
An Effective Strategy and Mathematical Model to Predict the Sustainable Evolution of the Impact of the Pandemic Lockdown


 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Related Work
2.1. Objectives
2.2. Contributions
- Unlike the classical Susceptible–Exposed–Infected–Removed (SEIR) model, the proposed SEIHRD model has six states that differentiate between diagnosed and non-diagnosed individuals.
- In this study, the authors consider two different transmission rates for a susceptible person to be infected and a susceptible person to become a carrier, respectively. This discrimination is significant because the diagnosed individual is isolated and less likely to spread the highly infectious coronavirus disease. In the absence of strong visible symptoms, it becomes difficult to test an individual for COVID-19 unless that individual has come in contact with a positive confirmed case.
- The mortality rate and recovery rate are taken as time functions as the disease progresses in India. This choice is data-driven. A change in mortality rate and recovery rate has been observed since the first case in January 2020.
- In addition, a time-dependent transmission rate, which incorporated government control policy and public perception of risk, has been investigated along with the conceptual model to perform a sensitivity analysis in Indian context.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Classical Model | Proposed Model |
|---|---|---|
| 1 | Classical SEIR model has four states | The proposed model has six states |
| 2 | The classical model SEIR do not differentiate be-tween diagnosed and non-diagnosed individual | The proposed model discriminates between diagnosed and non-diagnosed individual |
| 3 | Pre-symptomatic transmission is not taken into account | Pre-symptomatic transmission is taken into account |
| 4 | SEIR is not dependent on time | Various transmission rates are time-dependent |
| 5 | Governmental control and public perception of risk of the disease not included | Governmental control and public perception of risk of the disease are taken into account |
3. Mathematical Modeling of COVID-19
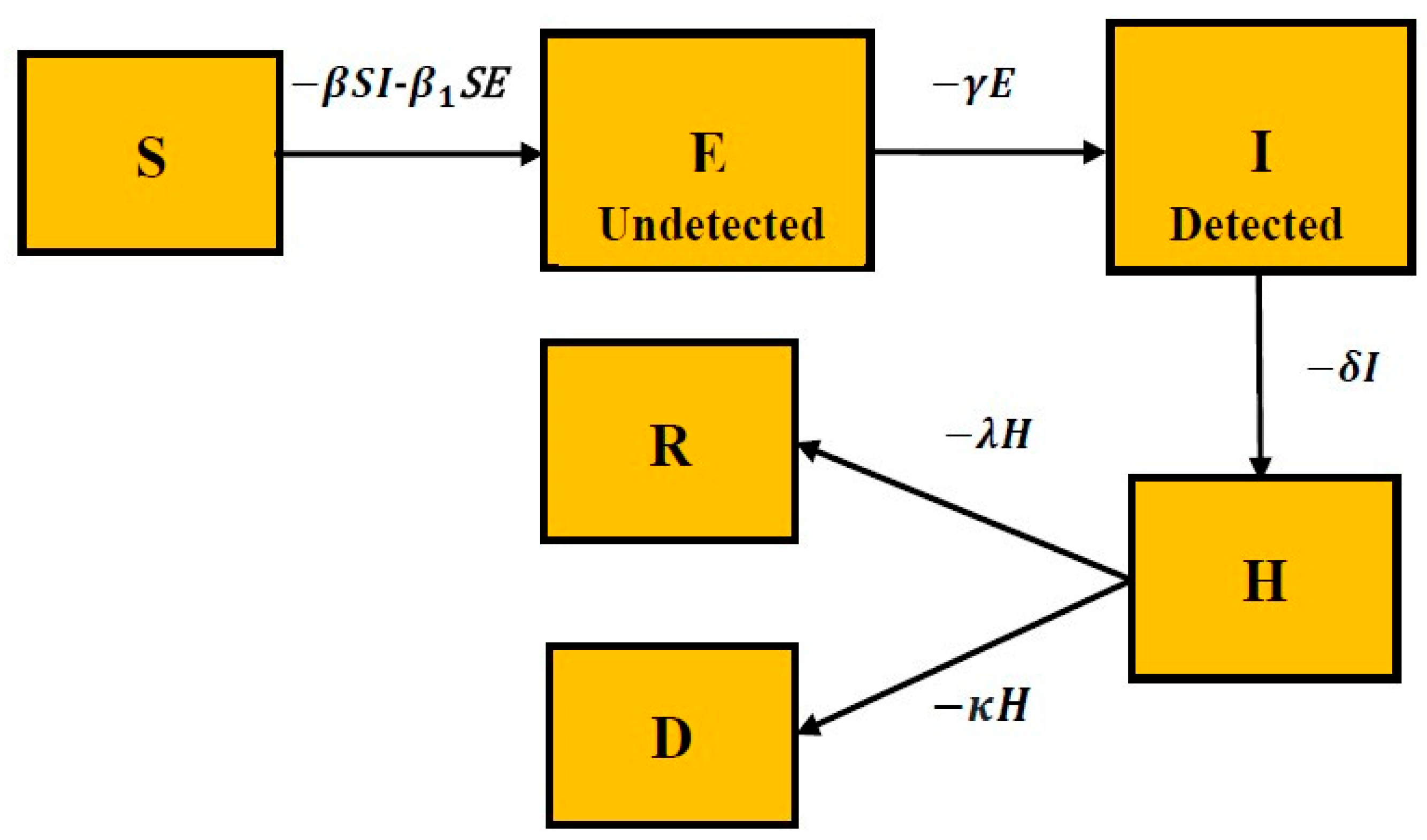
3.1. Proposed Model: SEIHRD
- The susceptible compartment contains the population that is susceptible to the highly infectious novel coronavirus.
- The exposed compartment consists of a fraction of susceptible populations comprising infected and asymptomatic infected individuals (carrier/latent class). They are not yet detected but are infectious.
- The infected state comprises the fraction of exposed people who are asymptomatic and symptomatic infected individuals. However, they are detected and infectious.
- The hospitalization compartment consists of a fraction of the infected population that is hospitalized.
- The recovered state contains the fraction of hospitalized people who have recovered from the infectious disease.
- The dead state consists of a fraction of hospitalized people who have died from the infectious disease.
- Step 1: Downloading the data from www.COVIDindia.org and read them.
- Step 2: Initialization of parameters: Recovered daily, Deaths daily, and Confirmed cases daily.
- Step 3: Fitting the proposed SEIHRD model to the real data with a function.
- Step 4: Estimation of the parameters such as fitted infection rate, transmission rate, recovery rate, rate at which individual is admitted to hospital, etc.
- Step 5: Simulate the epidemic outbreak based on the fitted parameters.
- Step 6: Comparison of the fitted data and the accurate data.
3.1.1. Assumptions
- A number of assumptions have been made based on the availability of data in India and periodic World Health Organization press releases: the natural death rate and birthrate do not change the population structure significantly across all compartments, and they are therefore taken to be constant so that the population size is constant.
- Unlike the usual SEIR model, the Latent population (E) here is asymptomatic but infectious and undetected or not diagnosed.
- The Infectious population (I) is asymptomatic, as well as infectious and detected/diagnosed.
- Upon coming into contact with Infected (I) or Latent (E) individuals, Susceptible (S) individuals become contagious.
- Only Infectious cases (I) fill up the hospitals and can lead to a higher fatality rate due to shortage of available care.
- Individuals are immune after recovery (R).
3.1.2. Mathematical Model
3.1.3. Dataset Description
3.1.4. Time-Dependent Transmission Rate
4. Results
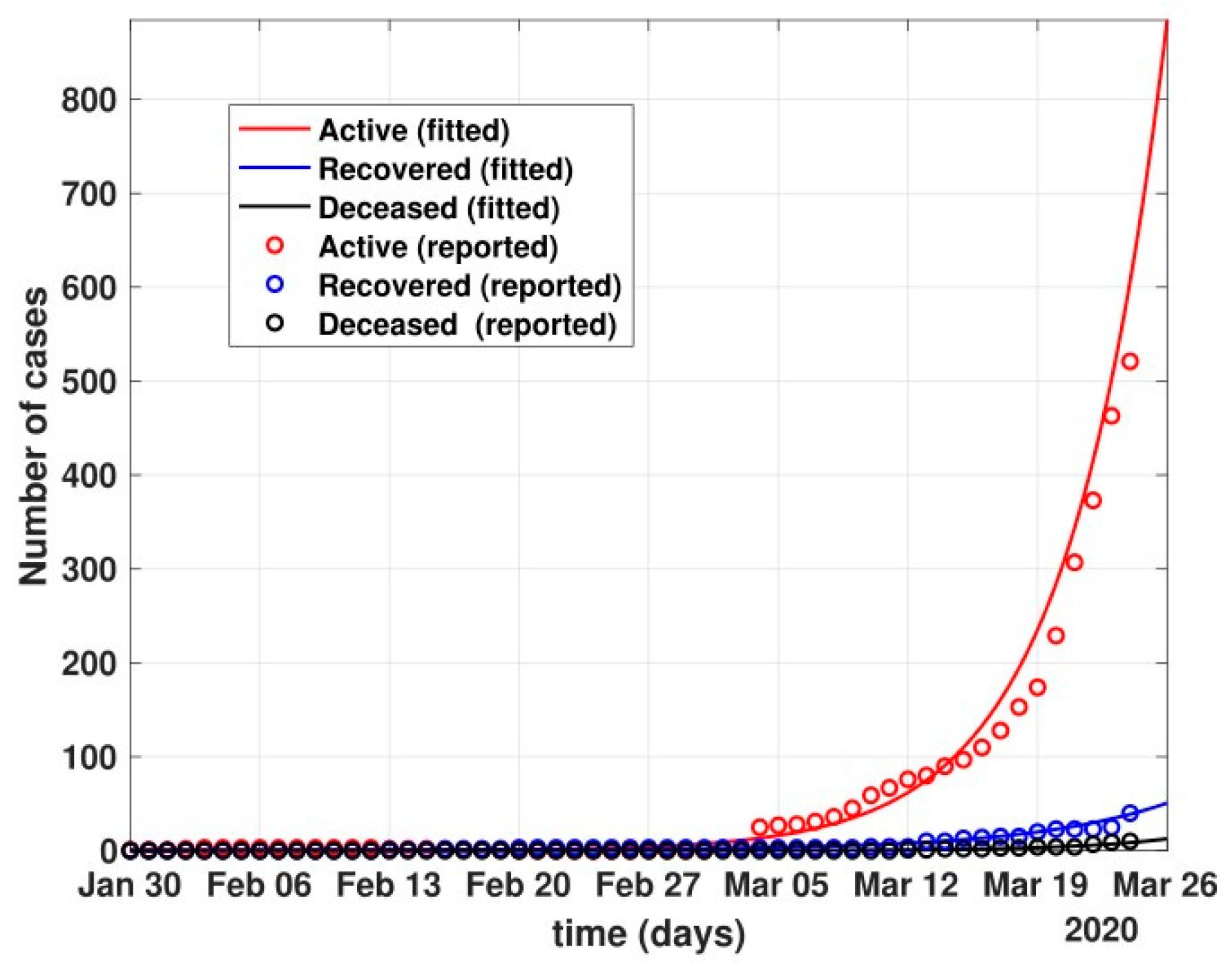
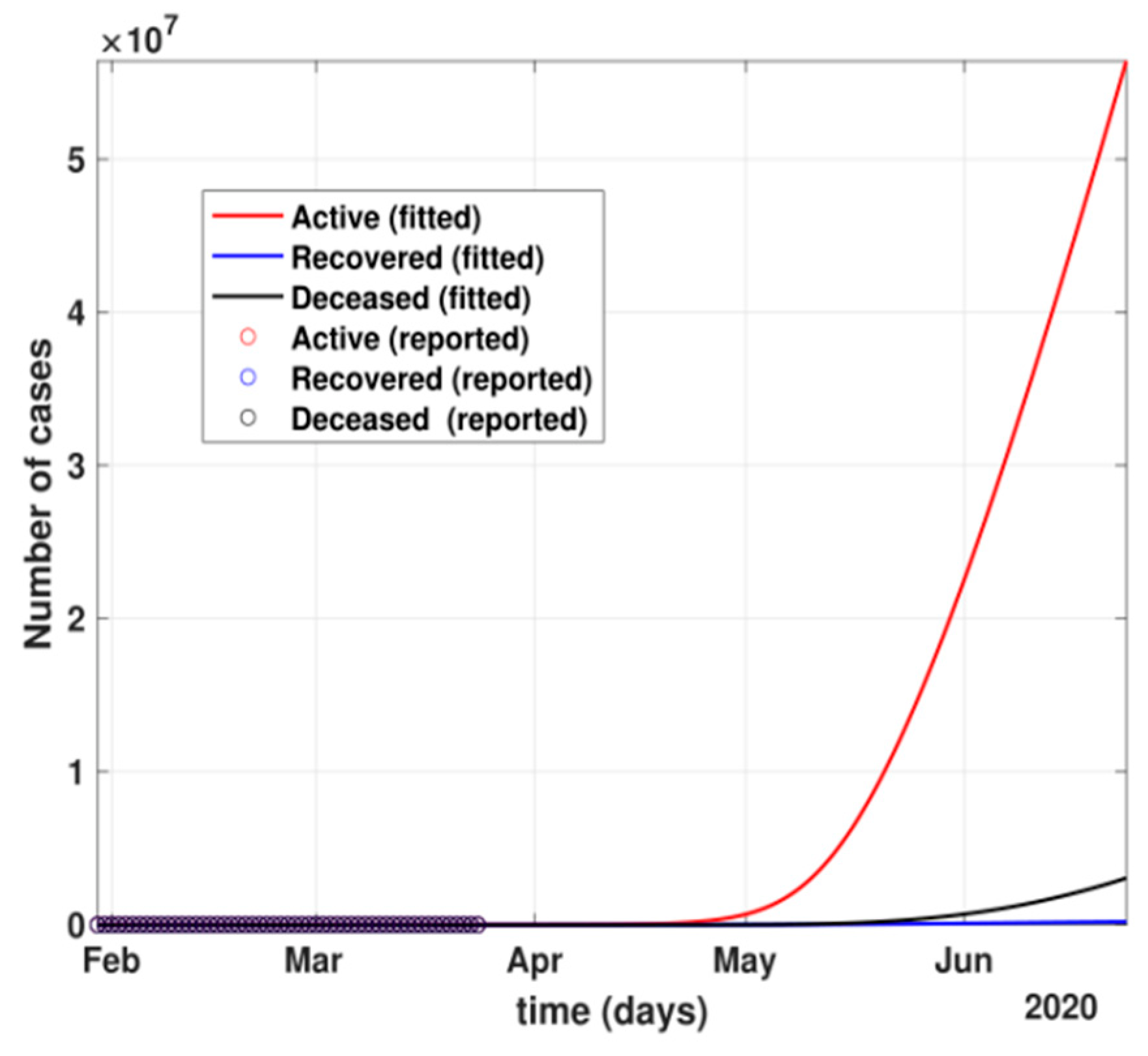
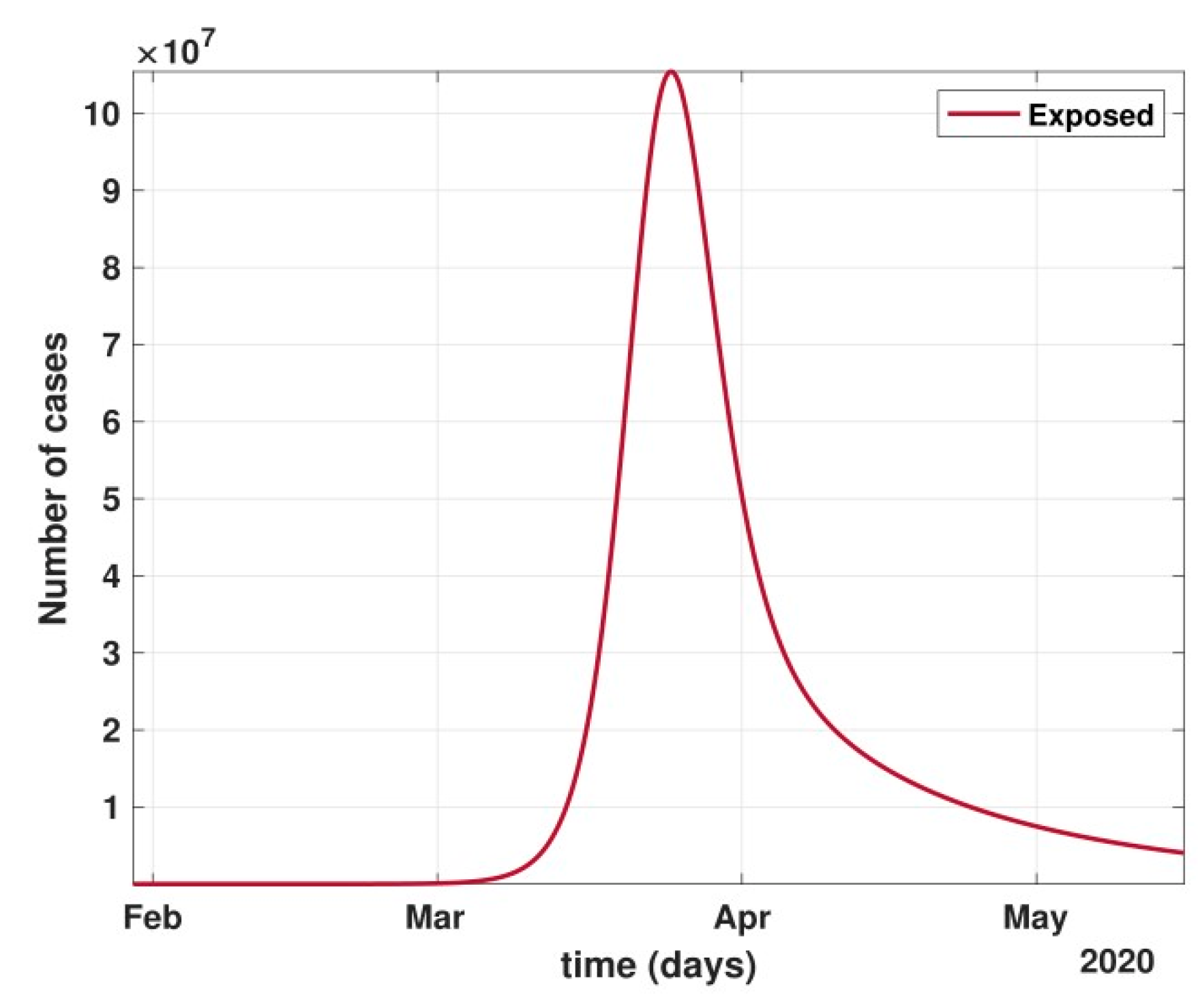
- The figure also shows the approximate huge number of active cases in the scenario with no government and no public reactions. The proposed model fit for number of cases before 24 March 2020 can be seen in Figure 5. Before 24 March, when the total number of active cases doubled every three days, without any control policy measures and slow but existing (as is visible from the transmission rates β and β1 values) public health perception such as washing hands regularly, etc., the peak of active cases was nowhere to be seen in near four months, as shown in Figure 6.
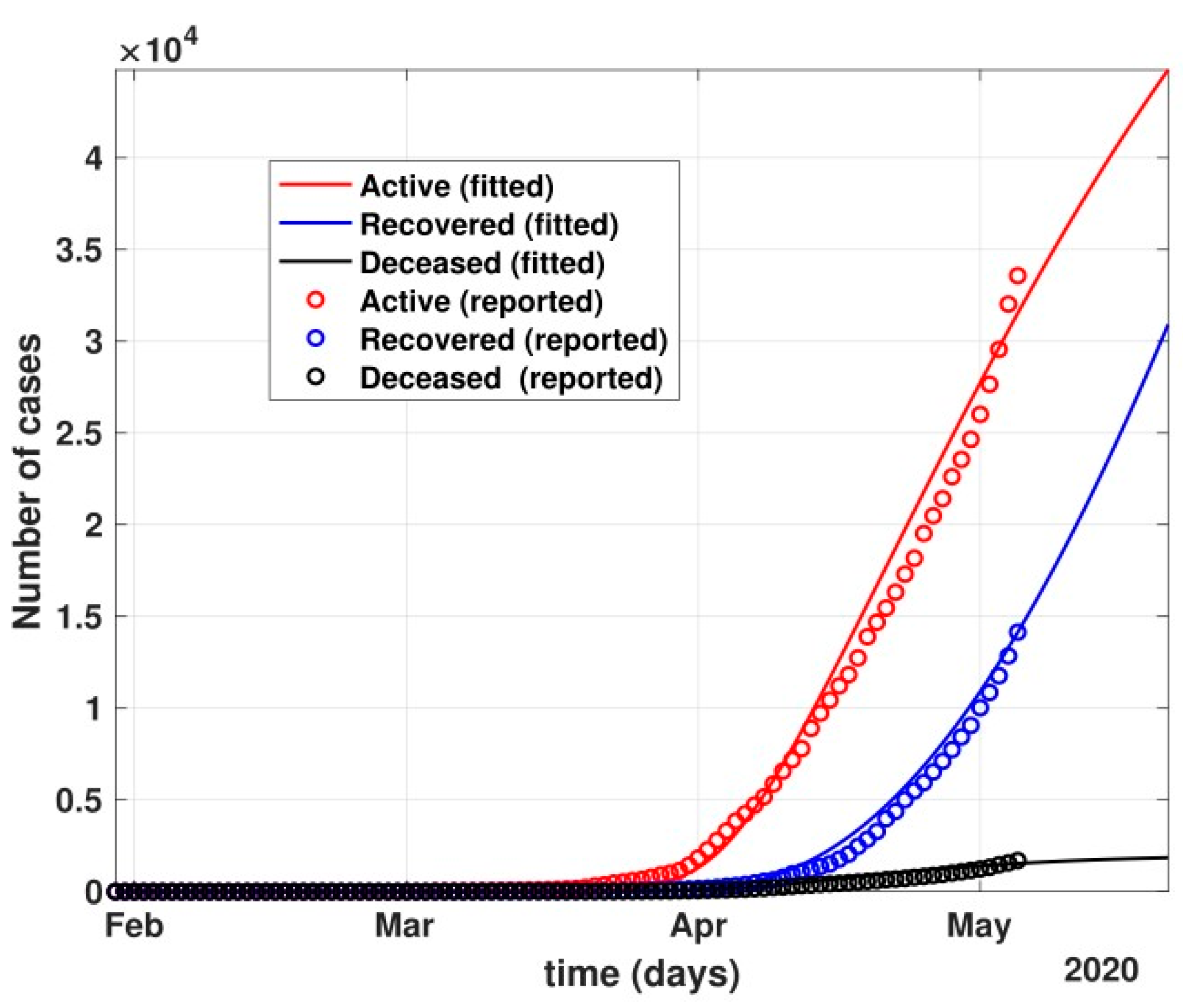
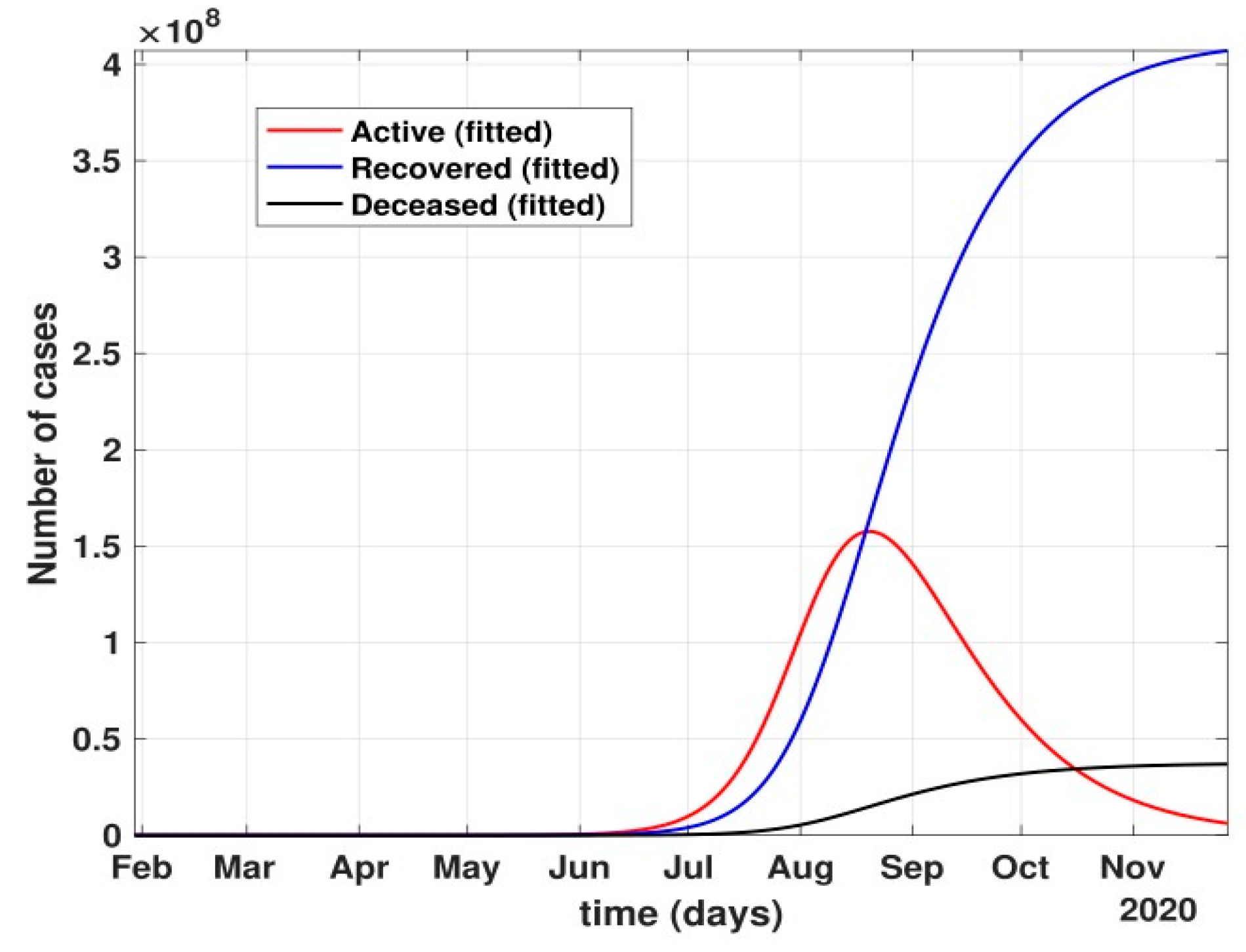
- Between 24 March and 4 May 2020, a time of two consecutive strict lockdowns in the country, there was a steady growth in the total number of active cases. When these data were fitted to the proposed model described in system (1) (shown in Figure 7), the curve of cumulative active cases intersected the curve of recovered cases in June 2020 and started further flattening, as is visible in Figure 8.
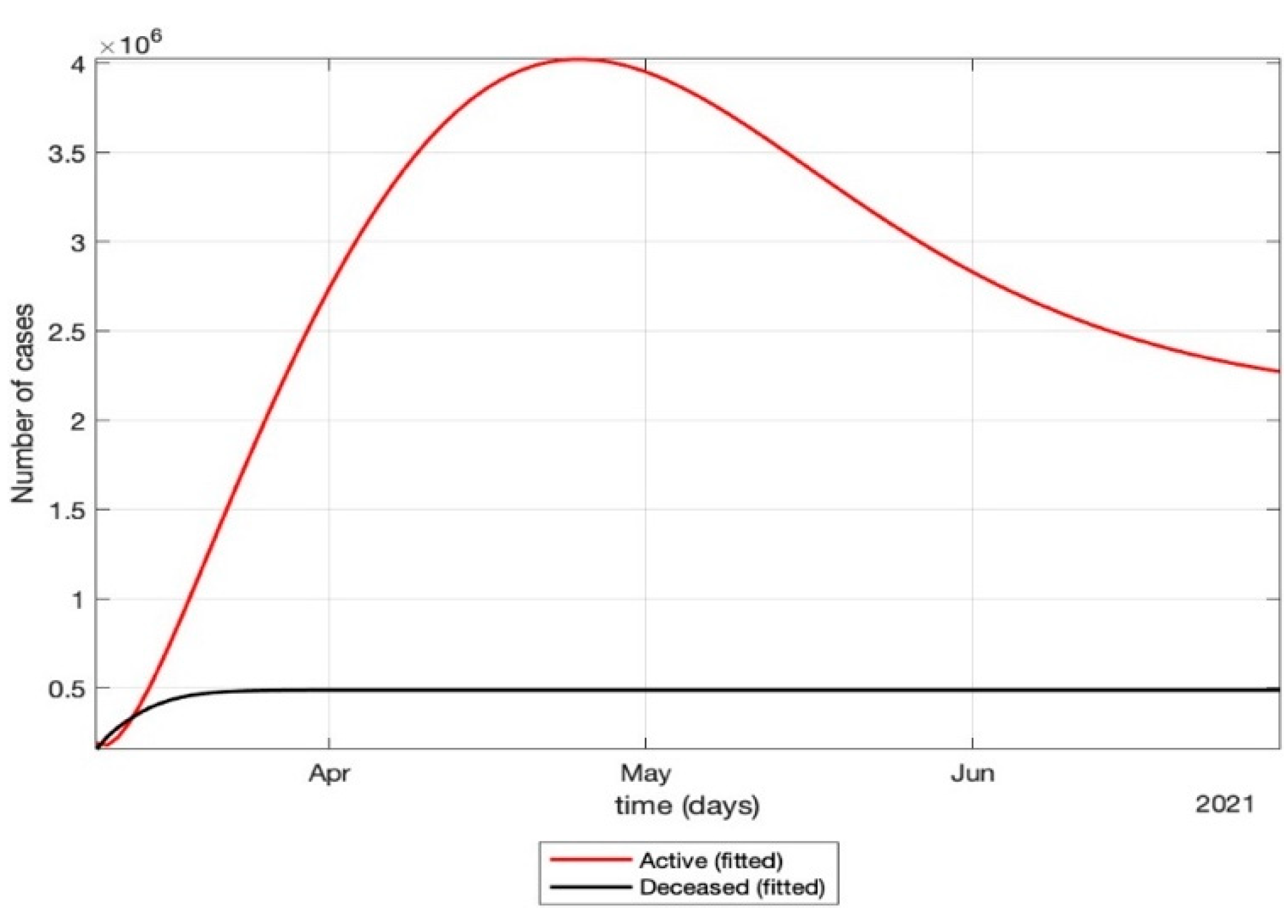
- The total number of active cases again increased in April 2021, as shown in Figure 9. Further, with the governmental control policies and public perception of COVID-19, the appropriate behavior was seen in terms of the number of active cases decreasing in the month of June 2021. As shown in Figure 10, the number of active cases and number of deaths during the second wave were much higher compared to that of the first wave, even with government control policies.
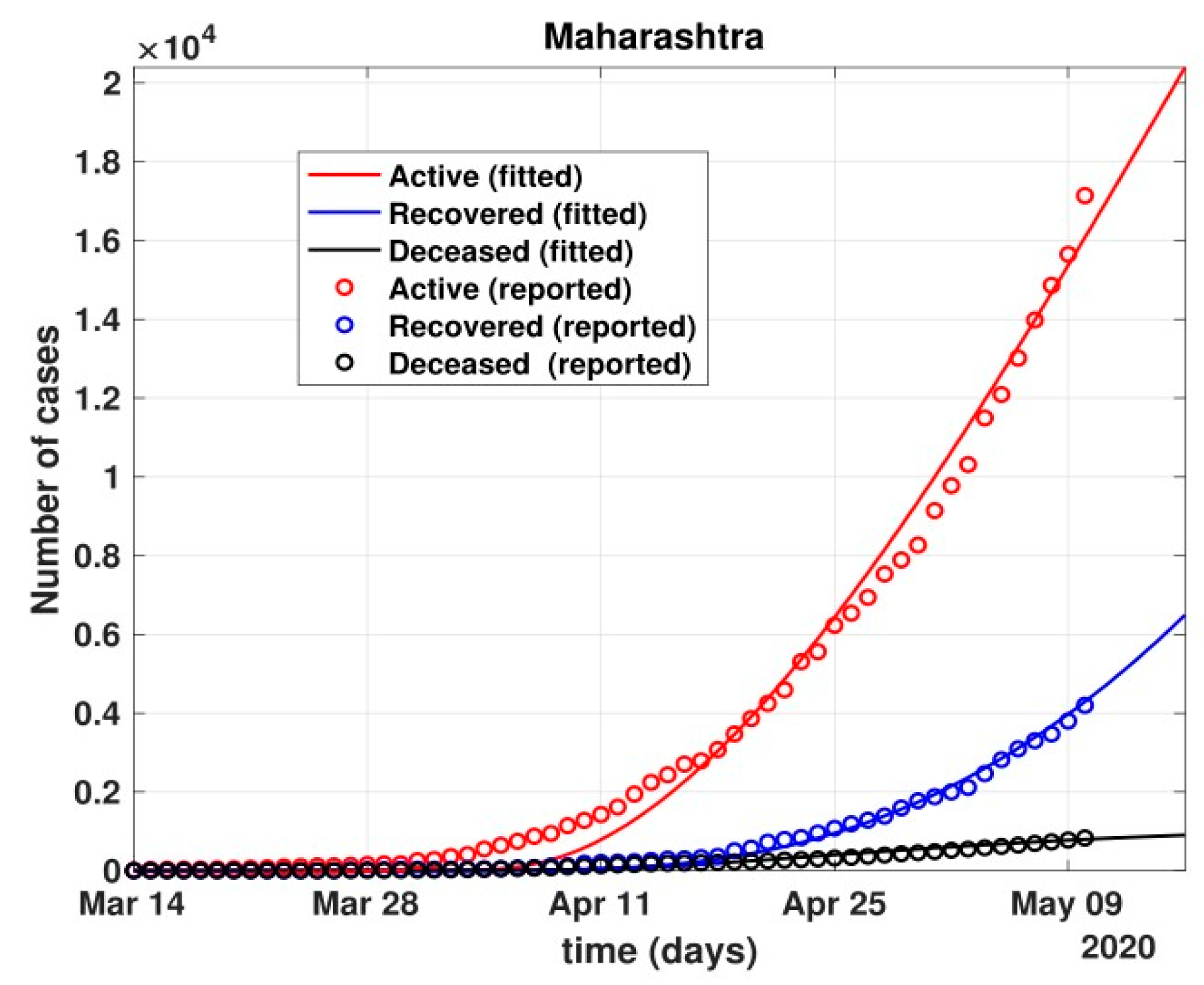
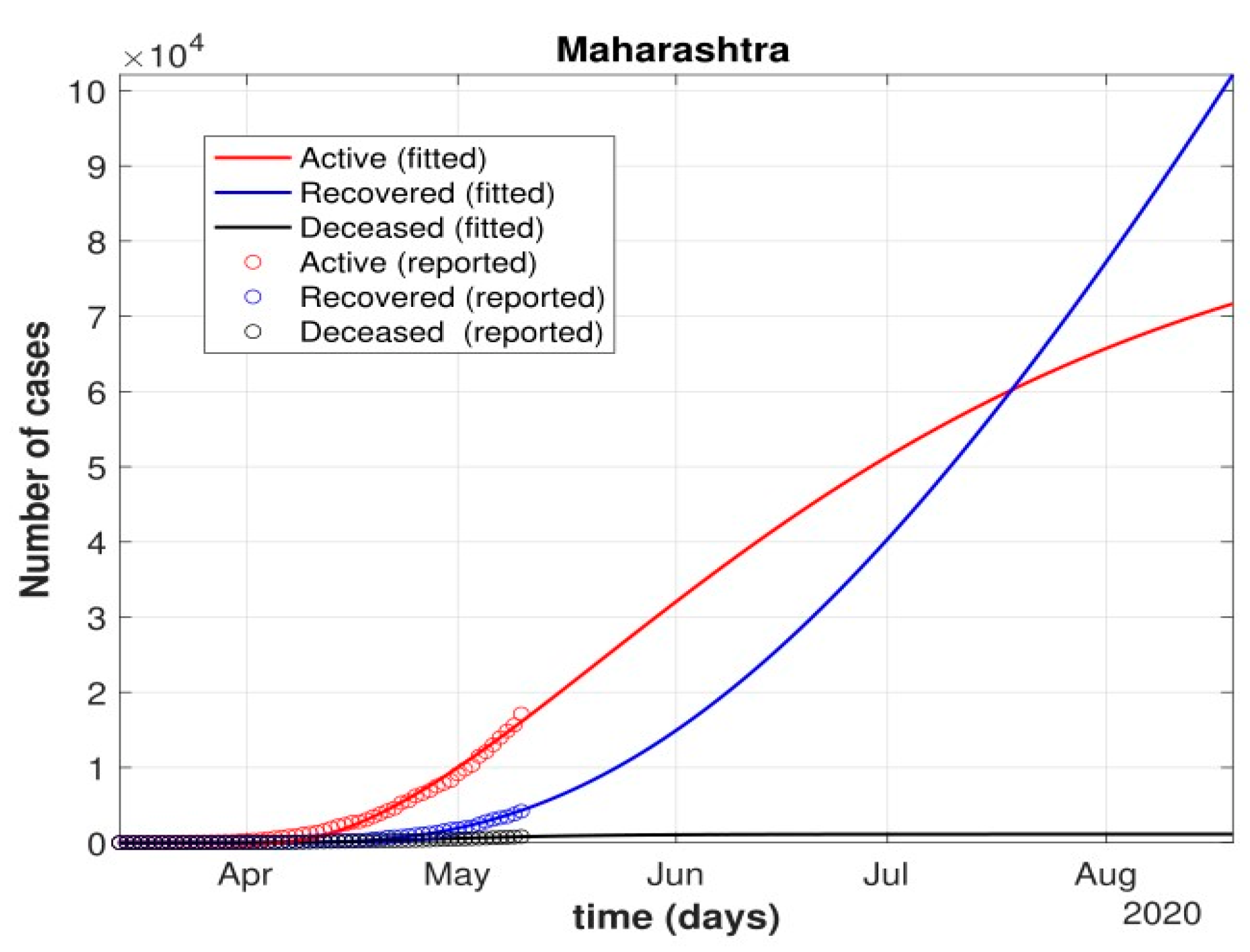
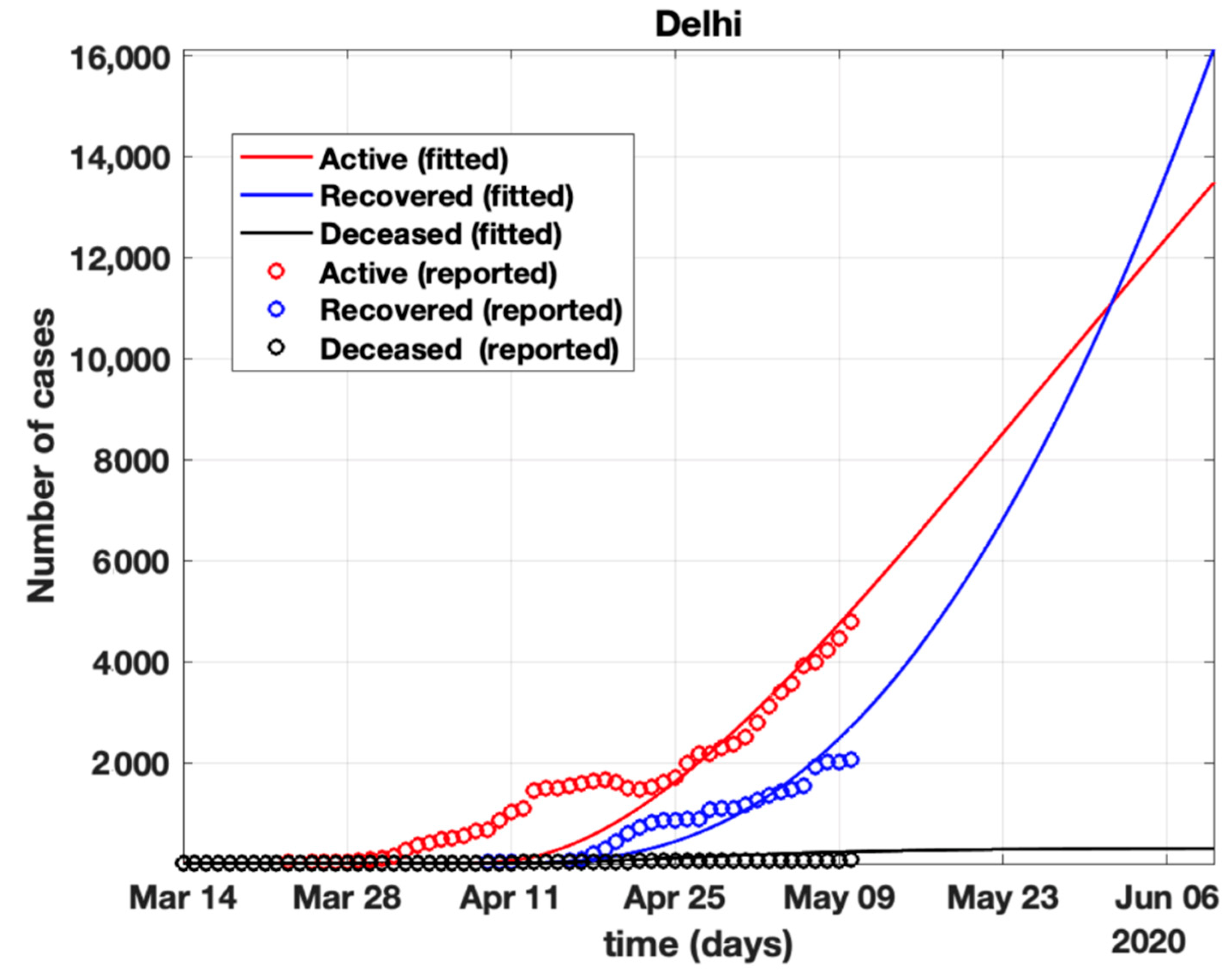
- Further, analysis for four Indian states, namely Maharashtra, Rajasthan, Kerala, and Delhi, was carried out. The proposed model was fitted to the data of COVID-19 confirmed cases, recovered cases, and deceased cases until 11 May 2020, from these four states, as shown in Figure 11, Figure 12, Figure 13, Figure 14, Figure 15 and Figure 16, respectively. Note that after 4 May 2020, the lockdown was opening up in many parts of these four states [12].
- The model when applied to the data of the number of coronavirus cases in 2021 in India. It was found that for the second wave, the transmission rate was quite high for both symptomatic and asymptomatic individuals, i.e., 0.7 and 0.96, respectively. Further, the mean time in which an infected individual entered the hospitalized compartment was found to be three days.
5. Discussions
- After 24 March, if the country was to have policies of governmental control, including the shutdown of educational institutes public recreational zones such as gyms, spas, and multiplex theatres, and public health safety measures such as compulsory wearing of mask and frequent hand washing then the analysis for such a scenario is carried out by first estimating the value of b = 0.0543 from the number of active cases till 24 March by fitting the real data to an exponential curve in MATLAB and then setting k = 5 and k1 = 15 to obtain the transmission rates from an infected individual to a susceptible individual and from a latent carrier (E) to a susceptible individual. It may be noted that the reason behind the choice of k1 = 15 is that most of the residential areas in India are densely populated with 7–15 people living in an average of one household. The curve of the active number of cases begins flattening in August with far more active cases, as seen in Figure 9 than the healthcare capacity. The result of such an analysis is far from the reality now. This suggests that the concept of partial control actions from the government among the public are not at all sufficient to control this pandemic in a densely populated and vastly dynamic country such as India. Therefore, a long period of strict lockdown (25 March to 4 May 2020) was essential to keep the highly infectious disease situation under control.
- The value of δ was found to be 0.13, which implies that only 13% of the total infected people moved from the state I to H. This implies that only 13% of the infected detected people were taken to the hospital, and rest of them did not require hospitalization, as they were asymptomatic or had mild symptoms. This is in line with the recent report of the Indian Council of Medical Research [12] that 85% of all COVID-19 confirmed cases in India were asymptomatic or had mild symptoms and mostly did not require hospitalization.
- Under policy-controlled measures such as lockdown and public health measures such as social distancing, frequently washing hands and the use of masks all the time will be beneficial in bending the curve of cumulative Active cases sooner, as is visible in Figure 8, under the strict lockdown phase from 25 March to 4 May 2020. It is clearly seen from Figure 8 that under strict policy measures as well as from a public health perspective, the curves of cumulative Active cases intersect the curve of the recovered cases in June and then start further flattening.
- An analysis of the proposed model was carried out under the presence of partial governmental policy measures and effective public health safety measures such as frequent hand washing, the use of face masks all the time, and maintaining social distancing among the general public, after the period of strict lockdown (after 4 May 2020). Value of b was obtained and was found to be equal to 0.0645 by fitting with the active cases data till 11 May and thereafter setting k = 5 and k1 = 15. The result, as shown in Figure 10, suggests that it would take a long time to further bend the curve of Active cases in India by August 2020. This delay may be a result of a sudden increase in the number of confirmed cases in India between 5 May and 11 May. This increase may be due to the huge migration of migrant workers from one city to another, in addition to the easing out of the lockdown in many places across the country. The increase in the number of daily confirmed cases between 5 May and 11 May 2020 may also be a result of increased testing of migrant workers. It may be noted that the choice of k1 = 15 in order to carry out such analysis is due to the fact that most of the residential areas in India are densely populated, with 7–15 people on average living in one household.
- Lockdowns have certainly delayed the peak, or eliminated the peak altogether, in cases of stringent public health measures such as social distancing, washing hands frequently, and the use of masks all the time.
- There are a large number of people in the carrier class/latent population (E), which saw a drastic decline during the strict lockdown period from 24 March to 4 May 2020 (as shown in Figure 10). These individuals are asymptomatic and infectious but the virus is not yet detected in them. This may be attributed to the compactness of the domestic settlements in and around the hotspot virus-affected areas of India. This re-implies that in the absence of a vaccine or an anti-viral drug, both government policy measures and public health safety perspective (controlled by k and k1) should be in place to control spread of the highly infectious COVID-19 in a multi-dynamical country such as India.
- The states of Rajasthan and Kerala are already witnessing the downfall of the coronavirus epidemic, as seen in Figure 14 and Figure 15. On the other hand, the states of Delhi and Maharashtra will take some time before their number of recovered cases is greater than their active cases, as is visible in Figure 13 and Figure 16.
- Finally, a prediction of the number of COVID-19 cases during the second wave in 2021 is depicted in Figure 11. The graph shows a peak in the coronavirus cases at the end of April and a decrease in number of cases in June 2021. This prediction is comparable to the real scenario during the second wave in India. This prediction is based on the government control measures in place, as well as the fact that the public safety perspective is higher. However, the number of active cases, i.e., individuals who require hospitalization, is very high, and the number of deaths is also very high compared to the first wave, even with various government control policies in place.
- The calculation is primarily based on the two different effective contact rates for asymptomatic and symptomatic individuals. These are proportional to the number of contacts that an individual has per day depending on government policies such as lockdown and closure of public places. The other two parameters are time-dependent mortality and recovery rates, which are data-driven and may depend on dynamic factors such as geographical location, weather conditions, and settlements specific to India. The spread can be controlled by controlling the first two parameters by strict government policy and responsible behavior by the public, which could bring down the first two parameters significantly. This is evident in the case of both the first and the second waves of COVID-19.
- It may be noted that the parameters of transmission rates and mean time of hospitalization for an individual, when compared to the first wave of COVID-19 in India, are quite high, which may be the cause of a huge number of active cases during the second wave in India putting a pressure on the medical resources of the country even during the second wave of COVID-19 in India.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yunfeng, S.; Haiwei, L.; Ren, Z. Effects of Pandemic Outbreak on Economies: Evidence from Business History Context. Front. Public Health 2021, 9, 632043. [Google Scholar]
- The Editors of Encyclopaedia Britannica. Black Death. Encyclopedia Britannica. 2022. Available online: https://www.britannica.com/event/Black-Death (accessed on 15 March 2022).
- Vaibhav, B.; Poonia, R.C.; Nagar, P.; Kumar, S.; Singh, V.; Raja, L.; Dass, P. Descriptive analysis of COVID-19 patients in the context of India. J. Interdiscip. Math. 2021, 24, 489–504. [Google Scholar]
- Sunil, C.; Mittal, M.; Chawla, M.; Goyal, L. Corona virus-SARS-CoV-2: An insight to another way of natural disaster. EAI Endorsed Trans. Pervasive Health Technol. 2020, 6, e2. [Google Scholar]
- Platt, C. King Death: The Black Death and its Aftermath in Late-Medieval England; Routledge: Abingdon-on-Thames, UK, 2014. [Google Scholar]
- DeWitte, S.N. Mortality risk and survival in the aftermath of the medieval Black Death. PLoS ONE 2014, 9, e96513. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Petkova, E.; Shaman, J. The 1918 influenza pandemic in New York City: Age-specific timing, mortality, and transmission dynamics. Influenza and Other Respiratory Viruses. Natl. Inst. Health 2013, 8, 177–188. [Google Scholar] [CrossRef]
- Simon, D.; McDonald, S.; Roberts, J. AIDS and economic growth in Africa: A panel data analysis. J. Int. Dev. J. Dev. Stud. Assoc. 2001, 13, 411–426. [Google Scholar]
- Frieden, N.M. The Russian Cholera Epidemic, 1892–1893, and Medical Professionalization. J. Soc. Hist. 1977, 10, 538–559. [Google Scholar] [CrossRef]
- Warren, J. Jared Diamond, Guns, Germs and Steel: The Fates of Human Societies. J. Mil. Strateg. Stud. 2001, 4, 79–81. [Google Scholar]
- Keogh-Brown, M.R.; Smith, R.D. The economic impact of SARS: How does the reality match the predictions? Health Policy 2008, 88, 110–120. [Google Scholar] [CrossRef]
- Achonu, C.; Laporte, A.; Gardam, M.A. The financialimpact of controlling a respiratory virus outbreak in a teaching hospital. Can. J. Public Health 2005, 96, 52–54. [Google Scholar] [CrossRef]
- Michele, T.; Bajardi, P.; Poletto, C.; Ramasco, J.J.; Balcan, D.; Gonçalves, B.; Perra, N.; Colizza, V.; Vespignani, A. Real-time numerical forecast of global epidemic spreading: Case study of 2009 A/H1N1pdm. BMC Med. 2012, 10, 165. [Google Scholar]
- Seema, J.; Kamimoto, L.; Bramley, A.M.; Schmitz, A.M.; Benoit, S.R.; Louie, J.; Sugerman, D.E.; Druckenmiller, J.K.; Ritger, K.A.; Chugh, R.; et al. Hospitalized patients with 2009 H1N1 influenza in the United States, April–June 2009. N. Engl. J. Med. 2009, 361, 1935–1944. [Google Scholar]
- Sharma, A.; Agarwal, B. A cyber-physical system approach for model based predictive control and modeling of COVID-19 in India. J. Interdiscip. Math. 2021, 24, 1–18. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- The Economic Times Mirror Now. Time to Re-Open Delhi, People Will Have to Be Ready to Live with Coronavirus: C M kejri-wal. Available online: https://www.business-standard.com/article/current-affairs/time-to-reopen-delhi-live-with-virus-120050400054_1.html (accessed on 5 May 2020).
- Bernoulli, D. Essai d’une nouvelle analyse de la mortalité causée par la petite verole et des avantages de l’inoculation pour la prevenir. Mem. Math. Phys. Acad. Roy. Sci. 1766, 1–45. Reprinted in; In Histoire de l’Academie Royale des Sciences; Haberman, S., Sibbett, T.A., Eds.; William Pickering: London, UK, 1995. [Google Scholar]
- Ogilvy, K.W.; McKendrick, A.G. A contribution to the mathematical theory of epidemics. Proc. R. Soc. Lond. A 1927, 115, 115700–1157721. [Google Scholar]
- Dietz, K.; Heesterbeek, J.A.P. Daniel Bernoulli’s epidemiological model revisited. Math. Biosci. 2002, 180, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernández-Flix, S.; de Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Andreychuk, N.; et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PLoS ONE 2021, 16, e0248029. [Google Scholar] [CrossRef]
- Lu, J. A new, simple projection model for COVID-19 pandemic. medRxiv 2020, preprint. [Google Scholar]
- Pierre, M.; Webb, G. Predicting the number of reported and unreported cases for the COVID-19 epidemic in South Korea, Italy, France and Germany. 2020. Available online: https://ssrn.com/abstract=3557360 (accessed on 30 April 2020).
- Bekiros, S.; Kouloumpou, D. Sbdiem: A new mathematical model of infectious disease dynamics. Chaos Solitons Fractals 2020, 136, 109828. [Google Scholar] [CrossRef]
- Victor, A. Mathematical predictions for COVID-19 as a global pandemic. medRxiv 2020. preprint. [Google Scholar] [CrossRef]
- Toda, A.A. Susceptible-infected-recovered (SIR) dynamics of Covid-19 and economic impact. arXiv 2020, arXiv:2003.11221. [Google Scholar]
- Caccavo, D. Chinese and italian covid-19 outbreaks can be correctly described by a modified sird model. medRxiv 2020, preprint. [Google Scholar]
- Jia, W.; Ke, H.; Yang, S.; Wenzhe, C.; Shengshu, W.; Shanshan, Y.; Jianwei, W.; Kou, F.; Tai, P.; Li, J.; et al. Extended SIR prediction of the epidemics trend of COVID-19 in Italy and compared with Hunan, China. Front. Med. 2020, 7, 169. [Google Scholar]
- Chandra, P.R.; Dass, P.; Raja, L.; Bhatnagar, V.; Prasad, J. The Review of Prediction Models for COVID-19 Outbreak in Indian Scenario. In Proceedings of the Third International Conference on Sustainable Computing, Jaipur, India, 19–20 March 2021; Springer: Singapore, 2022; pp. 567–576. [Google Scholar]
- Sameni, R. Mathematical modeling of epidemic diseases; a case study of the COVID-19 coronavirus. arXiv 2020, arXiv:2003.11371. [Google Scholar]
- Kaustuv, C.; Chatterjee, K.; Kumar, A.; Shankar, S. Healthcare impact of COVID-19 epidemic in India: A stochastic mathematical model. Med. J. Armed Forces India 2020, 76, 147–155. [Google Scholar]
- Dowd, J.B.; Andriano, L.; Brazel, D.M.; Ro-tondi, V.; Block, P.; Ding, X.; Liu, Y.; Mills, M.C. Demo-graphic science aids in understanding the spread and fatality rates of covid-19. Proc. Natl. Acad. Sci. USA 2020, 117, 9696–9698. [Google Scholar]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- Amitava, B.; Pasea, L.; Harris, S.; Gonzalez-Izquierdo, A.; Torralbo, A.; Shallcross, L.; Noursadeghi, M.; Pillay, D.; Sebire, N.; Holmes, C.; et al. Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: A population-based cohort study. Lancet 2020, 395, 1715–1725. [Google Scholar]
- Kucharski, A.J.; Russell, T.W.; Diamond, C.; Liu, Y.; Edmunds, J.; Funk, S.; Eggo, R.M.; Sun, F.; Jit, M.; Munday, J.D.; et al. Early dynamics of transmission and control of COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 553–558. [Google Scholar] [CrossRef] [Green Version]
- Gaurav, P.; Chaudhary, P.; Gupta, R.; Pal, S. SEIR and Regression Model based COVID-19 outbreak predictions in India. arXiv 2020, arXiv:2004.00958. [Google Scholar]
- Youssoufa, M.; Halidou, A.; Kapen, P.T. A review of mathematical modeling, artificial intelligence and datasets used in the study, prediction and management of COVID-19. Appl. Intell. 2020, 50, 3913–3925. [Google Scholar]
- Luo, J. When Will COVID-19 End? Data-Driven Prediction. Singapore University of Technology and Design. 2020. Available online: http://www.sutd.edu.sg (accessed on 30 November 2021).
- Liangrong, P.; Yang, W.; Zhang, D.; Zhuge, C.; Hong, L. Epidemic analysis of COVID-19 in China by dynamical modeling. arXiv 2020, arXiv:2002.06563. [Google Scholar]
- Zifeng, Y.; Zeng, Z.; Wang, K.; Wong, S.; Liang, W.; Zanin, M.; Liu, P.; Cao, X.; Gao, Z.; Mai, Z.; et al. Modified SEIR and AI prediction of the epidemics trend of COVID-19 in China under public health interventions. J. Thorac. Dis. 2020, 12, 165. [Google Scholar]
- Jinming, C.; Jiang, X.; Zhao, B. Mathematical modeling and epidemic prediction of COVID-19 and its significance to epidemic prevention and control measures. J. Biomed. Res. Innov. 2020, 1, 1–19. [Google Scholar]
- Otunuga, O.M.; Ogunsolu, M.O. Qualitative anal-ysis of a stochastic seitr epidemic model with multiple stages of infectionand treatment. Infect. Dis. Model. 2020, 5, 61–90. [Google Scholar] [PubMed]
- Soniya, L.; Sahni, G.; Mewara, B.; Kumar, R. Predicting optimal lockdown period with parametric approach using three-phase maturation SIRD model for COVID-19 pandemic. Chaos Solitons Fractals 2020, 138, 109939. [Google Scholar]
- Ghosh, A.; Roy, S.; Mondal, H.; Biswas, S.; Bose, R. Mathematical modelling for decision making of lockdown during COVID-19. Appl. Intell. 2022, 52, 699–715. [Google Scholar] [CrossRef]
- Swapnarekha, H.; Behera, H.S.; Nayak, J.; Naik, B. Role of intelligent computing in COVID-19 prognosis: A state-of-the-art review. Chaos Solitons Fractals 2020, 138, 109947. [Google Scholar] [CrossRef]
- Kotwal, A.; Yadav, A.K.; Yadav, J.; Kotwal, J.; Khune, S. Predictive models of COVID-19 in India: A rapid review. Med. J. Armed Forces India 2020, 76, 377–386. [Google Scholar] [CrossRef]
- Park, M.; Cook, A.R.; Lim, J.T.; Sun, Y.; Dickens, B.L. A systematic review of COVID-19 epidemiology based on current evidence. J. Clin. Med. 2020, 9, 967. [Google Scholar] [CrossRef] [Green Version]
- Harjule, P.; Rahman, A.; Agarwal, B. A cross-sectional study of anxiety, stress, perception and mental health towards online learning of school children in India during COVID-19. J. Interdiscip. Math. 2021, 24, 411–424. [Google Scholar] [CrossRef]
- Kermack, W.O.; McKendrick, A.G. Contributions to the mathematical theory of epidemics—I. 1927. Bull. Math. Biol. 1991, 53, 33–55. [Google Scholar] [PubMed]
- National Portal of India. Available online: https://main.icmr.nic.in/content/covid-19 (accessed on 12 May 2020).
- Covidindia Data. Available online: https://www.covid19india.org (accessed on 10 May 2020).
- He, D.; Dushoff, J.; Day, T.; Ma, J.; Earn, D.J.D. Inferring the causes of the three waves of the 1918 influenza pandemic in England and Wales. Proc. R. Soc. B Biol. Sci. 2013, 280, 20131345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
















| Place | Total Number of Active Cases | Total Number of Recovered Cases | Total Number of Deaths |
|---|---|---|---|
| India | 30,889 | 12,410 | 1522 |
| Maharashtra | 12,974 | 2115 | 548 |
| Rajasthan | 1500 | 2250 | 40 |
| Kerala | 34 | 462 | 3 |
| Delhi | 4549 | 1362 | 64 |
| S.no. | Coefficient | Meaning | Remark |
|---|---|---|---|
| 1 | β = k.b | Transmission rate from S to I. | Estimated |
| 2 | k | Total number of contacts, (effective), per day of an infected person. | Policy dependent |
| 3 | b | Probability of infection between infectious and susceptible individual. | To be fitted |
| 4 | β1 = k1.b1 | Transmission rate from S to E. | Estimated. |
| 5 | k1 | Total number of contacts, (effective), per day of an exposed individual. | Policy dependent |
| 6 | b1 | Probability of infection between carrier(E) and susceptible individual | Estimated |
| 7 | γ − 1 | Mean time for an individual to go from E to I. | To be fitted |
| 8 | δ − 1 | Mean time for an individual to go from I to H compartment. | To be fitted |
| 9 | κ(t) | Mortality rate (time-dependent). | To be fitted |
| 10 | λ(t) | Recovery rate (time-dependent). | To be fitted |
| S.No. | Coefficient | Value before 24 March | Value after 24 March |
|---|---|---|---|
| 1 | β | 0.455 | 0.41755 |
| 2 | k | 10 | 5 |
| 3 | b | 0.0455 | 0.08351 |
| 4 | β1 | 0.91 | 0.8351 |
| 5 | k1 | 20 | 10 |
| 6 | b1 | 0.0455 | 0.08351 |
| 7 | γ − 1 | 5 days | 5 days |
| 8 | δ − 1 | 4 days | 7 days |
| 9 | κ(t) | 0.05% | 1.02% |
| 10 | λ(t) | 5% | 26% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harjule, P.; Poonia, R.C.; Agrawal, B.; Saudagar, A.K.J.; Altameem, A.; Alkhathami, M.; Khan, M.B.; Hasanat, M.H.A.; Malik, K.M. An Effective Strategy and Mathematical Model to Predict the Sustainable Evolution of the Impact of the Pandemic Lockdown. Healthcare 2022, 10, 759. https://doi.org/10.3390/healthcare10050759
Harjule P, Poonia RC, Agrawal B, Saudagar AKJ, Altameem A, Alkhathami M, Khan MB, Hasanat MHA, Malik KM. An Effective Strategy and Mathematical Model to Predict the Sustainable Evolution of the Impact of the Pandemic Lockdown. Healthcare. 2022; 10(5):759. https://doi.org/10.3390/healthcare10050759
Chicago/Turabian StyleHarjule, Priyanka, Ramesh Chandra Poonia, Basant Agrawal, Abdul Khader Jilani Saudagar, Abdullah Altameem, Mohammed Alkhathami, Muhammad Badruddin Khan, Mozaherul Hoque Abul Hasanat, and Khalid Mahmood Malik. 2022. "An Effective Strategy and Mathematical Model to Predict the Sustainable Evolution of the Impact of the Pandemic Lockdown" Healthcare 10, no. 5: 759. https://doi.org/10.3390/healthcare10050759