
Ethics and Automated Systems in the Health Domain: Design and Submission of a Survey on Rehabilitation and Assistance Robotics to Collect Insiders’ Opinions and Perception


Abstract
:1. Introduction
1.1. Robotics in Rehabilitation and Assistance
- Robotic surgery
- Care and socially assistive robots
- Rehabilitation systems
- Training for health and care workers.
1.2. Ethics and the Introduction of the Automated Systems in the Health Domain
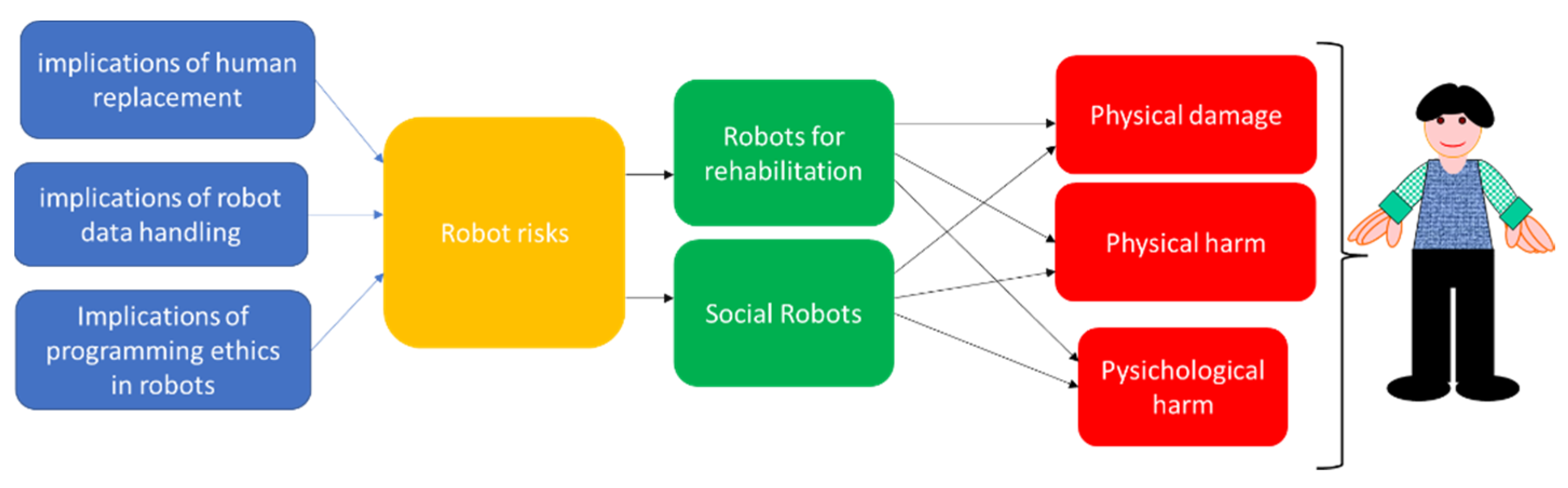
1.3. Ethics and Rehabilitation and Assistance Robotics
- the implications to work of those in contact with the patient;
- consequently, the quality of care in relation to what has been defined as a risk of dehumanization or even cold care.
- the implications of the decision-making autonomy of the decision-making robot (e.g., margins and impact);
- the chain of responsibility for the decision-making robot;
- the risk of deception, such as the risk of creating false friendships with social robots;
- the trust in placing a patient (for example a frail person) in the hands of a robot.
- privacy and data protection;
- safety and avoidance of harm.
1.4. Hypothesis of the Study
1.5. Objectives of the Study
- Develop and administer a remote electronic survey that would allow: (a) the collection of demographic data and (b) the collection of data on the training on ethics and the self-perception of the impact of the ethics, concerns, and suggestions.
- To collect feedback on the investigation and opinions on this topic.
2. Methods
2.1. Participants and Procedure
2.1.1. The Selected Tool and the Adequacy of Regulations
2.1.2. Main Characteristics of the Chosen Tool
2.1.3. The Tool: Structure
2.1.4. Submission and Participants
2.2. Measures
2.3. Statistics
3. Results
3.1. Submission
3.2. Preliminary Test of Statistical Significance
3.3. The Ethics Perception on the Insiders
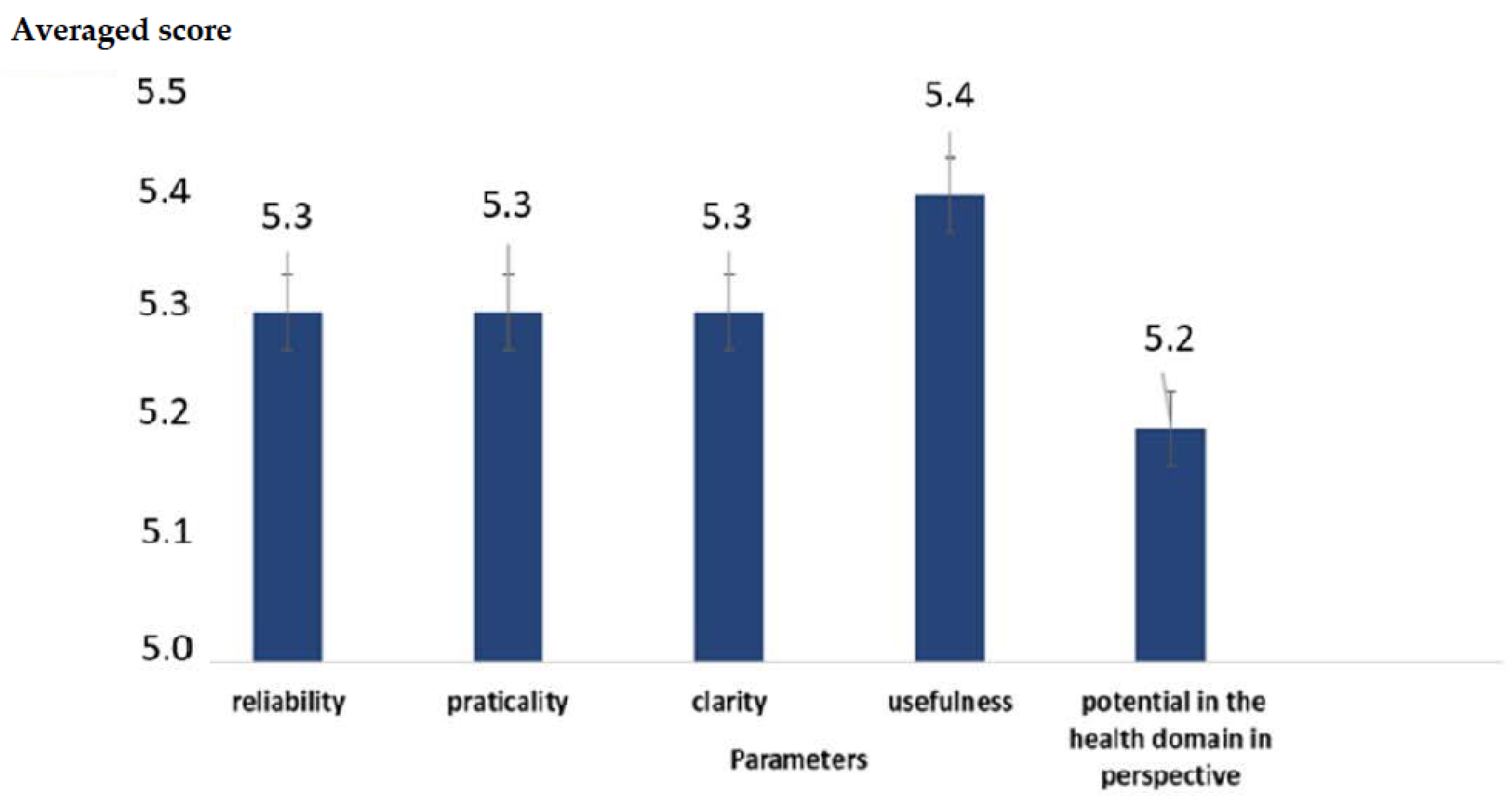
3.4. Feedback from the Participants
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dolic, Z.; Castro, R.; Moarcas, A. Robots in Healthcare: A Solution or a Problem? Study for the Committee on Environment, Public Health, and Food Safety. Luxembourg: Policy Department for Economic, Scientific and Quality of Life Policies, European Parliament. 2019. Available online: https://www.europarl.europa.eu/RegData/etudes/IDAN/2019/638391/IPOL_IDA(2019)638391_EN.pdf (accessed on 25 November 2021).
- Boldrini, P.; Bonaiuti, D.; Mazzoleni, S.; Posteraro, F. Rehabilitation assisted by robotic and electromechanical devices for people with neurological disabilities: Contributions for the preparation of a national conference in Italy. Eur. J. Phys. Rehabil. Med. 2021, 57, 458–459. [Google Scholar] [CrossRef] [PubMed]
- Giansanti, D. The Rehabilitation and the Robotics: Are They Going Together Well? Healthcare 2021, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, T.B. A review of recent research in social robotics. Curr. Opin. Psychol. 2020, 36, 7–12. [Google Scholar] [CrossRef]
- Lötsch, J.; Kringel, D.; Ultsch, A. Explainable Artificial Intelligence (XAI) in Biomedicine: Making AI Decisions Trustworthy for Physicians and Patients. BioMedInformatics 2022, 2, 1–17. [Google Scholar] [CrossRef]
- Datta, A.; Matlock, M.K.; Le Dang, N.; Moulin, T.; Woeltje, K.F.; Yanik, E.L.; Swamidass, S.J. ‘Black Box’ to ‘Conversational’ Machine Learning: Ondansetron Reduces Risk of Hospital-Acquired Venous Thromboembolism. IEEE J. Biomed. Health Inform. 2021, 25, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.; Flynn, N.R.; Barnette, D.A.; Woeltje, K.F.; Miller, G.P.; Swamidass, S.J. Machine learning liver-injuring drug interactions with non-steroidal anti-inflammatory drugs (NSAIDs) from a retrospective electronic health record (EHR) cohort. PLoS Comput. Biol. 2021, 17, e1009053. [Google Scholar] [CrossRef] [PubMed]
- Giovagnoli, M.R.; Giansanti, D. Artificial Intelligence in Digital Pathology: What Is the Future? Part 1: From the Digital Slide Onwards. Healthcare 2021, 9, 858. [Google Scholar] [CrossRef] [PubMed]
- Giansanti, D.; Di Basilio, F. The Artificial Intelligence in Digital Radiology: Part 1: The Challenges, Acceptance and Consensus. Healthcare 2022, 10, 509. [Google Scholar] [CrossRef] [PubMed]
- D’Antonoli, T.A. Ethical considerations for artificial intelligence: An overview of the current radiology landscape. Diagn. Interv. Radiol. 2020, 26, 504–511. [Google Scholar]
- Banks, J. The Human Touch: Practical and Ethical Implications of Putting AI and Robotics to Work for Patients. IEEE Pulse. 2018, 9, 15–18. [Google Scholar] [CrossRef]
- Fosch-Villaronga, E.; Mahler, T. Safety and robots: Strengthening the link between cybersecurity and safety in the context of care robots. Comput. Law Secur. Rev. 2021, 41, 105528. [Google Scholar] [CrossRef]
- Stahl, B.C.; Coeckelbergh, M. Ethics of healthcare robotics: Towards responsible research and innovation. Robot. Auton. Syst. 2016, 86, 152–161. [Google Scholar] [CrossRef]
- Datteri, E. Predicting the long-term effects of human robot interaction: A reflection on responsibility in medical robotics. Sci. Eng. Ethics 2013, 19, 139–160. [Google Scholar] [CrossRef]
- Iosa, M.; Morone, G.; Cherubini, A.; Paolucci, S. The Three Laws of Neurorobotics: A Review on What Neurorehabilitation Robots Should Do for Patients and Clinicians. J. Med. Biol Eng. 2016, 36, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morone, G. Robots for stroke rehabilitation: Not all that glitters is gold. Funct Neurol. 2019, 34, 5–6. [Google Scholar] [PubMed]
- Gordon, J.S. Building moral robots: Ethical pitfalls and challenges. Sci. Eng. Ethics 2020, 26, 141–157. [Google Scholar] [CrossRef]
- Coeckelbergh, M. Human development or human enhancement? A methodological reflection on capabilities and the evaluation of information technologies. Ethics Inf. Technol. 2011, 13, 81–92. [Google Scholar] [CrossRef] [Green Version]
- Coeckelbergh, M. Are emotional robots deceptive? IEEE Trans. Affect. Comput. 2012, 3, 388–393. [Google Scholar] [CrossRef]
- Coeckelbergh, M. E-care as craftsmanship: Virtuous work, skilled engagement, and information technology in health care. Med. Health Care Philos. 2013, 16, 807–816. [Google Scholar] [CrossRef]
- Coeckelbergh, M. Good healthcare is in the ‘‘how’’: The quality of care, the role of machines, and the need for new skills. In Machine Medical Ethics; van Rysewyk, S.P., Pontier, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 33–48. [Google Scholar]
- Decker, M.; Fleischer, T. Contacting the brain—aspects of a technology assessment of neural implants. Biotechnol. J. 2008, 3, 1502–1510. [Google Scholar] [CrossRef]
- Sharkey, A.; Sharkey, N. Granny and the robots: Ethical issues in robot care for the elderly. Ethics Inform. Technol. 2010, 14, 27–40. [Google Scholar] [CrossRef]
- Sparrow, R.; Sparrow, L. In the hands of machines? The future of aged care. Minds Mach. 2006, 16, 141–161. [Google Scholar] [CrossRef]
- Whitby, B. Do you want a robot lover? In Robot. Ethics: The Ethical and Social Implications of Robotics; Lin, P., Abney, K., Bekey, G.A., Eds.; MIT Press: Cambridge, MA, USA, 2011; pp. 233–249. [Google Scholar]
- Wallach, W.; Allen, C. Moral Machines: Teaching Robots Right from Wrong; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Anderson, M.; Anderson, S.L. Machine Ethics; Cambridge University Press: Cambridge, MA, USA, 2011. [Google Scholar]
- Gunkel, D.J.; Bryson, J. The machine as moral agent and patient. Philos. Technol. 2014, 27, 5–142. [Google Scholar] [CrossRef] [Green Version]
- Anderson, S.L. Machine metaethics. In Machine Ethics; Anderson, M., Anderson, S.L., Eds.; Cambridge University Press: Cambridge, MA, USA, 2011; pp. 21–27. [Google Scholar]
- Etemad-Sajadi, R.; Soussan, A.; Schöpfer, T. How Ethical Issues Raised by Human-Robot Interaction can Impact the Intention to use the Robot? Int. J. Soc. Robot. 2022, 13, 1–13. [Google Scholar] [CrossRef]
- Beer, J.M.; Prakash, A.; Mitzner, T.L.; Rogers, W.A. Understanding Robot Acceptance. Ga. Inst. Technol. 2011, 1–45. Available online: https://smartech.gatech.edu/bitstream/handle/1853/39672/HFA-TR-1103-RobotAcceptance.pdf (accessed on 10 March 2022).
- Gefen, D.; Karahanna, E.; Straub, D. Trust and TAM in online shopping: An integrated model. MIS Q 2003, 27, 51–90. [Google Scholar] [CrossRef]
- European Union’s Convention on Roboethics; European Union: Maastricht, The Netherlands, 2010.
- Lin, P.; Abney, K.; Bekey, G.A. Robot. Ethics: The Ethical and Social Implications of Robotics; The MIT Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Graeff, T.R.; Harmon, S. Collecting and using personal data: Consumers’ awareness and concerns. J. Consum Mark. 2002, 19, 302–318. [Google Scholar] [CrossRef]
- Nizamis, K.; Athanasiou, A.; Almpani, S.; Dimitrousis, C.; Astaras, A. Converging Robotic Technologies in Targeted Neural Rehabilitation: A Review of Emerging Solutions and Challenges. Sensors 2021, 21, 2084. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Powers, B.; Vogeli, C.; Mullainathan, S. Dissecting racial bias in an algorithm used to manage the health of populations. Science 2019, 366, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://forms.office.com/Pages/ResponsePage.aspx?id=DQSIkWdsW0yxEjajBLZtrQAAAAAAAAAAAAZAAOUXdFhUM1UxU0VDMEM0ODYyQUZXWTYzMU1WOTJYSS4u (accessed on 10 March 2022).
- Available online: https://drive.google.com/file/d/1rKPyhpYc9ThmhURJEfr2WiLOuZ9FUi86/view?usp=sharing (accessed on 10 March 2022).
- Available online: https://www.surveymonkey.com/mp/likert-scale/ (accessed on 10 March 2022).
- Eiben, Á.E.; Ellers, J.; Meynen, G.; Nyholm, S. Robot Evolution: Ethical Concerns. Front. Robot. AI 2021, 8, 744590. [Google Scholar] [CrossRef]
- Kok, B.C.; Soh, H. Trust in Robots: Challenges and Opportunities. Curr. Robot. Rep. 2020, 1, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Cornet, G. Robot companions and ethics a pragmatic approach of ethical design. J. Int. Bioethique 2013, 24, 49–58, 179–180. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, B.; Tremblay-Laprise, A.A.; Filion, M.; Boon, H.; Daly, C.; van den Hoven, M.; Heilbronn, R.; Lenselink, M.; Walters, S. A five-country survey on ethics education in preservice teaching programs. J. Teach. Educ. 2016, 67, 135–151. [Google Scholar] [CrossRef] [Green Version]
- Maccioni, G.; Ruscitto, S.; Gulino, R.A.; Giansanti, D. Opportunities and Problems of the Consensus Conferences in the Care Robotics. Healthcare 2021, 9, 1624. [Google Scholar] [CrossRef] [PubMed]
- SIMFER; SIRN. Documento Definitivo di Consenso a Cura della Giuria della Consensus Conference CICERONE. Available online: https://www.simfer.it/wp-content/uploads/doc_vari/2022_Doc_Finale_ConsensusConferenceRoboticaCICERONE/CONSENSUSCICERONE-DOCUMENTOFINALEDEF.-con-licenza-2.pdf (accessed on 10 March 2022).
- Choi, H.; Jeong, G. Characteristics of the Measurement Tools for Assessing Health Information-Seeking Behaviors in Nationally Representative Surveys: Systematic Review. J. Med. Internet Res. 2021, 23, e27539. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Age and Gender |
|---|---|
| 155 professionals of the health domain with specific academic training | Age between 23 and 64 years. 78 males (mean age 43.7; minimum age 24, maximum age 64) 77 females (mean age 44.3; minimum age 23, maximum age 64) |
| Question | Score |
|---|---|
| Ethics in general | 3.04 |
| Ethics and robotics | 2.87 |
| Ethics and artificial intelligence | 2.93 |
| Ethics and virtual reality | 2.99 |
| Question | Score |
|---|---|
| Ethics in general | 3.64 |
| Ethics and robotics | 3.51 |
| Ethics and artificial intelligence | 3.52 |
| Ethics and virtual reality | 3.53 |
| Question | N(1) | N(2) | N(3) | N(4) | N(5) | N(6) | Score |
|---|---|---|---|---|---|---|---|
| The relationships with the robotic devices | 2 | 6 | 4 | 27 | 40 | 76 | 5.01 |
| The impact of the virtual reality | 1 | 6 | 15 | 18 | 62 | 53 | 4.89 |
| The use of social robots | 3 | 7 | 16 | 18 | 64 | 47 | 4.77 |
| The use of Artificial Intelligence | 3 | 7 | 17 | 18 | 70 | 40 | 4.71 |
| The integration between the artificial intelligence and virtual reality with the robotcs | 4 | 5 | 14 | 18 | 68 | 46 | 4.80 |
| The regulation issues | 0 | 0 | 1 | 5 | 64 | 85 | 5.50 |
| Question | N(1) | N(2) | N(3) | N(4) | N(5) | N(6) | Score |
|---|---|---|---|---|---|---|---|
| The use of the robotics in general | 2 | 5 | 5 | 37 | 30 | 76 | 5.04 |
| The integration of robotics with artificial intelligence | 2 | 7 | 13 | 18 | 62 | 53 | 4.87 |
| The integration of robotics with the virtual reality | 4 | 6 | 15 | 19 | 54 | 57 | 4.83 |
| The use of the social robot | 0 | 0 | 1 | 11 | 11 | 132 | 5.77 |
| Question | Number of Choices |
|---|---|
| Social cues | 4 |
| Privacy and data protection | 2 |
| Replacement | 111 |
| Autonomy | 13 |
| Trust and safety | 5 |
| Responsibility | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morone, G.; Pirrera, A.; Meli, P.; Giansanti, D. Ethics and Automated Systems in the Health Domain: Design and Submission of a Survey on Rehabilitation and Assistance Robotics to Collect Insiders’ Opinions and Perception. Healthcare 2022, 10, 778. https://doi.org/10.3390/healthcare10050778
Morone G, Pirrera A, Meli P, Giansanti D. Ethics and Automated Systems in the Health Domain: Design and Submission of a Survey on Rehabilitation and Assistance Robotics to Collect Insiders’ Opinions and Perception. Healthcare. 2022; 10(5):778. https://doi.org/10.3390/healthcare10050778
Chicago/Turabian StyleMorone, Giovanni, Antonia Pirrera, Paola Meli, and Daniele Giansanti. 2022. "Ethics and Automated Systems in the Health Domain: Design and Submission of a Survey on Rehabilitation and Assistance Robotics to Collect Insiders’ Opinions and Perception" Healthcare 10, no. 5: 778. https://doi.org/10.3390/healthcare10050778