
Efficacy of an Integrated Mobile Application System for Patients with Radiation Therapy: A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Development
- Register patient/physician information;
- Manage patient care schedule;
- Enter the treatment area;
- Enter self-management method *;
- Enter the side effect questionnaire during treatment *;
- Enter disease information *.
2.2. Validation
3. Results
3.1. Management System
3.2. Mobile Application
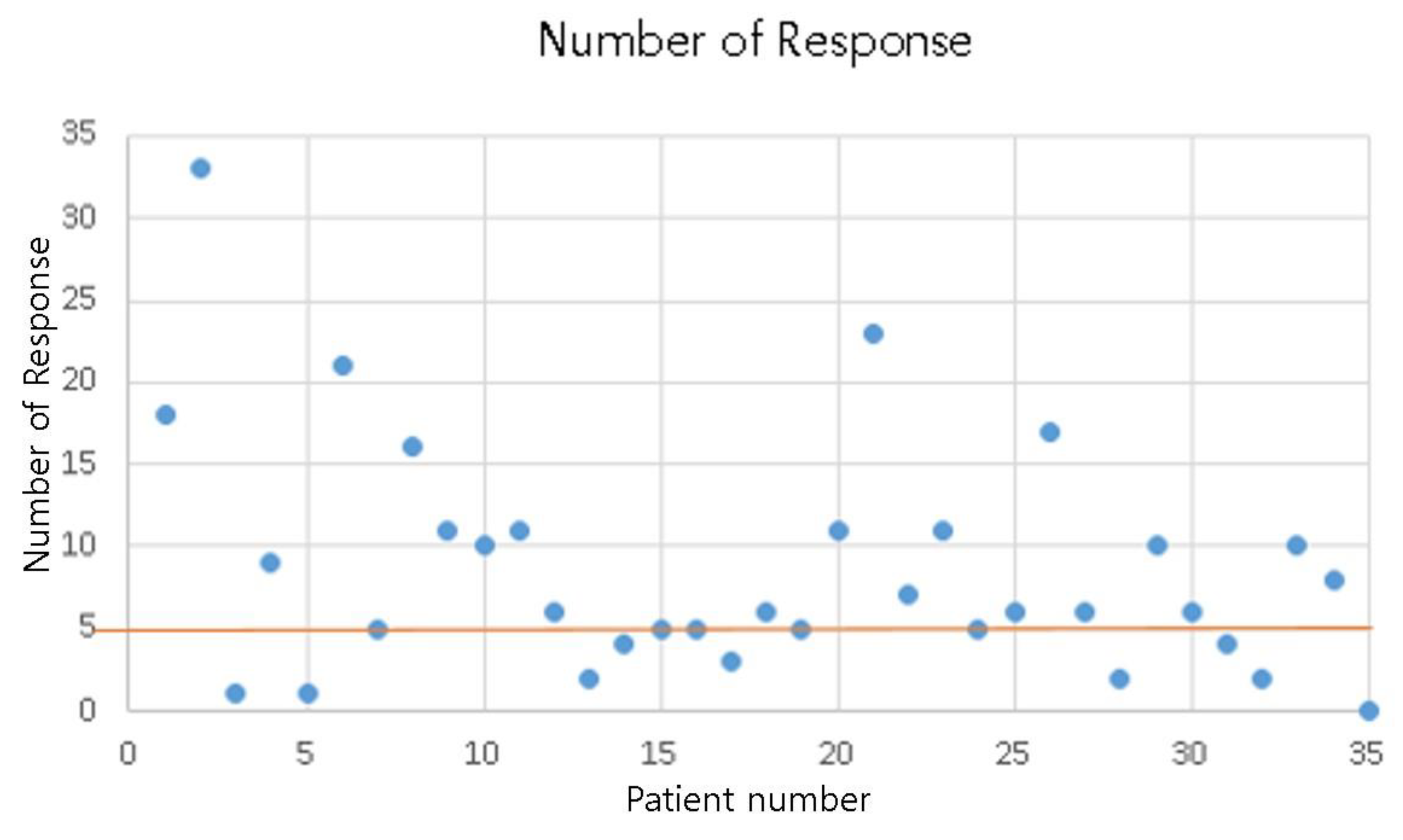
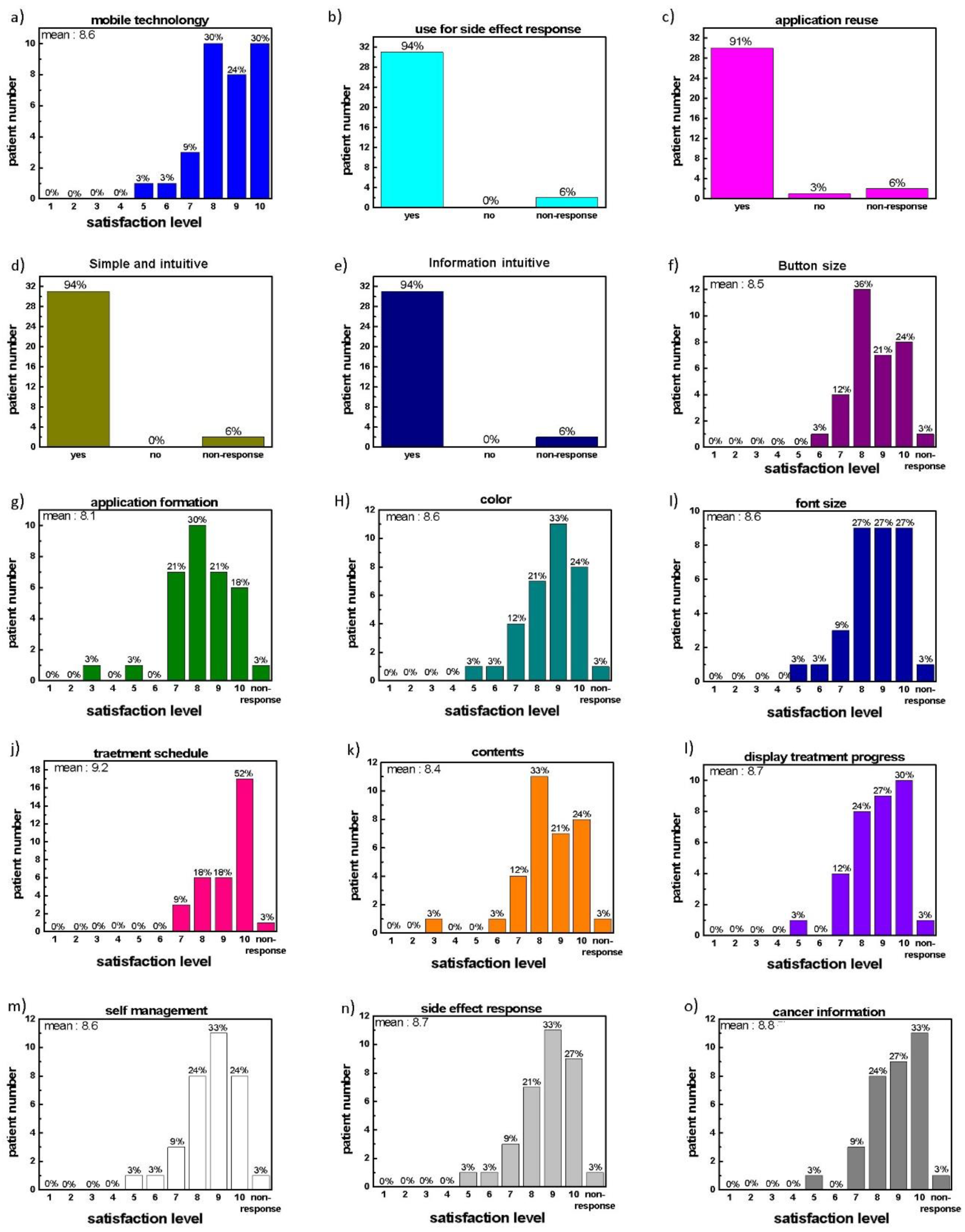
3.3. Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Won, Y.J.; Park, Y.R.; Jung, K.W.; Kong, H.J.; Lee, E.S. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2017. Cancer Res. Treat. 2020, 52, 335–350. [Google Scholar] [CrossRef]
- Heron, M.; Anderson, R.N. Changes in the Leading Cause of Death: Recent Patterns in Heart Disease and Cancer Mortality. NCHS Data Brief 2016, 254, 1–8. [Google Scholar]
- Kang, J.K.; Kim, M.S.; Jang, W.I.; Seo, Y.S.; Kim, H.J.; Cho, C.K.; Yoo, H.J.; Paik, E.K.; Cha, Y.J.; Song, H.J. The clinical utilization of radiation therapy in Korea between 2009 and 2013. Radiat. Oncol. J. 2016, 34, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Córdoba, E.E.; Lacunza, E.; Güerci, A.M. Clinical factors affecting the determination of radiotherapy-induced skin toxicity in breast cancer. Radiat. Oncol. J. 2021, 39, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Brouard, B.; Bardo, P.; Bonnet, C.; Mounier, N.; Vignot, M.; Vignot, S. Mobile applications in oncology: Is it possible for patients and healthcare professionals to easily identify relevant tools? Ann. Med. 2016, 48, 509–515. [Google Scholar] [CrossRef]
- Denis, F.; Viger, L.; Charron, A.; Voog, E.; Dupuis, O.; Pointreau, Y.; Letellier, C. Detection of lung cancer relapse using self-reported symptoms transmitted via an internet web-application: Pilot study of the sentinel follow-up. Support. Care Cancer 2014, 22, 1467–1473. [Google Scholar] [CrossRef]
- de Jongh, T.; Gurol-Urganci, I.; Vodopivec-Jamsek, V.; Car, J.; Atun, R. Mobile phone messaging for facilitating self-management of long-term illnesses. Cochrane Database Syst. Rev. 2012, 12, CD007459. [Google Scholar] [CrossRef]
- Denis, F.; Yossi, S.; Septans, A.L.; Charron, A.; Voog, E.; Dupuis, O.; Ganem, G.; Pointreau, Y.; Letellier, C. Improving Survival in Patients Treated for a Lung Cancer Using Self-Evaluated Symptoms Reported Through a Web Application. Am. J. Clin. Oncol. 2017, 40, 464–469. [Google Scholar] [CrossRef]
- El Shafie, R.A.; Bougatf, N.; Sprave, T.; Weber, D.; Oetzel, D.; Machmer, T.; Huber, P.E.; Debus, J.; Nicolay, N.H. Oncologic Therapy Support Via Means of a Dedicated Mobile App (OPTIMISE-1): Protocol for a Prospective Pilot Trial. JMIR Res. Protoc. 2018, 7, e70. [Google Scholar] [CrossRef]
- Ataei, G.; Cham, S.; Niksirat, F.; Shabestani Monfared, A.; Ebrahimnejad, G.K. Developing a Mobile Phone Application for Common Radiotherapy Calculations. J. Biomed Phys. Eng. 2020, 10, 235–240. [Google Scholar] [CrossRef]
- Rades, D.; Narvaez, C.A.; Doemer, C.; Janssen, S.; Olbrich, D.; Tvilsted, S.; Conde-Moreno, A.J.; Cacicedo, J. Radiotherapy-related skin toxicity (RAREST-02): A randomized trial testing the effect of a mobile application reminding head-and-neck cancer patients to perform skin care (reminder app) on radiation dermatitis. Trials 2020, 21, 424. [Google Scholar] [CrossRef] [PubMed]
- Zini, E.M.; Lanzola, G.; Quaglini, S.; Bossi, P.; Licitra, L.; Resteghini, C. A pilot study of a smartphone-based monitoring intervention on head and neck cancer patients undergoing concurrent chemo-radiotherapy. Int. J. Med. Inform. 2019, 129, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Di, R.; Li, G. Use of a Smartphone Medical App Improves Complications and Quality of Life in Patients with Nasopharyngeal Carcinoma Who Underwent Radiotherapy and Chemotherapy. Med. Sci. Monit. 2018, 24, 6151–6156. [Google Scholar] [CrossRef]
- Kessel, K.A.; Vogel, M.M.; Alles, A.; Dobiasch, S.; Fischer, H.; Combs, S.E. Mobile App Delivery of the EORTC QLQ-C30 Questionnaire to Assess Health-Related Quality of Life in Oncological Patients: Usability Study. JMIR mhealth uhealth 2018, 6, e45. [Google Scholar] [CrossRef]
- Weldring, T.; Smith, S.M. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv. Insights 2013, 6, 61–68. [Google Scholar] [CrossRef]
- Denis, F.; Lethrosne, C.; Pourel, N.; Molinier, O.; Pointreau, Y.; Domont, J.; Bourgeois, H.; Senellart, H.; Trémolières, P.; Lizée, T.; et al. Randomized Trial Comparing a Web-Mediated Follow-up with Routine Surveillance in Lung Cancer Patients. JNCI J. Natl. Cancer Inst. 2017, 109, 436. [Google Scholar] [CrossRef]
- Mooney, K.H.; Beck, S.L.; Wong, B.; Dunson, W.; Wujcik, D.; Whisenant, M.; Donaldson, G. Automated home monitoring and management of patient-reported symptoms during chemotherapy: Results of the symptom care at home RCT. Cancer Med. 2017, 6, 537–546. [Google Scholar] [CrossRef]
- Lee, K.E.; Kim, S.-H.; Ha, T.-Y.; Yoo, Y.-M.; Han, J.-J.; Jung, J.-H.; Jang, J.-Y. Dependency on Smartphone Use and Its Association with Anxiety in Korea. Public Health Rep. 2016, 131, 411–419. [Google Scholar] [CrossRef]
- Park, J.H.; Park, M. Smartphone use patterns and problematic smartphone use among preschool children. PLoS ONE 2021, 16, e0244276. [Google Scholar] [CrossRef]
- Lee, J.; Choi, Y.-J.; An, A.R.; Kim, Y. Duration of and fee for comprehensive assessment and care planning for patients with hypertension and/or diabetes in primary care. JKMA 2017, 60, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Maloney, E.K.; D’Agostino, T.A.; Heerdt, A.; Dickler, M.; Li, Y.; Ostroff, J.S.; Bylund, C.L. Sources and types of online information that breast cancer patients read and discuss with their doctors. Palliat. Support. Care 2015, 13, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Bantum, E.O.; Owen, J.; Bakken, S.; Elhadad, N. Online cancer communities as informatics intervention for social support: Conceptualization, characterization, and impact. J. Am. Med. Inform. Assoc. 2017, 24, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Park, K.; Jo, H.S. Gap between Perceived eHealth Literacy and Ability to Use Online Cancer-Related Information. J. Korean Med. Sci. 2020, 35, 1146036. [Google Scholar] [CrossRef]
- Jo, H.S.; Song, T.M.; Kim, B.G. Analysis of the Factors Affecting Consumer Acceptance of Accredited Online Health Information. J. Korean Med. Sci. 2017, 32, 1757–1763. [Google Scholar] [CrossRef]
- Talari, K.; Goyal, M. Retrospective studies—Utility and caveats. J. R. Coll. Physicians Edinb. 2020, 50, 398–402. [Google Scholar] [CrossRef]
- Hu, Z.; Melton, G.B.; Arsoniadis, E.G.; Wang, Y.; Kwaan, M.R.; Simon, G.J. Strategies for handling missing clinical data for automated surgical site infection detection from the electronic health record. J. Biomed. Inform. 2017, 68, 112–120. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Client | Server | |||
|---|---|---|---|---|
| Mobile Application (User) | Manager (Doctor) | |||
| Name | AROMA M | AROMA | AROMA S | |
| Minimal requirement | Android Lollipop | iOS 13 | Windows 10 Pro | Windows 10 Pro |
| Language | Kotlin 1.4.32 | Swift 5 | C# 7.3 | Go 1.15.5 |
| Software | Android Studio 4.1.3` | XCode 12.4 | Visual Studio 2019 | Visual Studio Code 1.55.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Yea, J.W.; Oh, S.A.; Park, J.W. Efficacy of an Integrated Mobile Application System for Patients with Radiation Therapy: A Pilot Study. Healthcare 2022, 10, 1696. https://doi.org/10.3390/healthcare10091696
Park J, Yea JW, Oh SA, Park JW. Efficacy of an Integrated Mobile Application System for Patients with Radiation Therapy: A Pilot Study. Healthcare. 2022; 10(9):1696. https://doi.org/10.3390/healthcare10091696
Chicago/Turabian StylePark, Jaehyeon, Ji Woon Yea, Se An Oh, and Jae Won Park. 2022. "Efficacy of an Integrated Mobile Application System for Patients with Radiation Therapy: A Pilot Study" Healthcare 10, no. 9: 1696. https://doi.org/10.3390/healthcare10091696