
Medication Errors in Intensive Care Units: An Umbrella Review of Control Measures

 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
- Participants: all systematic reviews of literature that had target populations of healthcare professionals involved in the prescription, distribution, or administration of medication in adult ICUs were included. These professionals included nurses, pharmacists, and physicians of any medical discipline or specialty. Systematic reviews that concerned nursing students and/or trainees of any healthcare discipline were excluded.
- Interventions: all systematic reviews that evaluated the efficacy of interventions aimed at preventing or reducing MEs were included.
- Outcomes: all systematic reviews that reported MEs and evaluated error rates, incidence, or prevalence as their primary or secondary outcome were included.
- Setting: all systematic reviews that analyzed interventions or strategies put in place in the ICU were included. Authors defined an ICU as all of the units that cater to the healthcare needs of patients in critical condition who require a high level of intensity of care.
- Study typology: only systematic reviews and/or meta-analysis studies were included.
2.2. Study Selection
2.3. Assessment of Quality
2.4. Data Extraction and Synthesis
3. Results
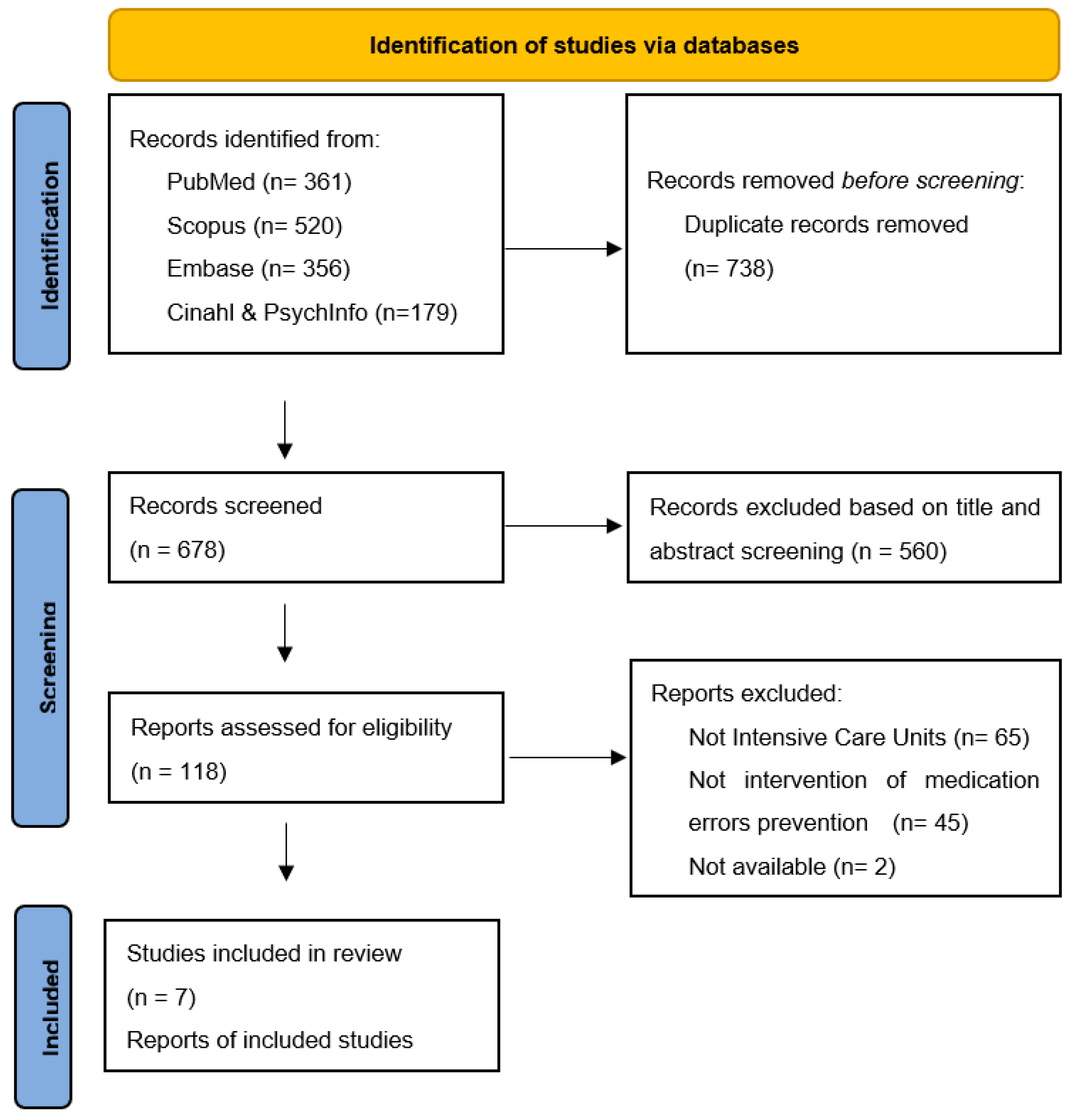
3.1. Study Selection
3.2. Characteristics of the Studies Included
- -
- by “systems”, we refer to technologies: computerized physician order entry (CPOE), smart infusion pumps, team members, e.g., pharmacists, and organizational factors, e.g., staff working shifts.
- -
- by “processes”, we refer to medication review and medicine reconciliation.
3.3. Technologies to Prevent MEs
- Barcode technology. This technology allows the electronic identification of patients and the cross-checking of medication details, patient data, the hour of administration, and the staff that executed the administration, based on checking the four Rs: right dosage, right drug, right time, and right administration of the drug. In their systematic review, Manias et al. [26] included a study that showed the real efficacy of this technology for reducing medication errors in the administration and dispensing stages [39].
- The use of automatized systems for the distribution of medication was examined in one study [40]. Based on its findings, the implementation of an automatized system for the distribution of medication did not have beneficial and/or protective effects concerning MEs during the dispensing stage.
- Technological systems for endovenous infusions (smart pumps). The efficacy of these systems for reducing error rates was not documented in the two studies included by Manias et al. [26]. The two studies showed an error reduction rate that was not statistically significant (4.78 vs. 4.95 per 1000 patients per day, p = 0.96; 2.03 vs. 2.41 errors per 100 patients per day, p = 0.124) [29,40].
- Support systems for clinical decisions, such as the computer-assisted antibiotic-dose monitor. Results from the five included studies demonstrated a statistically significant reduction in medication errors after the implementation of this new technology.
3.4. Processes to Prevent Medication Errors
3.5. Team Members to Prevent MEs
3.6. Organizational Interventions to Prevent Medication Errors
3.7. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Coordinating Council for Medication Error Reporting and Prevention. About Medication Errors. Available online: https://www.nccmerp.org/ (accessed on 20 June 2022).
- Wears, R.L.; Sutcliffe, K.M. Still Not Safe; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Giannetta, N.; Dionisi, S.; Tonello, M.; Di Simone, E.D.M.M. A Worldwide Bibliometric Analysis of Published Literature on Medication Errors. J. Patient Saf. 2022, 18, 201–209. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Medication without Harm. WHO Global Patient Safety Challenge. 2017. Available online: https://www.who.int/publications/i/item/WHO-HIS-SDS-2017.6 (accessed on 10 May 2022).
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768–770. [Google Scholar] [CrossRef] [Green Version]
- Maggiore, P.; Gajetti, M.; Bonifacino, A. Dal Fattore Umano alla Safety in Aviazione, 2017th ed.; Società Editrice Esculapio: Bologna, Italy, 2017. [Google Scholar]
- Giannetta, N.; Dionisi, S.; Ricciardi, F.; Di Muzio, F.; Penna, G.; Diella, G.; Di Simone, E.; Di Muzio, M. Look-alike, sound-alike drugs: Strategies for preventing medication errors. G. Ital. Farm. Clin. 2019, 33, 119–128. [Google Scholar]
- Giannetta, N.; Dionisi, S.; Cassar, M.; Trapani, J.; Renzi, E.; Di Simone, E.; Di Muzio, M. Measuring knowledge, attitudes and behavior of nurses in medication management: Cross-cultural comparisons in Italy and Malta. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 5167–5175. [Google Scholar] [PubMed]
- Giannetta, N.; Dionisi, S.; Stievano, A.; Eltaybani, S.; Abdelgawad, M.E.; Katigri, M.R.; Azadboni, T.T.; López-Soto, P.J.; Morales-Cané, I.; Ali, I.; et al. Comparison across 12 countries on knowledge, attitude, and behavior scores about medication errors in Intensive Care Units: An international study. Eur. Rev. Med. Pharm. Sci. 2021, 25, 7223–7230. [Google Scholar]
- Dionisi, S.; Di Simone, E.; Liquori, G.; De Leo, A.; Di Muzio, M.; Giannetta, N. Medication errors’ causes analysis in home care setting: A systematic review. Public Health Nurs. 2021, 1, 22. [Google Scholar] [CrossRef]
- Dionisi, S.; Giannetta, N.; Maselli, N.; Di Muzio, M.; Di Simone, E. Medication errors in homecare setting: An Italian validation study. Public Health Nurs. 2021, 38, 1116–1125. [Google Scholar] [CrossRef]
- Caggiano, G.; Napoli, C.; Coretti, C.; Lovero, G.; Scarafile, G.; De Giglio, O.; Montagna, M.T. Mold contamination in a con-trolled hospital environment: A 3-year surveillance in southern Italy. BMC Infect. Dis. 2014, 14, 595. [Google Scholar] [CrossRef] [Green Version]
- Pasquarella, C.; Veronesi, L.; Castiglia, P.; Liguori, G.; Montagna, M.T.; Napoli, C.; Rizzetto, R.; Torre, I.; Masia, M.D.; Di Onofrio, V. Italian multicentre study on microbial environmental contamination in dental clinics: A pilot study. Sci. Total Environ. 2010, 408, 4045–4051. [Google Scholar] [CrossRef]
- Iatta, R.; Napoli, C.; Borghi, E.; Montagna, M.T. Rare mycoses of the oral cavity: A literature epidemiologic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 647–655. [Google Scholar] [CrossRef]
- Aghili, M.; Kasturirangan, M.N. A clinical pharmacist-led integrated approach for evaluation of medication errors among medical intensive care unit patients. JBI Evid. Implement. 2021, 19, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Carayon, P.; Wetterneck, T.B.; Cartmill, R.; Blosky, M.A.; Brown, R.; Kim, R.; Kukreja, S.; Johnson, M.; Paris, B.; Wood, K.E.; et al. Characterising the complexity of medication safety using a human factors approach: An observational study in two intensive care units. BMJ Qual. Saf. 2014, 23, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Zirpe, K.G.; Seta, B.; Gholap, S.; Aurangabadi, K.; Gurav, S.K.; Deshmukh, A.M.; Wankhede, P.; Suryawanshi, P.; Vasanth, S.; Kurian, M.; et al. Incidence of Medication Error in Critical Care Unit of a Tertiary Care Hospital: Where Do We Stand? Indian J. Crit. Care Med. 2020, 24, 799. [Google Scholar] [CrossRef]
- Irajpour, A.; Farzi, S.; Saghaei, M.; Ravaghi, H. Causes of medication errors in intensive care units from the perspective of healthcare professionals. J. Res. Pharm. Pract. 2017, 6, 158–165. [Google Scholar] [CrossRef]
- Suclupe, S.; Martinez-Zapata, M.J.; Mancebo, J.; Font-Vaquer, A.; Castillo-Masa, A.M.; Viñolas, I.; Morán, I.; Robleda, G. Medication errors in prescription and administration in critically ill patients. J. Adv. Nurs. 2020, 76, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Giannetta, N.; Dionisi, S.; Villa, G.; Cappadona, R.; Fabbian, F.; De Giorgi, A.; Manara, D.F.; Di Muzio, M.; Manfredini, R.; Di Simone, E. Characteristics of registered clinical trials assessing strategies of medication errors prevention. An unusual cross sectional analysis. Acta Biomed. 2021, 92, e2021503. [Google Scholar]
- Giannetta, N.; Marson, D.; Della Donna, E.; Gaiotto, B.; Castellerin, C.; Di Simone, E.; Dionisi, S.; Di Muzio, M. Instruments to facilitate the decision-making process on how to administer infusions simultaneously in intensive care units. An Italian experience. G. Ital. Farm. Clin. 2020, 34, 62–74. [Google Scholar]
- Kaboodmehri, R.; Hasavari, F.; Adib, M.; Khaleghdoost Mohammadi, T.; Kazemnejhad Leili, E. Environmental Factors Contributing to Medication Errors in Intensive Care Units. J. Holist. Nurs. Midwifery 2019, 29, 57–64. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Aromataris, E.; Fernandez, R.; Godfrey, C.; Holly, C.; Khalil, H.; Tungpunkom, P. Chapter 10: Umbrella Reviews. In JBI Manual for Evidence Synthesis; JBI: North Adelaide, Australia, 2017. [Google Scholar]
- Prgomet, M.; Li, L.; Niazkhani, Z.; Georgiou, A.; Westbrook, J.I. Impact of commercial computerized provider order entry (CPOE) and clinical decision support systems (CDSSs) on medication errors, length of stay, and mortality in intensive care units: A systematic review and meta-analysis. J. Am. Med. Inform. Assoc. 2017, 24, 413–422. [Google Scholar] [CrossRef] [Green Version]
- Manias, E.; Williams, A.; Liew, D. Interventions to reduce medication errors in adult intensive care: A systematic review. Br. J. Clin. Pharmacol. 2012, 74, 411–423. [Google Scholar] [CrossRef] [Green Version]
- Reckmann, M.H.; Westbrook, J.I.; Koh, Y.; Lo, C.; Day, R.O. Does Computerized Provider Order Entry Reduce Prescribing Errors for Hospital Inpatients? A Systematic Review. J. Am. Med. Inform. Assoc. 2009, 16, 613–623. [Google Scholar] [CrossRef] [Green Version]
- Van Rosse, F.; Maat, B.; Rademaker, C.M.A.; van Vught, A.J.; Egberts, A.C.G.; Bollen, C.W. The Effect of Computerized Physician Order Entry on Medication Prescription Errors and Clinical Outcome in Pediatric and Intensive Care: A Systematic Review. Pediatrics 2009, 123, 1184–1190. [Google Scholar] [CrossRef]
- Rice, M.; Lear, A.; Kane-Gill, S.; Seybert, A.L.; Smithburger, P.L. Pharmacy Personnel’s Involvement in Transitions of Care of Intensive Care Unit Patients: A Systematic Review. J. Pharm. Pract. 2020, 34, 117–126. [Google Scholar] [CrossRef]
- Wang, T.; Benedict, N.; Olsen, K.M.; Luan, R.; Zhu, X.; Zhou, N.; Tang, H.; Yan, Y.; Peng, Y.; Shi, L. Effect of critical care pharmacist’s intervention on medication errors: A systematic review and meta-analysis of observational studies. J. Crit. Care 2015, 30, 1101–1106. [Google Scholar] [CrossRef]
- Hunter, S.; Considine, J.; Manias, E. Nurse management of vasoactive medications in intensive care: A systematic review. J. Clin. Nurs. 2020, 29, 381–392. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 89. [Google Scholar]
- Cinotti, R.; Di Denia, P.; Sapigni, E.; Campagnoli, D. Tecnologie Informatizzate per la Sicurezza Nell’uso dei Farmaci: Sussidi per la Gestione del Rischio. 2006. Available online: http://qualitarischioclinico.asppalermo.org/documenti/riferimentibibliografici/sussidiemiliaromagna/4tecnologieinformatizzate.pdf (accessed on 10 May 2022).
- Ali, J.; Barrow, L.; Vuylsteke, A. The impact of computerised physician order entry on prescribing practices in a cardiothoracic intensive care unit. Anaesthesia 2010, 65, 119–123. [Google Scholar] [CrossRef]
- Colpaert, K.; Claus, B.; Somers, A.; Vandewoude, K.; Robays, H.; Decruyenaere, J. Impact of computerized physician order entry on medication prescription errors in the intensive care unit: A controlled cross-sectional trial. Crit. Care 2006, 10, R21. [Google Scholar] [CrossRef] [Green Version]
- Shulman, R.; Singer, M.; Goldstone, J.; Bellingan, G. Medication errors: A prospective cohort study of hand-written and computerised physician order entry in the intensive care unit. Crit. Care (Lond. Engl.) 2005, 9, R516–R521. [Google Scholar] [CrossRef] [Green Version]
- Bradley, V.M.; Steltenkamp, C.L.; Hite, K.B. Evaluation of reported medication errors before and after implementation of computerized practitioner order entry. J. Healthc. Inf. Manag. 2006, 20, 46–53. [Google Scholar] [PubMed]
- Weant, K.A.; Cook, A.M.; Armitstead, J.A. Medication-error reporting and pharmacy resident experience during implementation of computerized prescriber order entry. Am. J. Health Syst. Pharm. 2007, 64, 526–530. [Google Scholar] [CrossRef]
- Deyoung, J.L.; Vanderkooi, M.E.; Barletta, J.F. Effect of bar-code-assisted medication administration on medication error rates in an adult medical intensive care unit. Am. J. Health Pharm. 2009, 66, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- Chapuis, C.; Roustit, M.; Bal, G.; Schwebel, C.; Pansu, P.; David-Tchouda, S.; Foroni, L.; Calop, J.; Timsit, J.-F.; Allenet, B.; et al. Automated drug dispensing system reduces medication errors in an intensive care setting. Crit. Care Med. 2010, 38, 2275–2281. [Google Scholar] [CrossRef] [PubMed]
- Pronovost, P.; Weast, B.; Schwarz, M.; Wyskiel, R.M.; Prow, D.; Milanovich, S.N.; Berenholtz, S.; Dorman, T.; Lipsett, P. Medication reconciliation: A practical tool to reduce the risk of medication errors. J. Crit. Care 2003, 18, 201–205. [Google Scholar] [CrossRef]
- Ford, D.G.; Seybert, A.L.; Smithburger, P.L.; Kobulinsky, L.R.; Samosky, J.T.; Kane-Gill, S.L. Impact of simulation-based learning on medication error rates in critically ill patients. Intensive Care Med. 2010, 36, 1526–1531. [Google Scholar] [CrossRef]
- Thomas, A.N.; Boxall, E.M.; Laha, S.K.; Day, A.J.; Grundy, D. An educational and audit tool to reduce prescribing error in intensive care. Qual. Saf. Health Care 2008, 17, 360–363. [Google Scholar] [CrossRef]
- Landrigan, C.P.; Rothschild, J.M.; Cronin, J.W.; Kaushal, R.; Burdick, E.; Katz, J.T.; Lilly, C.M.; Stone, P.H.; Lockley, S.W.; Bates, D.W.; et al. Effect of Reducing Interns’ Work Hours on Serious Medical Errors in Intensive Care Units. N. Engl. J. Med. 2004, 351, 1838–1848. [Google Scholar] [CrossRef] [Green Version]
- Giusti, A.; Maggini, M.; Colaceci, S. The burden of chronic diseases across Europe: What policies and programs to address diabetes? A SWOT analysis. Health Res. Policy Syst. 2020, 18, 12–17. [Google Scholar] [CrossRef]
- Khalil, H.; Kynoch, K.; Hines, S. Interventions to ensure medication safety in acute care: An umbrella review. Int. J. Evid. Based Healthc. 2020, 18, 188–211. [Google Scholar] [CrossRef]
- Dionisi, S.; Di Muzio, M.; Giannetta, N.; Di Simone, E.; Gallina, B.; Napoli, C.; Orsi, G.B. Nursing students’ experience of risk assessment, prevention and management: A systematic review. J. Prev. Med. Hyg. 2021, 62, e122–e131. [Google Scholar] [PubMed]
- Liquori, G.; De Leo, A.; Di Simone, E.; Dionisi, S.; Giannetta, N.; Ganci, E.; Trainito, S.P.; Orsi, G.B.; Di Muzio, M.; Napoli, C. Medication Adherence in Chronic Older Patients: An Italian Observational Study Using Medication Adherence Report Scale (MARS-5I). Int. J. Environ. Res. Public Health 2022, 19, 5190. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author(s) (Year) | Title | Study Design | Number of Studies | Number of Participants | Description of Interventions | Description of Outcomes Included in the Review | Search Details | Appraisal Instrument Used | Results |
|---|---|---|---|---|---|---|---|---|---|
| Prgomet et al. (2017) [25] | Impact of commercial computerized provider order entry (CPOE) and clinical decision support systems (CDSSs) on medication errors, length of stay, and mortality in intensive care units: a systematic review and meta-analysis | Unreported | 20 | Unreported | CPOE and CDSS | Medication errors, length of stay, mortality | Medline and Embase via Ovid, and CINAHL via EBSCOhost | EPHPP quantitative tool | “The transition from paper-based ordering to commercial CPOE systems in ICUs was associated with an 85% reduction in medication prescribing error rates and a 12% reduction in ICU mortality rates. Overall meta-analyses of LOS and hospital mortality did not demonstrate a significant change.” |
| Manias et al. (2012) [26] | Interventions to reduce medication errors in adult intensive care: a systematic review | Pre-post interventional studies; prospective randomized trials; quasi-experimental designs | 24 | 25 to 8.901 | Any interventions delivered in ICUs for adult patients with the intent of reducing medication errors | Error rates | PubMed, CINAHL (Nursing and Allied Health), EMBASE, Journals@Ovid, International Pharmaceutical Abstract Series via Ovid, Science Direct, Scopus, Web of Science, PsycInfo, Cochrane Database of Systematic Reviews, and the Cochrane Central Register of Controlled Trials | Oxford Centre for Evidence-Based Medicine | “Eight types of interventions were identified: computerized physician order entry (CPOE), changes in work schedules (CWS), intravenous systems (IS), modes of education (ME), medication reconciliation (MR), pharmacist involvement (PI), protocols and guidelines (PG) and support systems for clinical decision making (SSCD). Sixteen out of the twenty-four studies showed reduced medication error rates. Four intervention types demonstrated reduced medication errors post-intervention: CWS, ME, MR and PG. It is not possible to promote any interventions as positive models for reducing medication errors. Insufficient research was undertaken with any particular type of intervention, and there were concerns regarding the level of evidence and quality of research. Most studies involved single arm, before and after designs without a comparative control group.” |
| Reckmann et al. (2009) [27] | Does Computerized Provider Order Entry Reduce Prescribing Errors for Hospital Inpatients? A Systematic Review | Cross-sectional trial; prospective pre- and poststudy; prospective study | 3 | Unreported | CPOE and CDSS | Medication prescription errors | Ovid MEDLINE, CINAHL, EMBASE, Journals@Ovid, Inspec via Ovid, International Pharmaceutical Abstract Series via Ovid, Cochrane Database of Systematic Reviews, and the Cochrane Central Register of Controlled Trials | Unreported | “Three studies investigated the impact of CPOE on the incidence of prescribing errors in adult ICU patients. One evaluated CPOE with clinical decision support and two without. Two studies found that CPOE (without clinical decision support) was associated with a significant reduction in the prescribing error rate. In one study, prescribing error rates remained unchanged for intermittent drugs and prescribing errors increased for IV fluids and infusions.” |
| van Rosse et al. (2009) [28] | The effect of computerized physician order entry on medication prescription errors and clinical outcome in pediatric and intensive care: a systematic review | Retrospective cohort; prospective cohort; controlled cross-sectional trial | 4 | Unreported | CPOE and CDSS | Medication prescription errors, adverse drug events, and mortality | PubMed, the Cochrane Library, and Embase | STROBE (observational studies) and Jadad Tool (experimental studies) | “Meta-analysis showed a significant decreased risk of medication prescription errors with use of computerized physician order entry. However, there was no significant reduction in adverse drug events or mortality rates.” |
| Rice et al. (2020) [29] | Pharmacy Personnel’s Involvement in Transitions of Care of Intensive Care Unit Patients: A Systematic Review | Prospective randomized controlled trial; prospective cohort comparison studies; a prospective study with a pre- and post-design; two-period study with a retrospective pre-implementation component; prospective postimplementation component; retrospective investigations | 10 | Unreported | Pharmacist-led intervention | Medication errors, continuation of inappropriate therapies, and interventions on transfer into or out of the ICU | MEDLINE and Embase | Unreported | “A significant improvement was demonstrated with pharmacy-driven intervention in all 4 studies that evaluated the entire ICU patient population. Interventions specific to certain medication and disease improved medication safety measures but were not always statistically significant. Medication error rates are high in patients transferred into and out of the ICU, and limited data exist to address this concern.” |
| Wang et al. (2015) [30] | Effect of critical care pharmacist’s intervention on medication errors: A systematic review and meta-analysis of observational studies | Non-randomized controlled studies: controlled before and after | 8 | Unreported | Pharmacist-led intervention | Medication error rates, adverse drug events | MEDLINE, Embase, and Cochrane | Quality Assessment Tool for Before and After (Pre- and Post-) Studies With No Control Group (NIH) | “Results suggest that pharmacist intervention has no significant contribution to reducing general MEs, although pharmacist intervention may significantly reduce preventable adverse drug events and prescribing errors.” |
| Hunter et al. (2019) [31] | Nurse management of vasoactive medications in intensive care: A systematic review | Observational studies; pre- and post-intervention studies; survey studies; quasi-experimental studies; longitudinal time series; prospective controlled trials; and interviews incorporating content analysis | 13 | Unreported | Medication education | Risk of medication errors | CINAHL Complete, Medline Complete, and EMBASE | Critical Appraisal Skills Program (CASP) Appraisal Tool for Qualitative Research was used to assess quality | “These four studies indicated that providing education and standardisation of practices could support nursing practice on the preparation of vasoactive infusions and reduce risk for medication errors” |
| Studies | Prgomet et al. (2017) [25] | Manias et al. (2012) [26] | Reckmann et al. (2009) [27] | van Rosse et al. (2009) [28] |
|---|---|---|---|---|
| Evans et al. (1998a) * | ✓ | ✓ | ||
| Thompson et al. (2004) * | ✓ | |||
| Shulman et al. (2005) * | ✓ | ✓ | ✓ | ✓ |
| Bradley et al. (2006) * | ✓ | |||
| Colpaert et al. (2006) * | ✓ | ✓ | ✓ | ✓ |
| Weant et al. (2007) * | ✓ | ✓ | ||
| Carayon et al. (2009) * | ✓ | |||
| Ali et al. (2010) * | ✓ | ✓ | ||
| Armada et al. (2014) * | ✓ |
| Studies included | Prgomet et al. (2017) [25] | Manias et al. (2012) [26] |
|---|---|---|
| Barcode technology | ||
| DeYoung et al. (2009) * | ✓ | |
| Automatized systems for the distribution of medication | ||
| Chapuis et al. (2010) * | ✓ | |
| Technological systems for endovenous infusions | ||
| Rothschild et al. (2005) * | ✓ | |
| Nuckols et al. (2008) * | ✓ | |
| Support systems for clinical decisions | ||
| Evans et al. (1998b) * | ✓ | |
| Evans et al. (1999) * | ✓ | |
| Fernández Pérez et al. (2007) * | ✓ | |
| Fraenkel et al. (2003) * | ✓ | |
| Rana et al. (2006) * | ✓ | |
| Studies | Manias et al. (2012) [26] | Wang et al. (2015) [30] | Hunter et al. (2019) [31] |
|---|---|---|---|
| Herout et al. (2004) * | ✓ | ||
| Thomas et al. (2008) * | ✓ | ||
| Ford et al. (2010) * | ✓ | ||
| Alagha et al. (2011) * | ✓ | ||
| Jung et al. (2014) * | ✓ | ||
| Nguyen et al. (2014) * | ✓ | ||
| Melo et al. (2016) * | ✓ | ||
| Tan et al. (2017) * | ✓ |
| Studies | Manias et al. (2012) [26] | Rice et al. (2020) [29] | Wang et al. (2015) [30] |
|---|---|---|---|
| Medication reconciliation | |||
| Pronovost et al. (2003) * | ✓ | ||
| Zeigler et al. (2008) * | ✓ | ||
| Hatch et al. (2010) * | ✓ | ||
| Coutsouvelis et al. (2010) * | ✓ | ||
| Hatch et al. (2011) * | ✓ | ||
| Pavlov et al. (2014) * | ✓ | ||
| Heselmans et al. (2015) * | ✓ | ||
| Wills et al. (2016) * | ✓ | ||
| Bosma et al. (2018) * | ✓ | ||
| Wohlt et al. (2007) * | ✓ | ||
| D’Angelo et al. (2019) * | ✓ | ||
| Pharmacist in the ward | |||
| Leape et al. (1999) * | ✓ | ✓ | |
| Lee et al. (2007) * | ✓ | ✓ | |
| Kaushal et al. (2008) * | ✓ | ||
| Klopotowska et al. (2010) * | ✓ | ✓ | |
| Langebrake et al. (2010) * | ✓ | ||
| Alagha et al. (2011) * | ✓ | ||
| Jiang et al. (2012) * | ✓ | ||
| Studies | Manias et al. (2012) [26] |
|---|---|
| Work organization | |
| Landrigan et al. (2004) * | ✓ |
| Protocols and guidelines | |
| Wasserfallen et al. (2004) * | ✓ |
| McMullin et al. (2006) * | ✓ |
| Bertsche et al. (2008) * | ✓ |
| Authors (year) | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Prgomet et al. (2017) [25] | Y | Y | Y | N | Y | U | Y | Y | Y | U | Y |
| Manias et al. (2012) [26] | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y |
| Reckmann et al. (2009) [27] | Y | Y | U | Y | U | Y | U | U | N | Y | Y |
| van Rosse et al. (2009) [28] | Y | Y | Y | N | Y | U | U | Y | N | Y | Y |
| Rice et al. (2020) [29] | Y | Y | Y | N | U | U | Y | Y | U | Y | Y |
| Wang et al. (2015) [30] | Y | Y | Y | N | Y | Y | U | Y | Y | Y | Y |
| Hunter et al. (2019) [31] | Y | Y | Y | N | Y | Y | Y | Y | U | Y | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dionisi, S.; Giannetta, N.; Liquori, G.; De Leo, A.; D’Inzeo, V.; Orsi, G.B.; Di Muzio, M.; Napoli, C.; Di Simone, E. Medication Errors in Intensive Care Units: An Umbrella Review of Control Measures. Healthcare 2022, 10, 1221. https://doi.org/10.3390/healthcare10071221
Dionisi S, Giannetta N, Liquori G, De Leo A, D’Inzeo V, Orsi GB, Di Muzio M, Napoli C, Di Simone E. Medication Errors in Intensive Care Units: An Umbrella Review of Control Measures. Healthcare. 2022; 10(7):1221. https://doi.org/10.3390/healthcare10071221
Chicago/Turabian StyleDionisi, Sara, Noemi Giannetta, Gloria Liquori, Aurora De Leo, Victoria D’Inzeo, Giovanni Battista Orsi, Marco Di Muzio, Christian Napoli, and Emanuele Di Simone. 2022. "Medication Errors in Intensive Care Units: An Umbrella Review of Control Measures" Healthcare 10, no. 7: 1221. https://doi.org/10.3390/healthcare10071221