

Effects of Extensor Digitorum Longus and Tibialis Anterior Taping on Balance and Gait Performance in Patients Post Stroke
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Procedure
2.2. Sample Size Calculation
2.3. Participants
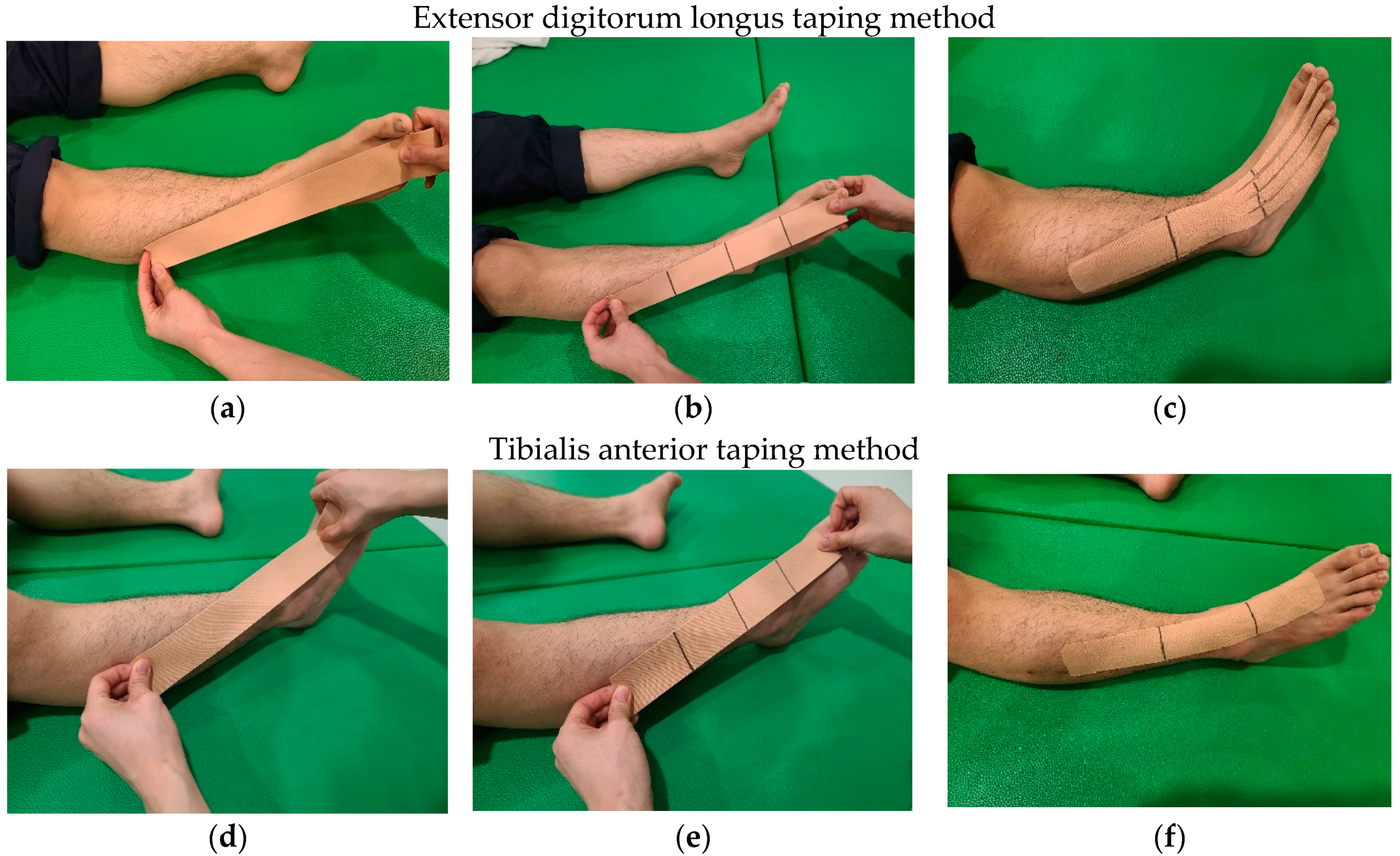
2.4. Intervention
Extensor Digitorum Longus and Tibialis Anterior Taping Method
2.5. Measurement
2.5.1. Balance Measurement
2.5.2. Gait Measurement
2.6. Statistical Analyses
3. Results
3.1. General Characteristics of the Subjects
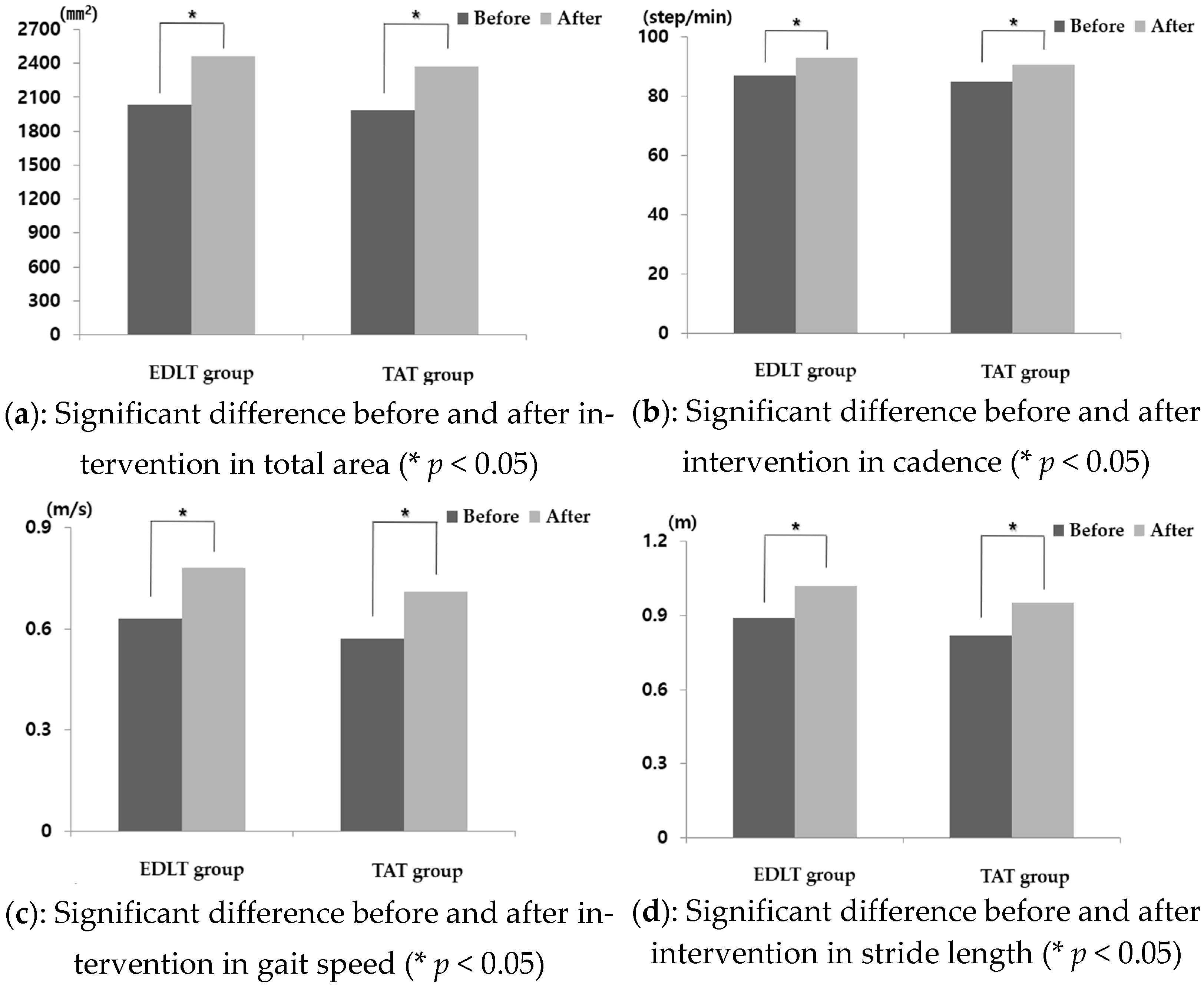
3.2. Results of Two-Way Repeated Measures of Limited Stability and Gait Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gorst, T.; Lyddon, A.; Marsden, J.; Paton, J.; Morrison, S.C.; Cramp, M.; Freeman, J. Foot and ankle impairments affect balance and mobility in stroke (FAiMiS): The views and experiences of people with stroke. Disabil. Rehabil. 2016, 38, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Van Asseldonk, E.H.; Buurke, J.H.; Bloem, B.R.; Renzenbrink, G.J.; Nene, A.V.; van der Helm, F.C.; van der Kooij, H. Disentangling the contribution of the paretic and non-paretic ankle to balance control in stroke patients. Exp. Neurol. 2006, 201, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Lamontagne, A.; Malouin, F.; Richards, C.L. Contribution of passive stiffness to ankle plantarflexor moment during gait after stroke. Arch. Phys. Med. Rehabil. 2000, 81, 351–358. [Google Scholar] [CrossRef]
- Lee, M.J.; Kilbreath, S.L.; Refshauge, K.M. Movement detection at the ankle following stroke is poor. Aust. J. Physiother. 2005, 51, 19–24. [Google Scholar] [CrossRef]
- Lin, P.Y.; Yang, Y.R.; Cheng, S.J.; Wang, R.Y. The relation between ankle impairments and gait velocity and symmetry in people with stroke. Arch. Phys. Med. Rehabil. 2006, 87, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Vattanasilp, W.; Ada, L.; Crosbie, J. Contribution of thixotropy, spasticity, and contracture to ankle stiffness after stroke. J. Neurol. Neurosurg. Psychiatry 2000, 69, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.I.; Hsu, L.J.; Wang, H.C. Effects of ankle proprioceptive interference on locomotion after stroke. Arch. Phys. Med. Rehabil. 2012, 93, 1027–1033. [Google Scholar] [CrossRef]
- Gefen, A. Simulations of foot stability during gait characteristic of ankle dorsiflexor weakness in the elderly. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 333–337. [Google Scholar] [CrossRef]
- Reynard, F.; Deriaz, O.; Bergeau, J. Foot varus in stroke patients: Muscular activity of extensor digitorum longus during the swing phase of gait. The Foot 2009, 19, 69–74. [Google Scholar] [CrossRef]
- Neumann, D.A. Kinesiology of the Musculoskeletal System-E-Book: Foundations for Rehabilitation; Elsevier Health Sciences: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Le Sant, G.; Nordez, A.; Hug, F.; Andrade, R.; Lecharte, T.; McNair, P.J.; Gross, R. Effects of stroke injury on the shear modulus of the lower leg muscle during passive dorsiflexion. J. Appl. Physiol. 2019, 126, 11–22. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, A.; Bolsterlee, B.; Herbert, R.D. Architecture of the medial gastrocnemius muscle in people who have had a stroke: A diffusion tensor imaging investigation. Clin. Biomech. 2020, 74, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Li, S. Ankle and foot spasticity patterns in chronic stroke survivors with abnormal gait. Toxins 2020, 12, 646. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.H.; Kim, H.G.; Min, K.S.; Lee, S.M. Effects of lower-leg kinesiology taping on balance ability in stroke patients with foot drop. Evid. Based Complement. Alternat. Med. 2015, 2015, 125629. [Google Scholar] [CrossRef]
- Yang, S.R.; Heo, S.Y.; Lee, H.J. Immediate effects of kinesio taping on fixed postural alignment and foot balance in stroke patients. J. Phys. Ther. Sci. 2015, 27, 3537–3540. [Google Scholar] [CrossRef] [PubMed]
- Hartoko, R.A.; Andriana, R.M.; Kusumawardni, M.K. Immediate effect of elastic taping application on gait functional ability in patients with stroke. Alami J. (Alauddin Islamic Med.) J. 2021, 5, 47–62. [Google Scholar] [CrossRef]
- Koseoglu, B.F.; Dogan, A.; Tatli, H.U.; Ozcan, D.S.; Polat, C.S. Can kinesio tape be used as an ankle training method in the rehabilitation of the stroke patients? Complement. Ther. Clin. Pract. 2017, 27, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Lee, Y.J. Immediate effects of kinesio taping of tibialis anterior and ankle joint on mobility and balance ability for chronic hemiparesis: Randomized controlled cross-sectional design. Phys. Med. Rehabil. Kurortmed. 2020, 30, 350–357. [Google Scholar] [CrossRef]
- Park, S.J.; Kim, T.H.; Oh, S.H. Immediate effects of tibialis anterior and calf muscle taping on center of pressure excursion in chronic stroke patients: A cross-over study. Int. J. Environ. Res. Public Health 2020, 17, 4109. [Google Scholar] [CrossRef]
- Shin, Y.J.; Kim, S.M.; Kim, H.S. Immediate effects of ankle eversion taping on dynamic and static balance of chronic stroke patients with foot drop. J. Phys. Ther. Sci. 2017, 29, 1029–1031. [Google Scholar] [CrossRef]
- Cho, K.H.; Park, S.J. Immediate effect of elastic taping on postural sway in patients with stroke. JIAPTR 2018, 9, 1631–1635. [Google Scholar] [CrossRef]
- Shin, Y.J.; Lee, J.H.; Choe, Y.W.; Kim, M.K. Immediate effects of ankle eversion taping on gait ability of chronic stroke patients. J. Bodyw. Mov. Ther. 2019, 23, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Bulley, C.; Shiels, J.; Wilkie, K.; Salisbury, L. User experiences, preferences and choices relating to functional electrical stimulation and ankle foot orthoses for foot-drop after stroke. Physiotherapy 2011, 97, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Langendoen, J.; Sertel, K. Kinesiology Taping: The Essential Step-By-Step Guide: Taping for Sports, Fitness & Daily Life: 160 Conditions & Ailments; Robert Rose Incorporated: Toronto, ON, Canada, 2014. [Google Scholar]
- Pamuk, U.; Yucesoy, C.A. MRI analyses show that kinesio taping affects much more than just the targeted superficial tissues and causes heterogeneous deformations within the whole limb. J. Biomech. 2015, 48, 4262–4270. [Google Scholar] [CrossRef]
- Van Dijk, M.M.; Meyer, S.; Sandstad, S.; Wiskerke, E.; Thuwis, R.; Vandekerckhove, C.; Myny, C.; Ghosh, N.; Beyens, H.; Dejaeger, E. A cross-sectional study comparing lateral and diagonal maximum weight shift in people with stroke and healthy controls and the correlation with balance, gait and fear of falling. PLoS ONE 2017, 12, e0183020. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.h.; Choi, B.R. Intra-and inter-rater reliability of BioRescue. J. Korea Contents Assoc. 2018, 18, 348–352. [Google Scholar] [CrossRef]
- Pau, M.; Coghe, G.; Atzeni, C.; Corona, F.; Pilloni, G.; Marrosu, M.G.; Cocco, E.; Galli, M. Novel characterization of gait impairments in people with multiple sclerosis by means of the gait profile score. J. Neurol. Sci. 2014, 345, 159–163. [Google Scholar] [CrossRef]
- D’Addio, G.; Donisi, L.; Pagano, G.; Improta, G.; Biancardi, A.; Cesarelli, M. Agreement between opal and G-walk wearable inertial systems in gait analysis on normal and pathological subjects. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 3286–3289. [Google Scholar] [CrossRef]
- Wright, A.; Smith, G.; Jobson, S.; Faulkner, J. Reliability of a trunk mounted accelerometer when determining gait parameters in people with stroke. ISBS Proc. Archive. 2022, 40, 775. [Google Scholar]
- De Ridder, R.; Lebleu, J.; Willems, T.; De Blaiser, C.; Detrembleur, C.; Roosen, P. Concurrent validity of a commercial wireless trunk triaxial accelerometer system for gait analysis. J Sport Rehabil. 2019, 28. [Google Scholar] [CrossRef]
- Rojhani-Shirazi, Z.; Amirian, S.; Meftahi, N. Effects of ankle kinesio taping on postural control in stroke patients. J. Stroke. Cerebrovasc. Dis. 2015, 24, 2565–2571. [Google Scholar] [CrossRef]
- Słupik, A.; Dwornik, M.; Białoszewski, D.; Zych, E. Effect of kinesio taping on bioelectrical activity of vastus medialis muscle. Prelim. Report. Ortop. Traumatol. Rehabil. 2007, 9, 644–651. [Google Scholar]
- Murray, M.P.; Mollinger, L.A.; Gardner, G.M.; Sepic, S.B. Kinematic and EMG patterns during slow, free, and fast walking. J. Orthop. Res. 1984, 2, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Mulroy, S.; Gronley, J.; Weiss, W.; Newsam, C.; Perry, J. Use of cluster analysis for gait pattern classification of patients in the early and late recovery phases following stroke. Gait Posture 2003, 18, 114–125. [Google Scholar] [CrossRef]
- Dorsch, S.; Ada, L.; Canning, C.G.; Al-Zharani, M.; Dean, C. The strength of the ankle dorsiflexors has a significant contribution to walking speed in people who can walk independently after stroke: An observational study. Arch. Phys. Med. Rehabil. 2012, 3, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Park, D.H.; Bae, Y.S. Proprioceptive neuromuscular facilitation kinesio taping improves range of motion of ankle dorsiflexion and balance ability in chronic stroke patients. Healthcare 2021, 9, 1426. [Google Scholar] [CrossRef] [PubMed]
- Daniele, V.; Andrea, P.; Ugo, M. Ankle elastic taping: Stabilometric and electromyographic evaluation of postural control. Sci. Riabil. 2015, 17, 21–32. [Google Scholar]
- De Oliveira, C.B.; de Medeiros, Í.R.T.; Ferreira, N.A.; Greters, M.E.; Conforto, A.B. Balance control in hemiparetic stroke patients: Main tools for evaluation. J. Rehabil. Res. Dev. 2008, 45, 1215–1226. [Google Scholar] [CrossRef]
- Eng, J.J.; Chu, K.S. Reliability and comparison of weight-bearing ability during standing tasks for individuals with chronic stroke. Arch. Phys. Med. Rehabil. 2002, 83, 1138–1144. [Google Scholar] [CrossRef] [PubMed]
- Tasseel-Ponche, S.; Yelnik, A.; Bonan, I. Motor strategies of postural control after hemispheric stroke. NCNR 2015, 45, 327–333. [Google Scholar] [CrossRef]
- Marigold, D.S.; Eng, J.J. The relationship of asymmetric weight-bearing with postural sway and visual reliance in stroke. Gait Posture 2006, 23, 249–255. [Google Scholar] [CrossRef]
- Das, S.; Haji Suhaimi, F.; Abd Latiff, A.; Pa Pa Hlaing, K.; Abd Ghafar, N.; Othman, F. Absence of the peroneus tertius muscle: Cadaveric study with clinical considerations. Rom. J. Morphol. Embryol. 2009, 50, 509–511. [Google Scholar]
- Oyedun, O.S.; Kanu, L.C.; Onatola, O.A.; Zelibe, P.O. Does peroneal tertius in absentia affect the range of motion of foot dorsiflexion and eversion? A kinesio-anatomical study. Adv. Life Sci. Technol. 2014, 21, 69–75. [Google Scholar]
- Yildiz, S.; Yalcin, B. An unique variation of the peroneus tertius muscle. Surg. Radiol. Anat. 2012, 34, 661–663. [Google Scholar] [CrossRef] [PubMed]
- Lemos, T.V.; Pereira, K.C.; Protássio, C.C.; Lucas, L.B.; Matheus, J.P.C. The effect of Kinesio Taping on handgrip strength. J. Phys. Ther Sci. 2015, 27, 567–570. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Soares, M.; Lopes, A.J.; dos Santos Vigario, P.; Souza, M.P.; da Costa, H.F.; Felicio, L.R. Does the kinesio tape provide more knee extensor torque? Asian J. Sports Med. 2018, 9, e63946. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Classification | EDLT Group (n = 20) | TAT Group (n = 20) | p |
|---|---|---|---|
| Gender (male/female) | 13/7 | 13/7 | 1.000 a |
| Paretic side (right/left) | 12/8 | 11/9 | 1.000 a |
| Type (infarction/hemorrhages) | 13/7 | 15/5 | 0.731 a |
| Disease duration (months) | 14.10 ± 3.80 | 13.85 ± 3.69 | 0.834 b |
| Age (years) | 63.00 ± 7.62 | 63.45 ± 7.96 | 0.856 b |
| Height (cm) | 165.60 ± 8.59 | 162.60 ± 7.04 | 0.234 b |
| Weight (kg) | 70.20 ± 7.74 | 68.20 ± 6.29 | 0.376 b |
| K-MMSE (score) | 26.70 ± 1.75 | 27.05 ± 1.73 | 0.529 b |
| Classification | Before Intervention | After Intervention | Tests of Within-Subjects Effects | Tests of between-Subjects Effects | ||
|---|---|---|---|---|---|---|
| F | p | F | p | |||
| Total area (mm2) | ||||||
| EDLT group | 2033.90 ± 255.81 | 2460.55 ± 378.12 a | 81.534 | 0.001 ** | 0.578 | 0.452 |
| TAT group | 1987.55 ± 259.27 | 2370.75 ± 354.28 a | ||||
| Cadence (step/min) | ||||||
| EDLT group | 86.96 ± 11.73 | 92.92 ± 10.0 a | 58.515 | 0.001 ** | 0.266 | 0.609 |
| TAT group | 84.81 ± 11.71 | 90.45 ± 12.02 a | ||||
| Gait Speed (m/s) | ||||||
| EDLT group | 0.63 ± 0.12 | 0.78 ± 0.08 a | 74.251 | 0.001 ** | 3.918 | 0.055 |
| TAT group | 0.57 ± 0.12 | 0.71 ± 0.14 a | ||||
| Stride Length (m) | ||||||
| EDLT group | 0.89 ± 0.19 | 1.02 ± 0.11 a | 47.559 | 0.001 ** | 0.001 | 0.978 |
| TAT group | 0.82 ± 0.21 | 0.95 ± 0.19 a | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, K.-H.; Park, S.-J. Effects of Extensor Digitorum Longus and Tibialis Anterior Taping on Balance and Gait Performance in Patients Post Stroke. Healthcare 2022, 10, 1692. https://doi.org/10.3390/healthcare10091692
Cho K-H, Park S-J. Effects of Extensor Digitorum Longus and Tibialis Anterior Taping on Balance and Gait Performance in Patients Post Stroke. Healthcare. 2022; 10(9):1692. https://doi.org/10.3390/healthcare10091692
Chicago/Turabian StyleCho, Kyun-Hee, and Shin-Jun Park. 2022. "Effects of Extensor Digitorum Longus and Tibialis Anterior Taping on Balance and Gait Performance in Patients Post Stroke" Healthcare 10, no. 9: 1692. https://doi.org/10.3390/healthcare10091692