
Design of Smart and Secured Healthcare Service Using Deep Learning with Modified SHA-256 Algorithm


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Smart Healthcare System
2.1. Login Module
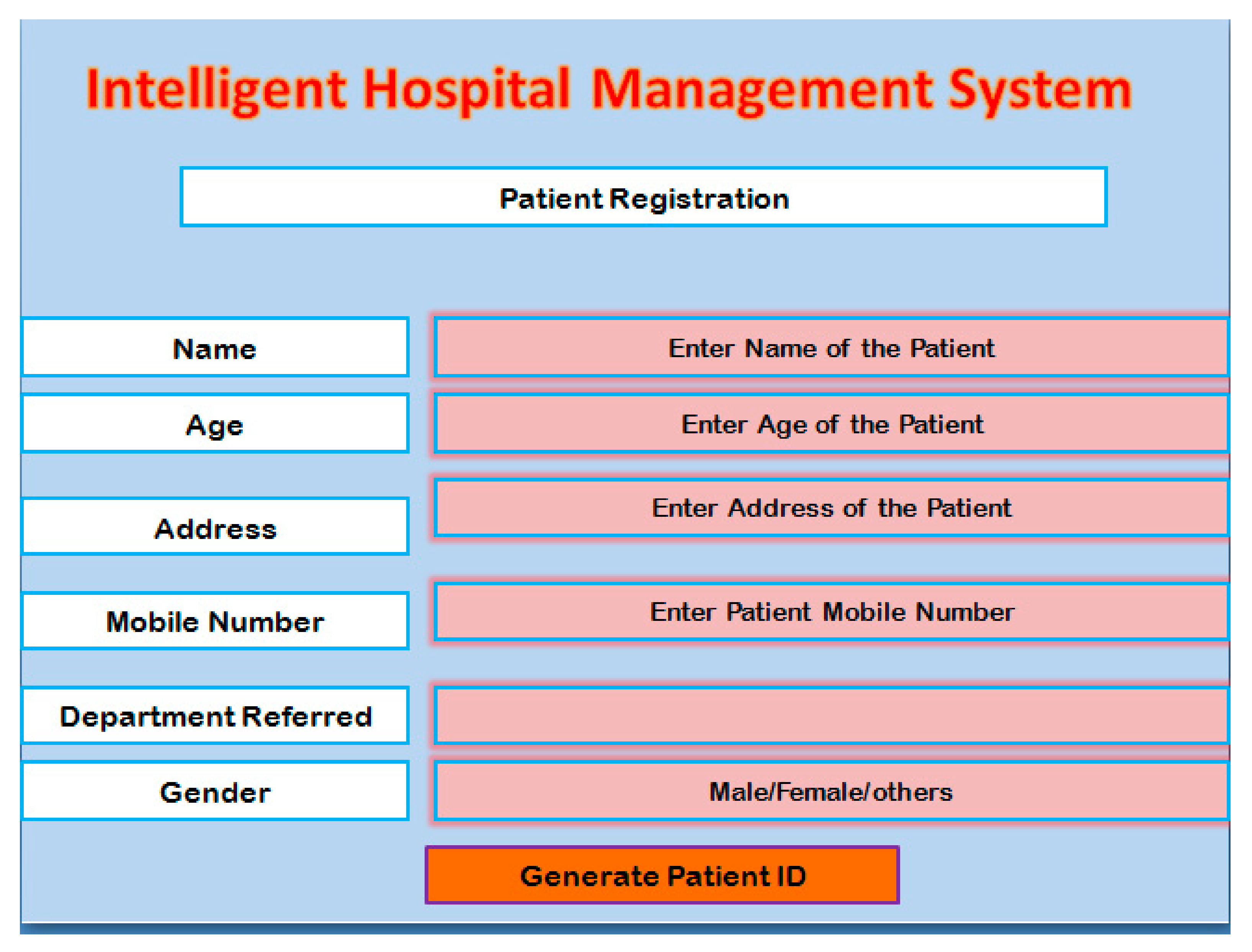
2.2. Registration Module
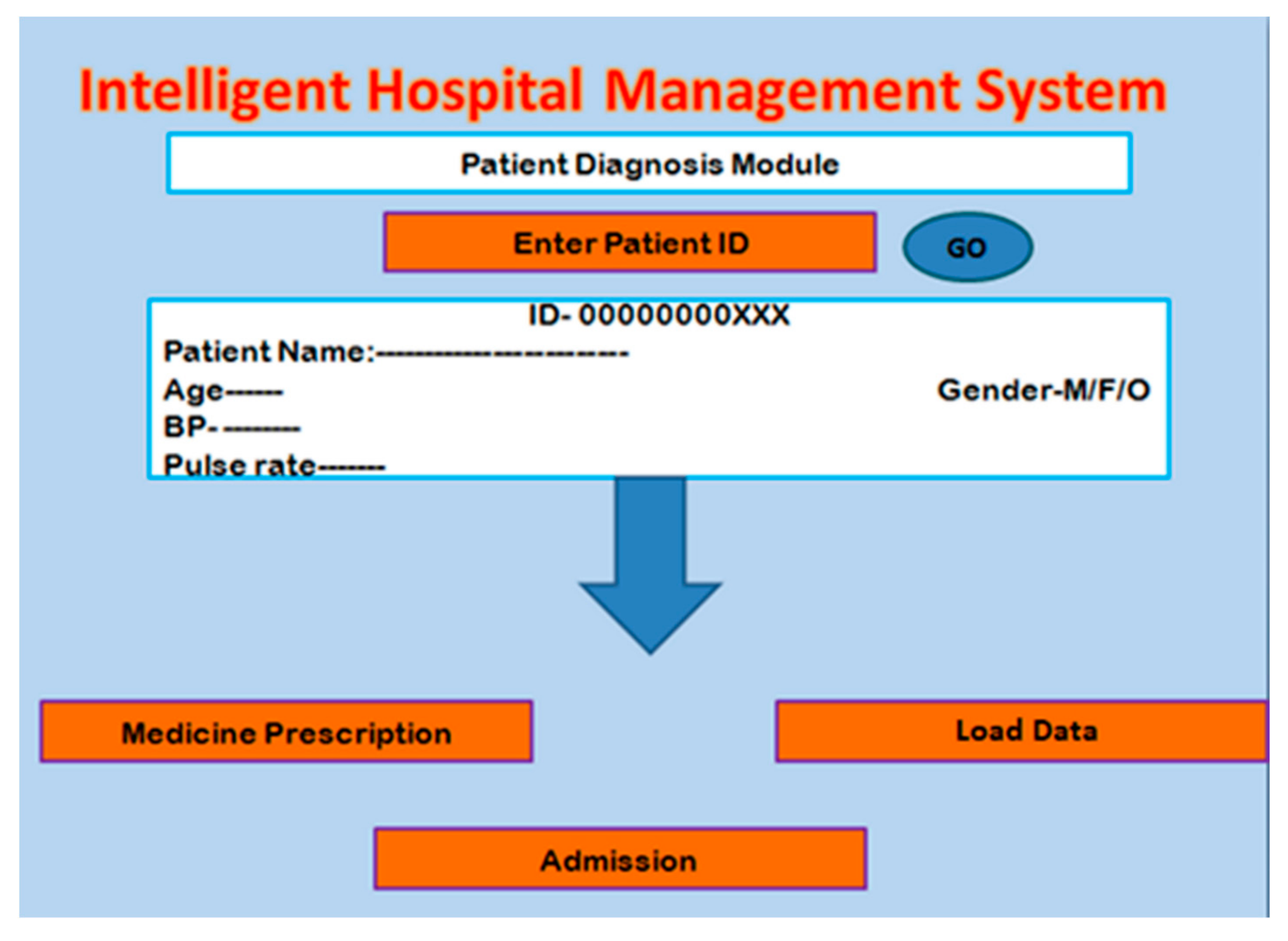
2.3. Patient Diagnosis Module
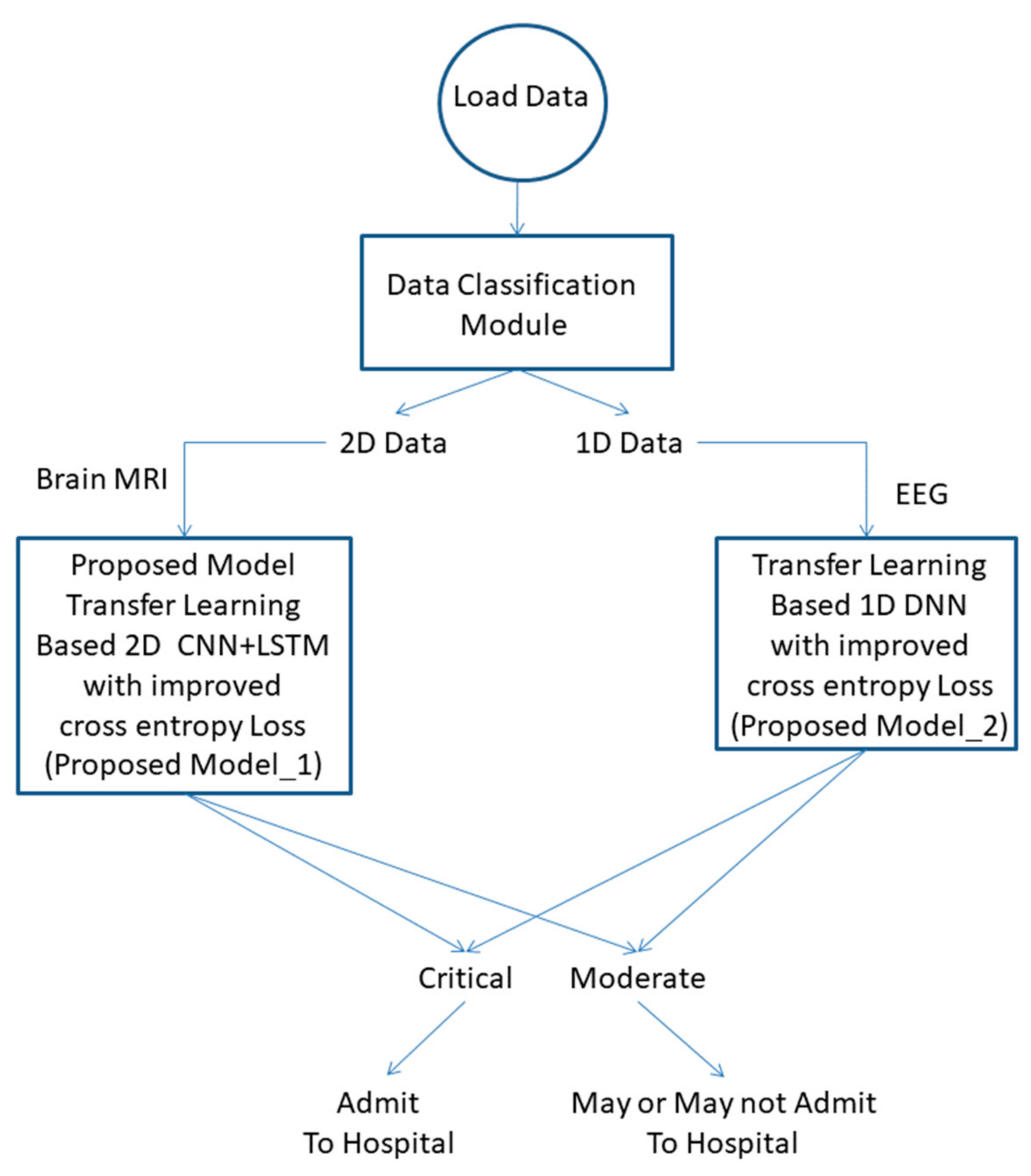
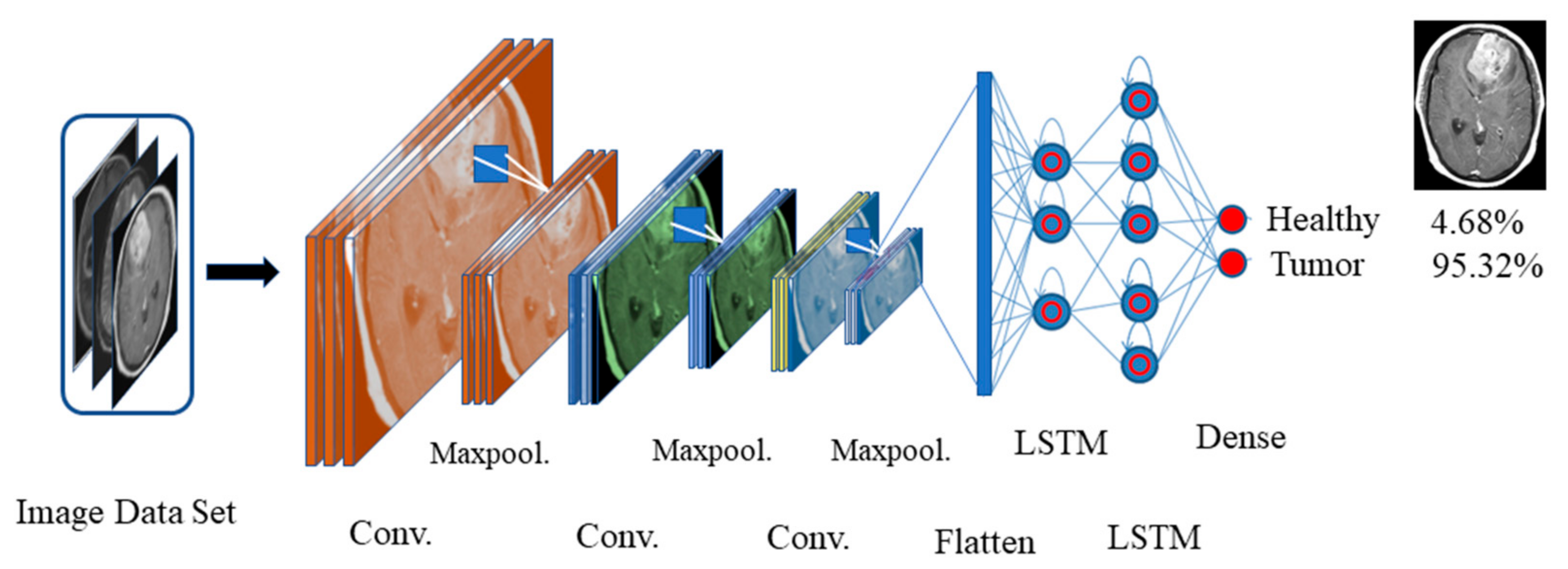
2.4. Deep-Learning-Based MRI and EEG Classification
2.4.1. Data Classification Module
| Algorithm 1: Data classification |
| Input: Data represents the length of data Step 1. Evaluate the size of the data Step 2. If transfer to the proposed mode_1 Step 3. If transfer to the proposed mode_2 Result: Data transfer to the corresponding model |
2.4.2. Transfer-Learning-Based CNN-LSTM Model
2.4.3. Transfer-Learning-Based DNN Model
2.4.4. Improved Cross-Entropy
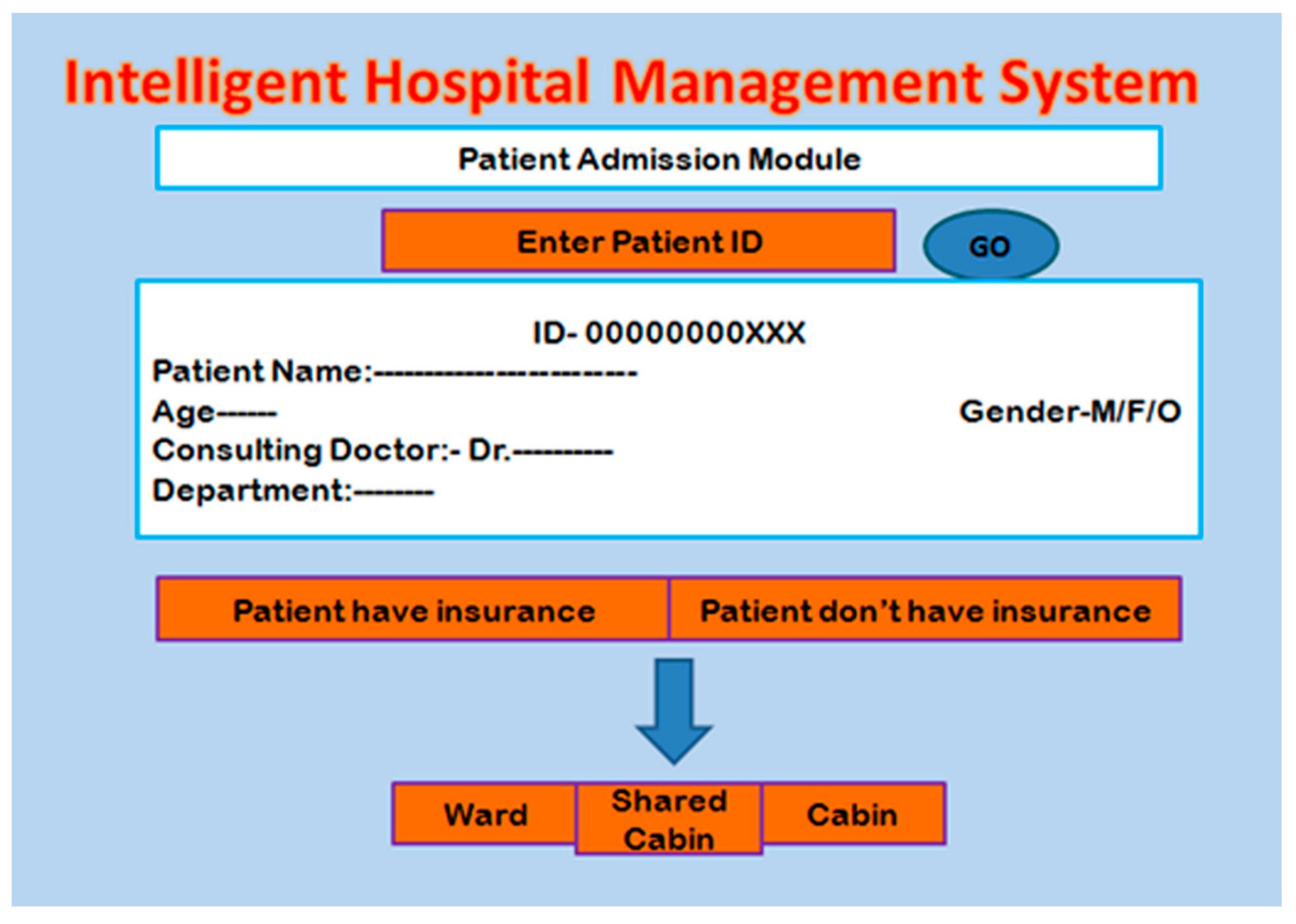
2.5. Patient Admission Module
2.6. Security Issue
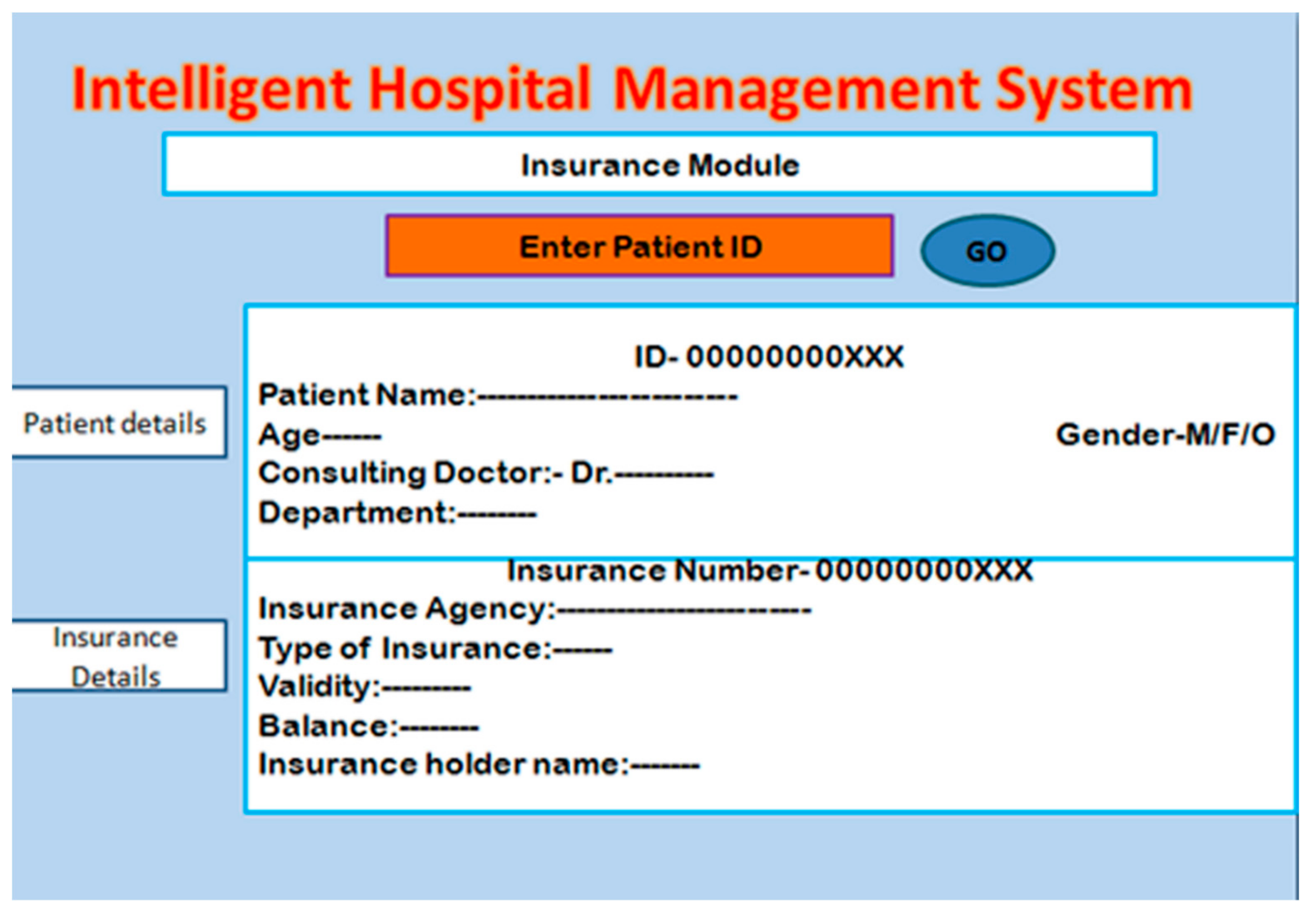
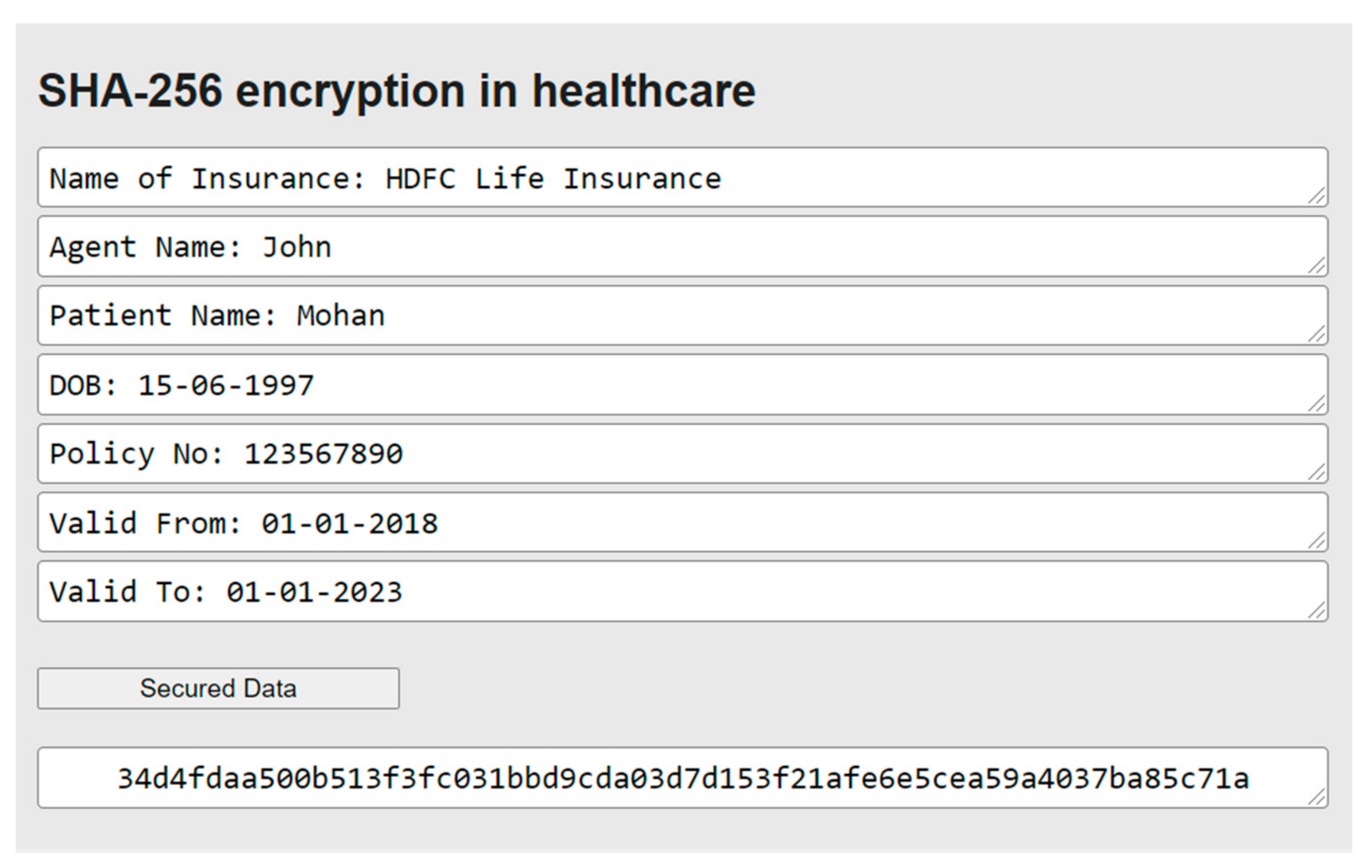
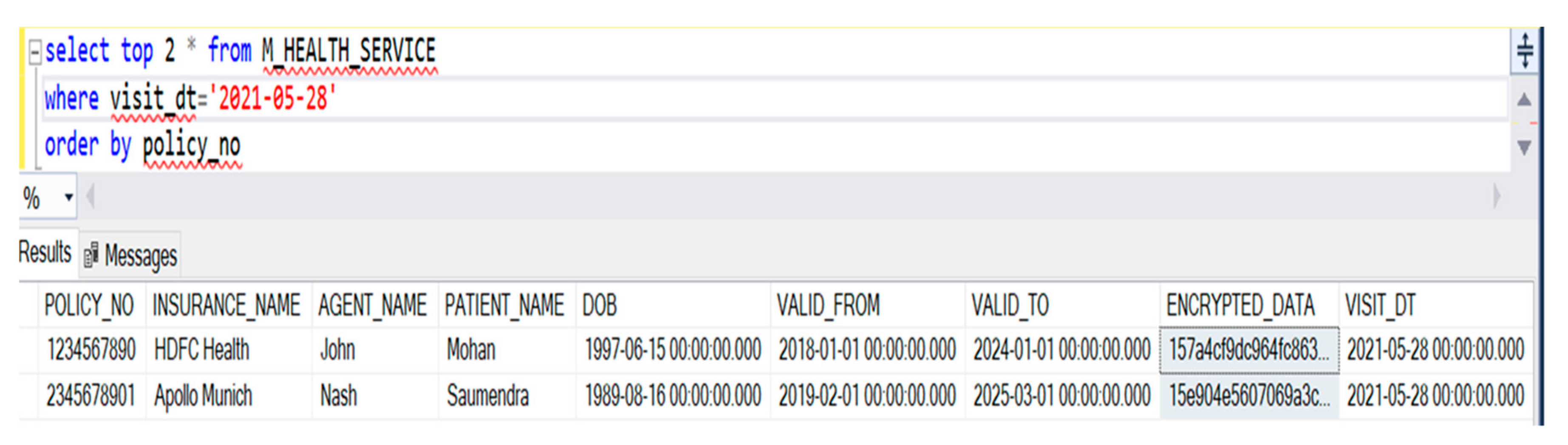
2.6.1. Insurance Module
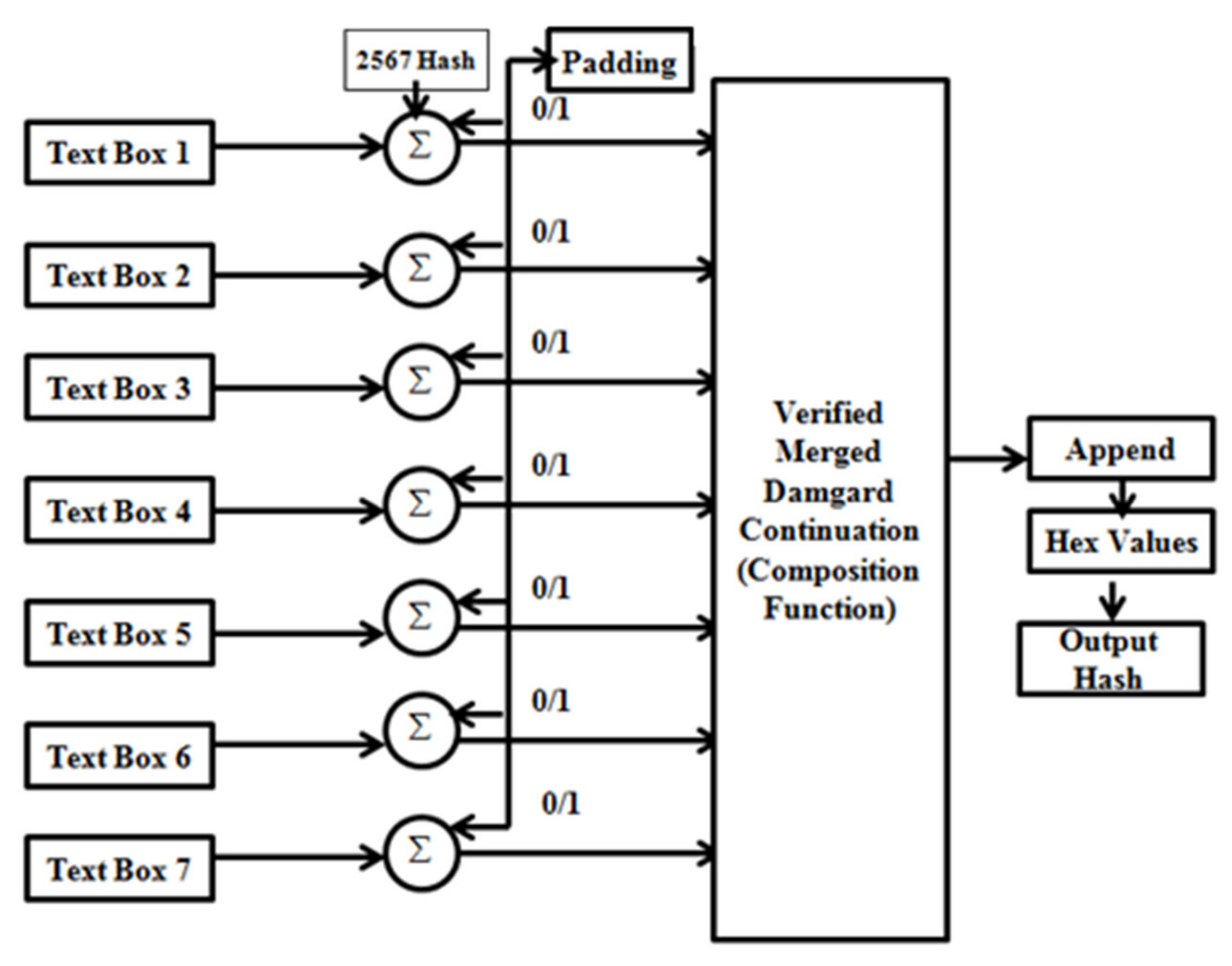
2.6.2. Hashing the Medical Management Data for Security
3. Results and Discussion
- 1.
- Preprocessing of inputs:
- Generate the SHA-2 constant K.
- Feed the input message from textboxes.
- 2.
- Convert the same into binary form.
- 3.
- Take the concatenation of the values from textboxes and constant K.
- 4.
- Check if padding is required:
- Case 1: If a 512-bit value is generated, then no padding is required.
- Case 2: If 512-bit is not generated, then pad with the 0 s and 1 s to generate the same.
- 5.
- Feed the same output into the MD construction compression function:
- Values get concatenated to the hashes of the compression function.
- Append the values.
- Repetitive compression of values.
- 6.
- Append the values of the hashing output
- 7.
- Result obtained.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahmud, R.; Koch, F.L.; Buyya, R. Cloud-fog interoperability in IoT-enabled healthcare solutions. ACM Int. Conf. Proceeding Ser. 2018, 2017, 1–10. [Google Scholar] [CrossRef]
- Dorj, U.O.; Lee, M.; Choi, J.Y.; Lee, Y.K.; Jeong, G. The Intelligent Healthcare Data Management System Using Nanosensors. J. Sens. 2017, 2017, 7483075. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.M.; Mallick, P.K. Blockchain technology for security issues and challenges in IoT. Procedia Comput. Sci. 2018, 132, 1815–1823. [Google Scholar] [CrossRef]
- Matloob, I.; Khan, S.A.; Rahman, H.U. Sequence Mining and Prediction-Based Healthcare Fraud Detection Methodology. IEEE Access 2020, 8, 143256–143273. [Google Scholar] [CrossRef]
- Canlas, R.D., Jr. Data mining in healthcare: Data Mining in Healthcare: Current Applications and Issues. Master’s Thesis, School of Information Systems & Management, Carnegie Mellon University, Adelaide, SA, Australia, 2009; pp. 1–10. [Google Scholar]
- Mohanty, M.N.; Mohapatra, S.K.; Pradhan, B.B. Multi-Agent Approach based Blood Bank Management System for Emergency Patients. In Proceedings of the 2019 Annual Meeting on Management Engineering, Kuala Lumpur, Malaysia, 8–10 December 2019; pp. 75–81. [Google Scholar]
- Sarangi, L.; Mohanty, M.N.; Patnaik, S. Design of ANFIS based e-health care system for cardio vascular disease detection. In Proceedings of the International Conference on Intelligent and Interactive Systems and Applications; Springer: Cham, Switzerland, 2016; pp. 445–453. [Google Scholar]
- Moosavi, S.R.; Gia, T.N.; Nigussie, E.; Rahmani, A.M.; Virtanen, S.; Tenhunen, H.; Isoaho, J. End-to-end security scheme for mobility enabled healthcare Internet of Things. Futur. Gener. Comput. Syst. 2016, 64, 108–124. [Google Scholar] [CrossRef]
- Manikandan, R.; Patan, R.; Gandomi, A.H.; Sivanesan, P.; Kalyanaraman, H. Hash polynomial two factor decision tree using IoT for smart health care scheduling. Expert Syst. Appl. 2020, 141, 112924. [Google Scholar] [CrossRef]
- Gahlot, S.; Reddy, S.R.N.; Kumar, D. Review of smart health monitoring approaches with survey analysis and proposed framework. IEEE Internet Things J. 2019, 6, 2116–2127. [Google Scholar] [CrossRef]
- Saha, R.; Kumar, G.; Rai, M.K.; Thomas, R.; Lim, S.J. Privacy ensured e-Healthcare for fog-enhanced IoT based applications. IEEE Access 2019, 7, 44536–44543. [Google Scholar] [CrossRef]
- Ali, A.; Pasha, M.F.; Ali, J.; Fang, O.H.; Masud, M.; Jurcut, A.D.; Alzain, M.A. Deep Learning Based Homomorphic Secure Search-Able Encryption for Keyword Search in Blockchain Healthcare System: A Novel Approach to Cryptography. Sensors 2022, 22, 528. [Google Scholar] [CrossRef]
- Garrido, A.; López, L.J.R.; Álvarez, N.B. A simulation-based AHP approach to analyze the scalability of EHR systems using blockchain technology in healthcare institutions. Inform. Med. Unlocked 2021, 24, 100576. [Google Scholar] [CrossRef]
- Saberi, M.A.; Adda, M.; Mcheick, H. Break-Glass Conceptual Model for Distributed EHR management system based on Blockchain, IPFS and ABAC. Procedia Comput. Sci. 2022, 198, 185–192. [Google Scholar] [CrossRef]
- Fatokun, T.; Nag, A.; Sharma, S. Towards a blockchain assisted patient owned system for electronic health records. Electronics 2021, 10, 580. [Google Scholar] [CrossRef]
- Mani, V.; Manickam, P.; Alotaibi, Y.; Alghamdi, S.; Khalaf, O.I. Hyperledger healthchain: Patient-centric IPFS-based storage of health records. Electronics 2021, 10, 3003. [Google Scholar] [CrossRef]
- Ahene, E.; Walker, J.; Gyening, R.M.O.M.; Abdul-Salaam, G.; Hayfron-Acquah, J.B. Heterogeneous signcryption with proxy re-encryption and its application in EHR systems. Telecommun. Syst. 2022, 80, 59–75. [Google Scholar] [CrossRef]
- Paliwal, G.; Bunglowala, A.; Kanthed, P. An architectural design study of electronic healthcare record systems with associated context parameters on MIMIC III. Health Technol. 2022, 12, 313–327. [Google Scholar] [CrossRef]
- Ali, A.; Almaiah, M.A.; Hajjej, F.; Pasha, M.F.; Fang, O.H.; Khan, R.; Zakarya, M. An Industrial IoT-Based Blockchain-Enabled Secure Searchable Encryption Approach for Healthcare Systems Using Neural Network. Sensors 2022, 22, 572. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Rahim, H.A.; Ali, J.; Pasha, M.F.; Masud, M.; Rehman, A.U.; Baz, M. A Novel Secure Blockchain Framework for Accessing Electronic Health Records Using Multiple Certificate Authority. Appl. Sci. 2021, 11, 9999. [Google Scholar] [CrossRef]
- Martsenyuk, V.; Povoroznyuk, V.; Semenets, A.; Martynyuk, L. On an approach of the solution of machine learning problems integrated with data from the open-source system of electronic medical records: Application for fractures prediction. In Proceedings of the International Conference on Artificial Intelligence and Soft Computing; Springer: Cham, Switzerland, 2019; pp. 228–239. [Google Scholar]
- Huang, Z.; Du, X.; Chen, L.; Li, Y.; Liu, M.; Chou, Y.; Jin, L. Convolutional Neural Network Based on Complex Networks for Brain Tumor Image Classification With a Modified Activation Function. IEEE Access 2020, 8, 89281–89290. [Google Scholar] [CrossRef]
- Ker, J.; Singh, S.P.; Bai, Y.; Rao, J.; Lim, T.; Wang, L. Image thresholding improves 3-dimensional convolutional neural network diagnosis of different acute brain hemorrhages on computed tomography scans. Sensors 2019, 19, 2167. [Google Scholar] [CrossRef] [Green Version]
- Ker, J.; Bai, Y.; Lee, H.Y.; Rao, J.; Wang, L. Automated brain histology classification using machine learning. J. Clin. Neurosci. 2019, 66, 239–245. [Google Scholar] [CrossRef]
- Ertosun, M.G.; Rubin, D.L. Automated grading of gliomas using deep learning in digital pathology images: A modular approach with ensemble of convolutional neural networks. AMIA Annu. Symp. Proc. 2015, 2015, 1899. [Google Scholar] [PubMed]
- Ge, C.; Gu, I.Y.H.; Jakola, A.S.; Yang, J. Enlarged training dataset by pairwise GANs for molecular-based brain tumor classification. IEEE Access 2020, 8, 22560–22570. [Google Scholar] [CrossRef]
- Huda, S.; Yearwood, J.; Jelinek, H.F.; Hassan, M.M.; Fortino, G.; Buckland, M. A hybrid feature selection with ensemble classification for imbalanced healthcare data: A case study for brain tumor diagnosis. IEEE Access 2016, 4, 9145–9154. [Google Scholar] [CrossRef]
- Naga Srinivasu, P.; Srinivasa Rao, T.; Dicu, A.M.; Mnerie, C.A.; Olariu, I. A comparative review of optimisation techniques in segmentation of brain MR images. J. Intell. Fuzzy Syst. 2020, 38, 6031–6043. [Google Scholar] [CrossRef]
- Srinivasu, P.N.; Rao, T.S.; Balas, V.E. Volumetric Estimation of the Damaged Area in the Human Brain from 2D MR Image. Int. J. Inf. Syst. Modeling Des. 2020, 11, 74–92. [Google Scholar] [CrossRef]
- Das, A.; Mohapatra, S.K.; Mohanty, M.N. Brain Image Classification Using Optimized Extreme Gradient Boosting Ensemble Classifier. In Proceedings of the Biologically Inspired Techniques in Many Criteria Decision Making (BITMDM); Springer: Singapore, 2022; pp. 221–229. [Google Scholar]
- Das, A.; Mohapatra, S.K.; Mohanty, M.N. Design of deep ensemble classifier with fuzzy decision method for biomedical image classification. Appl. Soft Comput. 2022, 115, 108178. [Google Scholar] [CrossRef]
- Panda, S.; Das, A.; Mishra, S.; Mohanty, M.N. Epileptic seizure detection using deep ensemble network with empirical wavelet transform. Meas. Sci. Rev. 2021, 4, 110–116. [Google Scholar] [CrossRef]
- Chakrabarty, N. Brain MRI Images for Brain Tumor Detection. 2019. Available online: https://www.kaggle.com/navoneel/brain-mri-images-for-brain-tumor-detection (accessed on 23 January 2022).
- Andrzejak, R.G.; Lehnertz, K.; Mormann, F.; Rieke, C.; David, P.; Elger, C. Indications of nonlinear deterministic and finite-dimensional structures in time series of brain electrical activity: Dependence on recording region and brain state. Phys. Rev. E 2001, 64, 061907. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, T.K.; Chakraborty, P.; Roy, G.G.; Panigrahi, B.K. Discrete harmony search based expert model for epileptic seizure detection in electroencephalography. Expert Syst. Appl. 2012, 39, 4055–4062. [Google Scholar] [CrossRef]
- Backes, M.; Barthe, G.; Berg, M.; Grégoire, B.; Kunz, C.; Skoruppa, M.; Béguelin, S.Z. Verified security of merkle-damgård. 2012 IEEE 25th Computer Security Foundations Symposium, Cambridge, MA, USA, 25–27 June 2012; 2012; pp. 354–368. [Google Scholar] [CrossRef] [Green Version]
- Nidhya, R.; Shanthi, S.; Kumar, M. A novel encryption design for wireless body area network in remote healthcare system using enhanced RSA algorithm. In Intelligent System Design; Springer: Singapore, 2021; pp. 255–263. [Google Scholar]
- Kumar, K.K.; Ramaraj, E.; Srikanth, B.; Rao, A.S.; Prasad, P.B.V.N. Role of MD5 Message-Digest Algorithm for Providing Security to Low-Power Devices. In Proceedings of the 2022 6th International Conference on Intelligent Computing and Control Systems (ICICCS), Madurai, India, 25–27 May 2022; pp. 352–358. [Google Scholar]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Input | Description |
|---|---|
| Name | The user inputs the name of the patient who needs the treatment. |
| Age | Age of the patient in years. |
| Address | Address of the patient. |
| Mobile number | Mobile number of the patient for communication. |
| Department referred | The patient is referred to the respective department based on the symptoms. |
| Gender | Gender of the patient (Male/Female/Other) |
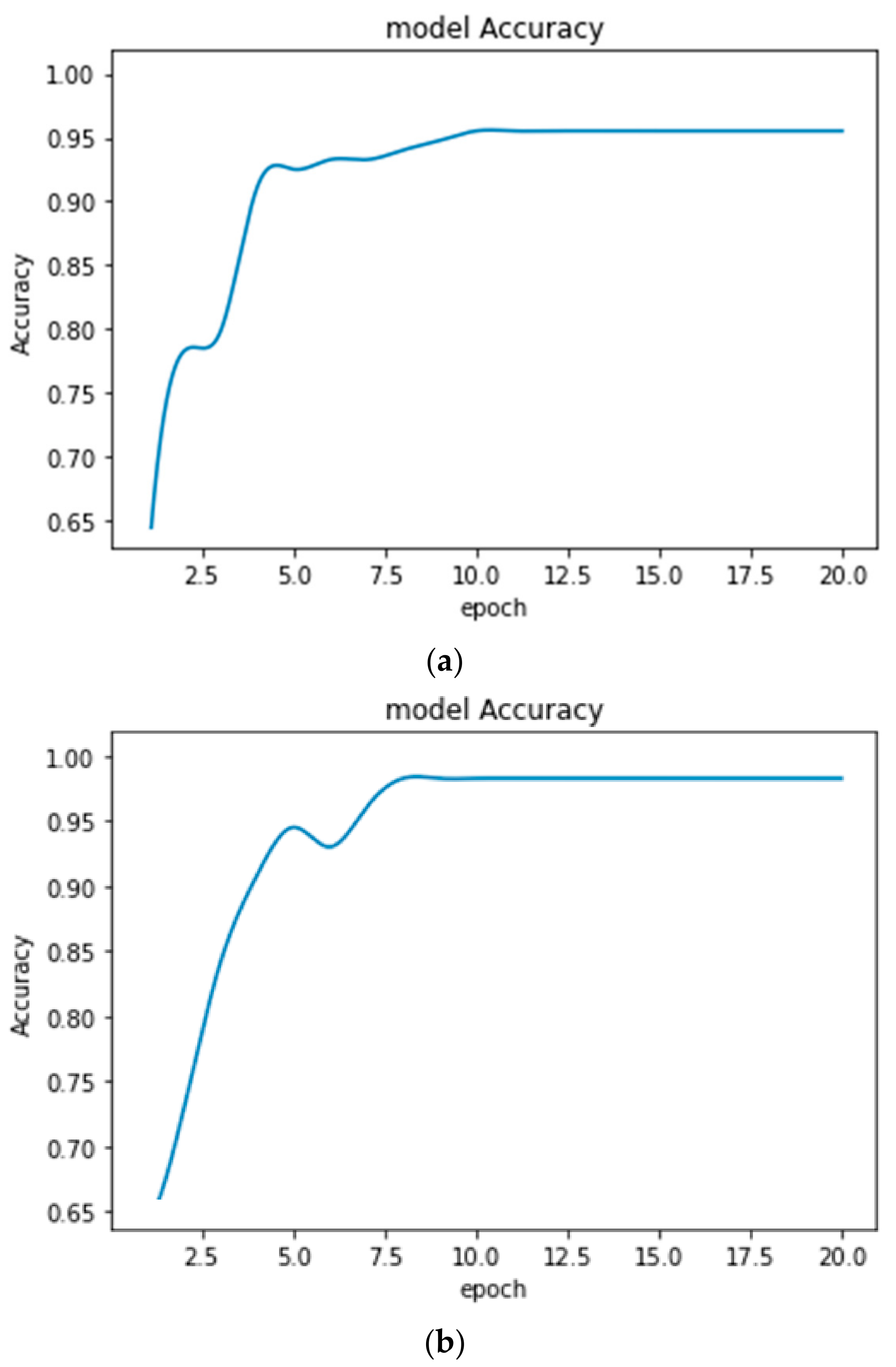
| Dataset | Accuracy (%) | |
|---|---|---|
| With the Earlier Form of CE | With Improved CE | |
| Brain MRI | 95.48 | 98.51 |
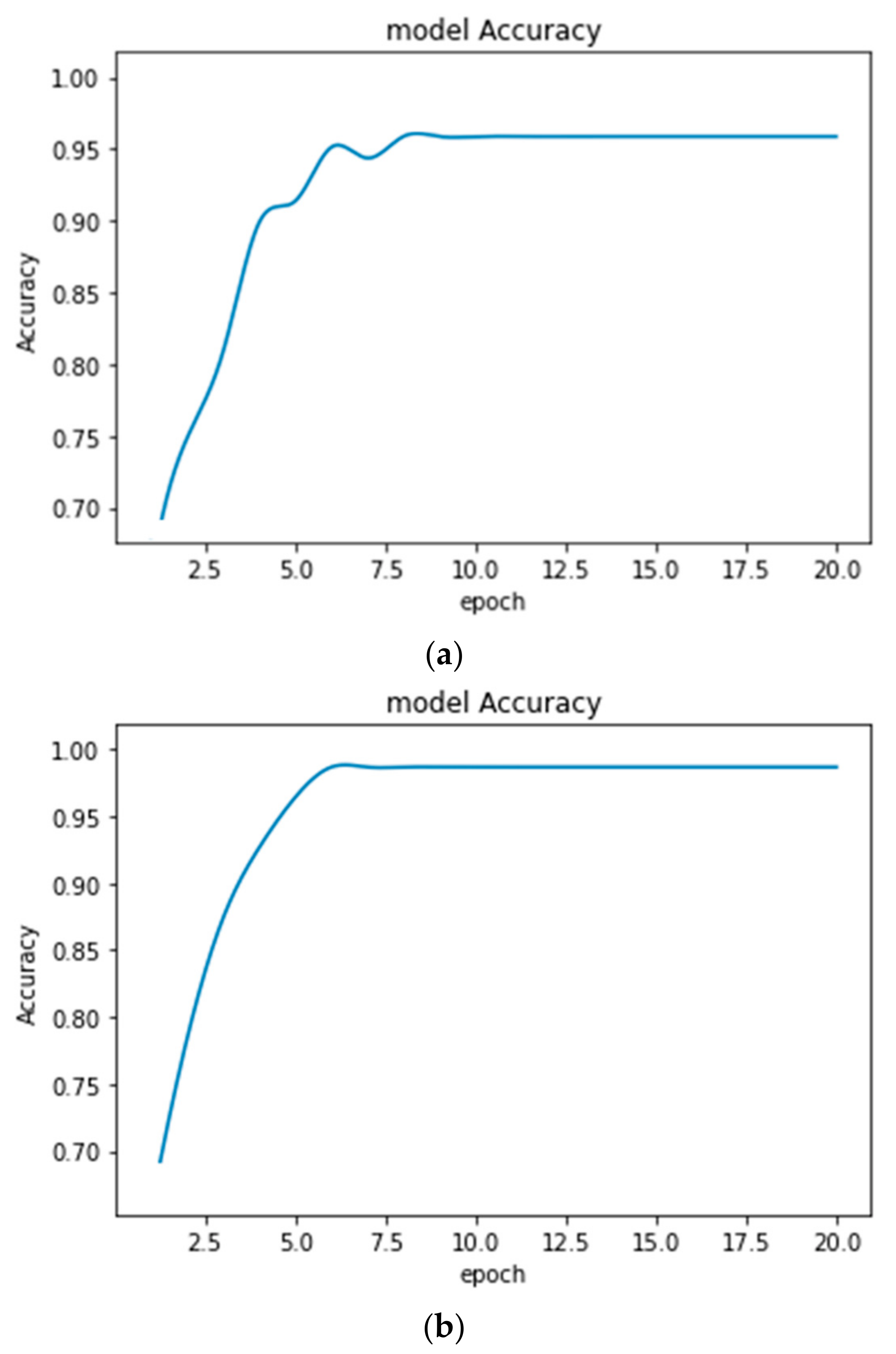
| Dataset | Accuracy (%) | |
|---|---|---|
| With the Earlier Form of CE | With Improved CE | |
| NSC-ND dataset | 95.16 | 96.60 |
| UoB dataset | 95.01 | 98.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohanty, M.D.; Das, A.; Mohanty, M.N.; Altameem, A.; Nayak, S.R.; Saudagar, A.K.J.; Poonia, R.C. Design of Smart and Secured Healthcare Service Using Deep Learning with Modified SHA-256 Algorithm. Healthcare 2022, 10, 1275. https://doi.org/10.3390/healthcare10071275
Mohanty MD, Das A, Mohanty MN, Altameem A, Nayak SR, Saudagar AKJ, Poonia RC. Design of Smart and Secured Healthcare Service Using Deep Learning with Modified SHA-256 Algorithm. Healthcare. 2022; 10(7):1275. https://doi.org/10.3390/healthcare10071275
Chicago/Turabian StyleMohanty, Mohan Debarchan, Abhishek Das, Mihir Narayan Mohanty, Ayman Altameem, Soumya Ranjan Nayak, Abdul Khader Jilani Saudagar, and Ramesh Chandra Poonia. 2022. "Design of Smart and Secured Healthcare Service Using Deep Learning with Modified SHA-256 Algorithm" Healthcare 10, no. 7: 1275. https://doi.org/10.3390/healthcare10071275