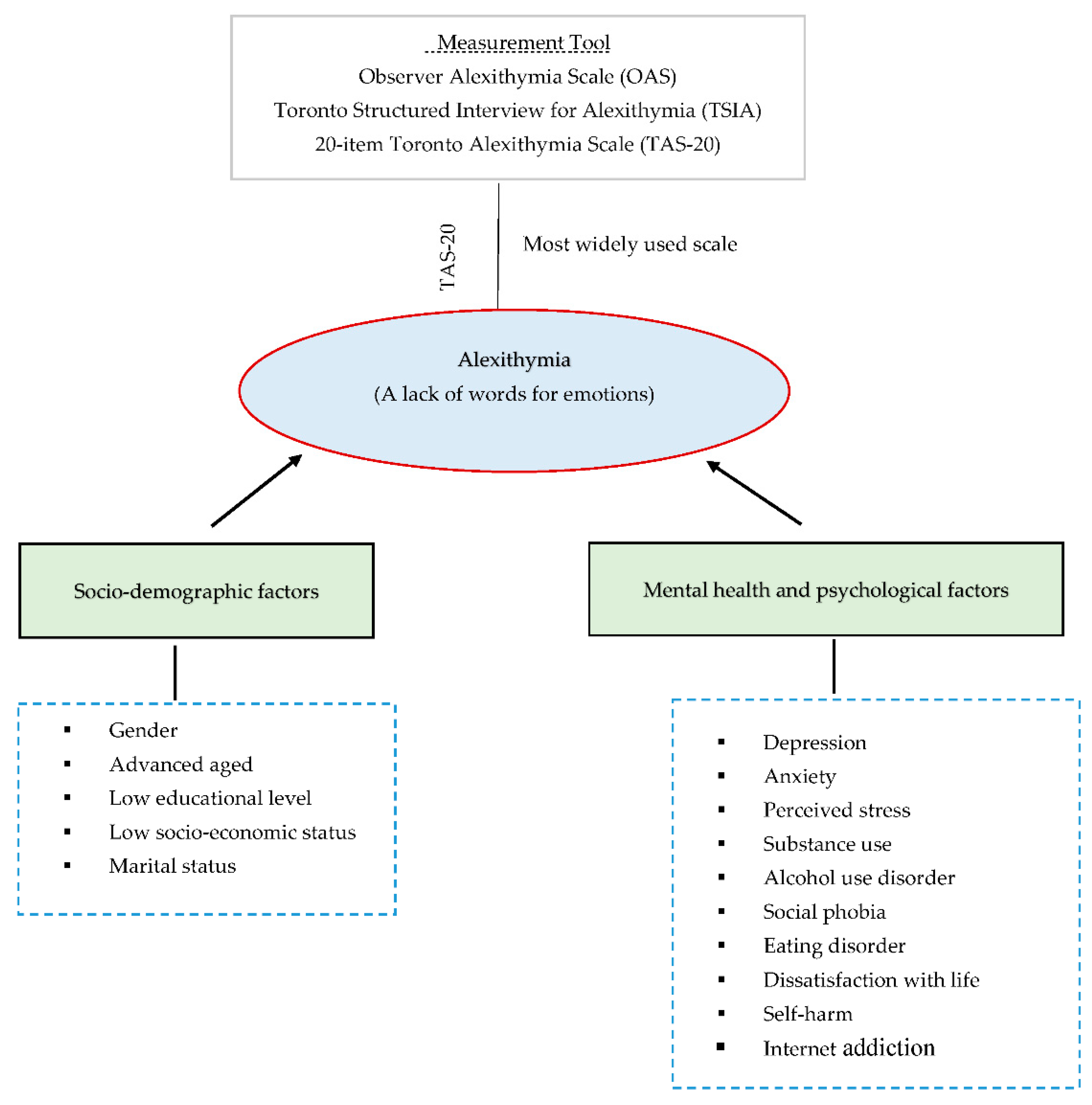
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sample Size
2.3. Sampling Technique
2.4. Survey
2.5. Ethical Consideration
2.6. Statistical Analysis
3. Results
3.1. Particpitants Demographic Chractristics
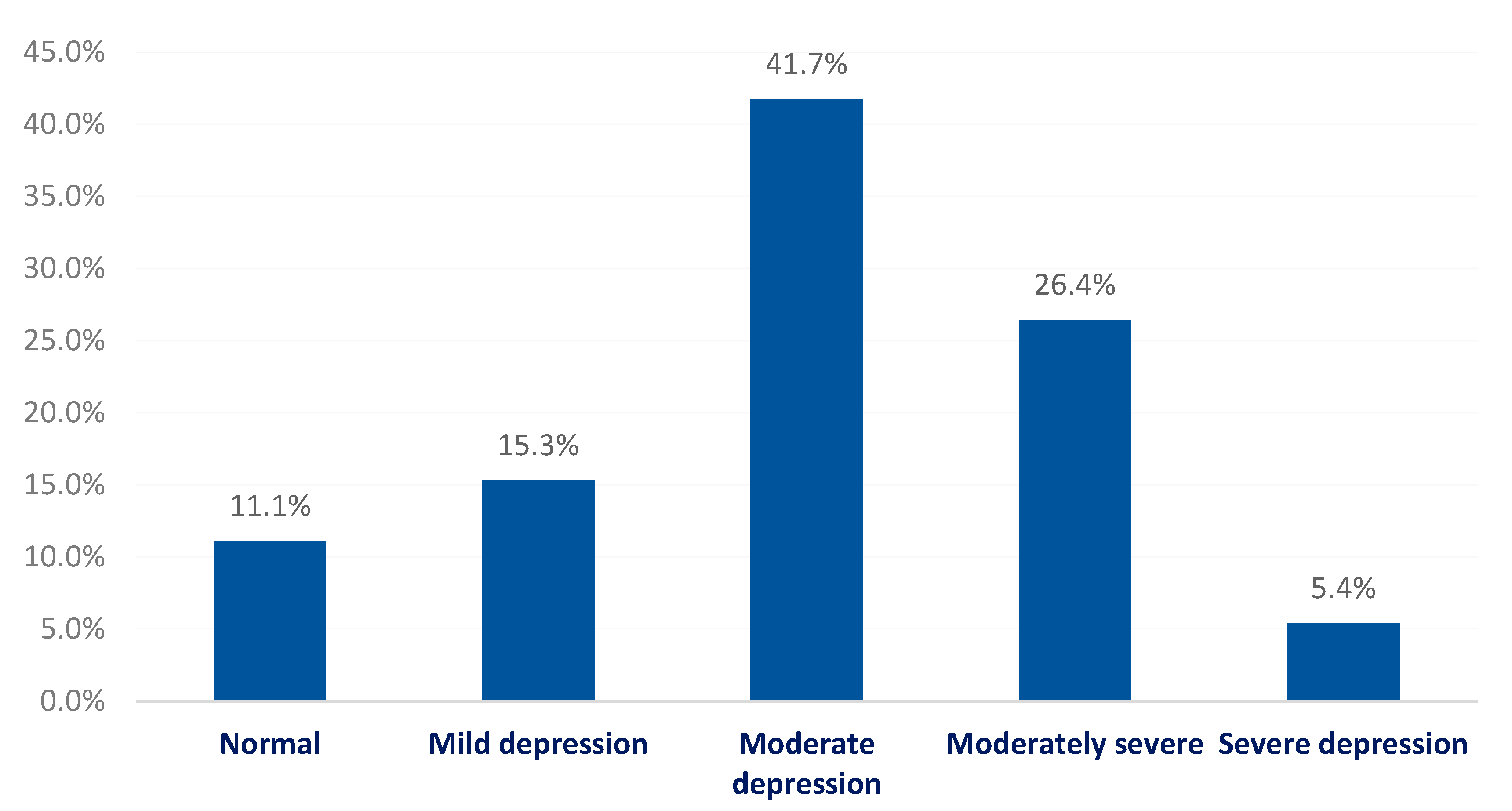
3.2. Prevalence of Alexithymia and Depression
3.3. Relationship between Alexithymia and Depression
3.4. Factors Associated with Alexithymia
4. Discussion
Strength and Limitations of this Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moffat, K.J.; McConnachie, A.; Ross, S.; Morrison, J.M. First year medical student stress and coping in a problem-based learning medical curriculum. Med. Educ. 2004, 38, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Messedi, N.; Feki, I.; Saguem, B.; Masmoudi, R.; Masmoudi, J. Alexithymia and coping strategies among medical students. Eur. Psychiatry 2017, 41, S695. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; West, C.P.; Satele, D.; Boone, S.; Tan, L.; Sloan, J.; Shanafelt, T.D. Burnout among US medical students, residents, and early career physicians relative to the general US population. Acad. Med. 2014, 89, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Hamaideh, S.H. Alexithymia among Jordanian university students: Its prevalence and correlates with depression, anxiety, stress, and demographics. Perspect. Psychiatr. Care 2017, 54, 274–280. [Google Scholar] [CrossRef]
- Sifneos, P.E. The prevalence of ‘alexithymic’ characteristics in psychosomatic patients. Psychother. Psychosom. 1973, 22, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Nemiah, J.C. Alexithymia: A view of the psychosomatic process. Mod. Trends Psychosom. Med. 1976, 3, 430–439. [Google Scholar]
- Dubey, A.; Pandey, R. Mental health problems in alexithymia: Role of positive and negative emotional experiences. J. Proj. Psychol. Ment. Health 2013, 20, 128–136. [Google Scholar]
- Bratis, D.; Tselebis, A.; Sikaras, C.; Moulou, A.; Giotakis, K.; Zoumakis, E.; Ilias, I. Alexithymia and its association with burnout, depression and family support among Greek nursing staff. Hum. Resour. Health 2009, 7, 72. [Google Scholar] [CrossRef]
- Reeves, R.R.; Johnson-Walker, D. Alexithymia: Should this personality disorder be considered during treatment of patients with mental illness? J. Psychosoc. Nurs. Ment. Health Serv. 2015, 53, 25–97. [Google Scholar] [CrossRef]
- Gilbert, P.; McEwan, K.; Catarino, F.; Baião, R.; Palmeira, L. Fears of happiness and compassion in relationship with depression, alexithymia, and attachment security in a depressed sample. Br. J. Clin. Psychol. 2014, 53, 228–244. [Google Scholar] [CrossRef]
- Essawy, H.I.; Hashem, N.Z.; El Hawary, Y.A.; Morsy, M.H.; El Awady, S.A. Prevalence of eating disorders and alexithymia among a sample of Egyptian medical students not attending psychiatric clinics. QJM Int. J. Med. 2021, 114, hcab102.024. [Google Scholar] [CrossRef]
- Popa-Velea, O.; Diaconescu, L.; Mihăilescu, A.; Macarie, G.; Popescu, M.J. Burnout and its relationships with alexithymia, stress, and social support among Romanian medical students: A cross-sectional study. Int. J. Environ. Res. Public Health 2017, 14, 560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzahrani, S.H.; Coumaravelou, S.; Mahmoud, I.; Beshawri, J.; Algethami, M. Prevalence of alexithymia and associated factors among medical students at King Abdulaziz University: A cross-sectional study. Ann. Saudi Med. 2020, 40, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Luo, T.; Liu, J.; Qu, B. Influencing factors of alexithymia in Chinese medical students: A cross-sectional study. BMC Med. Educ. 2017, 17, 66. [Google Scholar] [CrossRef]
- Saravanan, C.; Wilks, R. Medical students’ experience of and reaction to stress: The role of depression and anxiety. Sci. World J. 2014, 2014, 737382. [Google Scholar] [CrossRef]
- Morice-Ramat, A.; Goronflot, L.; Guihard, G. Are alexithymia and empathy predicting factors of the resilience of medical residents in France? Int. J. Med. Educ. 2018, 9, 122. [Google Scholar] [CrossRef]
- Abbasi, M.; Bagyan, M.J.; Dehghan, H. Cognitive failure and alexithymia and predicting high-risk behaviors of students with learning disabilities. Int. J. High Risk Behav. Addict. 2014, 3, e16948. [Google Scholar] [CrossRef]
- Faramarzi, M.; Khafri, S. Role of alexithymia, anxiety, and depression in predicting self-efficacy in academic students. Sci. World J. 2017, 2017, 5798372. [Google Scholar] [CrossRef]
- Schmitz, M.J. Alexithymia, Self-Care, and Satisfaction with Life in College Students. Diss. Abstr. Int. Sect. B: Sci. Eng. 2000, 60, 5790. [Google Scholar]
- Soliman, M. Perception of stress and coping strategies by medical students at King Saud University, Riyadh, Saudi Arabia. J. Taibah Univ. Med. Sci. 2014, 9, 30–35. [Google Scholar] [CrossRef]
- Kokkonen, P.; Karvonen, J.T.; Veijola, J.; Läksy, K.; Jokelainen, J.; Jarvelin, M.-R.; Joukamaa, M. Prevalence and sociodemographic correlates of alexithymia in a population sample of young adults. Compr. Psychiatry 2001, 42, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Mattila, A.K.; Salminen, J.K.; Nummi, T.; Joukamaa, M. Age is strongly associated with alexithymia in the general population. J. Psychosom. Res. 2006, 61, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Obeid, S.; Akel, M.; Haddad, C.; Fares, K.; Sacre, H.; Salameh, P.; Hallit, S. Factors associated with alexithymia among the Lebanese population: Results of a cross-sectional study. BMC Psychol. 2019, 7, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alharbi, H.; Almalki, A.; Alabdan, F.; Haddad, B. Depression among medical students in Saudi medical colleges: A cross-sectional study. Adv. Med. Educ. Pract. 2018, 9, 887. [Google Scholar] [CrossRef]
- Kulsoom, B.; Nasir, A.A. Stress, anxiety, and depression among medical students in a multiethnic setting. Neuropsychiatr. Dis. Treat. 2015, 11, 1713. [Google Scholar]
- AlJaber, M.I. The prevalence and associated factors of depression among medical students of Saudi Arabia: A systematic review. J. Fam. Med. Prim. Care 2020, 9, 2608. [Google Scholar] [CrossRef]
- Richards, D. Prevalence and clinical course of depression: A review. Clin. Psychol. Rev. 2011, 31, 1117–1125. [Google Scholar] [CrossRef]
- Leweke, F.; Leichsenring, F.; Kruse, J.; Hermes, S. Is alexithymia associated with specific mental disorders. Psychopathology 2012, 45, 22–28. [Google Scholar] [CrossRef]
- Scimeca, G.; Bruno, A.; Cava, L.; Pandolfo, G.; Muscatello, M.R.A.; Zoccali, R. The relationship between alexithymia, anxiety, depression, and internet addiction severity in a sample of Italian high school students. Sci. World J. 2014, 2014, 504376. [Google Scholar] [CrossRef]
- Alharthi, A.M.; Almasoudi, M.A.; Alotaibi, M.B.; Jalaladdin, M.S.; Shatla, M.M. Prevalence of Alexithymia and the influencing factors among medical students at Umm Al-Qura University: A cross-sectional study. Med. Sci. 2022, 26, ms26e1947. [Google Scholar] [CrossRef]
- Alenazi, S.F.; Hammad, S.M.; Mohamed, A.E. Prevalence of Depression, anxiety and stress among male secondary school students in Arar city, Saudi Arabia, during the school year 2018. Electron. Physician 2019, 11, 7522–7528. [Google Scholar] [CrossRef]
- Alsaleem, M.A. Depression, Anxiety, Stress, and Obesity among Male Adolescents at Abha City, Southwestern Saudi Arabia. J. Genet. Psychol. 2021, 182, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Raosoft. Online Sample Size Calculator. Available online: https://www.raosoft.com/samplesize.html (accessed on 4 April 2017).
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. The twenty-item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. APA PsycTests 1994. [Google Scholar] [CrossRef]
- Al-Eithan, M.H.; A Al Juban, H.; A Robert, A. Alexithymia among Arab mothers of disabled children and its correlation with mood disorders. Saudi Med. J. 2012, 33, 995–1000. [Google Scholar]
- Alkhormi, A.H.; Mahfouz, M.S.; Alshahrani, N.Z.; Hummadi, A.; Hakami, W.A.; Alattas, D.H.; Alhafaf, H.Q.; Kardly, L.E.; Mashhoor, M.A. Psychological Health and Diabetes Self-Management among Patients with Type 2 Diabetes during COVID-19 in the Southwest of Saudi Arabia. Medicina 2022, 58, 675. [Google Scholar] [CrossRef]
- Alzahrani, F.; Alshahrani, N.Z.; Abu Sabah, A.; Zarbah, A.; Abu Sabah, S.; Mamun, M.A. Prevalence and factors associated with mental health problems in Saudi general population during the coronavirus disease 2019 pandemic: A systematic review and meta-analysis. PsyCh. J. 2022, 11, 18–29. [Google Scholar] [CrossRef]
- AlHadi, A.N.; AlAteeq, D.A.; Al-Sharif, E.; Bawazeer, H.M.; Alanazi, H.; AlShomrani, A.T.; Shuqdar, R.M.; AlOwaybil, R. An arabic translation, reliability, and validation of Patient Health Questionnaire in a Saudi sample. Ann. Gen. Psychiatry 2017, 16, 32. [Google Scholar] [CrossRef]
- Soliman, E.S.; Allaboun, S.M.; Algenaimi, E.F.; Aldhuwayhi, R.H.; Almutairi, A.F.; Alwarthan, S.A. The relationship between alexithymia and internet addiction among university students in the Kingdom of Saudi Arabia. Int. J. Med. Dev. Ctries. 2021, 5, 433–438. [Google Scholar] [CrossRef]
- Alamri, Y. Mental illness in Saudi Arabia: Stigma and acceptability. Int. J. Soc. Psychiatry 2016, 62, 306–307. [Google Scholar] [CrossRef]
- Katsifaraki, M.; Tucker, P. Alexithymia and burnout in nursing students. J. Nurs. Educ. 2013, 52, 627–633. [Google Scholar] [CrossRef]
- Van Houtum, L.; Rijken, M.; Groenewegen, P. Do everyday problems of people with chronic illness interfere with their disease management? BMC Public Health 2015, 15, 1000. [Google Scholar] [CrossRef] [PubMed]
- Castelnuovo, G.; Pietrabissa, G.; Manzoni, G.M.; Corti, S.; Ceccarini, M.; Borrello, M.; Giusti, E.M.; Novelli, M.; Cattivelli, R.; Middleton, N.A.; et al. Chronic care management of globesity: Promoting healthier lifestyles in traditional and mHealth based settings. Front. Psychol. 2015, 6, 1557. [Google Scholar] [CrossRef] [PubMed]
- Tolmunen, T.; Lehto, S.M.; Heliste, M.; Kurl, S.; Kauhanen, J. Alexithymia is associated with increased cardiovascular mortality in middle-aged Finnish men. Psychosom. Med. 2010, 7, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Al bajjar, M.A.; Bakarman, M.A. Prevalence and correlates of depression among male medical students and interns in Albaha University, Saudi Arabia. J. Fam. Med. Prim. Care 2019, 8, 1889. [Google Scholar]
- Alamri, H.S.; Algarni, A.; Shehata, S.F.; Al Bshabshe, A.; Alshehri, N.N.; ALAsiri, A.M.; Hussain, A.H.; Alalmay, A.Y.; Alshehri, E.A.; Alqarni, Y.; et al. Prevalence of Depression, Anxiety, and Stress among the General Population in Saudi Arabia during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9183. [Google Scholar] [CrossRef]
- Alharbi, A. The Prevalence of Depression and Related Factors During the COVID-19 Pandemic Among the General Population of the Jazan Region of Saudi Arabia. Cureus 2022, 2, e21965. [Google Scholar] [CrossRef]
- Al Rashed, A.S.; Al-Naim, A.F.; Almulhim, B.J.; Alhaddad, M.S.; Al-Thafar, A.I.; Alali, M.J.; Aleem, A.M.; Kashif, S.; Bougmiza, I. Prevalence and associated factors of depression among general population in Al-Ahsa, Kingdom of Saudi Arabia: A community-based survey. Neurol. Psychiatry Brain Res. 2019, 31, 32–36. [Google Scholar] [CrossRef]
- Tian-Ci Quek, T.; Wai-San Tam, W.; Tran, B.X.; Zhang, M.; Zhang, Z.; Su-Hui Ho, C.; Chun-Man Ho, R. The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2735. [Google Scholar] [CrossRef]
- Moir, F.; Yielder, J.; Sanson, J.; Chen, Y. Depression in medical students: Current insights. Adv. Med. Educ. Pract. 2018, 9, 323–333. [Google Scholar] [CrossRef]
- Li, S.; Zhang, B.; Guo, Y.; Zhang, J. The association between alexithymia as assessed by the 20-item Toronto Alexithymia Scale and depression: A metaanalysis. Psychiatry Res. 2015, 227, 1–9. [Google Scholar] [CrossRef]
- Sfeir, E.; Geara, C.; Hallit, S.; Obeid, S. Alexithymia, aggressive behavior and depression among Lebanese adolescents: A cross-sectional study. Child Adolesc. Psychiatry Ment. Health 2020, 1, 32. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.; Beadea, J.N.; Paradiso, S. Towards a classification of alexithymia: Primary, secondary and organic. J. Psychopathol. 2014, 20, 38–49. [Google Scholar]
- Honkalampi, K.; Koivumaa-Honkanen, H.; Tanskanen, A.; Hintikka, J.; Lehtonen, J.; Viinamaki, H. Why do alexithymic features appear to be stable? A 12-month follow-up study of a general population. Psychother. Psychosom. 2001, 5, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Paradiso, S.; Caspers, K.; Tranel, D.; Coryell, W. Cognition and nondysphoric depression among adoptees at high risk for psychopathology. Compr. Psychiatry 2011, 5, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Hemming, L.; Haddock, G.; Shaw, J.; Pratt, D. Alexithymia and its associations with depression, suicidality, and aggression: An overview of the literature. Front. Psychiatry 2019, 10, 203. [Google Scholar] [CrossRef] [PubMed]
- Hintikka, J.; Honkalampi, K.; Lehtonen, J.; Viinamäki, H. Are alexithymia and depression distinct or overlapping constructs?: A study in a general population. Compr. Psychiatry 2001, 3, 234–239. [Google Scholar] [CrossRef]
- Honkalampi, K.; Hintikka, J.; Saarinen, P.; Lehtonen, J.; Viinamäki, H. Is alexithymia a permanent feature in depressed patients? Results from a 6-month follow-up study. Psychother. Psychosom. 2000, 69, 303–308. [Google Scholar] [CrossRef]
- Gilanifar, M.; Delavar, M.A. Alexithymia in pregnant women: Its relationship with depression. ASEAN J. Psychiatry 2016, 17, 35–41. [Google Scholar]
- De Berardis, D.; Fornaro, M.; Orsolini, L.; Valchera, A.; Carano, A.; Vellante, F.; Perna, G.; Serafini, G.; Gonda, X.; Pompili, M.; et al. Alexithymia and suicide risk in psychiatric disorders: A mini-review. Front. Psychiatry 2017, 8, 148. [Google Scholar] [CrossRef]
- Zhang, H.; Fan, Q.; Sun, Y.; Qiu, J.; Song, L. A study of the characteristics of alexithymia and emotion regulation in patients with depression. Shanghai Arch. Psychiatry 2017, 2, 95. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Data | N | % |
|---|---|---|
| Age in years | ||
| 18–20 | 53 | 15.9 |
| 21–23 | 202 | 60.7 |
| 24–27 | 78 | 23.4 |
| Gender | ||
| Male | 162 | 48.6 |
| Female | 171 | 51.4 |
| Academic phase | ||
| Pre-clinical | 118 | 35.4 |
| Clinical | 215 | 64.6 |
| Marital status | ||
| Single | 290 | 87.1 |
| Married | 43 | 12.9 |
| Body Mass Index (BMI) | ||
| Underweight | 32 | 9.6 |
| Normal weight | 145 | 43.5 |
| Overweight | 80 | 24 |
| Obesity Class I | 48 | 14.4 |
| Obesity Class II | 22 | 6.6 |
| Obesity Class III | 6 | 1.8 |
| Smoking status | ||
| Yes | 94 | 28.2 |
| No | 239 | 71.8 |
| How often do you take part in physical training per week? | ||
| >3 times | 47 | 14.1 |
| 3 times | 83 | 24.9 |
| 1 time | 108 | 32.4 |
| Never | 95 | 28.5 |
| Parents’ status | ||
| Married | 266 | 79.9 |
| Divorced | 67 | 20.1 |
| Family monthly income | ||
| SAR < 3000 | 20 | 6 |
| SAR 3000–6000 | 41 | 12.3 |
| SAR 6000–10,000 | 48 | 14.4 |
| SAR 10,000–15,000 | 91 | 27.3 |
| SAR>15,000 | 133 | 39.9 |
| Housing | ||
| Own house | 235 | 70.6 |
| Rented house | 59 | 17.7 |
| Students’ dormitory | 39 | 11.7 |
| Do you have any chronic illnesses? | ||
| Yes | 114 | 34.2 |
| No | 219 | 65.8 |
| TAS-20 | Depression | p-Value | |||
|---|---|---|---|---|---|
| Normal | Depression | ||||
| N | % | N | % | ||
| No alexithymia | 10 | 25 | 30 | 75 | 0.001 * |
| Possible alexithymia | 18 | 13.3 | 117 | 86.7 | |
| Alexithymia | 9 | 5.7 | 149 | 94.3 | |
| Factors | Alexithymia | p-Value | |||||
|---|---|---|---|---|---|---|---|
| No Alexithymia | Possible Alexithymia | Alexithymia | |||||
| N | % | N | % | N | % | ||
| Academic phase | |||||||
| Pre-clinical | 11 | 9.3 | 52 | 44.1 | 55 | 46.6 | 0.430 |
| Clinical | 29 | 13.5 | 83 | 38.6 | 103 | 47.9 | |
| Age in years | |||||||
| 18–20 | 6 | 11.3 | 19 | 35.8 | 28 | 52.8 | 0.216 |
| 21–23 | 30 | 14.9 | 81 | 40.1 | 91 | 45.0 | |
| 24–27 | 4 | 5.1 | 35 | 44.9 | 39 | 50 | |
| Gender | |||||||
| Male | 20 | 12.3 | 74 | 45.7 | 68 | 42 | 0.048 * |
| Female | 20 | 11.7 | 61 | 35.7 | 90 | 52.6 | |
| Body mass index (BMI) | |||||||
| Underweight | 4 | 12.5 | 15 | 46.9 | 13 | 40.6 | 0.908 $ |
| Normal weight | 17 | 11.7 | 54 | 37.2 | 74 | 51 | |
| Overweight | 11 | 13.8 | 34 | 42.5 | 35 | 43.8 | |
| Obese | 8 | 10.5 | 32 | 42.1 | 36 | 47.4 | |
| Smoking status | |||||||
| Yes | 14 | 14.9 | 41 | 43.6 | 39 | 41.5 | 0.334 |
| No | 26 | 10.9 | 94 | 39.3 | 119 | 49.8 | |
| How often do you take part in physical training per week? | |||||||
| >3 times | 3 | 6.4 | 22 | 46.8 | 22 | 46.8 | 0.907 $ |
| 3 times | 11 | 13.3 | 34 | 41 | 38 | 45.8 | |
| 1 time | 14 | 13.0 | 42 | 38.9 | 52 | 48.1 | |
| Never | 12 | 12.6 | 37 | 38.9 | 46 | 48.4 | |
| Parents’ status | |||||||
| Married | 30 | 11.3 | 110 | 41.4 | 126 | 47.4 | 0.667 |
| Divorced | 10 | 14.9 | 25 | 37.3 | 32 | 47.8 | |
| Family monthly income | |||||||
| SAR < 3000 | 7 | 35.0 | 6 | 30.0 | 7 | 35 | 0.011 * |
| SAR 3000–6000 | 6 | 14.6 | 23 | 56.1 | 12 | 29.3 | |
| SAR 6000–10,000 | 5 | 10.4 | 16 | 33.3 | 27 | 56.3 | |
| SAR 10,000–15,000 | 12 | 13.2 | 36 | 39.6 | 43 | 47.3 | |
| SAR >15,000 | 10 | 7.5 | 54 | 40.6 | 69 | 51.9 | |
| Housing | |||||||
| Own house | 29 | 12.3 | 90 | 38.3 | 116 | 49.4 | 0.494 $ |
| Rented house | 7 | 11.9 | 24 | 40.7 | 28 | 47.5 | |
| Students’ dormitory | 4 | 10.3 | 21 | 53.8 | 14 | 35.9 | |
| Do you have any chronic illnesses? | |||||||
| Yes | 16 | 14.0 | 52 | 45.6 | 46 | 40.4 | 0.171 |
| No | 24 | 11 | 83 | 37.9 | 112 | 51.1 | |
| Factors | p-Value | OR | 95% CI | |
|---|---|---|---|---|
| Lower | Upper | |||
| Female gender | 0.023 * | 2.09 | 1.18 | 4.78 |
| High income (>10,000 SAR) | 0.044 * | 0.39 | 0.17 | 0.97 |
| Have chronic disease | 0.041 * | 2.04 | 1.23 | 7.11 |
| Depression | 0.012 * | 1.91 | 1.11 | 3.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aleisa, M.A.; Abdullah, N.S.; Alqahtani, A.A.A.; Aleisa, J.A.J.; Algethami, M.R.; Alshahrani, N.Z. Association between Alexithymia and Depression among King Khalid University Medical Students: An Analytical Cross-Sectional Study. Healthcare 2022, 10, 1703. https://doi.org/10.3390/healthcare10091703
Aleisa MA, Abdullah NS, Alqahtani AAA, Aleisa JAJ, Algethami MR, Alshahrani NZ. Association between Alexithymia and Depression among King Khalid University Medical Students: An Analytical Cross-Sectional Study. Healthcare. 2022; 10(9):1703. https://doi.org/10.3390/healthcare10091703
Chicago/Turabian StyleAleisa, Mohammed Ahmed, Naif Saud Abdullah, Amar Abdullah A. Alqahtani, Jaber Ahmed J Aleisa, Mohammed R. Algethami, and Najim Z. Alshahrani. 2022. "Association between Alexithymia and Depression among King Khalid University Medical Students: An Analytical Cross-Sectional Study" Healthcare 10, no. 9: 1703. https://doi.org/10.3390/healthcare10091703