
What Aspects of Religion and Spirituality Affect the Physical Health of Cancer Patients? A Systematic Review

 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Articles published between 2015 and March 2022.
- Articles in English and Spanish.
- Cancer population and survivors. Articles whose sample consisted of persons with cancer at the time of the study or cancer survivors were examined.
- Individuals 18 years of age or older.
- Empirical studies.
- Studies that included measures of self-perceived or biomarker-derived physical health. Following Jim et al. [39], physical well-being, functional well-being, and self-assessed physical symptoms were utilized as measures of physical health. In addition, the presence/absence of biomarkers that provide an objective measure of the health status of individuals was added as a measure of physical health.
- 7.
- Population related to cancer but who were not patients or survivors: caregivers, family members, nurses.
- 8.
- Individuals under 18 years of age.
- 9.
- Review studies, theoretical articles, and case studies.
- 10.
- Studies whose only measure of R/S was religious and/or spiritual interventions. These types of studies were excluded as they did not apply to our objectives, since we were attempting to identify specific R/S variables that have an impact on physical health.
- 11.
- Studies that included only mental health measures.
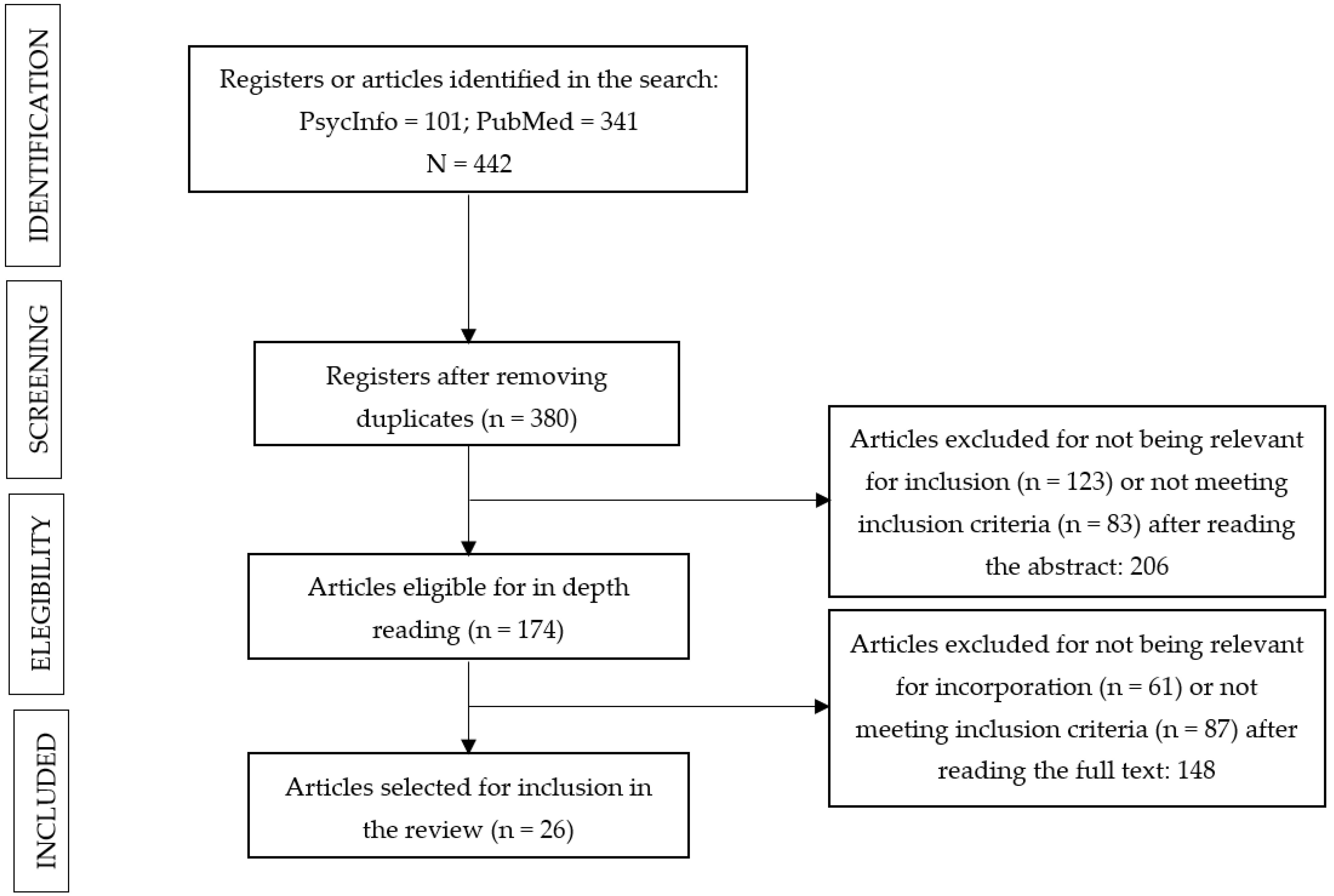
2.3. Selection Process
2.4. Evaluation of the Methological Quality of the Articles
- Excellent: 16.
- Very good: 14 to 15.
- Good: 12 to 13.
- Acceptable: 10 to 11.
- Poor: 9 or less.
2.5. Extracted Data
- Title, authors, year of publication and journal.
- Country in which the study was conducted.
- Study sample: number of participants, type and stage of cancer, and whether patient or survivor.
- Objective, research design and instruments used.
- Key variables: measures of R/S and physical health.
- Main results or findings of each investigation.
3. Results
3.1. Selected Articles
3.2. Quality Evaluation
3.3. R/S Variables, Health Variables and Main Results
3.3.1. R/S Variables
3.3.2. Physical Health Variables
3.3.3. Main Research Results
4. Discussion
Limitations and Future Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Author (Year) | Objectives | Sample | Measures | Design | Results |
|---|---|---|---|---|---|
| Al Ahwal et al., 2018 | (1) To explore the relationship between telomere length and religious participation; (2) To examine the demographic, social, psychological, and cancer-related correlates and mediators of the relationship | n = 50; 41–64 years; 52% female. Saudi Arabia | Sociodemographic data; 13-item Muslim Religiosity Scale; 11-item version of the Duke Social Support Index; 17-item Hamilton Depression Rating Scale; DSM-IV criteria checklist of mental disorders; Personal and family psychiatric history; Depression history; Family history of mental and nervous disease; Blood test telomeres | Cross-sectional | Positive association between religiosity and telomere length, weak and not significant. Neither religious beliefs nor religious practices were significantly associated with telomere length |
| Al-Natour et al., 2017 | (1) To investigate the relationship between spirituality and dimensions of quality of life for Jordanian women diagnosed with breast cancer, including physical, social, emotional and functional well-being | n = 150; 25–69 years; 100% female. Jordan. | Sociodemographic data; Arabic version of FACIT-Sp | Cross-sectional | Positive and significant association between spiritual well-being and physical and functional well-being |
| Asgeirsdottir et al., 2017 | (1) To examine the feasibility of the Icelandic version of the provisional EORTC SWB measure; (2) To explore the relationship between spiritual well-being and quality of life of palliative care patients in Iceland | n = 30; 51–83 years; 73.3% female. Iceland. | Provisional EORTC QLQ-SWB; EORTC QLQ-15-PAL | Cross-sectional | Global health/quality of life status correlated moderately and positively with total spiritual well-being. Physical functioning and physical symptom scale did not correlate with spiritual well-being |
| Bai et al., 2016 | (1) To examine individual patterns of spiritual well-being in newly diagnosed patients with advanced cancer using cluster analysis | n = 52; 21 years or older; 46.2% female. USA. | FACIT-Sp12; FACT-G; PHQ-9; Self-rated health item; Self-rated spirituality item | Cross-sectional | There were significant differences in functional well-being as a function of meaning, peace and faith, but no such differences were observed for physical well-being. The cluster with the highest meaning, peace and faith, had the highest level of functional well-being |
| Best et al., 2015 | (1) To examine the extent to which spirituality is associated with self-rated health among African American cancer survivors compared to other racial/ethnic groups; (2) To examine the extent to which cancer-related problems mediate the relationship between spirituality and self-rated health | n = 9006; 23–100 years; 55% female. USA. | Sociodemographic and health data; Self-rated health item; Cancer Problems in Living Scale; FACIT-Sp12 | Cross-sectional | Meaning was negatively and significantly associated with physical symptoms in both groups. There were significant negative associations between peace and physical symptoms in both groups, although these associations were stronger in African Americans. Faith was positively and significantly associated in both groups |
| Brown et al., 2015 | (1) To assess whether an individual’s level of meaning/peace predicts various measures of quality of life and mental well-being; (2) To identify goals that can improve the overall spiritual well-being and quality of life of ovarian cancer patients | n = 104; 33–83 years; 100% female. USA. | Sociodemographic data; FACIT-Sp12; FACT-O; HHI; ESAS; Death Anxiety Scale; HADS; Coping dimension of the BMMRS | Cross-sectional | Greater meaning/peace predicted higher levels of physical and functional well-being and fewer sleep problems. No correlations were found between meaning/peace and symptoms more physical in nature (pain, fatigue, etc.) |
| Canada et al., 2016 | (1) To clarify the relationship between dimensions of spiritual well-being and quality of life in cancer survivors | n = 8405; 23–100 years; 55.1% female. USA. | Sociodemographic data; FACIT-Sp12; Physical component of the SF-36; Mental component of the SF-36 | Cross-sectional | Meaning, peace and faith were associated with the physical component of the SF-36 (functional quality of life) |
| Cannon et al., 2022 | (1) To explore the relationship of spirituality and religiosity as it relates to the physical and mental quality of life of cancer survivors | n = 551; 19–85 years; 36.5% female. USA. | Sociodemographic data; FACIT-Sp; Two items on religiosity (beliefs and practices); Short-Form-12 Health Survey | Longitudinal | No significant interaction was observed between religiosity, spirituality and quality of life over time. Physical well-being of cancer survivors with low spirituality and religiosity was significantly lower that those with high religiosity and spirituality. The effect of spirituality on physical quality of life was only significant among highly religious participants |
| Chaar et al., 2018 | (1) To assess the impact of spirituality on quality of life, depression and anxiety in Lebanese cancer patients | n = 115; 18 years or older; 67% female. Lebanon. | Sociodemographic and clinical data; Arabic version of EORTC-QLQ-C30; Arabic version of FACIT-Sp12; Arabic version of HADS | Cross-sectional | Meaning was uniquely associated with dyspnea, in a negative and significative manner. Peace was negatively and significantly associated with fatigue, pain, dyspnea and loss of appetite. Faith was negatively and significantly associated with dyspnea and loss of appetite. All dimensions and total spiritual well-being were positively associated with overall health and quality of life status and role functioning |
| Chen et al., 2021 | (1) Investigated spiritual well-being and its association with quality of life, anxiety and depression in patients with gynecological cancer | n = 705; 18 years or older; 100% female. China. | EORTC QLQ-SWB32; EORTC QLQ-C30; HADS | Cross-sectional | Total spiritual well-being and the existential, relationship with self, and relationship with others correlated significantly and positively with physical functioning and negatively with most physical symptoms. The relationship with something superior dimension correlated only positively and significantly with loss of appetite |
| Cheng et al., 2019 | (1) To explore factors associated with spiritual well-being among cancer patients and the relationship between spiritual well-being and quality of life | n = 185; 18 years or older; 53% female. China. | Sociodemographic and clinical data; FACT-G; FACIT-Sp12 | Cross-sectional | All dimensions were significantly and positively related to functional well-being. In addition, peace was positively associated with physical well-being, while faith was negatively associated with physical well-being. Peace and faith had a predictive power on physical well-being, and these together with meaning predicted an important part of functional well-being |
| Damen et al., 2021 | (1) To examine the prevalence, predictors and correlates of R/S struggles in the palliative care cancer population | n = 331; 55–93 years; 56% female. USA. | Sociodemographic data; RRS-14; Three items on religious characteristic; ESAS; PDI; QUAL-E | Cross-sectional | Higher symptom burden was significantly and positively associated with higher R/S struggles. Higher scores in all subdomains of R/S struggles were associated with higher symptom burden, except for interpersonal struggle |
| Gielen et al., 2017 | (1) To examine the prevalence and nature of spiritual distress in Indian palliative care patients | n = 300; doesn’t specify age range; 49.3% female. India. | Sociodemographic data; Newly developed questionnaire for the study of spirituality in Indian palliative care patients; Item to assess pain | Cross-sectional | Statistic significant differences in pain scores were observed between the different clusters. Spiritually distressed patients suffered more severe pain, while patients who trust in God suffered less |
| Goyal et al., 2019 | (1) To examine the reciprocal relationship between spirituality and physical health status in breast cancer survivors | n = 634; 18 years or older; 100% female. USA. | Sociodemographic and cancer-related data; FACIT-Sp12; Physical component of the SF-36 | Longitudinal | Meaning and peace correlated significantly with the physical component both cross-sectionally and longitudinally. The correlations between faith and the physical component were very low and not significant |
| Hulett et al., 2018 | (1) To determine the feasibility and acceptability of a salivary cortisol self-collection protocol; (2) To examine the relationships between R/S, health perceptions and daytime salivary cortisol | n = 41; 51–88 years; 100% female. USA. | Sociodemographic data; BMMRS; SF-36v2; Cortisol | Cross-sectional | Positive spiritual experiences were the only spiritual variable that demonstrated a statistically significant relationship with peak cortisol. In general, poorer physical health was inversely associated with positive spiritual experiences and private religious practices. Specifically, positive religious experiences, spiritual coping and private religious practices were inversely and significantly correlated with physical function and bodily pain. Negative congregational support was significantly and negatively associated with physical function. Forgiveness, positive congregational support, and negative spiritual experiences were not significantly associated with physical health |
| Kamijo y Miyamura 2020 | (1) To examine patients’ level of spirituality, the relationship between spirituality and physical pain, and the association between spirituality and quality of life among patients undergoing chemotherapy for cancer | n = 176; 22–88 years; 75% female. Japan. | Sociodemographic and clinical data; OPTIM Screening Sheet; VAS; FACIT-Sp12; FACT-G | Cross-sectional | Total spiritual well-being and all its dimensions correlated significantly with physical and functional well-being. In addition, faith and meaning/peace correlated significantly with loss of appetite, and the latter dimension also correlated significantly with insomnia. |
| King et al., 2017 | (1) To describe the prevalence, demographic and medical correlates, and emotional and quality of life correlates of R/S struggles in HCT survivors | n = 1449; 18–89 years; 49% female. USA. | Sociodemographic and medical data; Brief RCOPE negative coping subscale; General health and pain subscales of the SF-36; Existential and social support subscales of the McGill Quality of Life Questionnaire; PHQ-8; Question about whether they have graft-versus-host disease | Cross-sectional | R/S struggles were not significantly associated with graft-versus-host disease or with pain or general health |
| King et al., 2018 | (1) To study the relationship between R/S struggle and existential quality of life; (2) To examine the demographic, medical, emotional and social correlates of quality (of life?) in young people | n = 172; 18–39 years; 55.8% female. USA. | This article presents the same measures as the previous one (see King et al., 2017) | Cross-sectional | R/S struggles were not significantly associated with graft-versus-host disease or with pain or general health |
| Leeson et al., 2015 | (1) To investigate changes in spirituality among HCT recipients over time; (2) To assess the extent to which spirituality before HCT predicted important dimensions of quality of life after transplantation | n = 220; 19–74 years; 38.2% female. USA. | FACIT-Sp12; IDAS; FSI; BPI; Physical and functional well-being dimensions of the FACIT | Longitudinal | Meaning/peace significantly predicted less fatigue and pain, as well as greater physical and functional well-being during the 12 months after transplantation. Faith was associated only with increased fatigue. Meaning/peace before HCT predicted changes in fatigue and physical well-being over time. |
| Mendoça et al., 2020 | (1) To analyze the relationships between the subjective experience of distress and the use of R/S coping in adult patients receiving chemotherapy | n = 100; 18 years or older; 47% female. Brazil. | Sociodemographic data; ISDEI; ECOG Scale; VAS; RSC-Brief | Cross-sectional | Negative coping correlated weakly, significantly and positively with physical distress |
| Narayanan et al., 2020 | (1) To identify the frequencies of spontaneously written religious content in participants’ emotional writing samples and the extent to which the religious content of their writing was associated with a validated self-report R/S scale and cancer-related psychosocial symptoms and outcomes | n = 138; 18 years or older; 40% female. USA. | Sociodemographic data; Religious content of the writings; Ironson-Woods Spirituality/Religious Index; BSI; BFI; PSQI; MOS-SSS | Longitudinal | Private religious engagement was negatively associated with fatigue. Negative religious coping was positively and significantly associated with sleep problems. Private religious engagement was significantly and negatively associated with cancer-related symptoms throughout the follow-up period, whereas no other R/S variable was associated with symptoms in that period |
| Pérez-Cruz et al., 2019 | (1) To characterize the association between spiritual pain and quality of life in a group of advanced cancer patients in a palliative care clinic | n = 208; 18 years or older; 50% female. Chile. | Sociodemographic data; MDAS; ESAS; ESAS-F; HADS; EORTC-QLQ-C15-PAL; Self-rated spirituality and religiosity items | Cross-sectional | Spiritual pain was associated with poorer overall quality of life and poorer physical quality of life. It was also associated with fatigue, drowsiness, anorexia, dyspnea, sleep problems and general physical symptom burden |
| Rohde et al., 2019 | (1) To report on an additional multivariate analysis, to investigate the relationships between sex, age and spiritual well-being of patients receiving palliative care | n = 451; 18–89 years; 54% female. International. | QLQ-SWB32; QLQ-C14-PAL | Cross-sectional | Spiritual well-being correlated significantly and positively with overall quality of life. No correlation was observed between spiritual well-being and physical functioning. A significative negative relationship of spiritual well-being with insomnia, fatigue and constipation was observed. All dimensions, with the exception of relationship with others, were associated with physical functioning and with one or more physical symptoms |
| Sleight et al., 2021 | (1) To assess the extent to which spiritual well-being moderates the relationship between anxiety and physical well-being in a diverse, community-based cohort of newly diagnosed cancer survivors | n = 5506; 21–84 years; 60% female. USA. | Meaning/peace subscale of the FACIT-Sp12; PROMIS Anxiety short form; FACT-G | Cross-sectional | A positive direct effect of meaning/peace on physical well-being was observed. A significant interaction was found between meaning/peace and anxiety, indicating that spiritual well-being moderated the relationship between anxiety and physical well-being. |
| Walker et al., 2017 | (1) To investigate the relationship between psychological state and traits in self-reported religious beliefs | n = 43; 52–79 years; 100% male. USA. | FACT-P; FACIT-Sp-Ex; PHQ-9; NEO Five-Factor Inventory | Cross-sectional | Meaning/peace correlated significantly and positively with physical well-being, functional well-being, and well-being related to prostate health. Faith was significantly associated with functional well-being, but not with physical well-being |
| Yilmaz y Cengiz 2020 | (1) To assess the relationship between spiritual well-being and quality of life in cancer survivors | n = 150; 20–65 years; 61.3% female. Turkey. | Sociodemographic data; FACIT-Sp12; FACT-G | Cross-sectional | Significant positive correlations were found between total spiritual well-being and its dimensions with physical and functional well-being, with the exception of faith, which was only associated with functional well-being |
References
- Koenig, H.G.; King, D.E.; Carson, V.B. Handbook of Religion and Health, 2nd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Schnell, T. Spirituality with and without religion—Differential relationships with personality. Arch. Psychol. Relig. 2012, 34, 33–61. [Google Scholar] [CrossRef] [Green Version]
- Moreira-Almeida, A.; Sharma, A.; van Rensburg, B.J.; Verhagen, P.J.; Cook, C.C.H. WPA Position Statement on Spirituality and Religion in Psychiatry. World Psychiatry 2016, 15, 87–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenig, H.G. Research on religion, spirituality, and mental health: A review. Can. J. Psychiatry 2009, 54, 283–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, S.R.; Pargament, K.I. The role of religion and spirituality in mental health. Curr. Opin. Psychiatry 2014, 27, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Holt, C.L.; Roth, D.L.; Huang, J.; Clark, E.M. Role of Religious Social Support in Longitudinal Relationships between Religiosity and Health-Related Outcomes in African Americans. J. Behav. Med. 2018, 41, 62–73. [Google Scholar] [CrossRef]
- Vitorino, L.M.; Lucchetti, G.; Leão, F.C.; Vallada, H.; Peres, M.F.P. The association between spirituality and religiousness and mental health. Sci. Rep. 2018, 8, 17233. [Google Scholar] [CrossRef] [Green Version]
- Saiz, J.; Chen-Chen, X.; Mills, P.J. Religiosity and Spirituality in the Stages of Recovery from Persistent Mental Disorders. J. Nerv. Ment. Dis. 2021, 209, 106–113. [Google Scholar] [CrossRef]
- Reynolds, N.; Mrug, S.; Wolfe, K.; Schwebel, D.; Wallander, J. Spiritual coping, psychosocial adjustment, and physical health in youth with chronic illness: A meta-analytic review. Health Psychol. Rev. 2016, 10, 226–243. [Google Scholar] [CrossRef]
- Shattuck, E.C.; Muehlenbein, M.P. Religiosity/Spirituality and Physiological Markers of Health. J. Relig. Health 2020, 59, 1035–1054. [Google Scholar] [CrossRef]
- Sherman, A.C.; Merluzzi, T.V.; Pustejovsky, J.E.; Park, C.L.; George, L.; Fitchett, G.; Jim, H.S.L.; Munoz, A.R.; Danhauer, S.; Snyder, M.A.; et al. A meta-analytic review of religious or spiritual involvement and social health among cancer patients. Cancer 2015, 121, 3779–3788. [Google Scholar] [CrossRef]
- Chen, Y.; Kim, E.S.; VanderWeele, J. Religious-service attendance and subsequent health and well-being throughout adulthood: Evidence from three prospective cohorts. Int. J. Epidemiol. 2020, 49, 2030–2040. [Google Scholar] [CrossRef] [PubMed]
- Parenteau, S.C.; Hurd, K.; Wu, H.; Feck, C. Attachment to God and Psychological Adjustment: God’s Responses and Our Coping Strategies. J. Relig. Health 2019, 58, 1286–1306. [Google Scholar] [CrossRef] [PubMed]
- Pirutinsky, S.; Cherniak, A.D.; Rosmarin, D.H. COVID-19, Mental Health, and Religious Coping among American Orthodox Jews. J. Relig. Health 2020, 59, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Garduño-Ortega, O.; Morales-Cruz, J.; Hunter-Hernández, M.; Gany, F.; Costas-Muñiz, R. Spiritual Well-Being, Depression, and Quality of Life among Latina Breast Cancer Survivors. J. Relig. Health 2021, 60, 1895–1907. [Google Scholar] [CrossRef]
- Hill, P.C.; Pargament, K.I. Advances in the conceptualization and measurement of religion and spirituality. Implications for physical and mental health research. Am. Psychol. 2003, 58, 64–74. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.; Macdonald, J.; MacLeod, R. Measuring Spirituality and Religiosity in Clinical Settings: A Scoping Review of Available Instruments. Religions 2018, 9, 70. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Punnoose, V.P.; Doval, N.; Nair, V.Y. Spirituality, religiousness and coping in patients with schizophrenia: A cross sectional study in a tertiary care hospital. Psychiatry Res. 2018, 256, 238–243. [Google Scholar] [CrossRef]
- Piccinini, C.R.P.; de Castro Almeida, V.; da Silva Ezequiel, O.; de Matos Fajardo, E.F.; Lucchetti, A.; Lucchetti, G. Religiosity/Spirituality and Mental Health and Quality of Life of Early Pregnant Women. J. Relig. Health 2021, 60, 1908–1923. [Google Scholar] [CrossRef]
- Esan, O.; Lawal, K. Spirituality and Suicidality among Cancer with Schizophrenia: A Cross-Sectional Study from Nigeria. J. Relig. Health 2021, 60, 2547–2559. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, Z. Cross-Sectional Studies: Strengths, Weaknesses, and Recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef] [PubMed]
- Dilmaghani, M. Importance of Religion or Spirituality and Mental Health in Canada. J. Relig. Health 2018, 57, 120–135. [Google Scholar] [CrossRef]
- Braam, A.W.; Koenig, H.G. Religion, spirituality and depression in prospective studies: A systematic review. J. Affect. Disord. 2019, 257, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L.; Lee, S.Y. Unique effects of religiousness/spirituality and social support on mental and physical well-being in people living with congestive heart failure. J. Behav. Med. 2020, 43, 630–637. [Google Scholar] [CrossRef]
- Koenig, H.G. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012, 2012, 278730. [Google Scholar] [CrossRef] [Green Version]
- Mendes, N.S.; Malaguti, C.; Dos Anjos Sena, L.; Lucchetti, G.; De Jesús, L.; Vitorino, L.M.; Mesquita, R.; Lee, A.L.; Oliveira, C.C. Spirituality and religiosity are associated with physical and psychological status in patients with chronic obstructive pulmonary disease. J. Clin. Nurs. 2022, 31, 669–678. [Google Scholar] [CrossRef]
- Moons, P.; Luyckx, K.; Dezutter, J.; Kovacs, A.H.; Thomet, C.; Budts, W.; Enomoto, J.; Sluman, M.A.; Yang, H.-L.; Jackson, J.L.; et al. Religion and spirituality as predictors of patient-reported outcomes in adults with congenital heart disease around the globe. Int. J. Cardiol. 2019, 274, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Hsieh, C.; Shih, Y.; Lin, Y. Spiritual well-being of patients with chronic renal failure: A cross-sectional study. Nurs. Open 2021, 8, 2461–2469. [Google Scholar] [CrossRef]
- Li, S.; Stampfer, M.J.; Williams, D.R.; WanderWeele, T.J. Association of Religious Service Attendance with Mortality among Women. JAMA Intern. Med. 2016, 176, 777–785. [Google Scholar] [CrossRef]
- Moreira, W.C.; Nóbrega, M.; Lima, F.P.S.; Lago, E.P.; Lima, M.O. Effects of the association between spirituality, religiosity and physical activity on health/mental health: A systematic review. Rev. Esc. Enferm. USP 2020, 54, e03631. [Google Scholar] [CrossRef] [PubMed]
- Balboni, T.A.; VanderWeele, T.J.; Doan-Soares, S.D.; Long, K.N.G.; Ferrell, B.R.; Fitchett, G.; Koenig, H.G.; Bain, P.A.; Puchalski, C.; Steinhauser, K.E.; et al. Spirituality in Serious Illness and Health. JAMA 2022, 328, 184–197. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.W. Religion, Health, and the Psychology of Religion: How the Research on Religion and Health Helps Us Understand Religion. J. Relig. Health 2004, 43, 317–328. [Google Scholar] [CrossRef]
- Aloush, V.; Gurevich-Shapiro, A.; Hazan, E.; Furer, V.; Elkayam, O.; Ablin, J.N. Relationship between religiosity, spirituality and physical health and mental outcomes in fibromyalgia patients. Clin. Exp. Rheumatol. 2021, 39, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L.; Sacco, S.J.; Kraus, S.W.; Mazure, C.M.; Hoff, R.A. Influences of religiousness/spirituality on mental and physical health in OEF/OIF/OND military veterans varies by sex and race/ethnicity. J. Psychiatr. Res. 2021, 138, 15–23. [Google Scholar] [CrossRef]
- Spanish Society of Medical Oncology. Cancer Figures in Spain. 2022. Available online: https://seom.org/prensa/el-cancer-en-cifras (accessed on 20 February 2022).
- Koenig, H.G. Concerns about measuring “spirituality” in research. J. Nerv. Ment. Dis. 2008, 196, 349–355. [Google Scholar] [CrossRef]
- Głaz, S. Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG). J. Relig. Health 2021, 60, 3545–3561. [Google Scholar] [CrossRef]
- Jim, H.S.L.; Pustejovsky, J.E.; Park, C.L.; Danhauer, S.C.; Sherman, A.C.; Fitchett, G.; Merluzzi, T.V.; Munoz, A.R.; George, L.; Snyder, M.A.; et al. Religion, Spirituality, and Physical Health in Cancer Patients: A Meta-Analysis. Cancer 2015, 121, 3760–3768. [Google Scholar] [CrossRef]
- Park, C.L.; Sherman, A.C.; Jim, H.S.L.; Salsman, J.M. Religion/Spirituality and Health in the Context of Cancer: Cross-Domain Integration, Unresolved Issues, and Future Directions: Religion/Spirituality and Health. Cancer 2015, 121, 3789–3794. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 statement: An updated guide for the publication of systematic reviews. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Stewart, D.; Letts, L.; Pollok, N.; Bosch, J.; Westmorland, M. Guidelines for Critical Review Form—Quantitative Studies. 1998. Available online: https://healthsci.mcmaster.ca/docs/librariesprovider130/default-document-library/guidelines-for-critical-review-form-quantiative-studies-english.pdf?sfvrsn=ee9f6c19_2 (accessed on 15 March 2022).
- Appelbaum, M.; Cooper, H.; Kline, R.B.; Mayo-Wilson, E.; Nezu, A.M.; Rao, S.M. Journal Article Reporting Standards for Quantitative Research in Psychology: The APA Publications and Communications Board Task Force Report. Am. Psychol. 2018, 73, 3–25. [Google Scholar] [CrossRef]
- Levitt, H.M.; Bamberg, M.; Creswell, J.W.; Frost, D.M.; Josselson, R.; Suárez-Orozco, C. Journal Article Reporting Standards for Qualitative Primary, Qualitative Meta-Analytic, and Mixed Methods Research in Psychology: The APA Publications and Communications Board Task Force Report. Am. Psychol. 2018, 73, 26–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannon, A.J.; Dokucu, M.E.; Loberiza, F.R. Interplay between Spirituality and Religiosity on the Physical and Mental Well-Being of Cancer Survivors. Support. Care Cancer 2022, 30, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Gielen, J.; Bhatnagar, S.; Chaturvedi, S.K. Prevalence and Nature of Spiritual Distress among Palliative Care Patients in India. J. Relig. Health 2017, 56, 530–544. [Google Scholar] [CrossRef]
- Al-Natour, A.; Al Momani, S.M.; Qandil, A.M.A. The Relationship between Spirituality and Quality of Life of Jordanian Women Diagnosed with Breast Cancer. J. Relig. Health 2017, 56, 2096–2108. [Google Scholar] [CrossRef]
- Bai, M.; Dixon, J.; Williams, A.; Jeon, S.; Lazenby, M.; McCorkle, R. Exploring the Individual Patterns of Spiritual Well-Being in People Newly Diagnosed with Advanced Cancer: A Cluster Analysis. Qual. Life Res. 2016, 25, 2765–2773. [Google Scholar] [CrossRef] [PubMed]
- Best, A.L.; Alcaraz, K.I.; McQueen, A.; Cooper, D.L.; Warren, R.C.; Stein, K. Examining the Mediating Role of Cancer-Related Problems on Spirituality and Self-Rated Health among African American Cancer Survivors: A Report from the American Cancer Society’s Studies of Cancer Survivors-II: Spirituality, Cancer-Related Problems, and Self-Rated Health. Psycho-Oncology 2015, 24, 1051–1059. [Google Scholar] [CrossRef]
- Brown, A.J.; Sun, C.C.; Urbauer, D.; Zhukovsky, D.S.; Levenback, C.; Frumovitz, M.; Thaker, P.H.; Bodurka, D.C.; Ramondetta, L.M. Targeting Those with Decreased Meaning and Peace: A Supportive Care Opportunity. Support. Care Cancer 2015, 23, 2025–2032. [Google Scholar] [CrossRef] [Green Version]
- Canada, A.L.; Murphy, P.E.; Fitchett, G.; Stein, K. Re-Examining the Contributions of Faith, Meaning, and Peace to Quality of Life: A Report from the American Cancer Society’s Studies of Cancer Survivors-II (SCS-II). Ann. Behav. Med. 2016, 50, 79–86. [Google Scholar] [CrossRef]
- Chaar, E.A.; Hallit, S.; Hajj, A.; Aaraj, R.; Kattan, J.; Jabbour, H.; Khabbaz, L.R. Evaluating the Impact of Spirituality on the Quality of Life, Anxiety, and Depression among Patients with Cancer: An Observational Transversal Study. Support. Care Cancer 2018, 26, 2581–2590. [Google Scholar] [CrossRef]
- Cheng, Q.; Liu, X.; Li, X.; Wang, Y.; Mao, T.; Chen, Y. Improving Spiritual Well-Being among Cancer Patients: Implications for Clinical Care. Support. Care Cancer 2019, 27, 3403–3409. [Google Scholar] [CrossRef]
- Goyal, N.G.; Ip, E.H.; Salsman, J.M.; Avis, N.E. Spirituality and Physical Health Status: A Longitudinal Examination of Reciprocal Effects in Breast Cancer Survivors. Support. Care Cancer 2019, 27, 2229–2235. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, Y.; Miyamura, T. Spirituality and Associated Factors among Cancer Patients Undergoing Chemotherapy. Jpn. J. Nurs. Sci. 2020, 17, e12276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leeson, L.A.; Nelson, A.M.; Rathouz, P.J.; Juckett, M.B.; Coe, C.L.; Caes, E.W.; Costanzo, E.S. Spirituality and the Recovery of Quality of Life following Hematopoietic Stem Cell Transplantation. Health Psychol. 2015, 34, 920–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sleight, A.G.; Boyd, P.; Klein, W.M.P.; Jensen, R.E. Spiritual Peace and Life Meaning May Buffer the Effect of Anxiety on Physical Well-Being in Newly Diagnosed Cancer Survivors. Psycho-Oncology 2021, 30, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.J.; Chen, Y.; Paik, K.; Mirly, B.; Thomas, C.R.; Hung, A.Y. The Relationships between Spiritual Well-Being, Quality of Life, and Psychological Factors before Radiotherapy for Prostate Cancer. J. Relig. Health 2017, 56, 1846–1855. [Google Scholar] [CrossRef]
- Yilmaz, M.; Cengiz, H.Ö. The Relationship between Spiritual Well-Being and Quality of Life in Cancer Survivors. Palliat. Support. Care 2020, 18, 55–62. [Google Scholar] [CrossRef]
- Chen, J.; You, H.; Liu, Y.; Kong, Q.; Lei, A.; Guo, X. Association between Spiritual Well-Being, Quality of Life, Anxiety and Depression in Patients with Gynaecological Cancer in China. Medicine 2021, 100, e24264. [Google Scholar] [CrossRef]
- Rohde, G.E.; Young, T.; Winstanley, J.; Arraras, J.I.; Black, K.; Boyle, F.; Bredart, A.; Costantini, A.; Guo, J.; Irarrazaval, M.E.; et al. Associations between Sex, Age and Spiritual Well-Being Scores on the EORTC QLQ-SWB32 for Patients Receiving Palliative Care for Cancer: A Further Analysis of Data from an International Validation Study. Eur. J. Cancer Care 2019, 28, e13145. [Google Scholar] [CrossRef]
- Asgeirsdottir, G.H.; Sigurdardottir, V.; Gunnarsdottir, S.; Sigurbjörnsson, E.; Traustadottir, R.; Kelly, E.; Young, T.; Vivat, B. Spiritual Well-Being and Quality of Life among Icelanders Receiving Palliative Care: Data from Icelandic Pilot-Testing of a Provisional Measure of Spiritual Well-Being from the European Organisation for Research and Treatment of Cancer. Eur. J. Cancer Care 2017, 26, e12394. [Google Scholar] [CrossRef]
- Damen, A.; Exline, J.; Pargament, K.I.; Yao, Y.; Chochinov, H.; Emanuel, L.; Handzo, G.; Wilkie, D.J.; Fitchett, G. Prevalence, Predictors and Correlates of Religious and Spiritual Struggles in Palliative Cancer Patients. J. Pain Symptom Manag. 2021, 62, e139–e147. [Google Scholar] [CrossRef]
- King, S.D.W.; Fitchett, G.; Murphy, P.E.; Pargament, K.I.; Martin, P.J.; Johnson, R.H.; Harrison, D.A.; Loggers, E.T. Spiritual or Religious Struggle in Hematopoietic Cell Transplant Survivors: Spiritual or Religious Struggle in HCT Survivors. Psycho-Oncology 2017, 26, 270–277. [Google Scholar] [CrossRef] [PubMed]
- King, S.D.W.; Fitchett, G.; Murphy, P.E.; Rajaee, G.; Pargament, K.I.; Loggers, E.T.; Harrison, D.A.; Johnson, R.H. Religious/Spiritual Struggle in Young Adult Hematopoietic Cell Transplant Survivors. J. Adolesc. Young Adult Oncol. 2018, 7, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Al Ahwal, M.S.; Al Zaben, F.; Sehlo, M.G.; Khalifa, D.A.; Koenig, H.G. Religiosity and Telomere Length in Colorectal Cancer Patients in Saudi Arabia. J. Relig. Health 2018, 57, 672–682. [Google Scholar] [CrossRef]
- Hulett, J.M.; Armer, J.M.; Leary, E.; Stewart, B.R.; McDaniel, R.; Smith, K.; Millspaugh, R.; Millspaugh, J. Religiousness, Spirituality, and Salivary Cortisol in Breast Cancer Survivorship: A Pilot Study. Cancer Nurs. 2018, 41, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, A.B.; Pereira, E.R.; Magnago, C.; Costa Rosa Andrade Silva, R.M.; Meira, K.C.; de Oliveira Martins, A. Distress and the Religious and Spiritual Coping of Brazilians Living with Cancer: A Cross-Sectional Study. Eur. J. Oncol. Nurs. 2020, 48, 101825. [Google Scholar] [CrossRef]
- Narayanan, S.; Milbury, K.; Wagner, R.; Cohen, L. Religious Coping in Cancer: A Quantitative Analysis of Expressive Writing Samples from Patients with Renal Cell Carcinoma. J. Pain Symptom Manag. 2020, 60, 737–745. [Google Scholar] [CrossRef]
- Pérez-Cruz, P.E.; Langer, P.; Carrasco, C.; Bonati, P.; Batic, B.; Tupper Satt, L.; Gonzalez Otaiza, M. Spiritual Pain Is Associated with Decreased Quality of Life in Advanced Cancer Patients in Palliative Care: An Exploratory Study. J. Palliat. Med. 2019, 22, 663–669. [Google Scholar] [CrossRef]
- Munoz, A.R.; Salsman, J.M.; Stein, K.D.; Cella, D. Reference values of the Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being: A report from the American Cancer Society’s studies of cancer survivors. Cancer 2015, 121, 1838–1844. [Google Scholar] [CrossRef] [Green Version]
- Leung, C.H.; Pong, H.K. Cross-Sectional Study of the Relationship between the Spiritual Wellbeing and Psychological Health among University Students. PLoS ONE 2021, 16, e0249702. [Google Scholar] [CrossRef]
- Chirico, F. Spiritual Well-Being in the 21st Century: It’s Time to Review the Current WHO’s Health Definition? J. Health Soc. Sci. 2016, 1, 11–16. [Google Scholar] [CrossRef]
- Peterman, A.H.; Fitchett, G.; Brady, M.J.; Hernandez, L.; Cella, D. Measuring spiritual well-being in people with cancer: The functional assessment of chronic illness therapy—Spiritual Well-being Scale (FACIT-Sp). Ann. Behav. Med. 2002, 24, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Puchalski, C.M. Spirituality in the cancer trajectory. Ann. Oncol. 2012, 23, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Hernandez, L.; Bonomi, A.E.; Corona, M.; Vaquero, M.; Shiomoto, G.; Baez, L. Spanish Language Translation and Initial Validation of the Functional Assessment of Cancer Therapy Quality-of-Life Instrument. Med. Care 1998, 36, 1407–1418. [Google Scholar] [CrossRef] [PubMed]
- Saiz, J.; Pung, M.A.; Wilson, K.L.; Pruitt, C.; Rutledge, T.; Redwine, L.; Taub, P.R.; Greenberg, B.H.; Mills, P.J. Is Belonging to a Religious Organization Enough? Differences in Religious Affiliation versus Self-Ratings of Spirituality on Behavioral and Psychological Variables in Individuals with Heart Failure. Healthcare 2020, 8, 129. [Google Scholar] [CrossRef]
- Hvidt, N.C.; Nielsen, K.T.; Kørup, A.K.; Prinds, C.; Hansen, D.G.; Viftrup, D.T.; Hvidt, E.A.; Hammer, E.R.; Falkø, E.; Locher, F.; et al. What is spiritual care? Professional perspectives on the concept of spiritual care identified through group concept making. BMJ Open 2020, 10, e042142. [Google Scholar] [CrossRef] [PubMed]
- Büssing, A. The Spiritual Needs Questionnaire in Research and Clinical Application: A Summary of Findings. J. Relig. Health 2021, 60, 3732–3748. [Google Scholar] [CrossRef]
- Toledo, G.; Ochoa, C.Y.; Farias, A.J. Religion and Spirituality: Their Role in the Psychosocial Adjustment to Breast Cancer and Subsequent Symptom Management of Adjuvant Endocrine Therapy. Support. Care Cancer 2021, 29, 3017–3024. [Google Scholar] [CrossRef]
- Cowden, R.G.; Pargament, K.I.; Chen, Z.J.; Davis, E.B.; Lemke, A.W.; Glowiak, K.J.; Rueger, S.Y.; Worthington, E.L. Religious/Spiritual Struggles and Psychological Distress: A Test of Three Models in a Longitudinal Study of Adults with Chronic Health Conditions. J. Clin. Psychol. 2022, 78, 544–558. [Google Scholar] [CrossRef]
- Leavitt-Alcántara, S.; Betz, J.; Medeiros Almeida, D.; Ferrara, B.; Xu, Y.; Diop, E.; Hamilton, O.; Young, C.; Ragsdale, J.R. Religiosity and Religious and Spiritual Struggle and Their Association to Depression and Anxiety among Adolescents Admitted to Inpatient Psychiatric Units. J. Health Care Chaplain. 2022, 1–13. [Google Scholar] [CrossRef]
- Rosmarin, D.H.; Pargament, K.I.; Mahoney, A. The Role of Religiousness in Anxiety, Depression, and Happiness in a Jewish Community Sample: A Preliminary Investigation. Ment. Health Relig. Cult. 2009, 12, 97–113. [Google Scholar] [CrossRef]
- Panier, L.Y.X.; Bruder, G.E.; Svob, C.; Wickramaratne, P.; Gameroff, M.J.; Weissman, M.M.; Tenke, C.E.; Kayser, J. Predicting Depression Symptoms in Families at Risk for Depression: Interrelations of Posterior EEG Alpha and Religion Spirituality. J. Affect. Disord. 2020, 274, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Stripp, T.K.; Wehberg, S.; Büssing, A.; Andersen-Ranberg, K.; Jensen, L.H.; Henriksen, F.; Laursen, C.B.; Søndergaard, J.; Hvidt, N.C. Protocol for EXICODE: The EXIstential health Cohort Denmark—A register and survey study of adult Danes. BMJ Open 2022, 12, e058257. [Google Scholar] [CrossRef] [PubMed]

| Authors | Total (%) | Methodological Quality |
|---|---|---|
| Al Ahwal et al., 2018 | 14/16 (87.5%) | Very good |
| Al-Natour et al., 2017 | 15/16 (93.75%) | Very good |
| Asgeirsdottir et al., 2017 | 12/16 (75%) | Good |
| Bai et al., 2016 | 13/16 (81.25%) | Good |
| Best et al., 2015 | 15/16 (93.75%) | Very good |
| Brown et al., 2015 | 14/16 (87.5%) | Very good |
| Canada et al., 2016 | 15/16 (93.75%) | Very good |
| Cannon et al., 2022 | 15/16 (93.75%) | Very good |
| Chaar et al., 2018 | 14/16 (87.5%) | Very good |
| Chen et al., 2021 | 15/16 (93.75%) | Very good |
| Cheng et al., 2019 | 15/16 (93.75%) | Very good |
| Damen et al., 2021 | 14/16 (87.5%) | Very good |
| Gielen et al., 2017 | 12/16 (75%) | Good |
| Goyal et al., 2019 | 15/16 (93.75%) | Very good |
| Hulett et al., 2018 | 15/16 (93.75%) | Very good |
| Kamijo and Miyamura 2020 | 15/16 (93.75%) | Very good |
| King et al., 2017 | 15/16 (93.75%) | Very good |
| King et al., 2018 | 15/16 (93.75%) | Very good |
| Leeson et al., 2015 | 15/16 (93.75%) | Very good |
| Mendoça et al., 2020 | 15/16 (93.75%) | Very good |
| Narayanan et al., 2020 | 15/16 (93.75%) | Very good |
| Pérez-Cruz et al., 2019 | 12/16 (75%) | Good |
| Rohde et al., 2019 | 14/16 (87.5%) | Very good |
| Sleight et al., 2021 | 14/16 (87.5%) | Very good |
| Walker et al., 2017 | 13/16 (81.25%) | Good |
| Yilmaz and Cengiz 2020 | 14/16 (87.5%) | Very good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almaraz, D.; Saiz, J.; Moreno Martín, F.; Sánchez-Iglesias, I.; Molina, A.J.; Goldsby, T.L. What Aspects of Religion and Spirituality Affect the Physical Health of Cancer Patients? A Systematic Review. Healthcare 2022, 10, 1447. https://doi.org/10.3390/healthcare10081447
Almaraz D, Saiz J, Moreno Martín F, Sánchez-Iglesias I, Molina AJ, Goldsby TL. What Aspects of Religion and Spirituality Affect the Physical Health of Cancer Patients? A Systematic Review. Healthcare. 2022; 10(8):1447. https://doi.org/10.3390/healthcare10081447
Chicago/Turabian StyleAlmaraz, David, Jesús Saiz, Florentino Moreno Martín, Iván Sánchez-Iglesias, Antonio J. Molina, and Tamara L. Goldsby. 2022. "What Aspects of Religion and Spirituality Affect the Physical Health of Cancer Patients? A Systematic Review" Healthcare 10, no. 8: 1447. https://doi.org/10.3390/healthcare10081447