
Perceptions of Dental Medicine Students on Equity within Healthcare Systems in Romania: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Characteristics of the Respondents
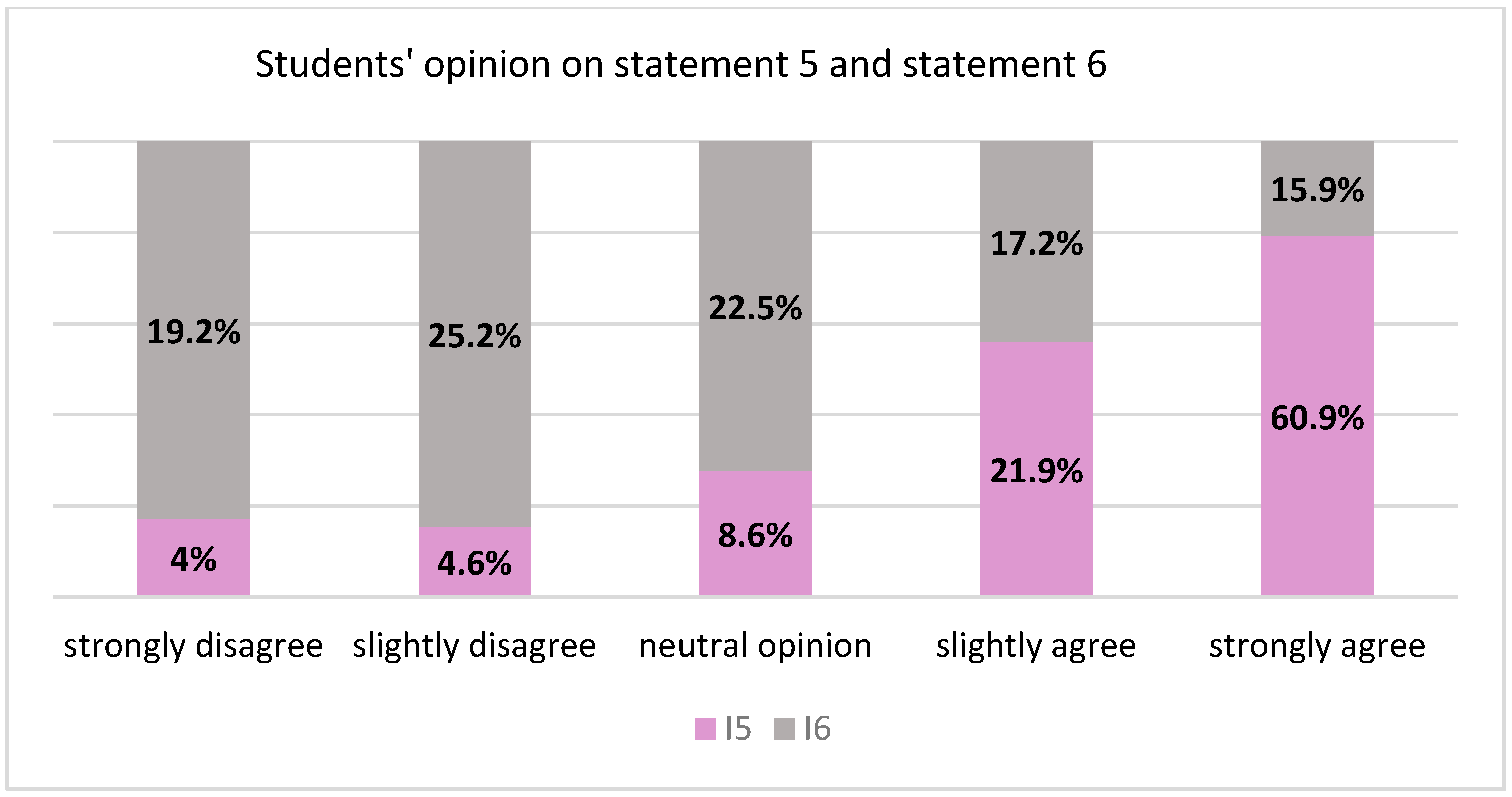
3.2. Opinions on Equity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Council of Europe. European Convention for the Protection of Human Rights and Fundamental Freedoms, as Amended by Protocols Nos. 11 and 14. 1950. Available online: https://www.refworld.org/docid/3ae6b3b04.html (accessed on 20 March 2022).
- Marmot, M.; Allen, J.J. Social Determinants of Health Equity. Am. J. Public Health 2014, 104, S517–S519. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Primary Health Care. Available online: https://www.who.int/health-topics/primary-health-care#tab=tab_1 (accessed on 8 April 2022).
- World Health Organization Health Equity. Available online: https://www.who.int/health-topics/health-equity#tab=tab_1 (accessed on 20 March 2022).
- Gollust, S.E.; Cappella, J.N. Understanding Public Resistance to Messages about Health Disparities. J. Health Commun. 2014, 19, 493–510. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.; Gruskin, S. Defining equity in health. J. Epidemiol. Commun. Health 2003, 57, 254–258. [Google Scholar] [CrossRef]
- Whitehead, M. The Concepts and Principles of Equity and Health. Int. J. Health Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef] [PubMed]
- Dean, H.D.; Roberts, G.W.; Bouye, K.E.; Green, Y.; McDonald, M. Sustaining a Focus on Health Equity at the Centers for Disease Control and Prevention through Organizational Structures and Functions. J. Public Health Manag. Pr. 2016, 22, S60–S67. [Google Scholar] [CrossRef] [PubMed]
- Isailă, O.-M.; Hostiuc, S.; Curcă, G.-C. Perspectives and Values of Dental Medicine Students Regarding Domestic Violence. Medicina 2021, 57, 780. [Google Scholar] [CrossRef]
- National Institute of Statistics. The Activity of the Sanitary Network and Healthcare in 2020. 2021. Available online: https://insse.ro/cms/ro/content/activitatea-rețelei-sanitare-și-de-ocrotire-sănătății-în-anul-2020 (accessed on 8 April 2022).
- National Institute of Statistics. Romania in Numbers-Statistically Brief; INS: Bucharest, Romania, 2019.
- McKneally, M.F.; Dickens, B.M.; Meslin, E.M.; Singer, P.A. Bioethics for clinicians: 13. Resource allocation. Can. Med. Assoc. J. J. L’association Med. Can. 1997, 157, 163–167. [Google Scholar]
- Hostiuc, S. Book of Medical and Dental Bioethics -Resource Allocation; C.H. Beck: Bucharest, Romania, 2021; pp. 256–260. [Google Scholar]
- Wilson, E.; Grumbach, K.; Huebner, J.; Agrawal, J.; Bindman, A.B. Medical student, physician, and public perceptions of health care disparities. Fam. Med. 2004, 36, 715–721. [Google Scholar]
- Fairbrother, H.; Woodrow, N.; Crowder, M.; Holding, E.; Griffin, N.; Er, V.; Dodd-Reynolds, C.; Egan, M.; Lock, K.; Goyder, E.; et al. ‘It All Kind of Links Really’: Young People’s Perspectives on the Relationship between Socioeconomic Circumstances and Health. Int. J. Environ. Res. Public Health 2022, 19, 3679. [Google Scholar] [CrossRef]
- Mooney, G.H. Equity in health care: Confronting the confusion. Eff. Health Care 1983, 1, 179–185. [Google Scholar]
- Wang, H.; Chukwuma, A.; Comsa, R.; Dmytraczenko, T.; Gong, E.; Onofrei, L. Generating Political Priority for Primary Health Care Reform in Romania. Health Syst. Reform 2021, 7, e1898187. [Google Scholar] [CrossRef] [PubMed]
- Kluge, E.-H.W. Resource allocation in healthcare: Implications of models of medicine as a profession. MedGenMed 2007, 9, 57. [Google Scholar] [PubMed]
- Cruess, R.L.; Cruess, S.R. Expectations and Obligations: Professionalism and Medicine’s Social Contract with Society. Perspect. Biol. Med. 2008, 51, 579–598. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Chase, L.E.; Wagnild, J.; Akhter, N.; Sturridge, S.; Clarke, A.; Chowdhary, P.; Mukami, D.; Kasim, A.; Hampshire, K. Community health workers and health equity in low- and middle-income countries: Systematic review and recommendations for policy and practice. Int. J. Equity Health 2022, 21, 49. [Google Scholar] [CrossRef] [PubMed]
- Lago, S.; Cantarero, D.; Rivera, B.; Pascual, M.; Blázquez-Fernández, C.; Casal, B.; Reyes, F. Socioeconomic status, health inequalities and non-communicable diseases: A systematic review. Z. Gesundh. Wiss. 2018, 26, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richard, L.; Furler, J.; Densley, K.; Haggerty, J.; Russell, G.; Levesque, J.-F.; Gunn, J. Equity of access to primary healthcare for vulnerable populations: The IMPACT international online survey of innovations. Int. J. Equity Health 2016, 15, 64. [Google Scholar] [CrossRef] [Green Version]
- Rawls, J. A Theory of Justice; Belknap Press: Cambridge, MA, USA, 1999. [Google Scholar]
- Green, R.M. Access to Healthcare: Going Beyond Fair Equality of Opportunity. Am. J. Bioeth. 2001, 1, 22–23. [Google Scholar] [CrossRef]
- Elias, A.; Paradies, Y. The Costs of Institutional Racism and its Ethical Implications for Healthcare. J. Bioethical Inq. 2021, 18, 45–58. [Google Scholar] [CrossRef]
- Better, S.O. Institutional Racism: A Primer on Theory and Strategies for Social Change, 2nd ed.; Rowman & Littlefield Publishers: Lanham, MD, USA, 2008. [Google Scholar]
- Daly, S. Racial differences in the quality of home health care: What are the contributing factors? Ph.D. Thesis, The University of North Carolina, Chaper Hill, NC, USA, 2016. [Google Scholar]
- Shmueli, L.; Davidovitch, N.; Pliskin, J.S.; Balicer, R.D.; Hekselman, I.; Greenfield, G. Seeking a second medical opinion: Composition, reasons and perceived outcomes in Israel. Isr. J. Health Policy Res. 2017, 6, 67. [Google Scholar] [CrossRef] [Green Version]
- Cortes, L.F.; Padoin, S.M.D.M.; Vieira, L.B.; Landerdahl, M.C.; Arboit, J. Cuidar mulheres em situação de violência: Empoderamento da enfermagem em busca de equidade de gênero. Rev. Gaúcha Enferm. 2015, 36, 77–84. [Google Scholar] [CrossRef]
- McCloskey, L.A.; Williams, C.M.; Lichter, E.; Gerber, M.; Ganz, M.L.; Sege, R. Abused Women Disclose Partner Interference with Health Care: An Unrecognized Form of Battering. J. Gen. Intern. Med. 2007, 22, 1067–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hostiuc, S.; Curcǎ, C.G.; Dermengiu, D. Consent and confidentiality in medical assistance for women victims of domestic violence. Rev. Rom. Bioet. 2011, 9, 96–107. [Google Scholar]



{kind=link}
{kind=link}
| Statement | Strongly Disagree | Slightly Disagree | Neutral Opinion | Slightly Agree | Strongly Agree |
|---|---|---|---|---|---|
| S1“The presence of disadvantaged populations is acknowledged on a social level.” | 3 (2%) | 13 (8.6%) | 13 (8.6%) | 43 (28.5%) | 79 (52.3%) |
| S2”Equity represents an essential element in public healthcare.” | 2 (1.3%) | 1 (0.7%) | 14 (9.3%) | 27 (17.9%) | 107 (70.9%) |
| S3 ”Disadvantaged populations have a poor state of health.” | 1 (0.7%) | 4 (2.6%) | 9 (6%) | 41 (27.2%) | 96 (63.6%) |
| S4 “It is equitable for dental healthcare to be free of charge as long as any person would have the right to a single dental appointment every two months.” | 7 (4.6%) | 13 (8.6%) | 37 (24.5%) | 30 (19.9%) | 64 (42.4%) |
| Statement | Strongly Disagree | Slightly Disagree | Neutral Opinion | Slightly Agree | Strongly Agree |
|---|---|---|---|---|---|
| S7 “It is inequitable if a person who is unemployed cannot benefit from dental treatments they need because they do not have the financial means.” | 11 (7.3%) | 23 (15.3.%) | 37 (24.7%) | 34 (22.7%) | 45 (30%) |
| S8 “It is inequitable if a person who is employed cannot benefit from the dental treatment they need because they do not have enough financial means.” | 6 (4.0%) | 13 (8.6%) | 24 (15.9%) | 47 (31.1%) | 61 (40.4%) |
| S9 “It is inequitable if the employees of a bank benefit from dental care with reduced costs, promptly and regularly through their place of work.” | 17 (11.3%) | 27 (17.9%) | 39 (25.8%) | 37 (24.5%) | 31 (20.5%) |
| S10 “It is inequitable if a person of a certain ethnicity refuses to ask for dental treatment they need because the dentists always approach them with contempt.” | 20 (13.2%) | 23 (15.2%) | 13 (8.6%) | 22 (14.6%) | 73 (48.3%) |
| S11 “It is inequitable if a dentist reduces treatment costs to attract patients.” | 42 (27.8%) | 39 (25.8%) | 47 (31.1%) | 14 (9.3%) | 9 (6.0%) |
| S13 “It is inequitable if a person is refused a second medical opinion.” | 6 (4.0%) | 3 (2.0%) | 10 (6.6%) | 10 (6.6%) | 122 (80.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hostiuc, S.; Isailă, O.-M.; Curcă, G.-C. Perceptions of Dental Medicine Students on Equity within Healthcare Systems in Romania: A Pilot Study. Healthcare 2022, 10, 857. https://doi.org/10.3390/healthcare10050857
Hostiuc S, Isailă O-M, Curcă G-C. Perceptions of Dental Medicine Students on Equity within Healthcare Systems in Romania: A Pilot Study. Healthcare. 2022; 10(5):857. https://doi.org/10.3390/healthcare10050857
Chicago/Turabian StyleHostiuc, Sorin, Oana-Maria Isailă, and George-Cristian Curcă. 2022. "Perceptions of Dental Medicine Students on Equity within Healthcare Systems in Romania: A Pilot Study" Healthcare 10, no. 5: 857. https://doi.org/10.3390/healthcare10050857