
Efficacy of Acupuncture, Intravenous Lidocaine, and Diet in the Management of Patients with Fibromyalgia: A Systematic Review and Network Meta-Analysis

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Literature Search
2.3. Eligibility Criteria and Study Selection
2.4. Data Extraction
2.5. Outcomes’ Scales
2.6. Risk of Bias
2.7. Data Synthesis
3. Results
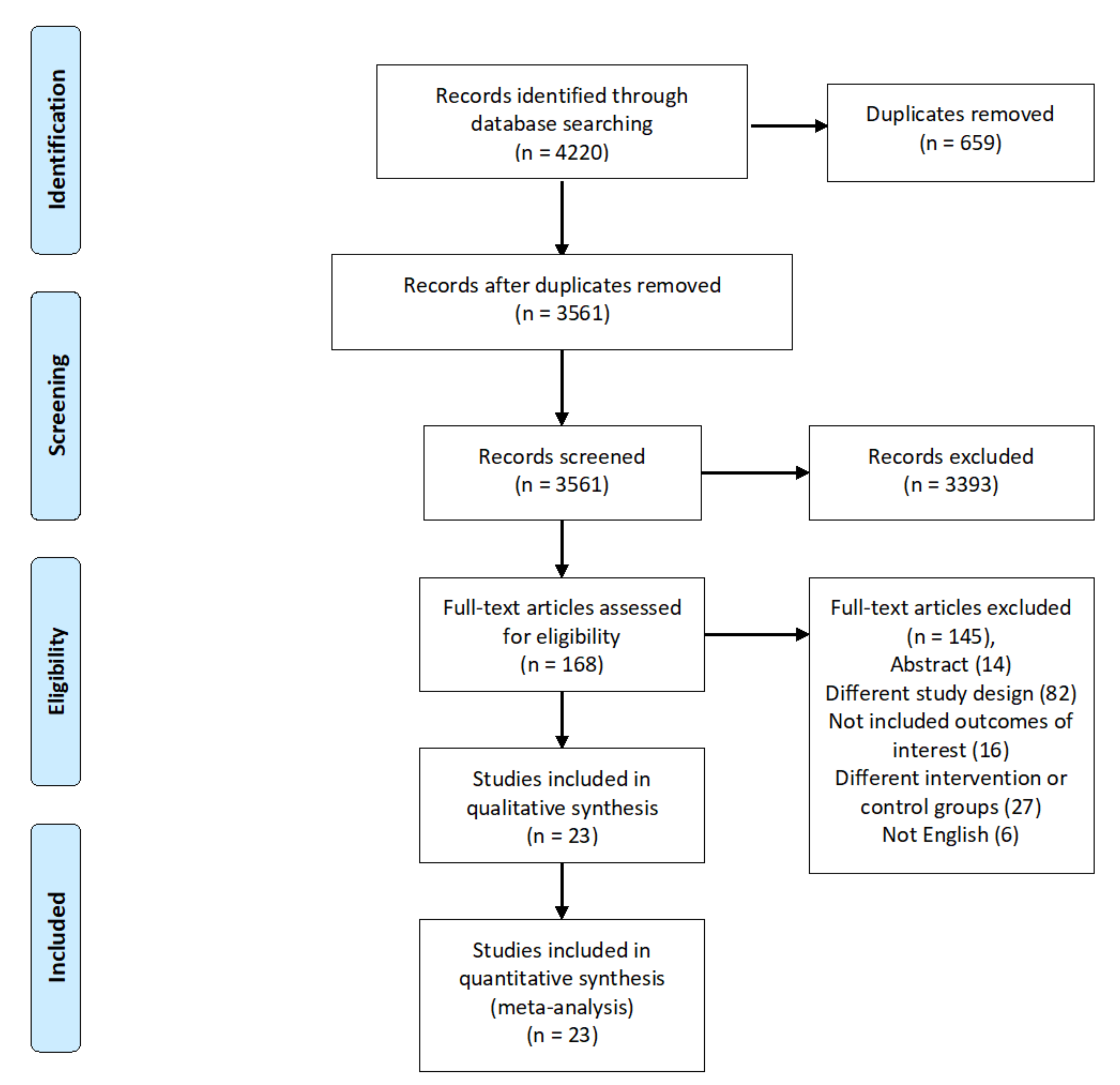
3.1. Literature Search
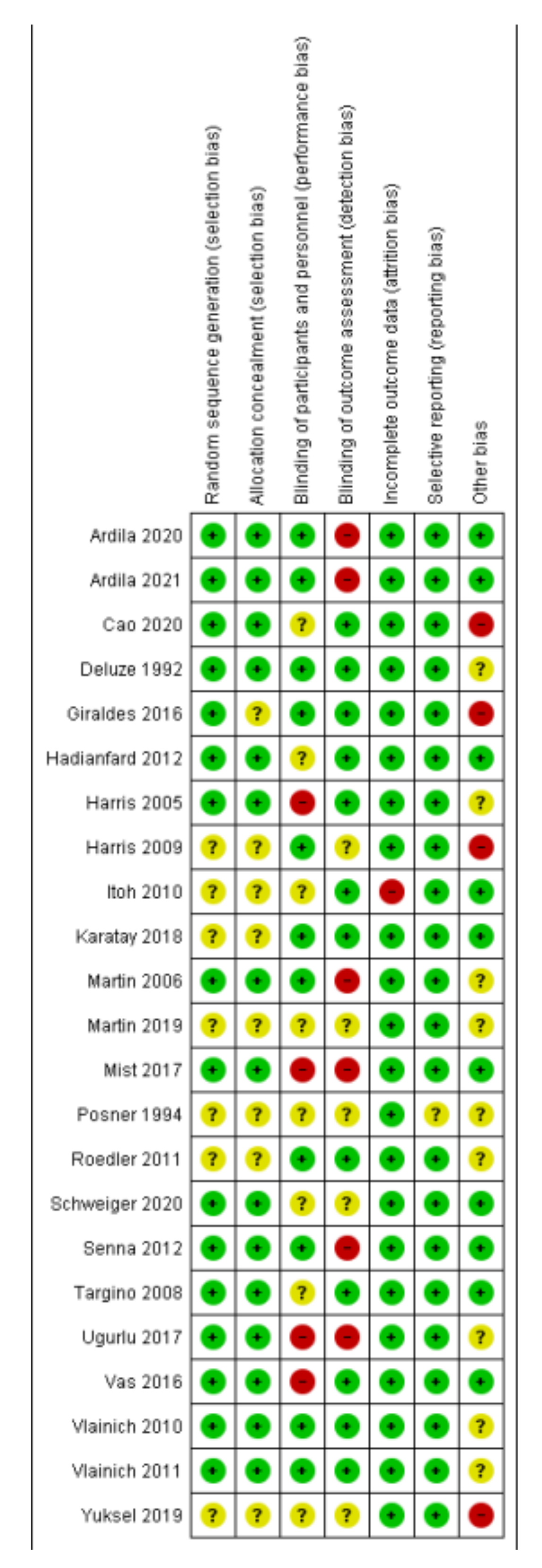
3.2. Risk of Bias
3.3. Outcomes
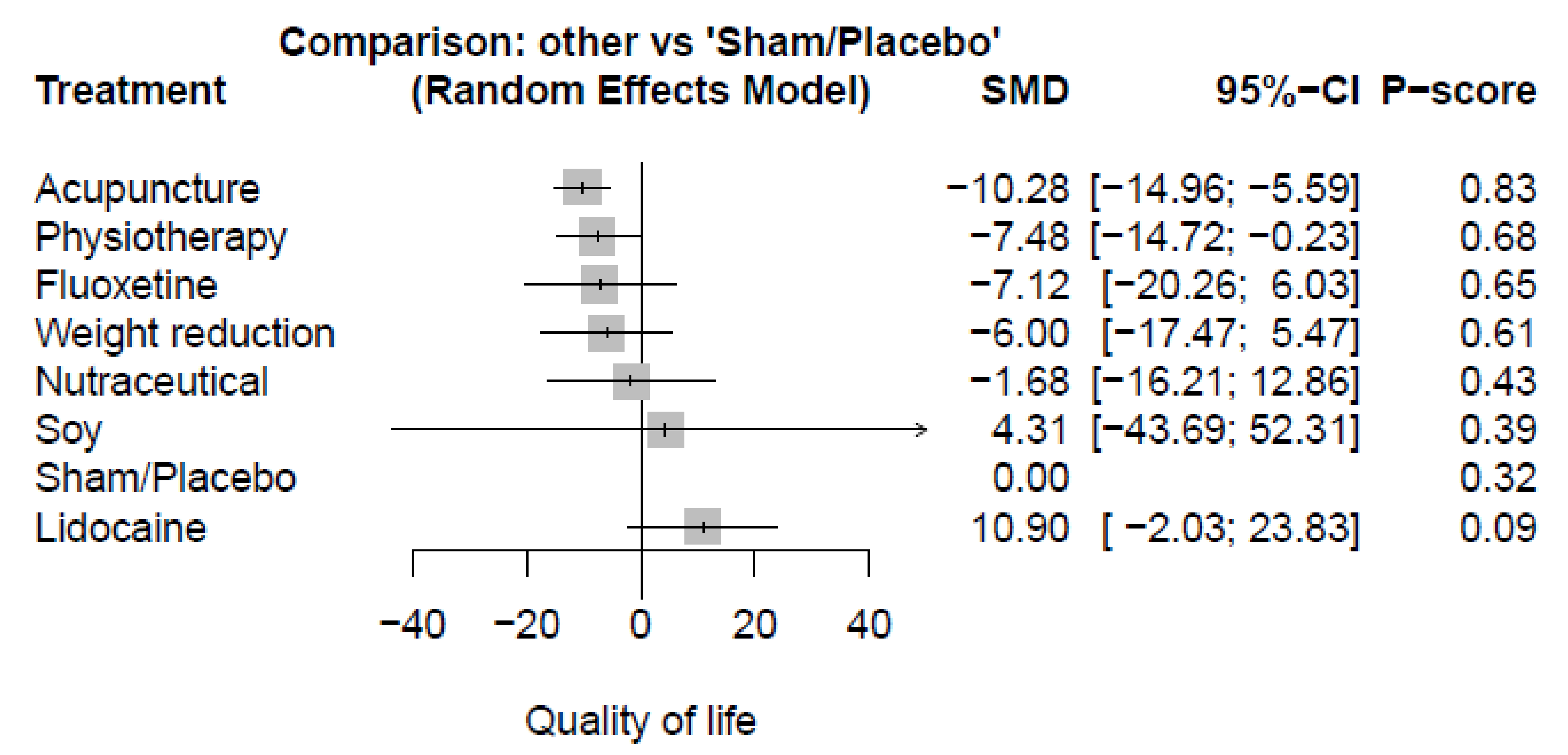
3.3.1. Quality of Life (QoL)
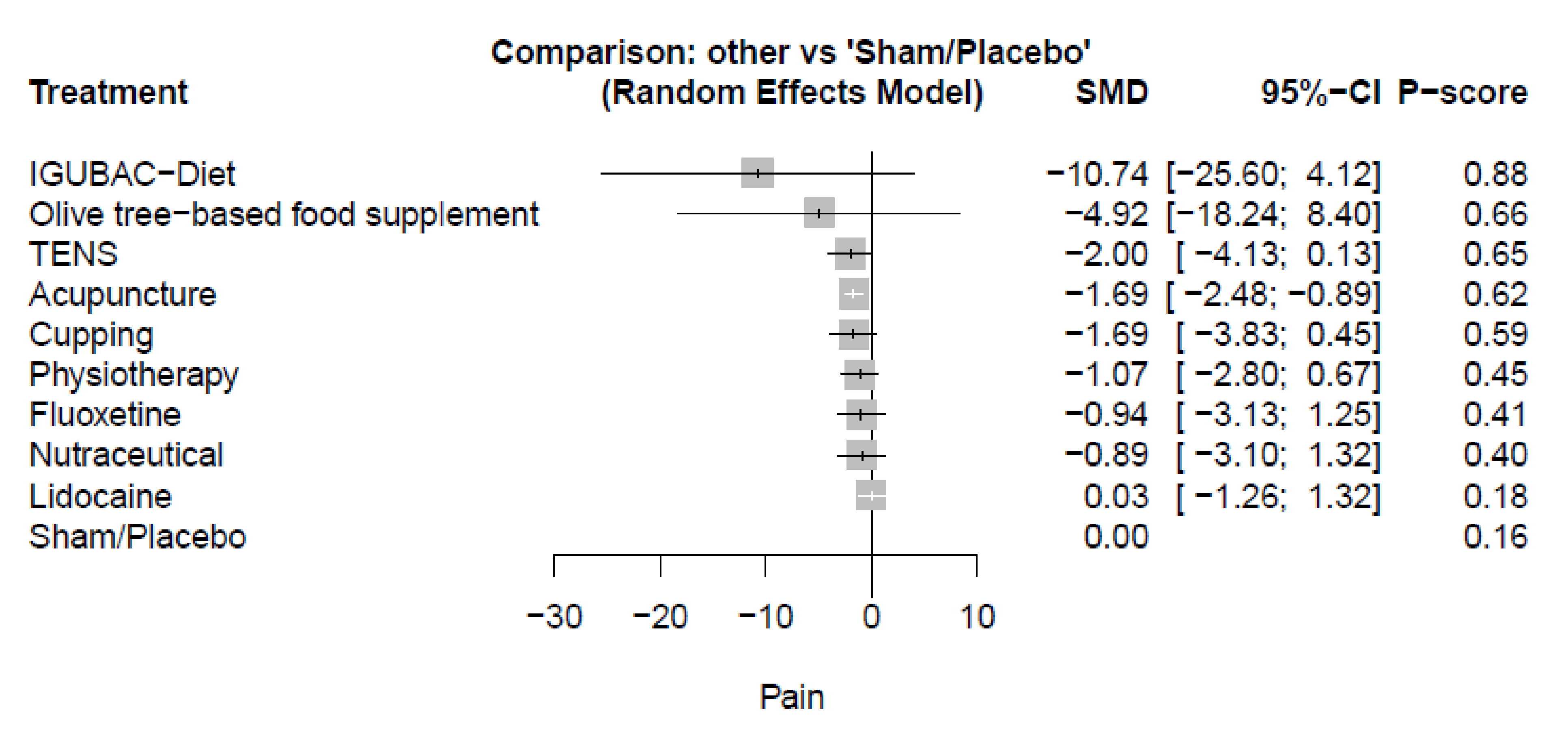
3.3.2. Pain
3.3.3. Depression
3.3.4. Stiffness
3.4. Heterogeneity
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. The Full Search Strategy of Databases
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, D.L. Fibromyalgia syndrome. An emerging but controversial condition. JAMA 1987, 257, 2782–2787. [Google Scholar] [CrossRef]
- Rivera, J.; Alegre, C.; Ballina, F.J.; Carbonell, J.; Carmona, L.; Castel, B.; Collado, A.; Esteve, J.J.; Martínez, F.G.; Tornero, J.; et al. Documento de consenso de la Sociedad Española de Reumatología sobre la fibromialgia. Reumatol. Clin. 2006, 2 (Suppl. 1), S55–S66. [Google Scholar] [CrossRef]
- Garrido-Ardila, E.M.; González-López-Arza, M.V.; Jiménez-Palomares, M.; García-Nogales, A.; Rodríguez-Mansilla, J. Effectiveness of acupuncture vs. core stability training in balance and functional capacity of women with fibromyalgia: A randomized controlled trial. Clin. Rehabil. 2020, 34, 630–645. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.D.; Horak, F.B.; Winters-Stone, K.; Irvine, J.M.; Bennett, R.M. Fibromyalgia is associated with impaired balance and falls. J. Clin. Rheumatol. Pract. Rep. Rheum. Musculoskelet. Dis. 2009, 15, 16–21. [Google Scholar] [CrossRef]
- Arnold, L.M.; Crofford, L.J.; Mease, P.J.; Burgess, S.M.; Palmer, S.C.; Abetz, L.; Martin, S.A. Patient perspectives on the impact of fibromyalgia. Patient Educ. Couns. 2008, 73, 114–120. [Google Scholar] [CrossRef]
- Henriksson, C.M.; Liedberg, G.M.; Gerdle, B. Women with fibromyalgia: Work and rehabilitation. Disabil. Rehabil. 2005, 27, 685–694. [Google Scholar] [CrossRef]
- Jones, J.; Rutledge, D.N.; Jones, K.D.; Matallana, L.; Rooks, D.S. Self-assessed physical function levels of women with fibromyalgia: A national survey. Womens Health Issues 2008, 18, 406–412. [Google Scholar] [CrossRef]
- Wolfe, F.; Anderson, J.; Harkness, D.; Bennett, R.M.; Caro, X.J.; Goldenberg, D.L.; Russell, I.J.; Yunus, M.B. Work and disability status of persons with fibromyalgia. J. Rheumatol. 1997, 24, 1171–1178. [Google Scholar]
- Ablin, J.; Fitzcharles, M.A.; Buskila, D.; Shir, Y.; Sommer, C.; Häuser, W. Treatment of fibromyalgia syndrome: Recommendations of recent evidence-based interdisciplinary guidelines with special emphasis on complementary and alternative therapies. Evid.-Based Complement. Altern. Med. 2013, 2013, 485272. [Google Scholar] [CrossRef] [PubMed]
- Deare, J.C.; Zheng, Z.; Xue, C.C.; Liu, J.P.; Shang, J.; Scott, S.W.; Littlejohn, G. Acupuncture for treating fibromyalgia. Cochrane Database Syst. Rev. 2013, 2013, Cd007070. [Google Scholar] [CrossRef] [PubMed]
- Langhorst, J.; Klose, P.; Musial, F.; Irnich, D.; Häuser, W. Efficacy of acupuncture in fibromyalgia syndrome—A systematic review with a meta-analysis of controlled clinical trials. Rheumatology 2010, 49, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Wang, W.T.; Yang, T.H.; Liou, T.H.; Chen, G.Y.; Lin, L.F. The balance effect of acupuncture therapy among stroke patients. J. Altern. Complement. Med. 2014, 20, 618–622. [Google Scholar] [CrossRef]
- Sautreuil, P.; Piquemal, M.; Thoumie, P.; Dib, M.; Mailhan, L.; Cobos Romana, R.; Lassaux, A. Sclérose en plaques et neuro-acupuncture. Acupunct. Moxibustion 2011, 10, 40–47. [Google Scholar]
- Lauder, G.R. A review of intravenous lidocaine infusion therapy for paediatric acute and chronic pain management. In Pain Relief–from Analgesics to Alternative Therapies; INTECH: London, UK, 2017; pp. 63–109. [Google Scholar]
- van der Wal, S.E.; van den Heuvel, S.A.; Radema, S.A.; van Berkum, B.F.; Vaneker, M.; Steegers, M.A.; Scheffer, G.J.; Vissers, K.C. The in vitro mechanisms and in vivo efficacy of intravenous lidocaine on the neuroinflammatory response in acute and chronic pain. Eur. J. Pain 2016, 20, 655–674. [Google Scholar] [CrossRef]
- Wilderman, I.; Pugacheva, O.; Perelman, V.S.; Wansbrough, M.C.T.; Voznyak, Y.; Zolnierczyk, L. Repeated Intravenous Lidocaine Infusions for Patients with Fibromyalgia: Higher Doses of Lidocaine Have a Stronger and Longer-Lasting Effect on Pain Reduction. Pain Med. 2020, 21, 1230–1239. [Google Scholar] [CrossRef]
- Haddad, H.W.; Mallepalli, N.R.; Scheinuk, J.E.; Bhargava, P.; Cornett, E.M.; Urits, I.; Kaye, A.D. The Role of Nutrient Supplementation in the Management of Chronic Pain in Fibromyalgia: A Narrative Review. Pain Ther. 2021, 10, 827–848. [Google Scholar] [CrossRef]
- Gill, H.; Perez, C.D.; Gill, B.; El-Halabi, S.; Lee, Y.; Lipsitz, O.; Park, C.; Mansur, R.B.; Rodrigues, N.B.; McIntyre, R.S.; et al. The Prevalence of Suicidal Behaviour in Fibromyalgia Patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 108, 110078. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Monterde, S.; Salvat, I.; Montull, S.; Fernández-Ballart, J. Validación de la versión española del Fibromyalgia Impact Questionnaire. Rev. Esp. Reumatol. 2004, 31, 507–513. [Google Scholar]
- Ware, J.E.J.; Snow, K.; Kosinski, M.; Gandek, B. SF-36 Health Survey Manual and Interprestation Guide; Quality-Metric, Inc.: Lincoln, RI, USA, 2000. [Google Scholar]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. 11), S240–S252. [Google Scholar]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in psychiatric outpatients. J. Personal. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Ramos-Brieva, J.; Cordero-Villafafila, A. A new validation of the Hamilton Rating Scale for Depression. J. Psychiatr. Res. 1988, 22, 21–28. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Yüksel, M.; Ayaş, Ş.; Cabıoğlu, M.T.; Yılmaz, D.; Cabıoğlu, C. Quantitative Data for Transcutaneous Electrical Nerve Stimulation and Acupuncture Effectiveness in Treatment of Fibromyalgia Syndrome. Evid.-Based Complement. Altern. Med. 2019, 2019, 9684649. [Google Scholar] [CrossRef]
- Vlainich, R.; Issy, A.M.; Sakata, R.K. Effect of intravenous lidocaine associated with amitriptyline on pain relief and plasma serotonin, norepinephrine, and dopamine concentrations in fibromyalgia. Clin. J. Pain 2011, 27, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Vlainich, R.; Issy, A.M.; Gerola, L.R.; Sakata, R.K. Effect of intravenous lidocaine on manifestations of fibromyalgia. Pain Pract. Off. J. World Inst. Pain 2010, 10, 301–305. [Google Scholar] [CrossRef]
- Vas, J.; Santos-Rey, K.; Navarro-Pablo, R.; Modesto, M.; Aguilar, I.; Campos, M.; Aguilar-Velasco, J.F.; Romero, M.; Párraga, P.; Hervás, V.; et al. Acupuncture for fibromyalgia in primary care: A randomised controlled trial. Acupunct. Med. J. Br. Med. Acupunct. Soc. 2016, 34, 257–266. [Google Scholar]
- Uğurlu, F.G.; Sezer, N.; Aktekin, L.; Fidan, F.; Tok, F.; Akkuş, S. The effects of acupuncture versus sham acupuncture in the treatment of fibromyalgia: A randomized controlled clinical trial. Acta Reumatol. Port. 2017, 42, 32–37. [Google Scholar] [PubMed]
- Targino, R.A.; Imamura, M.; Kaziyama, H.H.; Souza, L.P.; Hsing, W.T.; Furlan, A.D.; Imamura, S.T.; Azevedo Neto, R.S. A randomized controlled trial of acupuncture added to usual treatment for fibromyalgia. J. Rehabil. Med. 2008, 40, 582–588. [Google Scholar] [CrossRef]
- Senna, M.K.; Sallam, R.A.; Ashour, H.S.; Elarman, M. Effect of weight reduction on the quality of life in obese patients with fibromyalgia syndrome: A randomized controlled trial. Clin. Rheumatol. 2012, 31, 1591–1597. [Google Scholar] [CrossRef]
- Schweiger, V.; Secchettin, E.; Castellani, C.; Martini, A.; Mazzocchi, E.; Picelli, A.; Polati, E.; Donadello, K.; Valenti, M.T.; Dalle Carbonare, L. Comparison between Acupuncture and Nutraceutical Treatment with Migratens(®) in Patients with Fibromyalgia Syndrome: A Prospective Randomized Clinical Trial. Nutrients 2020, 12, 821. [Google Scholar] [CrossRef]
- Wahner-Roedler, D.L.; Thompson, J.M.; Luedtke, C.A.; King, S.M.; Cha, S.S.; Elkin, P.L.; Bruce, B.K.; Townsend, C.O.; Bergeson, J.R.; Eickhoff, A.L.; et al. Dietary soy supplement on fibromyalgia symptoms: A randomized, double-blind, placebo-controlled, early phase trial. Evid.-Based Complement. Altern. Med. 2011, 2011, 350697. [Google Scholar] [CrossRef] [PubMed]
- Posner, I.A. Treatment of Fibromyalgia Syndrome with Intravenous Lidocaine. J. Musculoskelet. Pain 1994, 2, 55–65. [Google Scholar] [CrossRef]
- Mist, S.D.; Jones, K.D. Randomized Controlled Trial of Acupuncture for Women with Fibromyalgia: Group Acupuncture with Traditional Chinese Medicine Diagnosis-Based Point Selection. Pain Med. 2018, 19, 1862–1871. [Google Scholar] [CrossRef]
- San Mauro, I.; Luis, C.-Y.; Sanz Rojo, S.; Sara, L.-O.; Raquel, C.; Ana, M.P.; Elena, G.-V. Short-Time Strategy for Fibromyalgia Treatment Based on Olive Nutraceutical and Inflammatory Gut-Brain Axis Control Diet (IGUBAC) Diet®. Curr. Top. Nutraceutical Res. 2018, 17, 23–32. [Google Scholar]
- Martin, D.P.; Sletten, C.D.; Williams, B.A.; Berger, I.H. Improvement in fibromyalgia symptoms with acupuncture: Results of a randomized controlled trial. Mayo Clin. Proc. 2006, 81, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Karatay, S.; Okur, S.C.; Uzkeser, H.; Yildirim, K.; Akcay, F. Effects of Acupuncture Treatment on Fibromyalgia Symptoms, Serotonin, and Substance P Levels: A Randomized Sham and Placebo-Controlled Clinical Trial. Pain Med. 2018, 19, 615–628. [Google Scholar] [CrossRef] [PubMed]
- Itoh, K.; Kitakoji, H. Effects of acupuncture to treat fibromyalgia: A preliminary randomised controlled trial. Chin. Med. 2010, 5, 11. [Google Scholar] [CrossRef]
- Harris, R.E.; Zubieta, J.K.; Scott, D.J.; Napadow, V.; Gracely, R.H.; Clauw, D.J. Traditional Chinese acupuncture and placebo (sham) acupuncture are differentiated by their effects on mu-opioid receptors (MORs). NeuroImage 2009, 47, 1077–1085. [Google Scholar] [CrossRef]
- Deluze, C.; Bosia, L.; Zirbs, A.; Chantraine, A.; Vischer, T.L. Electroacupuncture in fibromyalgia: Results of a controlled trial. BMJ 1992, 305, 1249–1252. [Google Scholar] [CrossRef]
- Mayhew, E.; Ernst, E. Acupuncture for fibromyalgia—A systematic review of randomized clinical trials. Rheumatology 2007, 46, 801–804. [Google Scholar] [CrossRef]
- Martin-Sanchez, E.; Torralba, E.; Díaz-Domínguez, E.; Barriga, A.; Martin, J.L. Efficacy of acupuncture for the treatment of fibromyalgia: Systematic review and meta-analysis of randomized trials. Open Rheumatol. J. 2009, 3, 25–29. [Google Scholar] [CrossRef]
- Yang, B.; Yi, G.; Hong, W.; Bo, C.; Wang, Z.; Liu, Y.; Xue, Z.; Li, Y. Efficacy of acupuncture on fibromyalgia syndrome: A meta-analysis. J. Tradit. Chin. Med. 2014, 34, 381–391. [Google Scholar]
- Colquhoun, D.; Novella, S.P. Acupuncture Is Theatrical Placebo. Anesth. Analg. 2013, 116, 1360–1363. [Google Scholar] [CrossRef]
- Zhang, X.C.; Chen, H.; Xu, W.T.; Song, Y.Y.; Gu, Y.H.; Ni, G.X. Acupuncture therapy for fibromyalgia: A systematic review and meta-analysis of randomized controlled trials. J. Pain Res. 2019, 12, 527–542. [Google Scholar] [CrossRef] [PubMed]
- Coutaux, A. Non-pharmacological treatments for pain relief: TENS and acupuncture. Jt. Bone Spine 2017, 84, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Ondrejkovicova, A.; Petrovics, G.; Svitkova, K.; Bajtekova, B.; Bangha, O. Why acupuncture in pain treatment? Neuro Endocrinol. Lett. 2016, 37, 163–168. [Google Scholar] [PubMed]
- Tang, Y.; Yin, H.Y.; Rubini, P.; Illes, P. Acupuncture-Induced Analgesia: A Neurobiological Basis in Purinergic Signaling. Neuroscientist 2016, 22, 563–578. [Google Scholar] [CrossRef]
- Silva, A.R.; Bernardo, A.; Costa, J.; Cardoso, A.; Santos, P.; de Mesquita, M.F.; Vaz Patto, J.; Moreira, P.; Silva, M.L.; Padrão, P. Dietary interventions in fibromyalgia: A systematic review. Ann. Med. 2019, 51 (Suppl. 1), 2–14. [Google Scholar] [CrossRef]
- Nadal-Nicolás, Y.; Miralles-Amorós, L.; Martínez-Olcina, M.; Sánchez-Ortega, M.; Mora, J.; Martínez-Rodríguez, A. Vegetarian and Vegan Diet in Fibromyalgia: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4955. [Google Scholar] [CrossRef]
- Pagliai, G.; Giangrandi, I.; Dinu, M.; Sofi, F.; Colombini, B. Nutritional Interventions in the Management of Fibromyalgia Syndrome. Nutrients 2020, 12, 2525. [Google Scholar] [CrossRef]
- Albertoni Giraldes, A.L.; Salomão, R.; Leal, P.D.; Brunialti, M.K.; Sakata, R.K. Effect of intravenous lidocaine combined with amitriptyline on pain intensity, clinical manifestations and the concentrations of IL-1, IL-6 and IL-8 in patients with fibromyalgia: A randomized double-blind study. Int. J. Rheum. Dis. 2016, 19, 946–953. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Country | Diagnostic Criteria | Duration (Month) | Interventions | Sample Size | Age | Female | Weight | BMI | Years of Diagnosis | FIQ | BDI | VAS (mm, Mean, SD) | Fibromyalgia Severity Scale | Number of Tender Points (TPN) | Acupuncture Site |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ardila 2020 | Spain | NR | 12 | Acupuncture | 34 | 56.15 (7.90) | 34 (100) | NR | NR | 8.59 (5.18) | 4.31 (2.40) | NR | NR | NR | NR | GV20 (Baihui 百会): Highest point in the head, in the mid-point of the line connecting the apexes of the two auricles; Bilateral ST36 (Zusanli 足 三 里): On the anterior aspect of the lower leg, 3cun below the inferior edge of the patella, and 1cun from the anterior crest of the tibia; Bilateral BL60 (Kunlun 昆仑): On the foot, behind the external malleolus, in the depression between the tip of the external malleolus, and the calcaneus tendon. |
| Physiotherapy | 36 | 56.06 (8.37) | 36 (100) | 8.03 (6.30) | 4.37 (1.97) | |||||||||||
| Sham | 33 | 54.39 (8.20) | 33 (100) | 8.30 (4.54) | 4.20 (1.81) | |||||||||||
| Ardila 2021 | Spain | NR | 12 | Acupuncture | 34 | 56.15 (7.90) | 34 (100) | NR | NR | 8.59 (5.18) | 68.97 (16.98) | NR | 7.12 (2.04) | NR | NR | GV20, ST36, and BL60 |
| Physiotherapy | 36 | 56.06 (8.37) | 36 (100) | 8.03 (6.30) | 70 (17.46) | 7.19 (2.1) | ||||||||||
| Sham | 33 | 54.39 (8.20) | 33 (100) | 8.30 (4.54) | 64.42 (15.03) | 7.15 (2.06) | ||||||||||
| Cao 2020 | China | ACR criteria (2010) | 8 | Randomized acupuncture | 30 | 54.5 (2) * | 22 (72.4) | 64.6 (11.7) | NR | NR | 29.3 (14.8) * | NR | 66 (15.9) | NR | NR | Ashi (tender) points |
| Randomized cupping | 30 | 53 (16) * | 23 (75.9) | 64.2 (10.6) | 40.2 (20.2) * | 73 (14) | ||||||||||
| Deluze 1992 | Switzerland | ACR criteria (1990) | NR | Acupuncture | 36 | 46.8 (2.3) | 3 (8.4) | NR | NR | 14.4 (3.7) | NR | NR | 56.61 (3.19) | NR | NR | Four common points: the first dorsal interosseous muscle of the hand and the anterior tibial muscle on both sides. Others: Based on the patient’s symptoms and pain and the empirical efficacy of the sites in the treatment of pain |
| Sham | 34 | 49 (2) | 13 (38.3) | 6.9 (1.3) | 60.89 (4.07) | |||||||||||
| Giraldes 2016 | Brazil | ACR criteria (1990) | 2 | Lidocaine | 21 | 42.4 (9.4) | 19 (90.5) | 69.8 (13.8) | 25 (4.6) | 5 (4.2) | 65.1 (11.2) | NR | NR | NR | 15.2 (2.5) | NA |
| Placebo | 21 | 47 (9.8) | 21 (100) | 65.2 (10.1) | 24.2 (3.5) | 6 (4.1) | 63.5 (15.4) | 15.1 (2.9) | ||||||||
| Hadianfard 2012 | Iran | ACR criteria (1990) | 12 | Acupuncture | 15 | 43.86 (7.9) | 15 (100) | NR | NR | 6.9 (5.7) | 38.1 (12.1) | NR | 7.5 (1.8) | NR | 15.8 (2.1) | ST-36, GB-34, RN-6, SP-6, LI-4, ST-44, BL-40, HT-7, and DU-20 |
| Fluoxetine | 15 | 44.2 (10.8) | 15 (100) | 6.6 (5.8) | 42.7 (9.6) | 7.5 (1.8) | 15.5 (2.1) | |||||||||
| Harris 2005 | USA | ACR criteria (1990) | 3.5 | Acupuncture | 30 | 44.5 (10.9) | 27 (90) | NR | NR | 5.26 (4.83) | NR | NR | NR | NR | NR | Du 20, LI 11, LI 4, GB 34, bi-lateral St 36, Sp 6, Liv 3, and Ear-Shenmen |
| Sham | 27 | 48.1 (10.9) | 26 (96.3) | 5.77 (4.10) | ||||||||||||
| Harris 2009 | USA | ACR criteria (1990) | 1 | Acupuncture | 10 | 44.3 (13.6) | 10 | NR | NR | NR | NR | NR | NR | NR | NR | Du20, ear Shenmen, LI4, LI11, Sp6, Liv3, GB34, and bilateral St36 |
| Sham | 10 | 10 | ||||||||||||||
| Itoh 2010 | Japan | ACR criteria (1990) | 2.3 | Acupuncture | 6 | 47.3 (13.3) | NR | NR | NR | 4.4 (2.3) | 66.3 (11.0) | NR | 77.9 (10.1) | NR | NR | Four common acupuncture points, and up to ten additional sites depending on the patient’s symptoms and pain pattern and the empirical choice of trigger point in pain treatment |
| Sham | 7 | 45.7 (15.2) | 3.9 (3.9) | 64.3 (6.4) | 74.2 (8.4) | |||||||||||
| Karatay 2018 | Turkey | ACR criteria (1990) | 3 | Acupuncture | 24 | 34.7 (6.09) | NR | NR | 26.49 (5.65) | 4.44 (3.99) | 70.8 (12.5) | 37.6 (18.8) | 8.10 (2.52) | NR | 15.9 (2.8) | Du-14 (DaZhui), Si-15 (Jian Zhong Shu), Li-4 (He Gu), Li-11 (QuChi), H-7 (Shen Men), P-6 (Nei Guan), Ren-6 (Qihai), Liv-3 (Tai Chong), St-36 (Zu San Li), and Sp-6 (San Yin Jiao). All were bilateral, apart from Du-14 and Ren-6 |
| Sham | 25 | 34.2 (6.84) | 26.94 (4.63) | 3.94 (3.30) | 65.8 (24.1) | 36.6 (16.7) | 7.73 (1.98) | 15.9 (2.4) | ||||||||
| Martin 2006 | Georgia | ACR criteria (1990) | 7 | Acupuncture | 25 | 51.7 (14.1) | 25 (100) | NR | NR | NR | 42.4 (11) | NR | NR | 40.4 (10.3) | NR | Bilateral points at large intestine 4, stomach 36, liver 2, spleen 6, pericardium 6, and heart 7. Others: Axial paramedian points along the bladder meridian at the cervical spine during the first 3 sessions |
| Sham | 24 | 47.9 (11.2) | 23 (95.9) | 44 (9.8) | 43.0 (7.7) | |||||||||||
| Martin 2019 | Spain | NR | 2 | IGUBAC Diet | 8 | 62.1 (7.8) | 8 (100) | 64.9 (5.9) | 26.1 (3.6) | NR | NR | NR | NR | NR | NR | NA |
| Placebo | 14 | 55.9 (11.9) | 14 (100) | 67.7 (10.6) | 26.8 (4.16) | |||||||||||
| Mist 2017 | USA | ACR criteria (1990) | 6 | Acupuncture | 16 | 52.3 (12.9) | 16 (100) | NR | 33.2 (10.2) | NR | 51.1 (15.9) | NR | 6.2 (1.8) | NR | NR | Depends on a combination of TCM Syndrome diagnosis and symptom management |
| Sham | 14 | 56 (12.0) | 14 (100) | 32.7 (7.7) | 52.8 (14.0) | 6.3 (1.4) | ||||||||||
| Posner 1994 | Island | ACR criteria (1990) | NR | Lidocaine | 11 | 37.9 (10.9) | 11 (100) | NR | NR | NR | NR | NR | 7.2 (1.2) | NR | NR | NA |
| Placebo | 10 | 32.6 (8.4) | 10 (100) | 6.2 (1.2) | ||||||||||||
| Roedler 2011 | USA | ACR criteria (1990) | 6 | Soy | 12 | 47.5 (16.7) | 12 (100) | NR | NR | NR | NR | NR | NR | NR | NR | NA |
| Placebo | 16 | 16 (100) | ||||||||||||||
| Schweiger 2020 | Italy | ACR criteria (2016) | 6 | acupuncture | 34 | 52.9 (8.5) | 34 (100) | NR | NR | NR | 74.2 (18.2) | NR | 8.5 (1.4) | 23.4 (4) | NR | The most recurrent points were: dumai (Governing Vessel) 20 and 24, heart 7, large intestine 4, renmai (Conception Vessel) 12 and 6, gall bladder 21 and 34, stomach 36, spleen 6, bladder 60, kidney 3, and liver 3. The choice of acupoints was personalized, and some of the acupoints were combined |
| Nutraceutical | 26 | 48.2 (7.4) | 26 (100) | 69 (15.9) | 7.7 (1.7) | 21.5 (5.2) | ||||||||||
| Senna 2012 | Egypt | ACR criteria (1990) | 6 | Placebo | 42 | 46.3 (14.4) | 38 (90.5) | NR | 32.8 (1.4) | 8.6 (4) | 53.2 (11.6) | 17.9 (8.9) | NR | NR | 17.2 (1.6) | NA |
| Weight reduction | 41 | 44.8 (13.6) | 37 (90.2) | 32.3 (1.4) | 9.8 (4.9) | 54.6 (13.1) | 18.6 (8.7) | 16.2 (2.2) | ||||||||
| Targino 2008 | Brazil | ACR criteria (1990) | 24 | Acupuncture | 34 | 52.09 (10.97) | 34 (100) | NR | NR | 9.9 (9.7) | NR | NR | 7.5 (1.8) | NR | 15.8 (2.1) | Ex-HN-3 and bilateral LR3, LI4, PC6, GB34, and SP6 points |
| Sham | 24 | 51.17 (11.20) | 24 (100) | 7.8 (6.3) | 7.5 (1.8) | 15.5 (2.1) | ||||||||||
| Ugurlu 2017 | Turkey | ACR criteria (1990) | 2 | Acupuncture | 25 | 47.28 (7.86) | 25 (100) | NR | NR | 6.28 (4.97) | 60.75 (910.88) | 28.24 (8.87) | 8.28 (1.45) | 55.28 (4.17) | NR | LI 4, ST 36, LV 3, GB 41, GB 34, GB 20, SI 3, SI 4, UB 62, UB 10, SP 6, HT 7, DU 20, DU 14, Kd 27, Ren 6, and PC 6 |
| Sham | 25 | 43.60 (8.18) | 25 (100) | 6.32 (2.21) | 63.92 (5.43) | 28.44 (9.30) | 8.60 (1.25) | 57.28 (6.27) | ||||||||
| Vas 2016 | Spain | ACR criteria (2010) | 12 | Acupuncture | 80 | 52.3 (9.6) | 80 (100) | NR | 28.5 (6.4) | 5.9 (3.7) | 71.7 (11) | NR | 79.3 (11) | NR | 15.6 (2.4) | NR |
| Sham | 82 | 53.2 (9.6) | 82 (100) | 27.7 (5.4) | 5.8 (3.6) | 70.1 (14.2) | 75.8 (13.3) | 15.5 (2.5) | ||||||||
| Vlainich 2010 | Brazil | ACR criteria (1990) | 1 | Lidocaine | 15 | 40.9 (11.6) | 15 (100) | NR | 25.6 (4.1) | 6.8 (5.3) | NR | NR | NR | NR | 15.6 (2.4) | NA |
| Placebo | 15 | 44.7 (10.5) | 15 (100) | 28.1 (5.9) | 5.6 (3.7) | 14.3 (1.8) | ||||||||||
| Vlainich 2011 | Brazil | ACR criteria (1990) | 3 | Lidocaine | 15 | 40.9 (11.6) | 15 (100) | NR | 25.6 (4.1) | NR | NR | NR | NR | NR | NR | NA |
| Placebo | 15 | 44.7 (10.5) | 15 (100) | 28.1 (5.9) | ||||||||||||
| Yuksel 2019 | Turkey | ACR criteria | NR | Acupuncture | 21 | 44.6 ± 10.34 | NR | NR | NR | 7.8 (5.7) | NR | NR | 4.5 (1.8) | NR | NR | Houxi (SI 3), Wangu (SI 4), Shenmai (UB 62), Jinggu (UB 64), Shugu (UB 65), and Yintang |
| TENS | 21 | 38.05 ± 11.3 | 4.25 (2.02) | 5.25 (2.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almutairi, N.M.; Hilal, F.M.; Bashawyah, A.; Dammas, F.A.; Yamak Altinpulluk, E.; Hou, J.-D.; Lin, J.-A.; Varrassi, G.; Chang, K.-V.; Allam, A.E.-S. Efficacy of Acupuncture, Intravenous Lidocaine, and Diet in the Management of Patients with Fibromyalgia: A Systematic Review and Network Meta-Analysis. Healthcare 2022, 10, 1176. https://doi.org/10.3390/healthcare10071176
Almutairi NM, Hilal FM, Bashawyah A, Dammas FA, Yamak Altinpulluk E, Hou J-D, Lin J-A, Varrassi G, Chang K-V, Allam AE-S. Efficacy of Acupuncture, Intravenous Lidocaine, and Diet in the Management of Patients with Fibromyalgia: A Systematic Review and Network Meta-Analysis. Healthcare. 2022; 10(7):1176. https://doi.org/10.3390/healthcare10071176
Chicago/Turabian StyleAlmutairi, Nawaf Masaad, Faisal Mohammed Hilal, Ahmed Bashawyah, Fatma Al Dammas, Ece Yamak Altinpulluk, Jin-De Hou, Jui-An Lin, Giustino Varrassi, Ke-Vin Chang, and Abdallah El-Sayed Allam. 2022. "Efficacy of Acupuncture, Intravenous Lidocaine, and Diet in the Management of Patients with Fibromyalgia: A Systematic Review and Network Meta-Analysis" Healthcare 10, no. 7: 1176. https://doi.org/10.3390/healthcare10071176