
Kundalini Yoga for Post-Treatment Lyme Disease: A Preliminary Randomized Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Registration
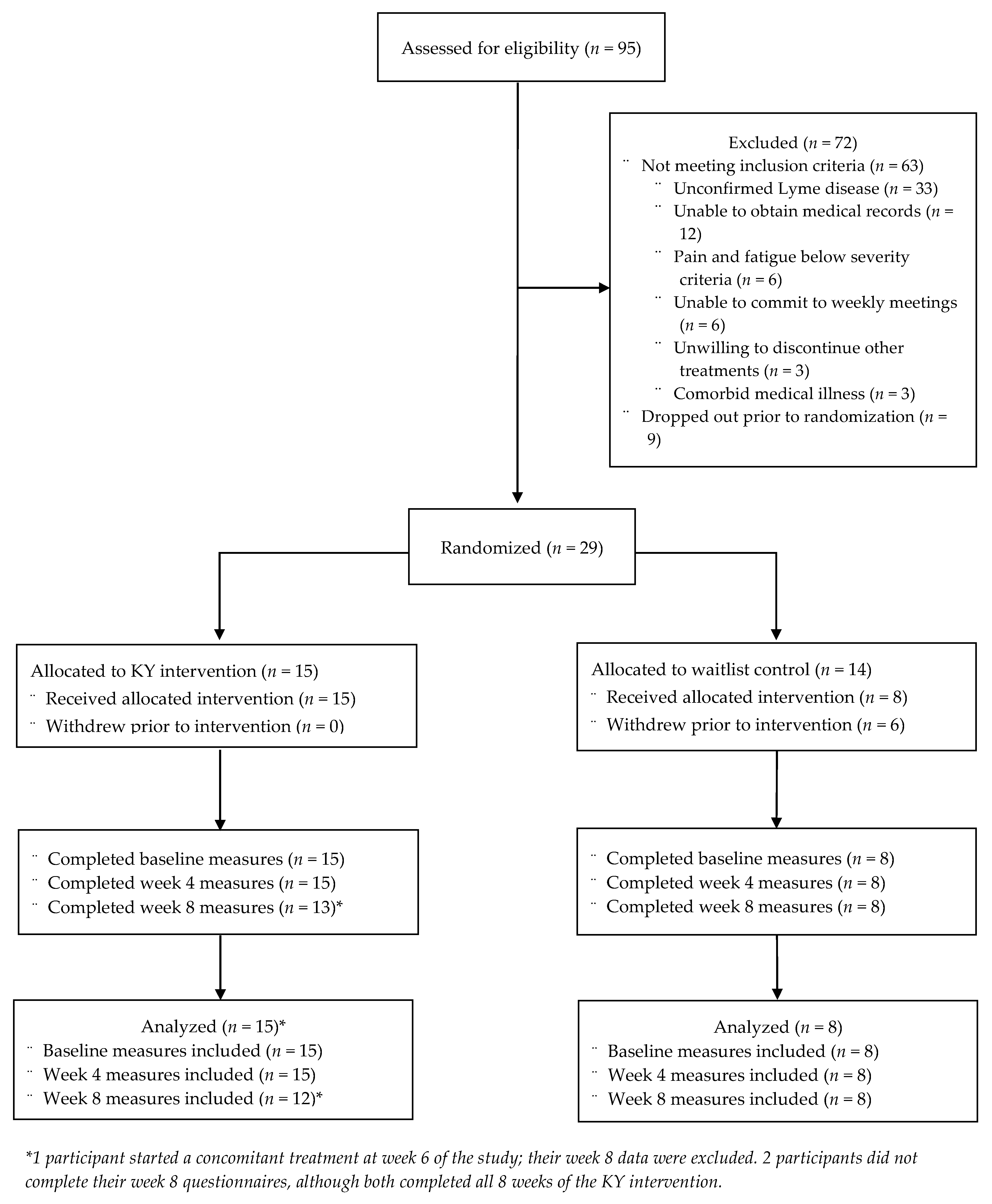
2.2. Participants
2.3. Measures
2.3.1. Adherence
2.3.2. Primary Outcome Measures
2.3.3. Secondary Outcome Measures
2.3.4. Pre-Treatment Variables
2.4. Intervention
2.5. Statistical Analysis
3. Results
3.1. Adherence
3.2. Primary Outcome Measures
3.3. Secondary Outcome Measures
3.4. Pre-Treatment Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Kundalini Yoga Daily Practice Protocol
Appendix A.1. Part 1: Light Stretching
Duration: 8 Minutes
- Standing: March in place. Inhale and elevate your right knee while bending your right arm at the elbow. Then, exhale and lower your leg and arm simultaneously. Repeat this motion using your left leg and arm. Continue for one minute.
- Standing: Inhale, raise your arms above your head and touch your palms together. Then, keeping your palms together and arms straight, exhale and bend towards the floor, hinging at the waist. Inhale again and return to the raised position. Continue for one minute.
- Sitting in a comfortable position with your legs crossed *: Shoulder lifts. Inhale and raise your shoulders. Exhale and lower your shoulders. Continue for one minute.
- Sitting in a comfortable position with your legs crossed *: Place your hands on your shoulders, ideally with your thumbs behind your shoulders, the rest of your fingers in front of your shoulders, and your elbows raised so that your arms are parallel to the floor. Inhale and twist your torso to the left, then exhale and twist your torso to the right. Continue for one minute. Finish with an inhale and exhale facing forward.
- Sitting in a comfortable position with your legs crossed *: Grab both ankles with your hands (or, if you are sitting in a chair, place your hands on your knees). Keep your elbows straight. Inhale and round your lumbar spine, then exhale and flex your lumbar spine. Continue for one minute.
- Sitting with legs stretched forward and spread apart in front of you *: Inhale and raise your arms above your head, then exhale and reach towards your right foot (or, if you are sitting in a chair, reach towards your right knee). Inhale and raise your arms above your head again, then exhale and reach towards the left foot (left knee if you are sitting in a chair). Continue for one minute.
- Sitting still in a comfortable position: Breathe steadily. Remain attentive and mindful of your body. Focus inward for two minutes.
Appendix A.2. Part 2: Directed Breathing
Duration: 8 Minutes
Appendix A.3. Part 3: Guided Meditation
Duration: 11 Minutes
References
- Rosenberg, R.; Lindsey, N.P.; Fischer, M.; Gregory, C.J.; Hinckley, A.F.; Mead, P.S.; Paz-Bailey, G.; Waterman, S.H.; Drexler, N.A.; Kersh, G.J.; et al. Vital signs: Trends in reported vectorborne disease cases—United States and territories, 2004–2016. Morb. Mortal. Wkly. Rep. 2018, 67, 496–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aucott, J.N. Posttreatment Lyme Disease Syndrome. Infect. Dis. Clin. N. Am. 2015, 29, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Fallon, B.A.; Sotsky, J. Conquering Lyme Disease: Science Bridges the Great Divide; Columbia University Press: New York, NY, USA, 2018. [Google Scholar]
- Batheja, S.; Nields, J.A.; Landa, A.; Fallon, B.A. Post-treatment lyme syndrome and central sensitization. J. Neuropsychiatry Clin. Neurosci. 2013, 25, 176–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, L.; Stricker, R.B. Final report of the Lyme disease review panel of the Infectious Diseases Society of America: A pyrrhic victory? Clin. Infect. Dis. 2010, 51, 1108–1109. [Google Scholar] [CrossRef] [Green Version]
- Fallon, B.A. A reappraisal of the U.S. clinical trials of post-treatment Lyme disease syndrome. Open Neurol. J. 2012, 6, 79–87. [Google Scholar] [CrossRef]
- Park, C.L.; Elwy, A.R.; Maiya, M.; Sarkin, A.J.; Riley, K.E.; Eisen, S.V.; Gutierrez, I.; Finkelstein-Fox, L.; Lee, S.Y.; Casteel, D.; et al. The Essential Properties of Yoga Questionnaire (EPYQ): Psychometric properties. Int. J. Yoga Therap. 2018, 28, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Lauche, R.; Klose, P.; Lange, S.; Langhorst, J.; Dobos, G. Yoga for improving health-related quality of life, mental health and cancer-related symptoms in women diagnosed with breast cancer. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonadonna, R. Meditation’s impact on chronic illness. Holist. Nurs. Pract. 2003, 17, 309–319. [Google Scholar] [CrossRef]
- Shannahoff-Khalsa, D.S. Kundalini Yoga meditation techniques for psycho-oncology and as potential therapies for cancer. Integr. Cancer Ther. 2005, 4, 87–100. [Google Scholar] [CrossRef]
- Rouleau, C.R.; Garland, S.N.; Carlson, L.E. The impact of mindfulness-based interventions on symptom burden, positive psychological outcomes, and biomarkers in cancer patients. Cancer Manag. Res. 2015, 7, 121–131. [Google Scholar] [CrossRef] [Green Version]
- Jindani, F.; Turner, N.; Khalsa, S.B.S. A yoga intervention for posttraumatic stress: A preliminary randomized control trial. Evid.-Based Complement. Altern. Med. 2015, 2015, 351746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saper, R.B.; Lemaster, C.; Delitto, A.; Sherman, K.J.; Herman, P.M.; Sadikova, E.; Stevans, J.; Keosaian, J.E.; Cerrada, C.J.; Femia, A.L.; et al. Yoga, physical therapy, or education for chronic low back pain: A randomized noninferiority trial. Ann. Intern. Med. 2017, 167, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Carson, J.W.; Carson, K.M.; Jones, K.D.; Bennett, R.M.; Wright, C.L.; Mist, S.D. A pilot randomized controlled trial of the Yoga of Awareness program in the management of fibromyalgia. Pain 2010, 151, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Cillessen, L.; Johannsen, M.; Speckens, A.E.M.; Zachariae, R. Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and survivors: A systematic review and meta-analysis of randomized controlled trials. Psychooncology. 2019, 28, 2257–2269. [Google Scholar] [CrossRef] [Green Version]
- Carlson, L.E. Mindfulness-based interventions for physical conditions: A narrative review evaluating levels of evidence. ISRN Psychiatry 2012, 2012, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Michalsen, A.; Traitteur, H.; Lüdtke, R.; Brunnhuber, S.; Meier, L.; Jeitler, M.; Büssing, A.; Kessler, C. Yoga for chronic neck pain: A pilot randomized controlled clinical trial. J. Pain 2012, 13, 1122–1130. [Google Scholar] [CrossRef]
- Park, J.; McCaffrey, R.; Newman, D.; Liehr, P.; Ouslander, J.G. A pilot randomized controlled trial of the effects of chair yoga on pain and physical function among community-dwelling older adults with lower eYoga for chronic neck pain: A pilot randomized controlled clinical trial extremity osteoarthritis. J. Am. Geriatr. Soc. 2017, 65, 592–597. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.A.; Petronis, J.; Smith, D.; Goodrich, D.; Wu, J.; Ravi, N.; Doyle, E.J.; Juckett, R.G.; Kolar, M.M.; Gross, R.; et al. Effect of Iyengar yoga therapy for chronic low back pain. Pain 2005, 115, 107–117. [Google Scholar] [CrossRef]
- Marciniak, R.; Sheardova, K.; Čermáková, P.; Hudeček, D.; Šumec, R.; Hort, J. Effect of meditation on cognitive functions in context of aging and neurodegenerative diseases. Front. Behav. Neurosci. 2014, 8, 17. [Google Scholar] [CrossRef] [Green Version]
- Simon, N.M.; Hofmann, S.G.; Rosenfield, D.; Hoeppner, S.S.; Hoge, E.A.; Bui, E.; Khalsa, S.B.S. Efficacy of yoga vs cognitive behavioral therapy vs stress education for the treatment of generalized anxiety disorder: A randomized clinical trial. JAMA Psychiatry 2021, 78, 13–20. [Google Scholar] [CrossRef]
- Victorson, D.; Hankin, V.; Burns, J.; Weiland, R.; Maletich, C.; Sufrin, N.; Schuette, S.; Gutierrez, B.; Brendler, C. Feasibility, acceptability and preliminary psychological benefits of mindfulness meditation training in a sample of men diagnosed with prostate cancer on active surveillance: Results from a randomized controlled pilot trial. Psychooncology 2017, 26, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Wolff, M.; Rogers, K.; Erdal, B.; Chalmers, J.P.; Sundquist, K.; Midlöv, P. Impact of a short home-based yoga programme on blood pressure in patients with hypertension: A randomized controlled trial in primary care. J. Hum. Hypertens. 2016, 30, 599–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, M.G.; Curtiss, J.; Hofmann, S.G.; Khalsa, S.B.S. Kundalini yoga for generalized anxiety disorder: An exploration of treatment efficacy and possible mechanisms. Int. J. Yoga Therap. 2018, 28, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.; Nissim, R.; Elliott, M. Mindfulness-based cognitive therapy for young adults with cancer. Univ. West. Ont. Med. J. 2018, 87, 11–13. [Google Scholar] [CrossRef]
- Grossman, P.; Kappos, L.; Gensicke, H.; D’Souza, M.; Mohr, D.C.; Penner, I.K.; Steiner, C. MS quality of life, depression, and fatigue improve after mindfulness training: A randomized trial. Neurology 2010, 75, 1141–1149. [Google Scholar] [CrossRef] [Green Version]
- Garfinkel, M.S.; Singhal, A.; Katz, W.A.; Allan, D.A.; Reshetar, R.; Schumacher, H.R. Yoga-based intervention for carpal tunnel syndrome: A randomized trial. J. Am. Med. Assoc. 1998, 280, 1601–1603. [Google Scholar] [CrossRef] [Green Version]
- Puksic, S.; Mitrovic, J.; Culo, M.-I.; Zivkovic, M.; Orehovec, B.; Bobek, D.; Morovic-Vergles, J. Effects of Yoga in Daily Life program in rheumatoid arthritis: A randomized controlled trial. Complement. Ther. Med. 2021, 57, 102639. [Google Scholar] [CrossRef]
- Pascoe, M.C.; Thompson, D.R.; Ski, C.F. Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology 2017, 86, 152–168. [Google Scholar] [CrossRef]
- García-Sesnich, J.; Flores, M.; Ríos, M.; Aravena, J. Longitudinal and immediate effect of Kundalini yoga on salivary levels of cortisol and activity of alpha-amylase and its effect on perceived stress. Int. J. Yoga 2017, 10, 73. [Google Scholar] [CrossRef]
- Liu, Y.Z.; Wang, Y.X.; Jiang, C.L. Inflammation: The common pathway of stress-related diseases. Front. Hum. Neurosci. 2017, 11, 1–11. [Google Scholar] [CrossRef]
- Lunde, C.E.; Sieberg, C.B. Walking the tightrope: A proposed model of chronic pain and stress. Front. Neurosci. 2020, 14, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geenen, R.; Dures, E. A biopsychosocial network model of fatigue in rheumatoid arthritis: A systematic review. Rheumatology 2019, 58, V10–V21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, T.L.; Epel, E.S.; Lin, J.; Blackburn, E.H.; Wolkowitz, O.M.; Bridwell, D.A.; Zanesco, A.P.; Aichele, S.R.; Sahdra, B.K.; MacLean, K.A.; et al. Intensive meditation training, immune cell telomerase activity, and psychological mediators. Psychoneuroendocrinology 2011, 36, 664–681. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, H.; Ravish, H.; Silvia, C.W.D.; Srinivas, H. Molecular signature of the immune response to yoga therapy in stress-related chronic disease conditions: An insight. Int. J. Yoga 2020, 13, 9–17. [Google Scholar]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef]
- Djalilova, D.M.; Schulz, P.S.; Berger, A.M.; Case, A.J.; Kupzyk, K.A.; Ross, A.C. Impact of yoga on inflammatory biomarkers: A systematic review. Biol. Res. Nurs. 2019, 21, 198–209. [Google Scholar] [CrossRef]
- Touradji, P.; Aucott, J.N.; Yang, T.; Rebman, A.W.; Bechtold, K.T. Cognitive decline in post-treatment Lyme Disease syndrome. Arch. Clin. Neuropsychol. 2019, 34, 455–465. [Google Scholar] [CrossRef]
- Eyre, H.A.; Siddarth, P.; Acevedo, B.; Van Dyk, K.; Paholpak, P.; Ercoli, L.; St Cyr, N.; Yang, H.; Khalsa, D.S.; Lavretsky, H. A randomized controlled trial of Kundalini yoga in mild cognitive impairment. Int. Psychogeriatrics 2017, 29, 557–567. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Singh, S.; Sibinga, E.M.S.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M.; et al. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Crawford, P.; Brown, B.; Charise, A. The Routledge Companion to Health Humanities, 1st ed.; Routledge: New York, NY, USA, 2020; ISBN 9781138579903. [Google Scholar]
- Cramer, H.; Quinker, D.; Schumann, D.; Wardle, J.; Dobos, G.; Lauche, R. Adverse effects of yoga: A national cross-sectional survey. BMC Complement. Altern. Med. 2019, 19, 190. [Google Scholar] [CrossRef] [Green Version]
- Amtmann, D.; Cook, K.F.; Jensen, M.P.; Chen, W.-H.; Choi, S.; Revicki, D.; Cella, D.; Rothrock, N.; Keefe, F.; Callahan, L. Development of A Promis Item Bank to Measure Pain Interference Keywords Quality-of-life outcomes; quality-of-life measurement. Pain 2010, 150, 173–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.S.; Cella, D.; Choi, S.; Junghaenel, D.U.; Christodoulou, C.; Gershon, R.; Stone, A. How item banks and their application can influence measurement practice in rehabilitation medicine: A PROMIS fatigue item bank example. Arch. Phys. Med. Rehabil. 2011, 92, S20–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHorney, C.A.; Ware, J.E.; Raczek, A.E. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and Clinical Tests of Validity in Measuring Physical and Mental Health Constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Newschaffer, C.J. Validation of Behavioral Risk Factor Surveillance System (BRFSS) HRQOL Measures in a Statewide Sample; Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion: Atlanta, GA, USA, 1998. [Google Scholar]
- Fallon, B.A.; Zubcevik, N.; Bennett, C.; Doshi, S.; Rebman, A.W.; Kishon, R.; Moeller, J.R.; Octavien, N.R.; Aucott, J.N. The General Symptom Questionnaire-30 (GSQ-30): A Brief Measure of Multi-System Symptom Burden in Lyme Disease. Front. Med. 2019, 6, 283. [Google Scholar] [CrossRef] [Green Version]
- Pilkonis, P.A.; Choi, S.W.; Reise, S.P.; Stover, A.M.; Riley, W.T.; Cella, D. Item Banks for Measuring Emotional Distress from the PROMIS: Depression, Anxiety and Anger. Assessment 2011, 18, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.; Stover, A.; Buysse, D.J.; Yu, L.; Moul, D.E.; Germain, A.; Stover, A.; Dodds, N.E. Development and validation of patient-reported outcome measures for sleep disturbance and sleep-related impairments. Sleep 2010, 33, 781–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, M.; Bjorner, J.B.; Gandek, B.; Bruce, B.; Fries, J.F.; Ware, J.E. The PROMIS Physical Function item bank was calibrated to a standardized metric and shown to improve measurement efficiency. J. Clin. Epidemiol. 2014, 67, 516–526. [Google Scholar] [CrossRef] [Green Version]
- Hahn, E.A.; DeWalt, D.A.; Bode, R.K.; Garcia, S.F.; DeVellis, R.F.; Correia, H.; Cella, D. PROMIS Cooperative Group New English and Spanish social health measures will facilitate evaluating health determinants. Health Psychol. 2014, 33, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Morgan, S.J.; Kelly, V.E.; Amtmann, D.; Salem, R.; Hafner, B.J. Self-Reported Cognitive Concerns in People with Lower Limb Loss. Arch. Phys. Med. Rehabil. 2016, 97, 912–918. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carleton, R.N.; Norton, M.A.P.J.; Asmundson, G.J.G. Fearing the unknown: A short version of the Intolerance of Uncertainty Scale. J. Anxiety Disord. 2007, 21, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; Riley, J.L.I.; Myers, C.D.; Sadler, I.J.; Kvaal, S.A.; Geisser, M.E.; Keefe, F.J. The Coping Strategies Questionnaire: A Large Sample, Item Level Factor Analysis. Clin. J. Pain 1997, 13, 43–49. [Google Scholar] [CrossRef]
- Carlson, E.B.; Smith, S.R.; Palmieri, P.A.; Dalenberg, C.; Ruzek, J.I.; Kimerling, R.; Burling, T.A.; Spain, D.A. Development and Validation of a Brief Self-Report Measure of Trauma Exposure: The Trauma History Screen. Psychol. Assess. 2011, 23, 463–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Speckens, A.E.M.; Spinhoven, P.; Sloekers, P.P.A.; Bolk, J.H.; Hemert, A.M. A validation study of the Whitley Index, the Illness Attitude Scales, and the Somatosensory Amplification Scale in general medical and general practice patients. J. Psychosom. Res. 1996, 40, 95–104. [Google Scholar] [CrossRef]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The Brief Illness Perception Questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef]
- R Core Team R. A Language and Environment for Statistical Computing 2018. Available online: https://www.r-project.org/ (accessed on 28 May 2022).
- Bates, D.; Mächler, M.; Bolker, B.M.; Walker, S.C. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest package: Tests in linear mixed effects models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Gendle, M.H. The problem of dualism in modern western medicine. Mens Sana Monogr. 2016, 14, 141–151. [Google Scholar] [CrossRef]
- Keilp, J.G.; Madden, S.P.; Gorlyn, M.; Burke, A.K.; Oquendo, M.A.; Mann, J.J. The lack of meaningful association between depression severity measures and neurocognitive performance. J. Affect. Disord. 2018, 241, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Rebman, A.W.; Aucott, J.N. Post-treatment Lyme disease as a model for persistent symptoms in Lyme disease. Front. Med. 2020, 7, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| KY | WLC | Overall | |
|---|---|---|---|
| (n = 15) | (n = 8) | (n = 23) | |
| Sex = Male (n (%)) | 7 (46.7) | 4 (50.0) | 11 (47.8) |
| Ethnicity (n (%)) | |||
| Hispanic | 1 (6.7) | 0 (0.0) | 1 (4.3) |
| White (non-Hispanic) | 12 (80.0) | 6 (75.0) | 18 (78.3) |
| Not reported | 2 (13.3) | 2 (25.0) | 4 (17.4) |
| Age (M (SD)) * | 48.47 (12.99) | 62.62 (14.51) | 53.39 (14.90) |
| Marital Status (n (%)) | |||
| Single (never married) | 1 (6.7) | 2 (25.0) | 3 (13.0) |
| Married/Living with partner | 11 (73.3) | 5 (62.5) | 16 (69.6) |
| Divorced/Separated | 1 (6.7) | 0 (0.0) | 1 (4.3) |
| Not reported | 2 (13.3) | 1 (12.5) | 3 (13.0) |
| Education (n (%)) | |||
| Completed high school or GED | 2 (13.3) | 0 (0.0) | 2 (8.7) |
| Some college (less than 4 years) | 4 (26.7) | 1 (12.5) | 5 (21.7) |
| Completed 4-year college degree | 2 (13.3) | 3 (37.5) | 5 (21.7) |
| Completed post-college degree | 4 (26.7) | 2 (25.0) | 6 (26.1) |
| Not reported | 3 (20.0) | 2 (25.0) | 5 (21.7) |
| Employment (n (%)) | |||
| Employed at least half-time for pay | 1 (6.7) | 0 (0.0) | 1 (4.3) |
| Employed full-time for pay | 2 (13.3) | 4 (50.0) | 6 (40.0) |
| Unemployed more than 6 months | 4 (26.7) | 0 (0.0) | 4 (17.4) |
| Disabled | 4 (26.7) | 0 (0.0) | 4 (17.4) |
| Retired | 0 (0.0) | 1 (12.5) | 1 (4.3) |
| Other | 1 (6.7) | 2 (25.0) | 3 (13.0) |
| Not reported | 3 (20.0) | 1 (12.5) | 4 (17.4) |
| Medical Utilization (n (%)) a | |||
| Lifetime: medical hospitalization | 11 (78.6) | 6 (75.0) | 17 (77.3) |
| Lifetime: psychiatric hospitalization | 3 (21.4) | 0 (0.0) | 3 (13.6) |
| Lifetime: major surgery | 11 (78.6) | 6 (75.0) | 17 (77.3) |
| Past 3 months: emergency room visit | 1 (7.1) | 0 (0.0) | 1 (4.5) |
| Past 3 months: urgent care visit | 2 (14.3) | 1 (12.5) | 3 (13.6) |
| Past 3 months: overnight hospitalization | 1 (7.1) | 0 (0.0) | 1 (4.5) |
| Variable | Baseline | Week 4 | Week 8 | |||
|---|---|---|---|---|---|---|
| KY | WLC | KY | WLC | KY | WLC | |
| M (SD) (n = 15) | M (SD) (n = 8) | M (SD) (n = 15) | M (SD) (n = 8) | M (SD) (n = 12) a | M (SD) (n = 8) | |
| Primary Outcomes | ||||||
| Pain | 5.87 (2.59) | 5.12 (2.90) | 4.93 (2.56) | 4.25 (2.38) | 4.50 (2.75) | 3.75 (2.71) |
| Pain Interference | 65.52 (9.43) | 55.86 (7.89) | 62.84 (11.85) | 52.70 (7.86) | 61.08 (11.68) | 52.90 (8.28) |
| Fatigue | 68.26 (9.77) | 57.56 (7.92) | 64.44 (8.70) | 57.14 (7.93) | 63.74 (6.46) | 57.15 (9.44) |
| Global Health | 1.86 (0.77) | 2.25 (0.46) | 2.00 (0.96) | 2.25 (0.89) | 2.58 (1.31) | 2.62 (0.74) |
| Secondary Outcomes | ||||||
| Multisystem Symptoms * | 67.92 (25.81) | 37.75 (11.47) | 49.45 (26.73) | 34.50 (13.50) | 54.90 (26.48) | 29.50 (16.32) |
| Depression (PROMIS) | 59.70 (11.61) | 51.85 (8.58) | 56.44 (12.93) | 47.97 (8.32) | 56.74 (11.88) | 48.71 (8.91) |
| Anxiety | 62.64 (12.00) | 53.98 (8.86) | 56.96 (13.34) | 51.10 (11.77) | 58.78 (13.77) | 52.17 (9.85) |
| Sleep Disturbance | 58.98 (11.83) | 56.10 (10.79) | 60.45 (11.01) | 55.01 (8.18) | 55.95 (13.19) | 54.14 (5.83) |
| Physical Functioning | 38.24 (7.36) | 42.66 (7.85) | 38.88 (8.05) | 39.80 (4.75) | 37.41 (8.56) | 41.26 (4.63) |
| Social Functioning | 35.49 (8.41) | 46.44 (8.72) | 38.78 (6.95) | 43.64 (6.28) | 38.75 (6.85) | 46.56 (5.86) |
| Depression (BDI) | 22.92 (13.11) | 13.63 (7.65) | 18.5 (11.30) | 13 (8.72) | 16 (10.72) | 11 (8.19) |
| Cognition * | 26.77 (7.95) | 39.38 (4.29) | 30.22 (9.49) | 37.73 (5.75) | 31.66 (7.77) | 37.61 (4.41) |
| Mindfulness | 3.68 (1.08) | 4.66 (0.85) | 3.68 (1.18) | 4.36 (1.05) | 3.72 (1.34) | 4.28 (0.78) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murray, L.; Alexander, C.; Bennett, C.; Kuvaldina, M.; Khalsa, G.; Fallon, B. Kundalini Yoga for Post-Treatment Lyme Disease: A Preliminary Randomized Study. Healthcare 2022, 10, 1314. https://doi.org/10.3390/healthcare10071314
Murray L, Alexander C, Bennett C, Kuvaldina M, Khalsa G, Fallon B. Kundalini Yoga for Post-Treatment Lyme Disease: A Preliminary Randomized Study. Healthcare. 2022; 10(7):1314. https://doi.org/10.3390/healthcare10071314
Chicago/Turabian StyleMurray, Lilly, Charles Alexander, Clair Bennett, Mara Kuvaldina, Gurucharan Khalsa, and Brian Fallon. 2022. "Kundalini Yoga for Post-Treatment Lyme Disease: A Preliminary Randomized Study" Healthcare 10, no. 7: 1314. https://doi.org/10.3390/healthcare10071314