
A Simulation-Based Clinical Nursing Education Framework for a Low-Resource Setting: A Multimethod Study



Abstract
:1. Introduction
2. Materials and Methods
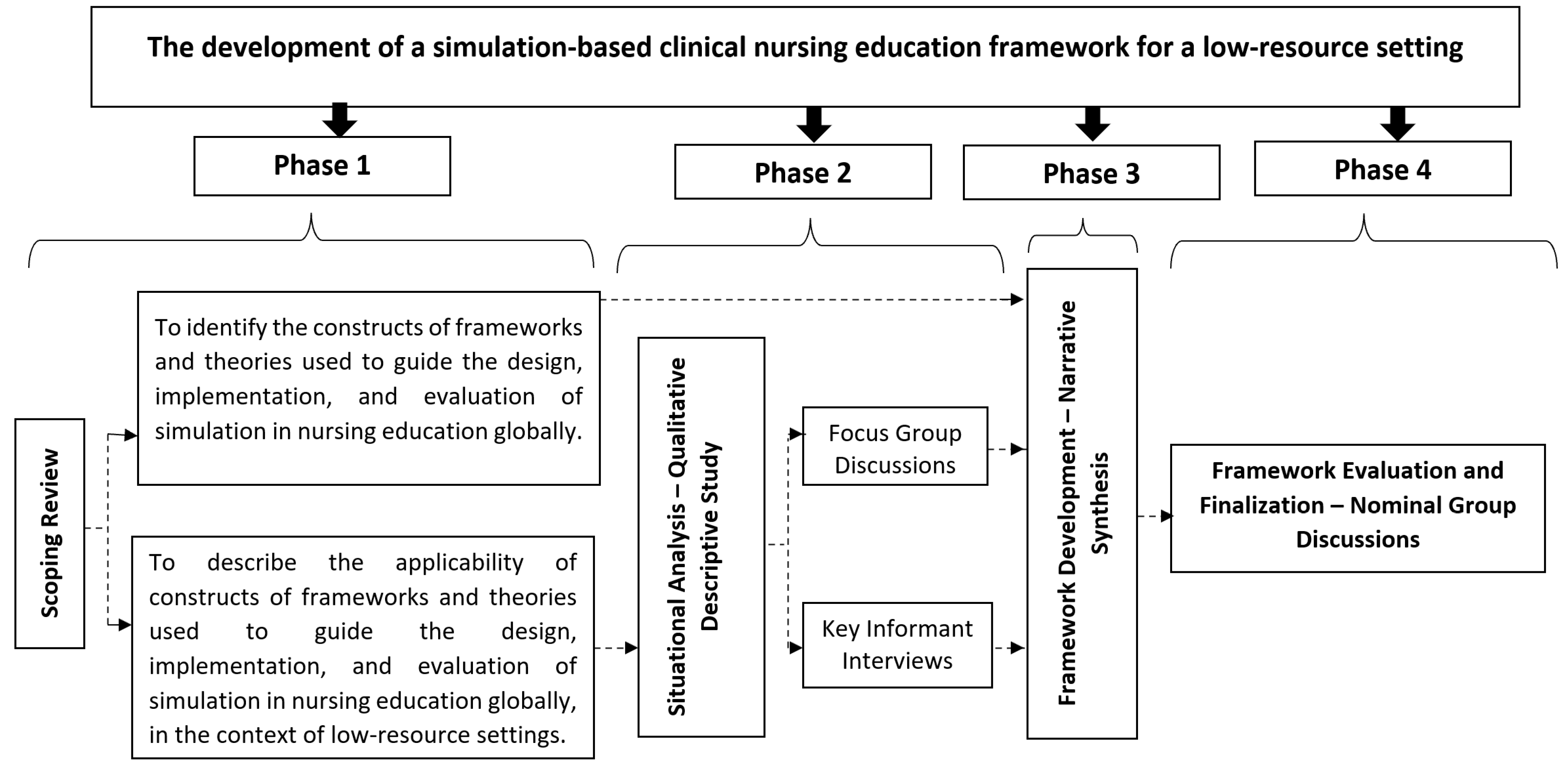
2.1. Design
2.1.1. Phase 1: Scoping Review
2.1.2. Phase 2: Situational Analysis–Qualitative Descriptive Study
2.1.3. Phases 3 and 4: The Development and Evaluation of the Framework
2.2. Ethics Approval
2.3. Rigor
3. Results
3.1. Phase 1: Scoping Review
3.2. Phase 2: Situational Analysis–Qualitative Descriptive Study
3.3. Evaluation of the Framework: Nominal Group Discussion
3.3.1. Category 1: Appropriateness, Acceptability, and Applicability
“…I strongly believe the framework is well structured, all the components of the framework are well related”.NGDPRN1
“I think if the framework is well implemented it is going to produce an excellent result at the end of the day, its objective of equipping nursing students with clinical competence is going to be achieved”.NGDPRN3
3.3.2. Category 2: Suggested Modifications
“The teaching and learning strategies aren’t living entities to co-exist with facilitators and participants in a team bound by mutual trust”. This relationship could be illustrated by expanding the community of learning to include the other members such as clinicians, other students, and other nurse educators as the three actors bound by the mutual respect and teamwork”.NGDNE1
“If learning has to be sustainable, the community of learning has to include other students, clinicians, the regulatory bodies, and all other persons who the students interact with during their learning journey”.NGDNE1
“Teaching and learning strategies should also be renamed as immersive teaching and learning strategies for the purpose of specificity and placed in the middle of the community of learning together with teamwork”.NGDNE1
3.3.3. Category 3: Development Process
“Well, with how it was developed that was how actually it should be done. You involved people who are into it, the framework is designed to develop the students, and in developing these students, it is the nurse educators that are supposed to help the students develop those competencies, and you spoke to both students and the nurse educators and went ahead and reviewed the literature that was available. So, the development process of the framework was okay and I think is good”.NGDPRN4
“Since it’s a framework you are trying to develop, I think doing a scoping review to find out what already exists and what has already been done in the field and also requesting the views of the implementers, that is the nurse educators and the students, would be a good idea. It is good because you will be able to draw a comparison”.NGDNE2
3.4. The Simulation-Based Clinical Nursing Education Framework for a Low-Resource Setting
3.4.1. Context
3.4.2. Planning
Needs Assessment
Skills Laboratory Retooling
Preparation/Training/Orientation
Facilitators
Participants and Other Members of the Simulation Community of Learning
Curriculum Integration
3.4.3. Design
Learning Objectives
Scenario Development
Simulation Modality
Pre-Briefing
Videography
Structured Debriefing
3.4.4. Community of Learning
Facilitator
Participant
Other Members
Immersive Teaching and Learning Strategies
Interactive Learning
Station Teaching
Time on Task
Guided Reflection
Deliberate Practice
Peer Learning
Teamwork
Support
Feedback
Outcomes
4. Discussion
5. Conclusions
6. Strengths and Limitations
7. Implications of the Study
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, L.; Williams, E.P. Contemporary Models for Clinical Nursing Education; Sigma Repository: Hattiesburg, MI, USA, 2017; Available online: http://hdl.handle.net/10755/623704 (accessed on 1 February 2022).
- Niederhauser, V.; Schoessler, M.; Gubrud-Howe, P.M.; Magnussen, L.; Codier, E. Creating innovative models of clinical nursing education. J. Nurs. Educ. 2012, 51, 603–608. [Google Scholar] [CrossRef] [PubMed]
- The Nursing Education Stakeholders Group. A poposed model for clinical nursing education and training in South Africa. Trend Nurs. 2012, 1, 152. [Google Scholar]
- Dahlke, S.; O’Connor, M.; Hannesson, T.; Cheetham, K. Understanding clinical nursing education: An exploratory study. Nurse Educ. Pract. 2016, 17, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Heidari, M.R.; Norouzadeh, R. Nursing students’ perspectives on clinical education. J. Adv. Med. Educ. Prof. 2015, 3, 39–43. [Google Scholar]
- Flood, L.S.; Robinia, K. Bridging the gap: Strategies to integrate classroom and clinical learning. Nurse Educ. Pract. 2014, 14, 329–332. [Google Scholar] [CrossRef]
- Kalayi, G.; Akintola, A.A. Preceptorship: Bridging the theory practice gap and enhancing transition of new graduates. Int. J. Nurs. Care 2013, 1, 25. [Google Scholar] [CrossRef]
- Jeffries, P.R. The NLN Jeffries Simulation Theory, 1st ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2016. [Google Scholar]
- Aebersold, M. Simulation-Based Learning: No Longer a Novelty in Undergraduate Education. Online J. Issues Nurs. 2018, 23. [Google Scholar] [CrossRef]
- American Association of Colleges of Nursing. Fact Sheet: Nursing Shortage. 2017. [cited 5 January 2022]. pp. 1–6. Available online: https://www.aacnnursing.org/news-information/fact-sheets/nursing-shortage (accessed on 5 February 2022).
- Salifu, D.A.; Gross, J.; Salifu, M.A.; Ninnoni, J.P.K. Experiences and perceptions of the theory-practice gap in nursing in a resource-constrained setting: A qualitative description study. Nurs. Open 2019, 6, 72–83. [Google Scholar] [CrossRef]
- Salifu, D.A.; Heymans, Y.; Christmals, C.D. Teaching and Learning of Clinical Competence in Ghana: Experiences of Students and Post-Registration Nurses. Healthcare 2022, 10, 538. [Google Scholar] [CrossRef]
- Cook, D.A.; Brydges, R.; Hamstra, S.J.; Zendejas, B.; Szostek, J.H.; Wang, A.T.; Erwin, P.J.; Hatala, R. Comparative Effectiveness of Technology-Enhanced Simulation Versus Other Instructional Methods. Simul. Healthc. 2012, 7, 308–320. [Google Scholar] [CrossRef]
- Turale, S.; Ito, M.; Nakao, F. Issues and challenges in nursing and nursing education in Japan. Nurse Educ. Pract. 2008, 8, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Pirie, J.; Kappus, L.; Sudikoff, S.N.; Bhanji, F. Simulation Curriculum Development, Competency-Based Education, and Continuing Professional Development. In Comprehensive Healthcare Simulation: Pediatrics; Springer: Cham, Switzerland, 2016; pp. 181–193. [Google Scholar] [CrossRef]
- Arthur, C.; Levett-jones, T.; Kable, A. Quality indicators for the design and implementation of simulation experiences: A Delphi study. Nurse Educ. Today 2013, 33, 1357–1361. [Google Scholar] [CrossRef]
- Massoth, C.; Röder, H.; Ohlenburg, H.; Hessler, M.; Zarbock, A.; Pöpping, D.M.; Wenk, M. High-fidelity is not superior to low-fidelity simulation but leads to overconfidence in medical students. BMC Med. Educ. 2019, 19, 29. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, W. Transforming and Scaling up Health Professionals’ Education and Training: World Health Organization Guidlines 2013; WHO: Geneva, Switzerland, 2013; Available online: Who.int/iris/bitstream/handle/10665/93635/9789241506502_eng.pdf;jsessionid=87B4A0ECDDA6510BD2F68A5192F78FC9?sequence=1 (accessed on 7 February 2022).
- WHO Regional Office for Europe. Simulation in Nursing and Midwifery Education; WHO Regional Office for Europe: Scotland, UK, 2018; Available online: https://www.euro.who.int/__data/assets/pdf_file/0011/383807/snme-report-eng.pdf (accessed on 11 February 2022).
- Park, K.; Ahn, Y.; Kang, N.; Sohn, M. Development of a simulation-based assessment to evaluate the clinical competencies of Korean nursing students. Nurse Educ. Today 2016, 36, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Agha, S.; Ahamrani, A.Y.; Khan, M.A. Satisfaction of medical students with simulation-based learning. Saudi Med. J. 2015, 36, 731–736. [Google Scholar] [CrossRef]
- Aqel, A.A.; Ahmad, M.M. High-fidelity stimulation effects on CPR knowledge, skills, acquisition, and retention in nursing students. Worldviews Evid.-Based Nurs. 2014, 11, 394–400. [Google Scholar] [CrossRef]
- Farzi, S.; Shahriari, M.; Farzi, S. Exploring the challenges of clinical education in nursing and strategies to improve it: A qualitative study. J. Educ. Health Promot. 2019, 7, 115. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.; Shin, S. Effectiveness of simulation-based nursing education depending on fidelity: A meta-analysis. BMC Med. Educ. 2016, 16, 152. [Google Scholar] [CrossRef]
- Shin, I.; Kim, J.H. The effect of problem-based learning in nursing education: A meta- analysis. Adv. Health Sci. Educ. Theory Pract. 2013, 18, 1103–1120. [Google Scholar] [CrossRef]
- Bvumbwe, T.; Mtshali, N. Nursing education challenges and solutions in Sub Saharan Africa: An integrative review. BMC Nurs. 2018, 17, 3. [Google Scholar] [CrossRef]
- Salifu, D.; Christmals, C.; Reitsma, G.M. Frameworks for the design, implementation, and evaluation of simulation-based nursing education: A scoping review. Nurs. Health Sci. Online ahead of print. [CrossRef]
- Cioffi, J. Clinical simulations: Development and validation. Nurse Educ. Today 2001, 21, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, M.A.; Biddle, C.; Fallacaro, M. Assessing the authenticity of the human simulation experience in anesthesiology. J. Am. Assoc. Nurse Anesth. 2002, 70, 470–473. [Google Scholar]
- Cowperthwait, A. NLN/Jeffries Simulation Framework for Simulated Participant Methodology. Clin. Simul. Nurs. 2020, 42, 12–21. [Google Scholar] [CrossRef]
- Daley, K.M.; Campbell, S.H. Framework for Simulation Learning in Nursing Education. In Simulation Scenarios for Nursing Educators: Making It Real, 3rd ed.; Campbell, S.H., Daley, K., Eds.; Springer: New York, NY, USA; pp. 22–23.
- Jeffries, P.R. Simulation in Nursing Education: From Conceptualization to Evaluation, 2nd ed.; National League for Nursing: New York, NY, USA, 2012. [Google Scholar]
- Kunst, E.L.; Henderson, A.; Johnston, A.N.B. A Scoping Review of the Use and Contribution of Simulation in Australian Undergraduate Nurse Education. Clin. Simul. Nurs. 2018, 19, 17–29. [Google Scholar] [CrossRef]
- Christmals, C.D.; Armstrong, S.J. Curriculum framework for advanced practice nursing in sub-Saharan Africa: A multimethod study. BMJ Open 2020, 10, e035580. [Google Scholar] [CrossRef] [PubMed]
- Hunter, A.; Brewer, J.D.J.D. Designing Multimethod Research: The Oxford Handbook of Multimethod and Mixed Methods Research Inquiry; Oxford University Press: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Mafuba, K.; Gates, B. Sequential multiple methods as a contemporary method in learning disability nursing practice research. J. Intellect. Disabil. 2012, 16, 287–296. [Google Scholar] [CrossRef]
- Tashakkori, A.; Teddie, C. SAGE Handbook of Mixed Methods in Social and Behavioural Research, 2nd ed.; SAGE Publications Limited: London, UK, 2010. [Google Scholar]
- Ellis, T.J.; Levy, Y. A Guide for Novice Researchers: Design and Development Research Methods. Informing Science & IT Education Conference (InSITE). 2010, pp. 107–118. Available online: http://proceedings.informingscience.org/InSITE2010/InSITE10p107-118Ellis725.pdf (accessed on 13 February 2022).
- Peffers, K.; Tuunanen, T.; Rothenberger, M.A.; Chatterjee, S.; Peffers, K.; Tuunanen, T.; Rothenberger, M.A.; Chatterjee, S. A Design Science Research Methodology for Information Systems Research. J. Manag. Inf. Syst. 2007, 24, 45–78. Available online: http://www.tuunanen.fi (accessed on 21 December 2021). [CrossRef]
- Salifu, D.; Heymans, Y.; Christmals, C.D. Facilitating the Development of Clinical Competence in a Low-Resource Setting: Perceptions and Challenges of Nurse Educators. Nurse Media J. Nurs. 2022, 12, 42–60. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef]
- Pope, C.; Ziebland, S.; Mays, N. Analyzing qualitative data. Qual. Res. Health Care. Br. Med. J. 2000, 320, 114–116. [Google Scholar]
- Hmelo-Silver, C.E.; Duncan, R.G.; Chinn, C.A. Scaffolding and achievement in problem-based and inquiry learning: A response to Kirschner, Sweller, and Clark (2006). Educ. Psychol. 2007, 42, 99–107. [Google Scholar] [CrossRef]
- Lavoie, P.; Michaud, C.; Bélisle, M.; Boyer, L.; Gosselin, É.; Grondin, M.; LaRue, C.; Lavoie, S.; Pepin, J. Learning theories and tools for the assessment of core nursing competencies in simulation: A theoretical review. J. Adv. Nurs. 2017, 74, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Snilstveit, B.; Oliver, S.; Vojtkova, M. Narrative approaches to systematic review and synthesis of evidence for international development policy and practice. J. Dev. Eff. 2012, 4, 409–429. [Google Scholar] [CrossRef]
- Dobbie, A.; Rhodes, M.; Tysinger, J.W.; Freeman, J. Using a modified nominal group technique as a curriculum evaluation tool. Fam. Med. 2004, 36, 402–406. [Google Scholar]
- Lloyd-Jones, G.; Fowell, S.; Bligh, J.G. The use of the nominal group technique as an evaluative tool in medical undergraduate education. Med. Educ. 1999, 33, 8–13. [Google Scholar] [CrossRef]
- Anim-Boamah, O. The Development of a Framework for Assessing Clinical Competence of Nursing Students in Ghana: A Multimethod Study; University of Witwatersrand: Johannesburg, South Africa, 2021. [Google Scholar]
- Perry, J.; Linsley, S. The use of nominal group technique as an evaluative tool in the teaching and summative assessment of the inter-personal skills of student mental health nurses. Nurse Educ. Today 2006, 26, 346–353. [Google Scholar] [CrossRef]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef]
- Gearing, R. Bracketing in research: A typology. Qual. Health Res. 2004, 14, 1429–1452. [Google Scholar] [CrossRef] [PubMed]
- Valle, R.S.; King, M.; Halling, S. An introduction to existential- phenomenological thought in psychology. In Existential-Phenomenological Perspectives in Psychology. Exploring the Breadth of Human Experience; Valle, R.S., Halling, S., Eds.; Plenum Press: New York, NY, USA, 1989. [Google Scholar]
- INACSL Standards Committee. INACSL Standards of Best Practice: SimulationSM Simulation Design. Clin. Simul. Nurs. 2016, 12, S5–S12. [Google Scholar] [CrossRef]
- Munangatire, T.; Naidoo, N. Exploration of high-fidelity simulation: Nurse educators’ perceptions and experiences at a school of nursing in a resource-limited setting. Afr. J. Health Prof. Educ. 2017, 9, 44–47. [Google Scholar] [CrossRef]
- Huffman, J.L.; McNeil, G.; Bismilla, Z.; Lai, A. Essentials of Scenario Building for Simulation- Based Education. In Comprehensive Healthcare Simulation: Pediatrics; Grant, V., Cheng, A., Eds.; Springer: Geneva, Switzerland, 2016; pp. 19–29. [Google Scholar] [CrossRef]
- Clapper, T.C.; Kardong-Edgren, S. Using Deliberate Practice and Simulation to Improve Nursing Skills. Clin. Simul. Nurs. 2012, 8, e109–e113. [Google Scholar] [CrossRef]
- Coutinho, V.R.D.; Martins, J.C.A.; Pereira, F. Structured debriefing in nursing simulation: Students’ perceptions. J. Nurs. Educ. Pract. 2016, 6, 127–134. [Google Scholar] [CrossRef]
- Botma, Y.; Rensburg, G.H.; Van Coetzee, I.M.; Heyns, T. A conceptual framework for educational design at modular level to promote transfer of learning. Innov. Educ. Teach. Int. 2016, 52, 499–509. [Google Scholar] [CrossRef]
- Billings, D.M.; Halstead, J.A. Teaching in Nursing: A Guide for Faculty, 2nd ed.; Elsevier Inc.: St. Louis, MO, USA, 2005. [Google Scholar]
- Bruce, J.; Klopper, H.; Mellish, J. Teaching and Learning the Practice of Nursing, 5th ed.; Pearson Education: Cape Town, South Africa, 2011. [Google Scholar]
- Hope, A.; Garside, J.; Prescott, S. Rethinking theory and practice: Pre-registration student nurses experiences of simulation teaching and learning in the acquisition of clinical skills in preparation for practice. Nurse Educ. Today. 2011, 31, 711–715. [Google Scholar] [CrossRef]
- Partin, J.L.; Payne, T.A.; Slemmons, M.F. Students’ perceptions of their learning experiences using high-fidelity simulation to teach concepts relative to obstetrics. Nurs. Educ. Perspect. 2011, 32, 186–188. [Google Scholar] [CrossRef]
- Cook, D.A.; Brydges, R.; Zendejas, B.; Hamstra, S.J.; Hatala, R. Technology-Enhanced Simulation to Assess Health Professionals: A Systematic Review of Validity Evidence, Research Methods, and Reporting Quality. Academic Medicine; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2013; pp. 872–883. [Google Scholar] [CrossRef]
- Issenberg, S.B.; McGaghie, W.C.; Petrusa, E.R.; Gordon, D.L.; Scalese, R.J. Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Med. Teach. 2005, 27, 10–28. [Google Scholar] [CrossRef]
- Jeffries, P.R. A framework for designing, implementing, and evaluating: Simulations used as teaching strategies in nursing. Nurs. Educ. Perspect. 2005, 26, 96–103. [Google Scholar] [CrossRef]
- Padden-Denmead, M.L.; Scaffidi, R.M.; Kerley, R.M.; Farside, A.L. Simulation with debriefing and guided reflective journaling to stimulate critical thinking in prelicensure baccalaureate degree nursing students. J. Nurs Educ. 2016, 55, 645–650. [Google Scholar] [CrossRef]
- Welch, T.D.; Carter, M. Deliberate Practice and Skill Acquisition in Nursing Practice. J. Contin. Educ. Nurs. 2018, 49, 269–273. [Google Scholar] [CrossRef]
- Levin, O.; Flavian, H. Simulation-based learning in the context of peer learning from the perspective of preservice teachers: A case study. Eur. J. Teach. Educ. 2020, 10, 373–394. [Google Scholar] [CrossRef]
- Havnes, A.; Christiansen, B.; Bjørk, I.T.; Hessevaagbakke, E. Peer learning in higher education: Patterns of talk and interaction in skills centre simulation. Learn. Cult. Soc. Interact. 2016, 8, 75–87. [Google Scholar] [CrossRef]
- Abd, R.; Ahmed, E.S.; Gad, A.; Administration, N.; Nursing, F. Nursing Interns ’ Perceived Feedback and its Influence on Gaining 21 st Century Skills. J. Nurs. Health Sci. 2019, 8, 89–103. [Google Scholar] [CrossRef]
- Yu, J.H.; Chang, H.J.; Kim, S.S.; Park, J.E.; Chung, W.Y.; Lee, S.K.; Kim, M.; Lee, J.H.; Jung, Y.J. Effects of high-fidelity simulation education on medical students’ anxiety and confidence. PLoS ONE 2021, 16, e0251078. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.A.; Andersen, D.K.; Combes, J.R.; Feldman, D.L.; Sachdeva, A.K. The value proposition of simulation-based education. Surgery 2018, 163, 944–949. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Rodríguez, D.; Arrogante, O. Simulated Video Consultations as a Learning Tool in Undergraduate Nursing: Students’ Perceptions. Healthcare 2020, 8, 280. [Google Scholar] [CrossRef]
- Cortés-Rodríguez, A.E.; Roman, P.; López-Rodríguez, M.M.; Fernández-Medina, I.M.; Fernández-Sola, C.; Hernández-Padilla, J.M. Role-Play versus Standardised Patient Simulation for Teaching Interprofessional Communication in Care of the Elderly for Nursing Students. Healthcare 2021, 10, 46. [Google Scholar] [CrossRef]
- Lapkin, S.; Levett-Jones, T. EDUCATIONAL ISSUES IN NURSING PRACTICE A cost-utility analysis of medium vs. high-fidelity human patient simulation manikins in nursing education. J. Clin. Nurs. 2011, 20, 3543–3552. [Google Scholar] [CrossRef]
- Burch, V. Does simulation-based training have a future in Africa? Editorial. Afr. J. Health Prof. Educ. 2014, 6, 117–119. [Google Scholar] [CrossRef]
- Cheng, A.; Lockey, A.; Bhanji, F.; Lin, Y.; Hunt, E.A.; Lang, E. The use of high- fidelity manikins for advanced life support training—A systematic review and metaanalysis. Resuscitation 2015, 93, 142–149. [Google Scholar] [CrossRef]
- Nimbalkar, A.; Patel, D.; Kungwani, A.; Phatak, A.; Vasa, R.; Nimbalkar, S. Randomized control trial of high-fidelity vs low-fidelity simulation for training undergraduate students in neonatal resuscitation. BMC Res. Notes 2015, 8, 636. [Google Scholar] [CrossRef] [Green Version]
- Talley, B. Nurses and nursing education in Ghana: Creating collaborative opportunities. Int. Nurs. Rev. 2006, 53, 47–51. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Part 1–Focus Group Discussions | Part 2–Semi-Structured Interviews | |
|---|---|---|
| Population | Post-registration diploma nurses within their first year of practice and nursing students (second- and third-year students) from six different sites (three NEIs which were all accredited diploma-awarding public nursing colleges and their primary clinical sites) in three geographical (northern, middle, and southern) zones of Ghana, a low-resource setting. | Nurse educators with full appointment and working in an accredited diploma-awarding public nursing college in the three geographical (northern, middle, and southern) zones of Ghana, a low-resource setting with three years’ experience in the teaching of practical skills and facilitating clinical competence development and fluent in English. |
| Aim | The study explored and described the experiences and perceptions of nursing students and post-registration nurses in the teaching and learning of clinical competence in Ghana, a low-resource setting. | To explore and describe the perceptions and challenges of nurse educators in in the teaching of practical skills and in facilitating the development of clinical competence in diploma nursing education in Ghana, a low-resource setting. Additionally, the study also explored and described the pedagogical strategies used by nurse educators in the teaching of practical skills and clinical competence development in Ghana, a low-resource setting. |
| Question 1 Indicate below what you believe is/are the strength(s)/weakness(es) of this simulation-based clinical nursing education framework per the areas listed? When indicating the weaknesses of the framework, make suggestion in how to better the weaknesses. | |||
| Areas | Strength | Weakness | Suggestions |
| Structure (The graphical illustration of the phenomenon) | |||
| Components (Inter-relations of the main and sub-components) | |||
| Acceptability/Applicability | |||
| Development process | |||
Question 2
Others: Provide further comment(s) you believe can help improve the applicability of the simulation-based nursing education framework. | |||
| Variables | Students | Post-Registration Nurses | Nurse Educators |
|---|---|---|---|
| Gender | |||
| Male | 5 | 4 | 1 |
| Female | 3 | 2 | 5 |
| Age (in years) | |||
| 21–25 | 6 | 2 | |
| 26–30 | 2 | 4 | |
| 31–35 | - | - | 1 |
| 36–40 | - | - | 1 |
| 41–45 | - | - | 3 |
| 46–50 | - | - | - |
| 51–55 | - | - | 1 |
| Programme level | |||
| Second year | 4 | - | - |
| Third year | 4 | - | - |
| Zone | |||
| Northern zone | 3 | 2 | 2 |
| Middle zone | 3 | 2 | 2 |
| Southern zone | 2 | 2 | 2 |
| Work experience (in years) | |||
| 1–5 | - | 6 | 2 |
| 6–10 | - | - | 3 |
| 11–15 | - | - | - |
| 16–20 | - | - | 1 |
| Highest academic qualification | |||
| Diploma | - | - | - |
| Bachelor’s degree | - | - | - |
| Master’s degree | - | - | 5 |
| MPhil | - | - | 1 |
| Doctorate degree | - | - | - |
| Professional qualification in teaching | |||
| Diploma in Education | - | - | - |
| Bachelor of Education Health Sciences | - | - | 3 |
| Post-graduate diploma in education (PGDE) | - | - | 1 |
| Masters in Nursing Education | 1 | ||
| Master of Education | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salifu, D.A.; Heymans, Y.; Christmals, C.D. A Simulation-Based Clinical Nursing Education Framework for a Low-Resource Setting: A Multimethod Study. Healthcare 2022, 10, 1639. https://doi.org/10.3390/healthcare10091639
Salifu DA, Heymans Y, Christmals CD. A Simulation-Based Clinical Nursing Education Framework for a Low-Resource Setting: A Multimethod Study. Healthcare. 2022; 10(9):1639. https://doi.org/10.3390/healthcare10091639
Chicago/Turabian StyleSalifu, David Abdulai, Yolande Heymans, and Christmal Dela Christmals. 2022. "A Simulation-Based Clinical Nursing Education Framework for a Low-Resource Setting: A Multimethod Study" Healthcare 10, no. 9: 1639. https://doi.org/10.3390/healthcare10091639