
Prevalence of Frailty among Community-Dwelling Older Adults in Asian Countries: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
- What is the overall prevalence of frailty among community-dwelling adults living in Asian countries?
- What factors are associated with the overall prevalence of frailty among community-dwelling adults in Asian countries?
2. Materials and Methods
2.1. Register and Protocol
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection Methods
2.5. Methodological Quality Assessment
2.6. Data Extraction
2.7. Data Synthesis and Analysis
3. Results
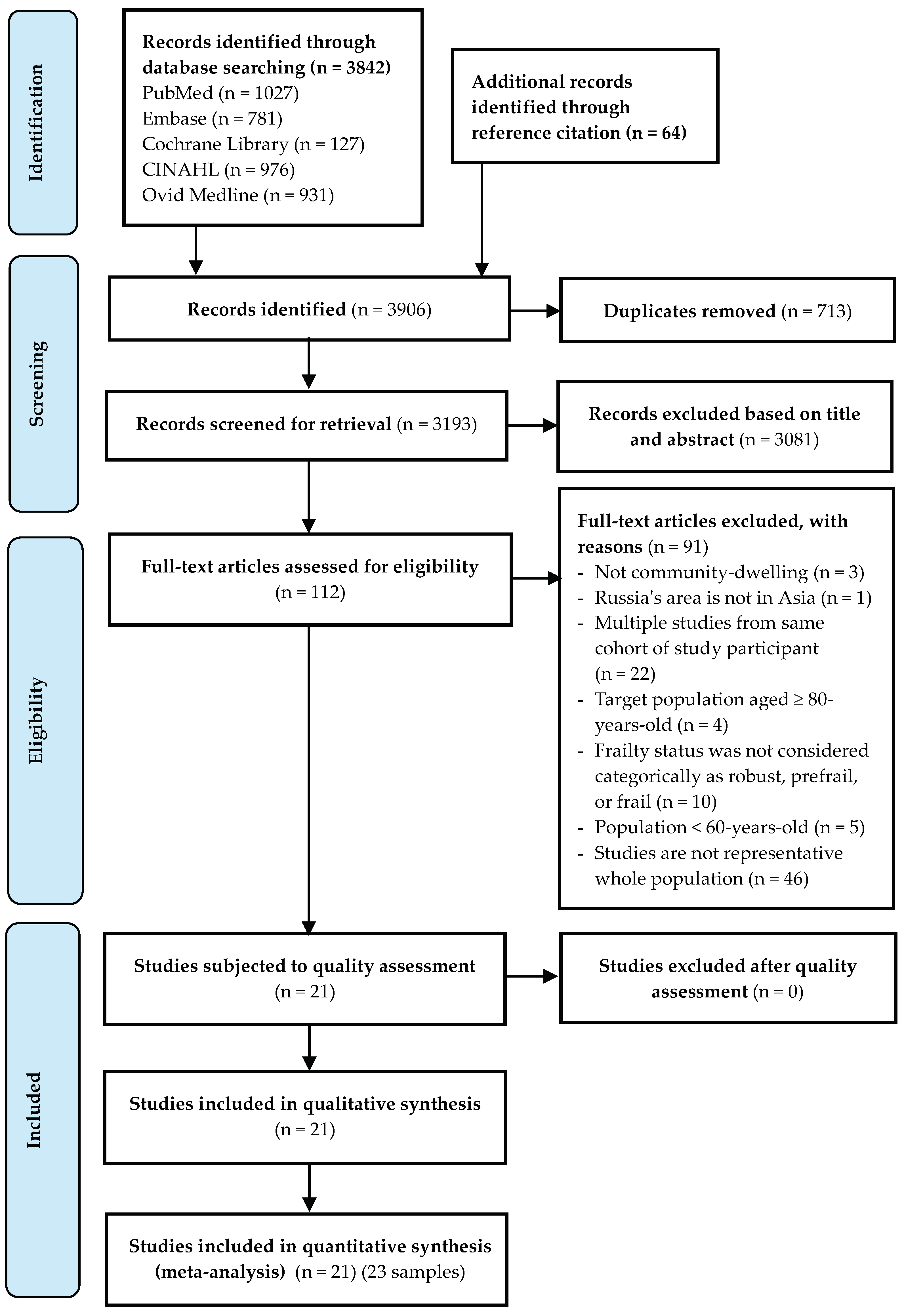
3.1. Selection Process
3.2. Study Characteristics
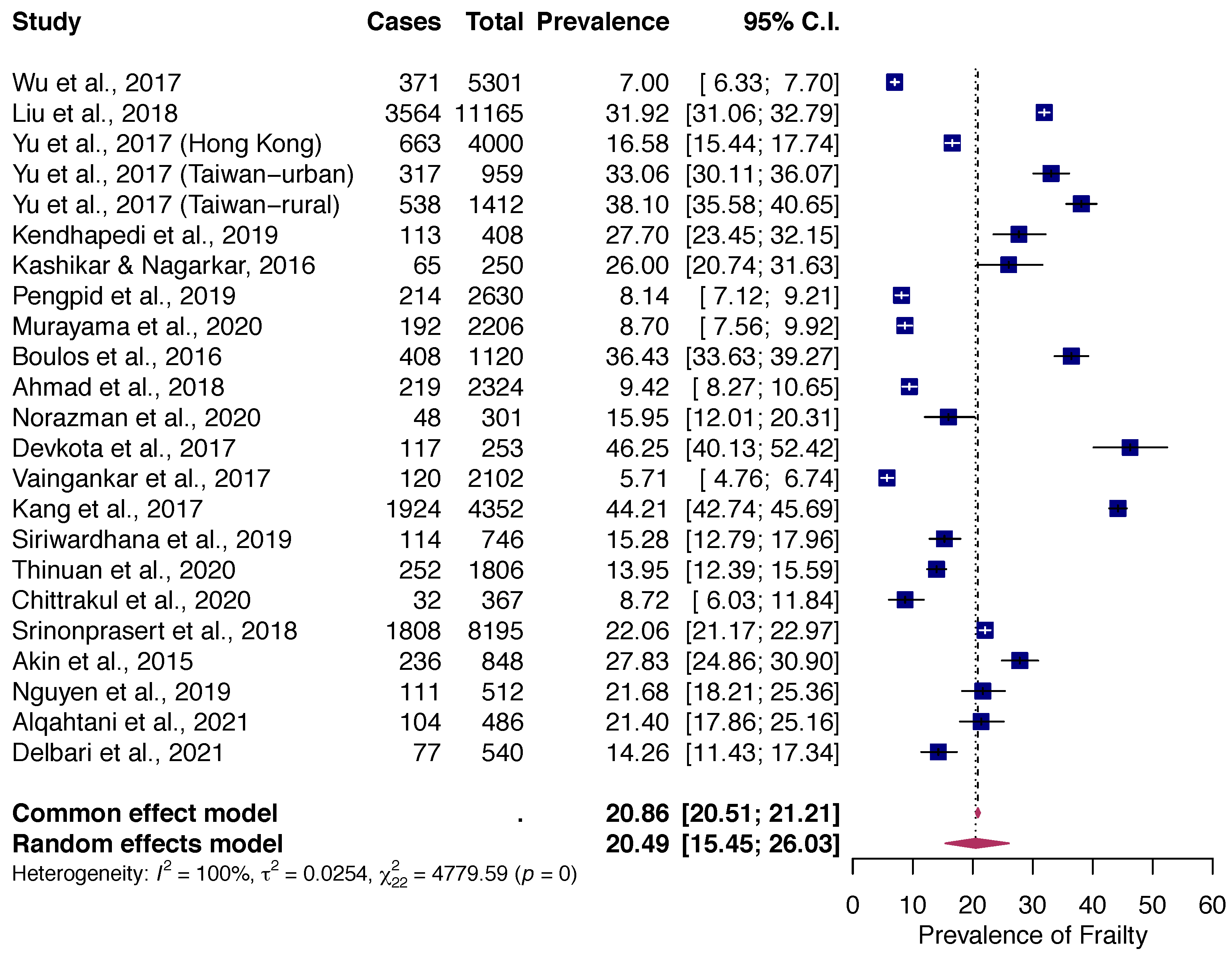
3.3. Prevalence of Frailty
3.4. Factors Associated with Prevalence of Frailty
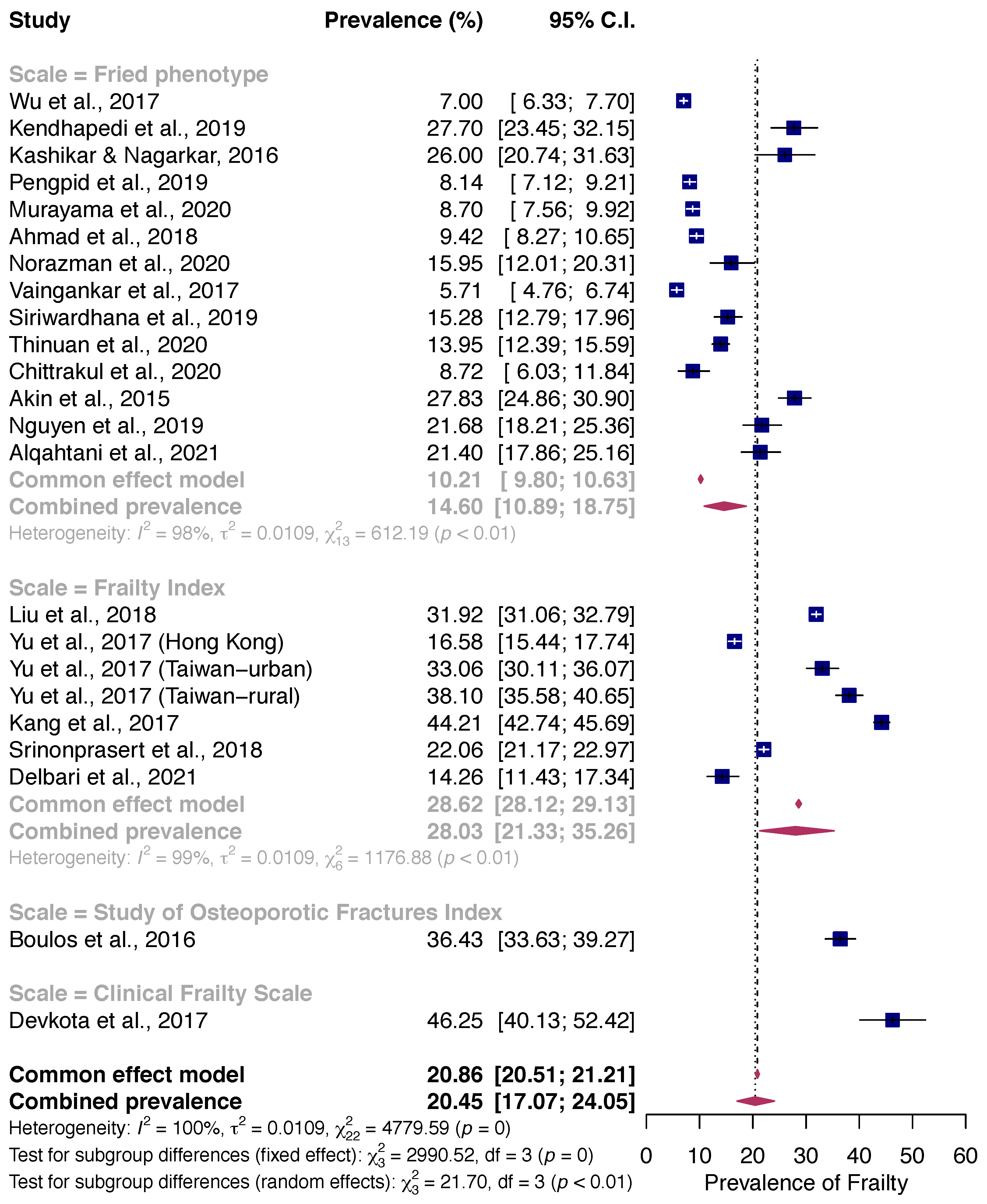
3.4.1. Frailty Assessment Methods
3.4.2. Geographic and Socio-Demographic Characteristics and Lifestyle Factor
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.; Buta, B.; Xue, Q.L. Frailty Screening and Interventions: Considerations for Clinical Practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Vermeiren, S.; Vella-Azzopardi, R.; Beckwée, D.; Habbig, A.-K.; Scafoglieri, A.; Jansen, B.; Bautmans, I.; Bautmans, I.; Verté, D.; Beyer, I.; et al. Frailty and the Prediction of Negative Health Outcomes: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1163.e1–1163.e17. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Xue, Q.L. The frailty syndrome: Definition and natural history. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Gambassi, G.; van Kan, G.A.; Vellas, B. The frailty phenotype and the frailty index: Different instruments for different purposes. Age Ageing 2014, 43, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin. Geriatr. Med. 2011, 27, 17–26. [Google Scholar] [CrossRef]
- Feng, Z.; Lugtenberg, M.; Franse, C.; Fang, X.; Hu, S.; Jin, C.; Raat, H. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: A systematic review of longitudinal studies. PLoS ONE 2017, 12, e0178383. [Google Scholar] [CrossRef] [Green Version]
- Woods, N.F.; LaCroix, A.Z.; Gray, S.L.; Aragaki, A.; Cochrane, B.B.; Brunner, R.L.; Masaki, K.; Murray, A.; Newman, A.B. Frailty: Emergence and consequences in women aged 65 and older in the Women’s Health Initiative Observational Study. J. Am. Geriatr. Soc. 2005, 53, 1321–1330. [Google Scholar] [CrossRef] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Lorenzo-Lopez, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodriguez-Villamil, J.L.; Millan-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Mata, F.A.F.; Pereira, P.P.d.S.; Andrade, K.R.C.d.; Figueiredo, A.C.M.G.; Silva, M.T.; Pereira, M.G. Prevalence of Frailty in Latin America and the Caribbean: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0160019. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Galluzzo, L.; Rodriguez-Laso, A.; Van der Heyden, J.; Ranhoff, A.H.; Lamprini-Koula, M.; Ciutan, M.; Lopez-Samaniego, L.; Carcaillon-Bentata, L.; Kennelly, S.; et al. Prevalence of frailty at population level in European ADVANTAGE Joint Action Member States: A systematic review and meta-analysis. Ann. Ist. Super. Sanita 2018, 54, 226–238. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Sezgin, D.; O’Donovan, M.R.; Molloy, D.W.; Clegg, A.; Rockwood, K.; Liew, A. Prevalence of frailty in 62 countries across the world: A systematic review and meta-analysis of population-level studies. Age Ageing 2021, 50, 96–104. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Cawthon, P.M.; Stone, K.L.; Hillier, T.A.; Cauley, J.A.; Hochberg, M.C.; Rodondi, N.; et al. Comparison of 2 Frailty Indexes for Prediction of Falls, Disability, Fractures, and Death in Older Women. Arch. Intern. Med. 2008, 168, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Cmaj 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Bloom, D.E. 7 Billion and Counting. Science 2011, 333, 562. [Google Scholar] [CrossRef] [Green Version]
- United Nations. World Population Ageing 2017; United Nations: San Francisco, CA, USA, 2017. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- United Nations. World Population Ageing; United Nations: San Francisco, CA, USA, 2019. [Google Scholar]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. JBI Evid. Implement. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Wang, N. How to Conduct a Meta-Analysis of Proportions in R: A Comprehensive Tutorial. N. Y. NY John Jay Coll. Crim. Justicev 2018, 1–62. [Google Scholar] [CrossRef]
- Barendregt, J.J.; Doi, S.A.; Lee, Y.Y.; Norman, R.E.; Vos, T. Meta-analysis of prevalence. J. Epidemiol. Community Health 2013, 67, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Sedgwick, P. Meta-analyses: What is heterogeneity? BMJ 2015, 350, h1435. [Google Scholar] [CrossRef] [Green Version]
- United Nation Statistics Division. Standard Country or Area Codes for Statistical Use. Available online: https://unstats.un.org/unsd/methodology/m49/ (accessed on 10 April 2020).
- Yu, R.; Wu, W.C.; Leung, J.; Hu, S.C.; Woo, J. Frailty and Its Contributory Factors in Older Adults: A Comparison of Two Asian Regions (Hong Kong and Taiwan). Int. J. Environ. Res. Public Health 2017, 14, 1096. [Google Scholar] [CrossRef]
- Wu, C.; Smit, E.; Xue, Q.L.; Odden, M.C. Prevalence and Correlates of Frailty Among Community-Dwelling Chinese Older Adults: The China Health and Retirement Longitudinal Study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 73, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.Y.; Wei, Y.Z.; Wei, L.Q.; Jiang, X.Y.; Wang, X.F.; Shi, Y.; Hai, H. Frailty transitions and types of death in Chinese older adults: A population-based cohort study. Clin. Interv. Aging 2018, 13, 947–956. [Google Scholar] [CrossRef] [Green Version]
- Murayama, H.; Kobayashi, E.; Okamoto, S.; Fukaya, T.; Ishizaki, T.; Liang, J.; Shinkai, S. National prevalence of frailty in the older Japanese population: Findings from a nationally representative survey. Arch. Gerontol. Geriatr. 2020, 91, 104220. [Google Scholar] [CrossRef]
- Kang, M.G.; Kim, S.W.; Yoon, S.J.; Choi, J.Y.; Kim, K.I.; Kim, C.H. Association between Frailty and Hypertension Prevalence, Treatment, and Control in the Elderly Korean Population. Sci. Rep. 2017, 7, 7542. [Google Scholar] [CrossRef] [PubMed]
- Pengpid, S.; Peltzer, K. Prevalence and Associated Factors of Frailty in Community-Dwelling Older Adults in Indonesia, 2014–2015. Int. J. Environ. Res. Public Health 2019, 17, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, N.S.; Hairi, N.N.; Said, M.A.; Kamaruzzaman, S.B.; Choo, W.Y.; Hairi, F.; Othman, S.; Ismail, N.; Peramalah, D.; Kandiben, S.; et al. Prevalence, transitions and factors predicting transition between frailty states among rural community-dwelling older adults in Malaysia. PLoS ONE 2018, 13, e0206445. [Google Scholar] [CrossRef]
- Norazman, C.W.; Adznam, S.N.; Jamaluddin, R. Physical Frailty among Urban-Living Community-Dwelling Older Adults in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 6549. [Google Scholar] [CrossRef]
- Thinuan, P.; Siviroj, P.; Lerttrakarnnon, P.; Lorga, T. Prevalence and Potential Predictors of Frailty among Community-Dwelling Older Persons in Northern Thailand: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4077. [Google Scholar] [CrossRef]
- Chittrakul, J.; Siviroj, P.; Sungkarat, S.; Sapbamrer, R. Physical Frailty and Fall Risk in Community-Dwelling Older Adults: A Cross-Sectional Study. J. Aging Res. 2020, 2020, 3964973. [Google Scholar] [CrossRef]
- Srinonprasert, V.; Chalermsri, C.; Aekplakorn, W. Frailty index to predict all-cause mortality in Thai community-dwelling older population: A result from a National Health Examination Survey cohort. Arch. Gerontol. Geriatr. 2018, 77, 124–128. [Google Scholar] [CrossRef]
- Nguyen, A.T.; Nguyen, L.H.; Nguyen, T.X.; Nguyen, H.T.T.; Nguyen, T.N.; Pham, H.Q.; Tran, B.X.; Latkin, C.A.; Ho, C.S.H.; Ho, R.C.M.; et al. Frailty Prevalence and Association with Health-Related Quality of Life Impairment among Rural Community-Dwelling Older Adults in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 3869. [Google Scholar] [CrossRef] [Green Version]
- Vaingankar, J.A.; Chong, S.A.; Abdin, E.; Picco, L.; Chua, B.Y.; Shafie, S.; Ong, H.L.; Chang, S.; Seow, E.; Heng, D.; et al. Prevalence of frailty and its association with sociodemographic and clinical characteristics, and resource utilization in a population of Singaporean older adults. Geriatr. Gerontol. Int. 2017, 17, 1444–1454. [Google Scholar] [CrossRef]
- Kendhapedi, K.K.; Devasenapathy, N. Prevalence and factors associated with frailty among community-dwelling older people in rural Thanjavur district of South India: A cross-sectional study. BMJ Open 2019, 9, e032904. [Google Scholar] [CrossRef]
- Kashikar, Y.; Nagarkar, A. Prevalence and Determinants of Frailty in Older Adults in India. Indian J. Gerontol. 2016, 30, 364–381. [Google Scholar]
- Devkota, S.; Myint, P.K.; Anderson, B.; Soiza, R.L. Prevalence and determinants of frailty and associated comorbidities among older Gurkha welfare pensioners in Nepal. Geriatr. Gerontol. Int. 2017, 17, 2493–2499. [Google Scholar] [CrossRef] [PubMed]
- Siriwardhana, D.D.; Weerasinghe, M.C.; Rait, G.; Falcaro, M.; Scholes, S.; Walters, K.R. Prevalence of frailty in rural community-dwelling older adults in Kegalle district of Sri Lanka: A population-based cross-sectional study. BMJ Open 2019, 9, e026314. [Google Scholar] [CrossRef]
- Delbari, A.; Zanjari, N.; Momtaz, Y.A.; Rahim, F.; Saeidimehr, S. Prevalence of frailty and associated socio-demographic factors among community-dwelling older people in southwestern Iran: A cross-sectional study. J. Diabetes Metab. Disord. 2021, 20, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Boulos, C.; Salameh, P.; Barberger-Gateau, P. Malnutrition and frailty in community dwelling older adults living in a rural setting. Clin. Nutr. 2016, 35, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Akin, S.; Mazicioglu, M.M.; Mucuk, S.; Gocer, S.; Deniz Safak, E.; Arguvanli, S.; Ozturk, A. The prevalence of frailty and related factors in community-dwelling Turkish elderly according to modified Fried Frailty Index and FRAIL scales. Aging Clin. Exp. Res. 2015, 27, 703–709. [Google Scholar] [CrossRef]
- Alqahtani, B.A.; Alenazi, A.M.; Alshehri, M.M.; Osailan, A.M.; Alsubaie, S.F.; Alqahtani, M.A. Prevalence of frailty and associated factors among Saudi community-dwelling older adults: A cross-sectional study. BMC Geriatr. 2021, 21, 185. [Google Scholar] [CrossRef]
- Siriwardhana, D.D.; Hardoon, S.; Rait, G.; Weerasinghe, M.C.; Walters, K.R. Prevalence of frailty and prefrailty among community-dwelling older adults in low-income and middle-income countries: A systematic review and meta-analysis. BMJ Open 2018, 8, e018195. [Google Scholar] [CrossRef] [Green Version]
- Melo, R.C.; Cipolli, G.C.; Buarque, G.L.A.; Yassuda, M.S.; Cesari, M.; Oude Voshaar, R.C.; Aprahamian, I. Prevalence of Frailty in Brazilian Older Adults: A Systematic Review and Meta-analysis. J. Nutr. Health Aging 2020, 24, 708–716. [Google Scholar] [CrossRef]
- He, B.; Ma, Y.; Wang, C.; Jiang, M.; Geng, C.; Chang, X.; Ma, B.; Han, L. Prevalence and Risk Factors for Frailty among Community-Dwelling Older People in China: A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2019, 23, 442–450. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Taniguchi, Y.; Shimada, H.; Rakugi, H.; Walters, K. Prevalence of frailty in Japan: A systematic review and meta-analysis. J. Epidemiol. 2017, 27, 347–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Eggimann, B.; Cuenoud, P.; Spagnoli, J.; Junod, J. Prevalence of frailty in middle-aged and older community-dwelling Europeans living in 10 countries. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 675–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, H.; Ferrucci, L.; Guralnik, J.; Hogan, D.B.; Hummel, S.; Karunananthan, S.; Wolfson, C. Frailty: An emerging research and clinical paradigm-issues and controversies. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Boccardi, V.; Marano, L. The Geriatric Surgery: The Importance of Frailty Identification Beyond Chronological Age. Geriatrics 2020, 5, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, B.; Li, Q.; Chen, X. Effects of the frailty phenotype on post-operative complications in older surgical patients: A systematic review and meta-analysis. BMC Geriatr. 2019, 19, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, J.M.; Duarte, Y.A.d.O.; Alves, L.C.; Andrade, F.C.D.; Souza Junior, P.R.B.d.; Lima-Costa, M.F.; Andrade, F.B.d. Frailty profile in Brazilian older adults: ELSI-Brazil. Rev. Saúde Pública 2018, 52, S1518–S8787. [Google Scholar]
- Gordon, E.H.; Peel, N.M.; Samanta, M.; Theou, O.; Howlett, S.E.; Hubbard, R.E. Sex differences in frailty: A systematic review and meta-analysis. Exp. Gerontol. 2017, 89, 30–40. [Google Scholar] [CrossRef]
- Littell, J.H.; Corcoran, J.; Pillai, V. Systematic Reviews and Meta-Analysis; Oxford University Press: Oxford, UK, 2008; p. 202. [Google Scholar] [CrossRef]
- Loecker, C.; Schmaderer, M.; Zimmerman, L. Frailty in Young and Middle-Aged Adults: An Integrative Review. J. Frailty Aging 2021, 10, 327–333. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author and Year of Publication | Country/Territory | United Nations Subdivisions | Effective Sample Size a | Age (Mean or Median and Range) | % Female | Frailty Assessment Methods | Data Stratified According to Age | Data Stratified According to Sex | Prevalence of Frailty | Study Quality Assessment Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Wu et al., 2017 [31] | China | Eastern Asia | 5301 | 60+ (69.2 ± 7.0) | 49.4 | * Fried phenotype | yes | yes | 7.0 | 8 |
| Liu et al., 2018 [32] | China | Eastern Asia | 11,165 | 65+ (82.6 ± 9.6) | 52.0 | Frailty Index–44 items | no | no | 31.9 | 8 |
| Yu et al., 2017 (Hong Kong) [30] | Hong Kong | Eastern Asia | 4000 | 65+ (75.21) | 50.0 | Frailty Index–30 items | yes | yes | 16.6 | 8 |
| Yu et al., 2017 (Urban Taiwan) [30] | Taiwan | Eastern Asia | 959 | 60+ (75.36) | 45.78 | Frailty Index–30 items | yes | yes | 33.1 | 8 |
| Yu et al., 2017 (Rural Taiwan) [30] | Taiwan | Eastern Asia | 1412 | 60+ (75.45) | 47.73 | Frailty Index–30 items | yes | yes | 38.1 | 9 |
| Kendhapedi et al., 2019 (Southern India) [43] | India | Southern Asia | 408 | 60+ (67.5 ± 6.62) | 56.86 | * Fried phenotype | no | yes | 27.6 | 8 |
| Frailty index–40 items | 59.2 | |||||||||
| Tilburg Frailty Indicator | 62.6 | |||||||||
| Kashikar & Nagarkar, 2016 (Western India) [44] | India | Southern Asia | 250 | 65+ (73.9 ± 6.4) | 50.0 | * Fried phenotype | yes | yes | 26.0 | 8 |
| Pengpid et al., 2019 [35] | Indonesia | South-Eastern Asia | 2630 | 60–101 (66.0) | 50.60 | * Fried phenotype | yes | yes | 8.14 | 8 |
| Murayama et al., 2020 [33] | Japan | Eastern Asia | 2206 | 65+ | 56.4 | * Fried phenotype | yes | yes | 8.7 | 9 |
| Boulos et al., 2016 [48] | Lebanon | Western Asia | 1120 | 65+ (75.7 ± 7.1) | 50.45 | Study of Osteoporotic Fractures (SOF) index | yes | yes | 36.4 | 8 |
| Ahmad et al., 2018 (Rural Malaysia) [36] | Malaysia | South-Eastern Asia | 2324 | 60+ (70.6) | 61.8 | * Fried phenotype | yes | yes | 9.4 | 8 |
| Norazman et al., 2020 (Urban Malaysia) [37] | Malaysia | South-Eastern Asia | 301 | 60+ (67.08 ± 5.536) | 69.4 | * Fried phenotype | yes | yes | 15.9 | 8 |
| Devkota et al., 2017 [45] | Nepal | Southern Asia | 253 | 60+ | 68.0 | b The Clinical Frailty Scale | no | yes | 46.2 | 5 |
| Vaingankar et al., 2017 [42] | Singapore | South-Eastern Asia | 2102 | 60+ (69) | 53.95 | * Fried phenotype | yes | yes | 5.7 | 8 |
| Kang et al., 2017 [34] | South Korea | Eastern Asia | 4352 | 65+ (72.6 ± 5.4) | 57.4 | Frailty index–42 items | no | yes | 44.2 | 8 |
| Siriwardhana et al., 2019 [46] | Sri Lanka | Southern Asia | 746 | 60–94 (68) | 56.7 | * Fried phenotype | yes | yes | 15.2 | 8 |
| Srinonprasert et al., 2018 [40] | Thailand | South-Eastern Asia | 8195 | 60+ (69.2 ± 6.8) | 0.508 | Frailty Index–30 items | yes | yes | 22.1 | 7 |
| Thinuan et al., 2020 (Northern Thailand) [38] | Thailand | South-Eastern Asia | 1806 | 60–93 (70.74 ± 7.5) | 70.54 | * Fried phenotype | yes | yes | 13.9 | 9 |
| Chittrakul et al., 2020 (Chiang Mai Province) [39] | Thailand | South-Eastern Asia | 367 | 65+ (73.22 ± 7.00) | 64.6 | * Fried phenotype | no | yes | 8.7 | 8 |
| Akin et al., 2015 [49] | Turkey | Western Asia | 848 | 60+ (71.5 ± 5.6) | 50.4 | ‡ Fried phenotype | yes | yes | 27.8 | 9 |
| FRAIL scale | 10.0 | |||||||||
| Nguyen et al., 2019 [41] | Vietnam | South-Eastern Asia | 512 | 60+ | 69.9 | * Fried phenotype | yes | yes | 21.7 | 8 |
| Alqahtani et al., 2021 [50] | Saudi Arabia | Western Asia | 486 | 71 (60–89) | 34.7 | * Fried phenotype | yes | yes | 21.4 | 8 |
| Delbari et al., 2021 [47] | Iran | Southern Asia | 540 | 60+ (72.61 ± 8.72) | 55.93 | Frailty index–30 items | yes | yes | 14.3 | 8 |
| Factors | Number of Datasets | Number of Frail Participants | Prevalence (%) (95% CI) | I2 (%) | p-Value for Difference |
|---|---|---|---|---|---|
| Region | |||||
| Eastern Asia | 2 | 563 | 7.8 (3.9–13.0) | 84 | <0.01 ** |
| South-Eastern Asia | 7 | 996 | 11.3 (8.5–14.5) | 96 | |
| Southern Asia | 3 | 292 | 22.5 (16.5–29.0) | 93 | |
| Western Asia | 2 | 340 | 24.6 (17.4–32.7) | 85 | |
| Gender | 0.67 | ||||
| Male | 14 | 895 | 13.3 (10.1–16.9) | 95.1 | |
| Female | 14 | 1348 | 15.6 (12.3–19.2) | 95.7 | |
| Age groups | 0.01 * | ||||
| 60–64 | 11 | 511 | 8.1 (5.3–11.4) | 95.8 | |
| 65–69 | 12 | 560 | 8.8 (6.1–12.0) | 95.5 | |
| 70–74 | 12 | 718 | 14.4 (10.1–19.3) | 96.1 | |
| 75–79 | 12 | 728 | 19.2 (14.2–24.7) | 95.0 | |
| 80–84 | 12 | 641 | 29.8 (22.6–37.6) | 93.7 | |
| 85+ | 12 | 630 | 34.0 (29.7–38.3) | 73.2 | |
| Marital status | 0.02 * | ||||
| Married | 10 | 881 | 9.0 (7.1–10.9) | 91.6 | |
| Single | 10 | 1211 | 21.5 (14.3–29.5) | 98.1 | |
| Living arrangement | 0.18 | ||||
| Living alone | 6 | 166 | 18.8 (11.8–27.0) | 88.2 | |
| Living with family | 5 | 721 | 11.5 (8.3–15.1) | 95.1 | |
| Smoking status | 0.81 | ||||
| No smoking | 3 | 432 | 12.5 (7.0–19.2) | 96.98 | |
| Current smoking | 4 | 138 | 11.3 (4.8–20.1) | 92.57 | |
| Alcohol Drinking | 0.24 | ||||
| No drinking | 2 | 243 | 16.4 (7.2–28.5) | 96.4 | |
| Current drinking | 2 | 59 | 10.3 (1.0–27.6) | 94.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
To, T.-L.; Doan, T.-N.; Ho, W.-C.; Liao, W.-C. Prevalence of Frailty among Community-Dwelling Older Adults in Asian Countries: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 895. https://doi.org/10.3390/healthcare10050895
To T-L, Doan T-N, Ho W-C, Liao W-C. Prevalence of Frailty among Community-Dwelling Older Adults in Asian Countries: A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(5):895. https://doi.org/10.3390/healthcare10050895
Chicago/Turabian StyleTo, Thi-Lien, Thanh-Nhan Doan, Wen-Chao Ho, and Wen-Chun Liao. 2022. "Prevalence of Frailty among Community-Dwelling Older Adults in Asian Countries: A Systematic Review and Meta-Analysis" Healthcare 10, no. 5: 895. https://doi.org/10.3390/healthcare10050895