
Artificial Intelligence Analysis of Ulcerative Colitis Using an Autoimmune Discovery Transcriptomic Panel


Abstract
:1. Introduction
2. Materials and Methods
3. Results
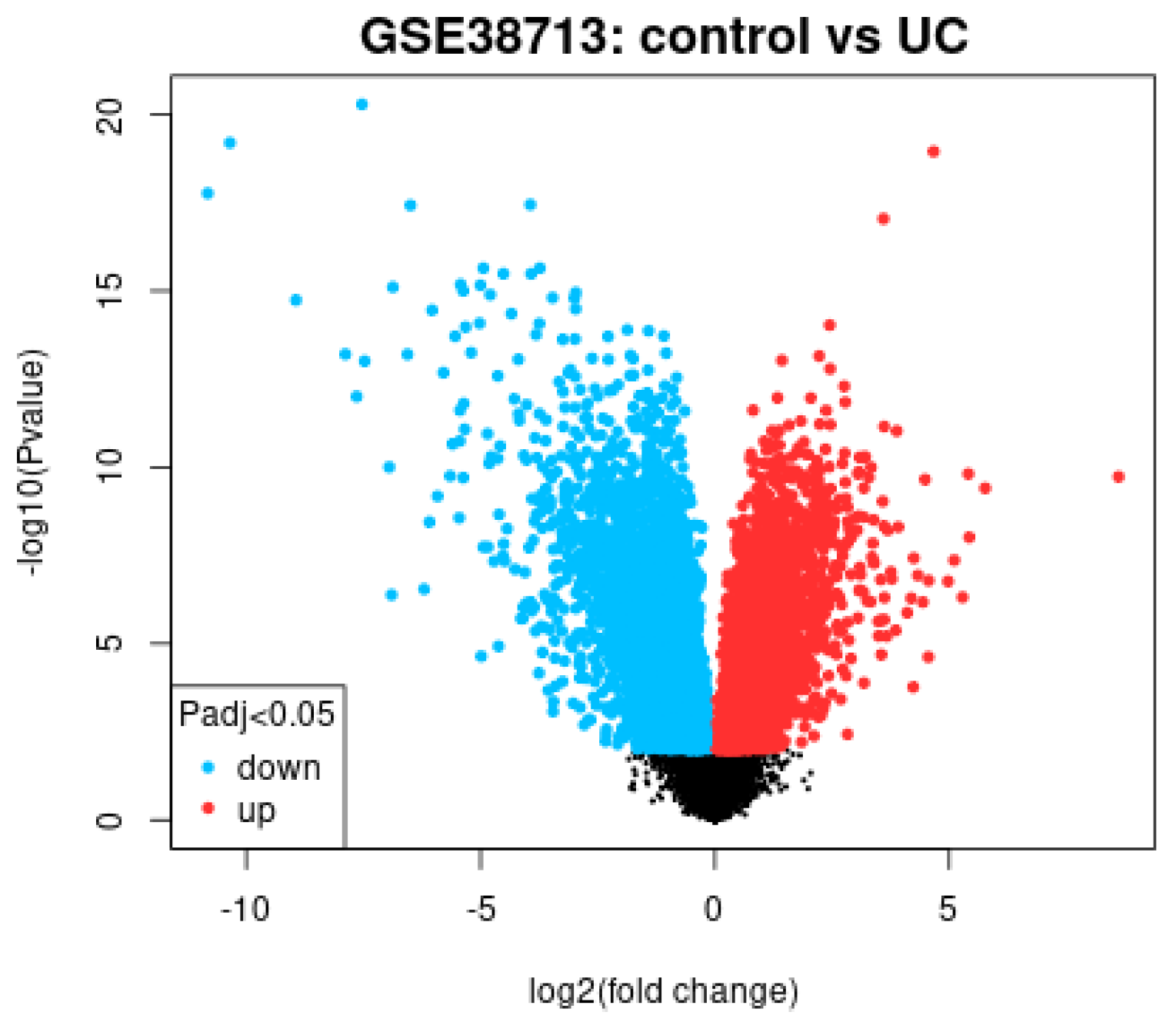
- Conventional gene expression analysis using volcano plot differentiated the expression of active ulcerative colitis vs healthy donors broadly using all the genes of the array.
- Gene set enrichment analysis (GSEA) using an autoimmune discovery panel showed enrichment toward the ulcerative colitis phenotype, highlighting the most relevant genes in the leading edge.
- Several machine learning and artificial neural network analyses predicted ulcerative colitis against healthy donors using the autoimmune discovery gene expression panel.
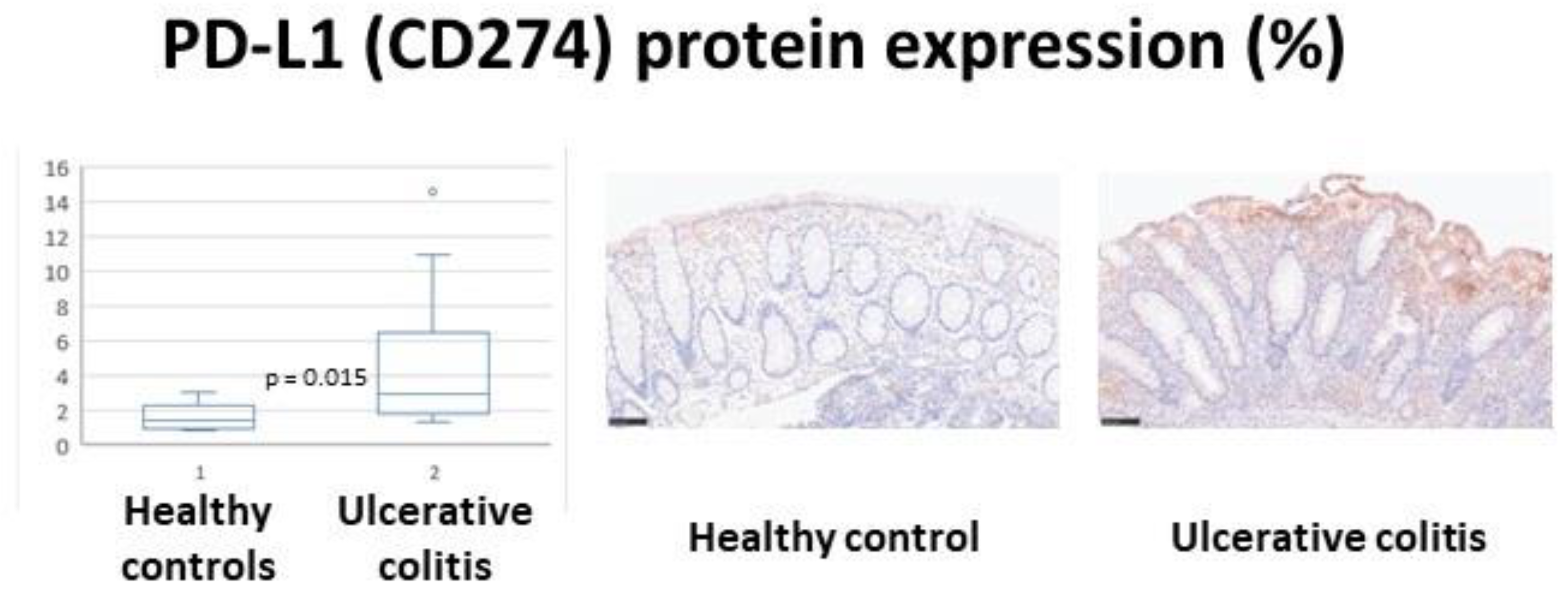
- A high expression of programmed cell death 1 ligand 1 (PD-L1, CD274) in ulcerative colitis was validated in an independent series using immunohistochemistry analysis for histological identification of protein expression.
3.1. Conventional Analysis Using the GEO2R Software
3.2. Gene Set Enrichment Analysis (GSEA) Using an Autoimmune Discovery Panel
3.3. Machine Learning and Artificial Neural Networks
3.3.1. Ulcerative Colitis Versus Healthy Controls
3.3.2. Ulcerative Colitis (Involved Active, Non-Involved Active, and Inactive/Remission) Versus Healthy Controls
3.4. Validation of CD274 (PD-L1) in an Independent Series
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | PD-L1 (%) | Biopsy | Age | Sex | Baron Score | Geboes Score |
|---|---|---|---|---|---|---|
| Control | 0.84 | Rectum | 64 | Male | - | - |
| Control | 1.14 | Descending | 56 | Male | - | - |
| Control | 1.45 | Descending | 59 | Male | - | - |
| Control | 1.45 | Rectum | 26 | Male | - | - |
| Control | 3.09 | Rectum | 59 | Female | - | - |
| Ulcerative colitis | 1.38 | Rectum | 51 | Male | 1 | 1 |
| Ulcerative colitis | 1.47 | Sigmoid | 31 | Female | 2 | 2 |
| Ulcerative colitis | 1.61 | Rectum | 37 | Female | 1 | 2 |
| Ulcerative colitis | 1.80 | Rectum | 37 | Female | 2 | 2 |
| Ulcerative colitis | 2.06 | Rectum | 33 | Male | 2 | 3 |
| Ulcerative colitis | 2.24 | Rectum | 77 | Female | 2 | 2 |
| Ulcerative colitis | 2.97 | Rectum | 46 | Male | 1 | 3 |
| Ulcerative colitis | 2.98 | Sigmoid | 41 | Male | 2 | 3 |
| Ulcerative colitis | 4.74 | Rectum | 59 | Male | 1 | 2 |
| Ulcerative colitis | 6.34 | Rectum | 23 | Male | 2 | 2 |
| Ulcerative colitis | 4.04 | Rectum | 22 | Female | 2 | 4 |
| Ulcerative colitis | 6.52 | Sigmoid | 43 | Female | 3 | 2 |
| Ulcerative colitis | 6.89 | Descending | 54 | Female | 2 | 4 |
| Ulcerative colitis | 10.99 | Rectum | 20 | Male | 3 | 4 |
| Ulcerative colitis | 14.55 | Descending | 17 | Female | 2 | 2 |
References
- Silverberg, M.S.; Satsangi, J.; Ahmad, T.; Arnott, I.D.R.; Bernstein, C.N.; Brant, S.R.; Caprilli, R.; Colombel, J.-F.; Gasche, C.; Geboes, K.; et al. Toward an Integrated Clinical, Molecular and Serological Classification of Inflammatory Bowel Disease: Report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can. J. Gastroenterol. 2005, 19, 5A–36A. [Google Scholar] [CrossRef] [PubMed]
- Peppercorn, M.A.; Kane, S.V. Clinical Manifestations, Diagnosis, and Prognosis of Ulcerative Colitis in Adults. Available online: https://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-prognosis-of-ulcerative-colitis-in-adults?search=ulcerative%20colitis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 5 July 2022).
- Satsangi, J.; Silverberg, M.S.; Vermeire, S.; Colombel, J.F. The Montreal classification of inflammatory bowel disease: Controversies, consensus, and implications. Gut 2006, 55, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated Oral 5-Aminosalicylic Acid Therapy for Mildly to Moderately Active Ulcerative Colitis. N. Engl. J. Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef]
- Jauregui-Amezaga, A.; Geerits, A.; Das, Y.; Lemmens, B.; Sagaert, X.; Bessissow, T.; Lobatón, T.; Ferrante, M.; Van Assche, G.; Bisschops, R.; et al. A Simplified Geboes Score for Ulcerative Colitis. J. Crohn’s Colitis 2017, 11, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Sedano, R.; Almradi, A.; Casteele, N.V.; Parker, C.E.; Guizzetti, L.; Schaeffer, D.F.; Riddell, R.H.; Pai, R.K.; Battat, R.; et al. An International Consensus to Standardize Integration of Histopathology in Ulcerative Colitis Clinical Trials. Gastroenterology 2021, 160, 2291–2302. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, S.; Carreras, J.; Kikuti, Y.Y.; Nakae, H.; Dekiden-Monma, M.; Imai, J.; Tsuruya, K.; Nakamura, J.; Tsukune, Y.; Uchida, T.; et al. Prediction of steroid demand in the treatment of patients with ulcerative colitis by immunohistochemical analysis of the mucosal microenvironment and immune checkpoint: Role of macrophages and regulatory markers in disease severity. Pathol. Int. 2019, 69, 260–271. [Google Scholar] [CrossRef]
- Planell, N.; Lozano, J.J.; Mora-Buch, R.; Masamunt, M.C.; Jimeno, M.; Ordás, I.; Esteller, M.; Ricart, E.; Piqué, J.M.; Panés, J.; et al. Transcriptional analysis of the intestinal mucosa of patients with ulcerative colitis in remission reveals lasting epithelial cell alterations. Gut 2013, 62, 967–976. [Google Scholar] [CrossRef]
- Carreras, J.; Hamoudi, R.; Nakamura, N. Artificial Intelligence Analysis of Gene Expression Data Predicted the Prognosis of Patients with Diffuse Large B-Cell Lymphoma. Tokai J. Exp. Clin. Med. 2020, 45, 37–48. [Google Scholar]
- Carreras, J.; Kikuti, Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Nakamura, N.; Hamoudi, R. A Combination of Multilayer Perceptron, Radial Basis Function Artificial Neural Networks and Machine Learning Image Segmentation for the Dimension Reduction and the Prognosis Assessment of Diffuse Large B-Cell Lymphoma. AI 2021, 2, 106–134. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Shiraiwa, S.; Hamoudi, R.; et al. A Single Gene Expression Set Derived from Artificial Intelligence Predicted the Prognosis of Several Lymphoma Subtypes; and High Immunohistochemical Expression of TNFAIP8 Associated with Poor Prognosis in Diffuse Large B-Cell Lymphoma. AI 2020, 1, 342–360. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.; Roncador, G.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Shiraiwa, S.; et al. High Expression of Caspase-8 Associated with Improved Survival in Diffuse Large B-Cell Lymphoma: Machine Learning and Artificial Neural Networks Analyses. BioMedInformatics 2021, 1, 18–46. [Google Scholar] [CrossRef]
- Carreras, J.; Hiraiwa, S.; Kikuti, Y.Y.; Miyaoka, M.; Tomita, S.; Ikoma, H.; Ito, A.; Kondo, Y.; Roncador, G.; Garcia, J.F.; et al. Artificial Neural Networks Predicted the Overall Survival and Molecular Subtypes of Diffuse Large B-Cell Lymphoma Using a Pancancer Immune-Oncology Panel. Cancers 2021, 13, 6384. [Google Scholar] [CrossRef] [PubMed]
- Carreras, J.; Nakamura, N.; Hamoudi, R. Artificial Intelligence Analysis of Gene Expression Predicted the Overall Survival of Mantle Cell Lymphoma and a Large Pan-Cancer Series. Healthcare 2022, 10, 155. [Google Scholar] [CrossRef] [PubMed]
- Carreras, J.; Kikuti, Y.; Miyaoka, M.; Roncador, G.; Garcia, J.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; et al. Integrative Statistics, Machine Learning and Artificial Intelligence Neural Network Analysis Correlated CSF1R with the Prognosis of Diffuse Large B-Cell Lymphoma. Hemato 2021, 2, 182–206. [Google Scholar] [CrossRef]
- Carreras, J.; Hamoudi, R. Artificial Neural Network Analysis of Gene Expression Data Predicted Non-Hodgkin Lymphoma Subtypes with High Accuracy. Mach. Learn. Knowl. Extr. 2021, 3, 720–739. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Nakamura, N.; Hamoudi, R. Artificial Intelligence Analysis of the Gene Expression of Follicular Lymphoma Predicted the Overall Survival and Correlated with the Immune Microenvironment Response Signatures. Mach. Learn. Knowl. Extr. 2020, 2, 647–671. [Google Scholar] [CrossRef]
- Carreras, J.; Kikuti, Y.Y.; Miyaoka, M.; Hiraiwa, S.; Tomita, S.; Ikoma, H.; Kondo, Y.; Ito, A.; Hamoudi, R.; Nakamura, N. The Use of the Random Number Generator and Artificial Intelligence Analysis for Dimensionality Reduction of Follicular Lymphoma Transcriptomic Data. BioMedInformatics 2022, 2, 268–280. [Google Scholar] [CrossRef]
- Machine Learning. IBM Cloud Education. IBM Cloud Learn Hub. IBM Corporation. Available online: https://www.ibm.com/cloud/learn/machine-learning (accessed on 15 July 2020).
- IBM. IBM SPSS Neural Networks 26; IBM: Armonk, NY, USA, 2019. [Google Scholar]
- IBM. IBM SPSS Neural Networks; New Tools for Building Predictive Models; YTD03119-GBEN-01; IBM: Somers, NY, USA, 2012. [Google Scholar]
- Matson, J.; Ramamoorthy, S.; Lopez, N. The Role of Biomarkers in Surgery for Ulcerative Colitis: A Review. J. Clin. Med. 2021, 10, 3362. [Google Scholar] [CrossRef]
- Pantic, I.; Jevtic, D.; Nordstrom, C.W.; Madrid, C.; Milovanovic, T.; Dumic, I. Clinical Manifestations of Leukocytoclastic Vasculitis, Treatment, and Outcome in Patients with Ulcerative Colitis: A Systematic Review of the Literature. J. Clin. Med. 2022, 11, 739. [Google Scholar] [CrossRef]
- Okahara, K.; Ishikawa, D.; Nomura, K.; Ito, S.; Haga, K.; Takahashi, M.; Shibuya, T.; Osada, T.; Nagahara, A. Matching between Donors and Ulcerative Colitis Patients Is Important for Long-Term Maintenance after Fecal Microbiota Transplantation. J. Clin. Med. 2020, 9, 1650. [Google Scholar] [CrossRef]
- Haga, K.; Shibuya, T.; Nomura, K.; Okahara, K.; Nomura, O.; Ishikawa, D.; Sakamoto, N.; Osada, T.; Nagahara, A. Effectiveness and Nephrotoxicity of Long-Term Tacrolimus Administration in Patients with Ulcerative Colitis. J. Clin. Med. 2020, 9, 1771. [Google Scholar] [CrossRef] [PubMed]
- Nomura, K.; Ishikawa, D.; Okahara, K.; Ito, S.; Haga, K.; Takahashi, M.; Arakawa, A.; Shibuya, T.; Osada, T.; Kuwahara-Arai, K.; et al. Bacteroidetes Species Are Correlated with Disease Activity in Ulcerative Colitis. J. Clin. Med. 2021, 10, 1749. [Google Scholar] [CrossRef] [PubMed]
- Yeshi, K.; Ruscher, R.; Hunter, L.; Daly, N.L.; Loukas, A.; Wangchuk, P. Revisiting Inflammatory Bowel Disease: Pathology, Treatments, Challenges and Emerging Therapeutics Including Drug Leads from Natural Products. J. Clin. Med. 2020, 9, 1273. [Google Scholar] [CrossRef]
- Kobayashi, T.; Siegmund, B.; Le Berre, C.; Wei, S.C.; Ferrante, M.; Shen, B.; Bernstein, C.N.; Danese, S.; Peyrin-Biroulet, L.; Hibi, T. Ulcerative colitis. Nat. Rev. Dis. Prim. 2020, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Gajendran, M.; Loganathan, P.; Jimenez, G.; Catinella, A.P.; Ng, N.; Umapathy, C.; Ziade, N.; Hashash, J.G. A comprehensive review and update on ulcerative colitis. Dis. Mon. 2019, 65, 100851. [Google Scholar] [CrossRef]
- Feuerstein, J.D.; Moss, A.C.; Farraye, F.A. Ulcerative Colitis. Mayo Clin. Proc. 2019, 94, 1357–1373. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Carreras, J.; Shimizu, T.; Kakizaki, M.; Kikuti, Y.Y.; Roncador, G.; Nakamura, N.; Kotani, A. Anti-HBV drug entecavir ameliorates DSS-induced colitis through PD-L1 induction. Pharmacol. Res. 2022, 179, 105918. [Google Scholar] [CrossRef]
- Asano, K.; Matsumoto, T.; Umeno, J.; Hirano, A.; Esaki, M.; Hosono, N.; Matsui, T.; Kiyohara, Y.; Nakamura, Y.; Kubo, M.; et al. Impact of Allele Copy Number of Polymorphisms in FCGR3A and FCGR3B Genes on Susceptibility to Ulcerative Colitis. Inflamm. Bowel Dis. 2013, 19, 2061–2068. [Google Scholar] [CrossRef]
- Söderman, J.; Berglind, L.; Almer, S. Gene Expression-Genotype Analysis Implicates GSDMA, GSDMB, and LRRC3C as Contributors to Inflammatory Bowel Disease Susceptibility. BioMed Res. Int. 2015, 2015, 834805. [Google Scholar] [CrossRef]
- Gonsky, R.; Deem, R.L.; Landers, C.J.; Derkowski, C.A.; Berel, D.; McGovern, D.P.; Targan, S.R. Distinct IFNG methylation in a subset of ulcerative colitis patients based on reactivity to microbial antigens. Inflamm. Bowel Dis. 2011, 17, 171–178. [Google Scholar] [CrossRef]
- Pandey, S.P.; Yan, J.; Turner, J.R.; Abraham, C. Reducing IRF5 expression attenuates colitis in mice, but impairs the clearance of intestinal pathogens. Mucosal Immunol. 2019, 12, 874–887. [Google Scholar] [CrossRef] [PubMed]
- Iwańczak, B.; Ruczka, M.; Matusiewicz, M.; Pytrus, T.; Matusiewicz, K.; Krzesiek, E. Correlation between biomarkers (calprotectin, seromucoid, metalloproteinase-3 and CRP) and clinical and endoscopic activity of ulcerative colitis in children. Adv. Med Sci. 2020, 65, 259–264. [Google Scholar] [CrossRef] [PubMed]







| Model | Overall Accuracy (%) | No. Fields (Genes) Used | Most Relevant Genes |
|---|---|---|---|
| C5 | 100 | 2 | GART, IL21R |
| Logistic regression | 100 | 734 | AAMP, ABHD6, ACKR2, ACOXL, ACSL6, ADA, ADAM30, ADCY3, ADCY7, AFF3, AGAP2, AHI1, AHR, AIRE, ANKRD55, ANTXR2, APEH, APOBEC3G, ARG1, ARHGAP30, ARID5B, ARPC2, ATF4, ATG16L1, ATG5, ATM, B2M, B3GNT2, BABAM2, BACH2, BAD, BANK1, BATF, BATF3, BCL10, BCL3, BCL6, BID, BLK, BLNK, BORCS5, and BSN. |
| Discriminant | 100 | 734 | - |
| LSVM | 100 | 734 | CCL11, IL1RN, MMP3, CXCL3, FCGR3A, TLR3, NFIL3, TTYH3, NLRP2, and OSMR |
| SVM | 100 | 734 | - |
| XGBoost Linear | 100 | 734 | - |
| XGBoost Tree | 100 | 734 | - |
| Neural Network | 100 | 734 | BSN, TBX21, ITGAE, TMBIM1, IRF5, IL12B, IL18R1, PLEKHG5, COG6, and RBM17 |
| CHAID | 97.7 | 2 | IP6K1, ZFP90 |
| Random Forest | 97.7 | 734 | PDLIM4, SLC22A5, SCAMP3, VDR, MAPKAPK2, SLC15A4, KLF4, IRAK2, NFIL3, and CXCL11 |
| KNN Algorithm | 95.4 | 734 | - |
| C&R Tree | 95.4 | 12 | METTL1, ADA |
| Quest | 83.7 | 6 | IRAK1 |
| Bayesian Network | 65.1 | 734 | - |
| Random Trees | 0 | 734 | N/A |
| Model | Overall Accuracy (%) | No. Fields (Genes) Used | Most Relevant Genes |
|---|---|---|---|
| Logistic regression | 100 | 734 | - |
| Discriminant | 100 | 734 | - |
| SVM | 100 | 734 | - |
| XGBoost Linear | 100 | 734 | - |
| XGBoost Tree | 100 | 734 | - |
| CHAID | 97.7 | 4 | MMP3, OSMR, ZFP90, and GSDMB |
| Random Forest | 97.7 | 734 | TLR2, IFNAR2, BID, NCF2, IDO1, FCGR1A, CSF2RB, TGFBI, S1PR1, and IRAK1 |
| Neural Network | 97.7 | 734 | UBASH3A, IL22, TBX21, IL12B, TIGIT, CD19, TRAF1, IFNG, CARD14, and IRF5 |
| Bayesian Network | 95.4 | 734 | - |
| KNN Algorithm | 93.0 | 734 | - |
| LSVM | 86.1 | 734 | - |
| C5 | 83.7 | 2 | CD274 and SULT1A1 |
| C&R Tree | 65.1 | 6 | CD274 |
| Quest | 62.8 | 6 | FCGR3A |
| Random Trees | 0 | 734 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carreras, J. Artificial Intelligence Analysis of Ulcerative Colitis Using an Autoimmune Discovery Transcriptomic Panel. Healthcare 2022, 10, 1476. https://doi.org/10.3390/healthcare10081476
Carreras J. Artificial Intelligence Analysis of Ulcerative Colitis Using an Autoimmune Discovery Transcriptomic Panel. Healthcare. 2022; 10(8):1476. https://doi.org/10.3390/healthcare10081476
Chicago/Turabian StyleCarreras, Joaquim. 2022. "Artificial Intelligence Analysis of Ulcerative Colitis Using an Autoimmune Discovery Transcriptomic Panel" Healthcare 10, no. 8: 1476. https://doi.org/10.3390/healthcare10081476