
Effects of Occlusal Splints on Spinal Posture in Patients with Temporomandibular Disorders: A Systematic Review

 , , , , , and
, , , , , and
Abstract
:1. Introduction
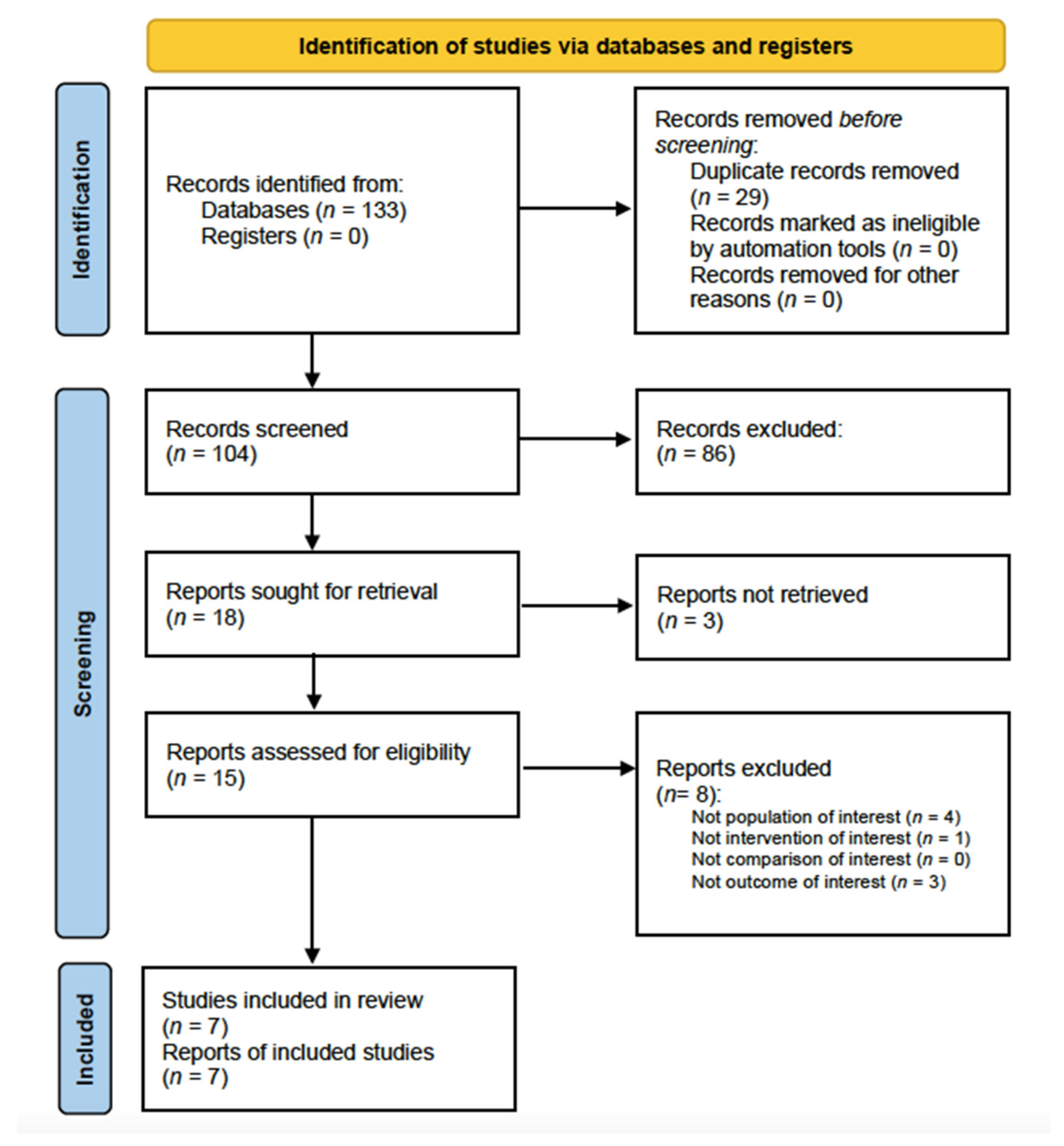
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Data Synthesis
3. Results
3.1. Main Characteristics of the Included Studies
3.2. Occlusal Splints
3.3. Posture Analysis
3.4. Risk-of-Bias Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Okeson, J.P. Bell’s Oral and Facial Pain (Formerly Bell’s Orofacial Pain). Stomatol. Edu. J. 2016, 3, 250. [Google Scholar] [CrossRef]
- Schiffman, E.L.; Truelove, E.L.; Ohrbach, R.; Anderson, G.C.; John, M.T.; List, T.; Look, J.O. The Research Diagnostic Criteria for Temporomandibular Disorders. I: Overview and methodology for assessment of validity. J. Orofac. Pain 2010, 24, 7. [Google Scholar] [PubMed]
- Diraçoglu, D.; Yildirim, N.K.; Saral, I.; Özkan, M.; Karan, A.; Özkan, S.; Aksoy, C. Temporomandibular dysfunction and risk factors for anxiety and depression. J. Back Musculoskelet. Rehabil. 2016, 29, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Ammendolia, A.; Paduano, S.; Calafiore, D.; Marotta, N.; Migliario, M.; Fortunato, L.; Giudice, A.; Michelotti, A.; de Sire, A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. 2022, 18, 1–16. [Google Scholar] [CrossRef]
- Yan, Z.B.; Wan, Y.D.; Xiao, C.Q.; Li, Y.Q.; Zhang, Y.Y.; An, Y.; Xiong, X. Craniofacial Morphology of Orthodontic Patients with and without Temporomandibular Disorders: A Cross-Sectional Study. Pain Res. Manag. 2022, 2022, 9344028. [Google Scholar] [CrossRef]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef]
- Montinaro, F.; Nucci, L.; d’Apuzzo, F.; Perillo, L.; Chiarenza, M.C.; Grassia, V. Oral nonsteroidal anti-inflammatory drugs as treatment of joint and muscle pain in temporomandibular disorders: A systematic review. Cranio 2022, 7, 1–10. [Google Scholar] [CrossRef]
- Singh, H.; Sunil, M.K.; Kumar, R.; Singla, N.; Dua, N.; Garud, S.R. Evaluation of TENS therapy and Placebo drug therapy in the management of TMJ pain disorders: A comparative study. J. Indian Acad. Oral Med. Radiol. 2014, 26, 139–144. [Google Scholar] [CrossRef]
- Marotta, N.; Ferrillo, M.; Demeco, A.; Drago Ferrante, V.; Inzitari, M.T.; Pellegrino, R.; Pino, I.; Russo, I.; de Sire, A.; Ammendolia, A. Effects of Radial Extracorporeal Shock Wave Therapy in Reducing Pain in Patients with Temporomandibular Disorders: A Pilot Randomized Controlled Trial. Appl. Sci. 2022, 12, 3821. [Google Scholar] [CrossRef]
- de Sire, A.; Marotta, N.; Ferrillo, M.; Agostini, F.; Sconza, C.; Lippi, L.; Respizzi, S.; Giudice, A.; Invernizzi, M.; Ammendolia, A. Oxygen-Ozone Therapy for Reducing Pro-Inflammatory Cytokines Serum Levels in Musculoskeletal and Temporomandibular Disorders: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 2528. [Google Scholar] [CrossRef]
- Alvarez-Arenal, A.; Junquera, L.M.; Fernández, J.P.; González, I.; Olay, S. Effect of occlusal splint and transcutaneous electric nerve stimulation on the signs and symptoms of temporomandibular disorders in patients with bruxism. J. Oral Rehabil. 2002, 29, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Al-Ani, Z.; Gray, R.J.; Davies, S.J.; Sloan, P.; Glenny, A.-M. Stabilization Splint Therapy for the Treatment of Temporomandibular Myofascial Pain: A Systematic Review. J. Dent. Educ. 2005, 69, 1242–1250. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, S.; Montoya, L.; Busse, J.W.; Carrasco-Labra, A.; Guyatt, G.H. The effectiveness of splint therapy in patients with temporomandibular disorders. J. Am. Dent. Assoc. 2012, 143, 847–857. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Nucci, L.; Lanza, A.; Femiano, F.; Contaldo, M.; Grassia, V. Temporomandibular disc displacement with reduction treated with anterior repositioning splint: A 2-year clinical and magnetic resonance imaging (MRI) follow-up. J. Biol. Regul. Homeost. Agents 2020, 34, 151–160. [Google Scholar] [PubMed]
- Deregibus, A.; Ferrillo, M.; Piancino, M.G.; Domini, M.C.; de Sire, A.; Castroflorio, T. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turkish J. Phys. Med. Rehabil. 2021, 67, 32–40. [Google Scholar] [CrossRef]
- Michelotti, A.; Iodice, G.; Vollaro, S.; Steenks, M.H.; Farella, M. Evaluation of the short-term effectiveness of education versus an occlusal splint for the treatment of myofascial pain of the jaw muscles. J. Am. Dent. Assoc. 2012, 143, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Dalewski, B.; Kamińska, A.; Kiczmer, P.; Węgrzyn, K.; Pałka, Ł.; Janda, K.; Sobolewska, E. Pressure Algometry Evaluation of Two Occlusal Splint Designs in Bruxism Management-Randomized, Controlled Clinical Trial. J. Clin. Med. 2021, 10, 2342. [Google Scholar] [CrossRef]
- Dalewski, B.; Chruściel-Nogalska, M.; Frączak, B. Occlusal splint versus modified nociceptive trigeminal inhibition splint in bruxism therapy: A randomized, controlled trial using surface electromyography. Aust. Dent. J. 2015, 60, 445–454. [Google Scholar] [CrossRef] [Green Version]
- Ferrario, V.F.; Sforza, C. Biomechanical model of the human mandible in unilateral clench: Distribution of temporomandibular joint reaction forces between working and balancing sides. J. Prosthet. Dent. 1994, 72, 169–176. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Tartaglia, G.M.; Dellavia, C. Immediate effect of a stabilization splint on masticatory muscle activity in temporomandibular disorder patients. J. Oral Rehabil. 2002, 29, 810–815. [Google Scholar] [CrossRef]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral superior condylar neck fracture with dislocation in a child treated with an acrylic splint in the upper arch for functional repositioning of the mandible. Cranio-J. Craniomandib. Pract. 2017, 35, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Piancino, M.G.; Dalmasso, P.; Borello, F.; Cinnella, P.; Crincoli, V.; Garagiola, U.; de Biase, C.; Tonni, I.; Matacena, G.; Deregibus, A. Thoracic-lumbar-sacral spine sagittal alignment and cranio-mandibular morphology in adolescents. J. Electromyogr. Kinesiol. 2019, 48, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Gomes, L.; Horta, K.; Gonçalves, J.; Santos-Pinto, A. Systematic review: Craniocervical posture and craniofacial morphology. Eur. J. Orthod. 2014, 36, 55–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monzani, D.; Guidetti, G.; Chiarini, L.; Setti, G. Combined effect of vestibular and craniomandibular disorders on postural behaviour. Acta Otorhinolaryngol. Ital. 2003, 23, 4–9. [Google Scholar]
- Marini, I.; Alessandri Bonetti, G.; Bortolotti, F.; Bartolucci, M.L.; Gatto, M.R.; Michelotti, A. Effects of experimental insoles on body posture, mandibular kinematics and masticatory muscles activity. A pilot study in healthy volunteers. J. Electromyogr. Kinesiol. 2015, 25, 531–539. [Google Scholar] [CrossRef] [Green Version]
- Flores, H.F.; Ottone, N.E.; Fuentes, R. Analysis of the morphometric characteristics of the cervical spine and its association with the development of temporomandibular disorders. Cranio-J. Craniomandib. Pract. 2017, 35, 79–85. [Google Scholar] [CrossRef]
- Ortega-Santiago, R.; González-Aguado, Á.J.; Fernández-de-las-Peñas, C.; Cleland, J.A.; de-la-Llave-Rincón, A.I.; Kobylarz, M.D.; Plaza-Manzano, G. Pressure pain hypersensitivity and referred pain from muscle trigger points in elite male wheelchair basketball players. Braz. J. Phys. Ther. 2020, 24, 333–341. [Google Scholar] [CrossRef]
- Hong, S.W.; Lee, J.K.; Kang, J.H. Relationship among Cervical Spine Degeneration, Head and Neck postures, and Myofascial Pain in Masticatory and Cervical Muscles in Elderly with Temporomandibular Disorder. Arch. Gerontol. Geriatr. 2019, 81, 119–128. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Galán-Del-Río, F.; Alonso-Blanco, C.; Jiménez-García, R.; Arendt-Nielsen, L.; Svensson, P. Referred pain from muscle trigger points in the masticatory and neck-shoulder musculature in women with temporomandibular disoders. J. Pain 2010, 11, 1295–1304. [Google Scholar] [CrossRef]
- De Farias Neto, J.P.; De Santana, J.M.; De Santana-Filho, V.J.; Quintans-Junior, L.J.; De Lima Ferreira, A.P.; Bonjardim, L.R. Radiographic measurement of the cervical spine in patients with temporomandibular dysfunction. Arch. Oral Biol. 2010, 55, 670–678. [Google Scholar] [CrossRef]
- Barone, S.; Muraca, D.; Averta, F.; Diodati, F.; Giudice, A. Qualitative and quantitative assessment of condylar displacement after orthognathic surgery: A voxel-based three-dimensional analysis. J. Stomatol. Oral Maxillofac. Surg. 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- Czaprowski, D.; Stoliński, L.; Tyrakowski, M.; Kozinoga, M.; Kotwicki, T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis Spinal Disord. 2018, 13, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, L.; Maharaj, M.M.; Mobbs, R.J. The role of wearables in spinal posture analysis: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 55. [Google Scholar] [CrossRef] [PubMed]
- Chiba, R.; Takakusaki, K.; Ota, J.; Yozu, A.; Haga, N. Human upright posture control models based on multisensory inputs; in fast and slow dynamics. Neurosci. Res. 2016, 104, 96–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riccelli, R.; Passamonti, L.; Toschi, N.; Nigro, S.; Chiarella, G.; Petrolo, C.; Lacquaniti, F.; Staab, J.P.; Indovina, I. Altered Insular and Occipital Responses to Simulated Vertical Self-Motion in Patients with Persistent Postural-Perceptual Dizziness. Front. Neurol. 2017, 8, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Ray, D.; Guayasamin, M. How Does the Central Nervous System for Posture and Locomotion Cope With Damage-Induced Neural Asymmetry? Front. Syst. Neurosci. 2022, 16, 828532. [Google Scholar] [CrossRef]
- Waterston, J.; Chen, L.; Mahony, K.; Gencarelli, J.; Stuart, G. Persistent Postural-Perceptual Dizziness: Precipitating Conditions, Co-morbidities and Treatment With Cognitive Behavioral Therapy. Front. Neurol. 2021, 12, 795516. [Google Scholar] [CrossRef]
- Carvalho, C.E.; da Silva, R.A.; Gil, A.W.; Oliveira, M.R.; Nascimento, J.A.; Pires-Oliveira, D.A.A. Relationship between foot posture measurements and force platform parameters during two balance tasks in older and younger subjects. J. Phys. Ther. Sci. 2015, 27, 705–710. [Google Scholar] [CrossRef] [Green Version]
- Baldini, A.; Nota, A.; Tripodi, D.; Longoni, S.; Cozza, P. Evaluation of the correlation between dental occlusion and posture using a force platform. Clinics 2013, 68, 45–49. [Google Scholar] [CrossRef]
- Leiva, M.; Miralles, R.; Palazzi, C.; Marulanda, H.; Ormeño, G.; Valenzuela, S.; Santander, H. Effects of laterotrusive occlusal scheme and body position on bilateral sternocleidomastoid EMG activity. Cranio 2003, 21, 99–109. [Google Scholar] [CrossRef]
- Marini, I.; Gatto, M.R.; Bartolucci, M.L.; Bortolotti, F.; Alessandri Bonetti, G.; Michelotti, A. Effects of experimental occlusal interference on body posture: An optoelectronic stereophotogrammetric analysis. J. Oral Rehabil. 2013, 40, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Deliagina, T.G.; Orlovsky, G.N.; Zelenin, P.V.; Beloozerova, I.N. Neural bases of postural control. Physiology 2006, 21, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Carini, F.; Mazzola, M.; Fici, C.; Palmeri, S.; Messina, M.; Damiani, P.; Tomasello, G. Posture and posturology, anatomical and physiological profiles: Overview and current state of art. Acta Biomed. 2017, 88, 11–16. [Google Scholar] [PubMed]
- Valla, J.; Delfini, C.; Diagne, M.; Pinganaud, G.; Buisseret, P.; Buisseret-Delmas, C. Vestibulotrigeminal and vestibulospinal projections in rats: Retrograde tracing coupled to glutamic acid decarboxylase immunoreactivity. Neurosci. Lett. 2003, 340, 225–228. [Google Scholar] [CrossRef]
- Ferrillo, M.; Curci, C.; Roccuzzo, A.; Migliario, M.; Invernizzi, M.; de Sire, A. Reliability of cervical vertebral maturation compared to hand-wrist for skeletal maturation assessment in growing subjects: A systematic review. J. Back Musculoskelet. Rehabil. 2021, 34, 925–936. [Google Scholar] [CrossRef]
- Festa, F.; Tecco, S.; Dolci, M.; Ciufolo, F.; Di Meo, S.; Filippi, M.R.; Ferritto, A.L.; D’Attillio, M. Relationship between cervical lordosis and facial morphology in Caucasian women with a skeletal class II malocclusion: A cross-sectional study. Cranio 2003, 21, 121–129. [Google Scholar] [CrossRef]
- Sandoval, C.; Díaz, A.; Manríquez, G. Assessing cervical spine and craniofacial morphology in Class II and Class III malocclusions: A geometric morphometric approach. Cranio. 2021, 8, 1–11. [Google Scholar] [CrossRef]
- Ferrillo, M.; Migliario, M.; Curci, C.; Roccuzzo, A.; Invernizzi, M.; de Sire, A. Reliability of dental calcification compared to hand-wrist X-ray to evaluate skeletal maturation in growing subjects: A systematic review. J. Biol. Regul. Homeost. Agents 2021, 35, 717–723. [Google Scholar] [CrossRef]
- Nucci, L.; Costanzo, C.; Carfora, M.; d’Apuzzo, F.; Franchi, L.; Perillo, L. Dentoskeletal effects of early class III treatment protocol based on timing of intervention in children. Prog. Orthod. 2021, 22, 49. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 9781119536604. [Google Scholar]
- Joanna Briggs Institute Critical Appraisal Checklist for Quasi-Experimental Studies (Non-Randomized Experimental Studies) Checklist. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Quasi-Experimental_Appraisal_Tool2017_0.pdf (accessed on 5 April 2022).
- Strini, P.J.; Machado, N.A.; Gorreri, M.C.; Ferreira Ade, F.; Sousa Gda, C.; Fernandes Neto, A.J. Postural evaluation of patients with temporomandibular disorders under use of occlusal splints. J. Appl. Oral Sci. 2009, 17, 539–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldini, A.; Tecco, S.; Cioffi, D.; Rinaldi, A.; Longoni, S. Gnatho-Postural treatment in an air force pilot. Aviat. Sp. Environ. Med. 2012, 83, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Walczynska-Dragon, K.; Baron, S.; Nitecka-Buchta, A.; Tkacz, E. Correlation between TMD and cervical spine pain and mobility: Is the whole body balance TMJ related? Biomed. Res. Int. 2014, 2014, 582414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Giorgi, I.; Castroflorio, T.; Cugliari, G.; Deregibus, A. Does occlusal splint affect posture? A randomized controlled trial. Cranio-J. Craniomandib. Pract. 2020, 38, 264–272. [Google Scholar] [CrossRef]
- Oliveira, S.S.I.; Pannuti, C.M.; Paranhos, K.S.; Tanganeli, J.P.C.; Laganá, D.C.; Sesma, N.; Duarte, M.; Frigerio, M.L.M.A.; Cho, S.C. Effect of occlusal splint and therapeutic exercises on postural balance of patients with signs and symptoms of temporomandibular disorder. Clin. Exp. Dent. Res. 2019, 5, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.H. Effects on migraine, neck pain, and head and neck posture, of temporomandibular disorder treatment: Study of a retrospective cohort. Arch. Oral Biol. 2020, 114, 104718. [Google Scholar] [CrossRef]
- El Zoghbi, A.; Halimi, M.; Hobeiche, J.; Haddad, C. Effect of occlusal splints on posture balance in patients with temporomandibular joint disorder: A prospective study. J. Contemp. Dent. Pract. 2021, 22, 615–619. [Google Scholar] [CrossRef]
- Gao, D.; Zhang, S.; Kan, H.; Zhang, Q. Relationship between cervical angle and temporomandibular disorders in young and middle-aged population. Cranio. 2022, 15, 1–7. [Google Scholar] [CrossRef]
- Garstka, A.A.; Brzózka, M.; Bitenc-Jasiejko, A.; Ardan, R.; Gronwald, H.; Skomro, P.; Lietz-Kijak, D. Cause-Effect Relationships between Painful TMD and Postural and Functional Changes in the Musculoskeletal System: A Preliminary Report. Pain Res. Manag. 2022, 2022, 1429932. [Google Scholar] [CrossRef]
- Agostini, F.; de Sire, A.; Di Giacomo, G.; Paoloni, M.; Murgia, M.; Di Cesare, A.; Ammendolia, A.; Bernetti, A.; Mangone, M. Postural evaluation and risk of musculoskeletal injuries in professional male rugby players: A proof-of-principle study. J Sports Med. Phys. Fitness. 2022, 21, 21. [Google Scholar] [CrossRef]
- Chandu, A.; Suvinen, T.I.; Reade, P.C.; Borromeo, G.L. The effect of an interocclusal appliance on bite force and masseter electromyography in asymptomatic subjects and patients with temporomandibular pain and dysfunction. J. Oral Rehabil. 2004, 31, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Szczygieł, E.; Fudacz, N.; Golec, J.; Golec, E. The impact of the position of the head on the functioning of the human body: A systematic review. Int. J. Occup. Med. Environ. Health 2020, 33, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Cha, Y.J.; Choi, J.D. Correlation between forward head posture, respiratory functions, and respiratory accessory muscles in young adults. J. Back Musculoskelet. Rehabil. 2017, 30, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.B.; Lee, J.H.; Jeong, H.J.; Cynn, H.S. Effects of suboccipital release with craniocervical flexion exercise on craniocervical alignment and extrinsic cervical muscle activity in subjects with forward head posture. J. Electromyogr. Kinesiol. 2016, 30, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Castroflorio, T.; Perinetti, G.; Guarda-Nardini, L. Dental occlusion, body posture and temporomandibular disorders: Where we are now and where we are heading for. J. Oral Rehabil. 2012, 39, 463–471. [Google Scholar] [CrossRef]
- Perinetti, G.; Contardo, L. Posturography as a diagnostic aid in dentistry: A systematic review. J. Oral Rehabil. 2009, 36, 922–936. [Google Scholar] [CrossRef]
- Kim, T.Y.; Shin, J.S.; Lee, J.; Lee, Y.J.; Kim, M.R.; Ahn, Y.; Park, K.B.; Hwang, D.S.; Ha, I.H. Gender difference in associations between chronic temporomandibular disorders and general quality of life in Koreans: A cross-sectional study. PLoS ONE 2015, 10, e0145002. [Google Scholar] [CrossRef]
- Wang, J.; Chao, Y.; Wan, Q.; Zhu, Z. The possible role of estrogen in the incidence of temporomandibular disorders. Med. Hypotheses 2008, 71, 564–567. [Google Scholar] [CrossRef]
- Yazici, H.; Taskin, M.I.; Guney, G.; Hismiogullari, A.A.; Arslan, E.; Tulaci, K.G. The novel relationship between polycystic ovary syndrome and temporomandibular joint disorders. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 544–548. [Google Scholar] [CrossRef]


{kind=link}
| PubMed (“Temporomandibular Joint Disorders” [MeSH]) AND (“occlusal splints” OR “occlusal splint” OR “stabilization splints” OR “splints” OR “splint”) AND (“posture” OR “postural” OR “postural balance” OR “back” OR “spine” OR “spinal”) |
| Scopus TITLE-ABS-KEY(((“temporomandibular disorders”) AND (“occlusal splints” OR “occlusal splint” OR “stabilization splints” OR “splints” OR “splint”) AND (“posture” OR “postural” OR “postural balance” OR “back” OR “spine” OR “spinal”))) |
| Web of Science ((“temporomandibular disorders”) AND (“occlusal splints” OR “occlusal splint” OR “stabilization splints” OR “splints” OR “splint”) AND (“posture” OR “spinal” OR “postural balance” OR “back” OR “spine” OR “spinal”)) |
| Articles excluded after title and abstract screening phase (n = 86) * | |
| Study design | 15 (17.44%) |
| Not population of interest | 23 (26.74%) |
| Not intervention of interest | 42 (48.84%) |
| Not comparison of interest | 45 (52.33%) |
| Not outcome of interest | 51 (59.30%) |
| Articles excluded after full-text screening phase (n = 11) | |
| Study design | 0 (0.00%) |
| Not population of interest | 4 (40.00%) |
| Not intervention of interest | 1 (10.00%) |
| Not comparison of interest | 0 (0.00%) |
| Not outcome of interest | 3 (30.00%) |
| Full text not available | 3 (30.00%) |
| Authors | Journal | Nationality | Design | Pop. (M/F) | Age (Years) | TMD Diagnosis | Intervention | Comparator | Outcome | Time Points | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Strini et al., 2009 [53] | Journal of Applied Oral Science | Brazil | Observational | n = 20 (1/19) | 28.4 ± 8.4 | Mixed temporomandibular disorders (TMD) plus parafunctional habits (e.g., bruxism) | The upper arch occlusal splint was fabricated programming the mandibular position in centric relation occlusion. The resin rigid occlusal splint was consistent with the technique advocated by Okeson. The patients were instructed to use the splint continuously for 24 h within the first week of treatment and, after this period, to use the splint every night. | N/A | Head position (HP) assessment | Data were collected at baseline (T0), after 1 week (T1), and 1 month (T2). | Regarding physical examination and the patient’s posture, among the values obtained in the HP at the start of treatment, after 1 week and 1 month there were statistically significant differences (p < 0.05). In conclusion, the individual’s postural position can suffer biomechanical alterations due to stomatognathic alterations, causing clinically visible changes in dysfunctional individuals and affecting the performance of the involved structures. |
| Baldini et al., 2012 [54] | Aviation, Space, and Environmental Medicine | Italy | Case Report | n = 1 (1/0) | 32 | Arthrogenous TMD plus parafunctional habits (e.g., bruxism) | The lower arch stabilization splint was fabricated programming the mandibular position in centric relation occlusion. The occlusal splint was a resin Michigan rigid splint designed to be worn in flight | N/A | Stabilometric force platform | N/A | The analysis on the force platform showed good postural balance, both with and without the occlusal splint. The clinical gnatho-postural treatment involving a functional diagnostic instrument used on Italian Air Force pilots, protects the masticatory system from dental abrasion and, in this particular case, seemed to improve the pilot’s posture control system as analyzed by the stabilometric platform. |
| Walczynska-Dragon et al., 2014 [55] | BioMed Research International | Poland | Observational | n = 60 (30/30) | 33.76 ± 9.1 | Mixed TMD plus parafunctional habits (e.g., bruxism) | The Sagittal Vertical Extrusion Device (SVED) was a flat-plane appliance which makes contact only with the anterior teeth in the opposing arch. The patients were instructed to use the splints during sleep, but not more than 8–10 h per day | Behavioural therapy | Kinematics of the cervical spine | Data were collected at baseline (T0), after 3 weeks (T1), and 3 months (T2). | The highest improvement was seen during the flexion movement, which, on the 1st examination only in 22% of patients, was within normative values. During the 3rd examination in 70% of patients from treated group, flexion movement conformed to the norm. For the anteflexion movement, the improvement of the results was highly significant (p = 0.0006); for the retroflexion movement, the results were improved by a highly significant factor (p = 0.0082). In the control group, no significant changes were found. In conclusion, there is a significant association between TMD treatment and reduction in cervical spine pain, as far as improvement of cervical spine mobility. |
| De Giorgi et al., 2018 [56] | CRANIO®: The Journal of Craniomandibular & Sleep Practice | Italy | Randomized controlled trial (RCT) | n = 45 (0/45) | 41.6 ± 17.3 | Arthrogenous TMD | The rigid lower arch occlusal stabilization splint was prepared following the biomechanical models proposed by Ferrario and Sforza, with only posterior contacts (from the second premolar to the second or first permanent molar), without static and dynamic anterior contacts. Patients wore the occlusal splints all night. | No treatment | Rasterstereography | Data were collected at baseline (T0), after 1 month (T1), 3 months (T2), and 6 months (T3). | The evaluation of the cervical arrow at rest position showed a statistically significant difference at T1 between the control group (CG) and the occlusal splint group (SG) (p = 0.001). Concerning the kyphotic angle, cervicothoracic inflection point-thoracolumbar inflection point at rest position, a statistically significant difference was found at T1 between CG and SG (p = 0.012) and also at T2 between CG and SG (p = 0.019). With regard to the lordotic angle, thoracolumbar inflection point-lumbosacral inflection point, a statistically significant difference was found at rest position at T2 between CG and SG (p = 0.017). In conclusion, even if some differences were found between the control and the occlusal splint group, the low range of statistical significance made these results not significant from a clinical point of view. |
| Oliveira et al., 2019 [57] | Clinical and Experimental Dental Research | Brazil | RCT | n = 49 (10/39) | 39.8 ± 16.3 | Mixed TMD | Occlusal stabilization splint plus physical therapy. Occlusal splint was performed under the occlusal stability criteria (simultaneous bilateral contacts with absence of interferences in canine and anterior guides). The occlusal splint was used throughout night plus 2 h in the morning and 2 h in the afternoon | Physical therapy | Stabilometric force platform | Data were collected at baseline (T0) and after 12 weeks (T1). | The patients of the test group presented a significant increase in antero-posterior velocity from the center of pressure (COP) with eyes open (p = 0.023) and eyes closed (p < 0.001). Control group did not present a significant increase in the eyes open (p = 0.249) primary outcome only with eyes closed (p < 0.046). There was an additional beneficial effect of the use of occlusal splint on the postural balance and guidelines of therapeutic exercises, with a significant increase in antero-posterior velocity of COP of the body with eyes open and closed. |
| Kang et al., 2020 [58] | Archives of Oral Biology | South Korea | Observational | n = 187 (34/153) | 35.3 ± 15.4 | Mixed TMD plus parafunctional habits (e.g., bruxism)/migraine | Upper arch occlusal stabilization splint plus physical therapy plus behavioral therapy. All patients were instructed to wear the rigid splint every night for at least eight hours per day | N/A | Computerized cephalometric analysis | Data were collected at baseline (T0) and after 6 months (T1). | Using cephalometric analysis, the results demonstrated that controlling the orofacial pain in patients with TMD and migraine showed remarkable improvement in neck pain, head and neck posture, and migraine. |
| El Zoghbi et al., 2021 [59] | The Journal of Contemporary Dental Practice | Lebanon | Observational | n = 47 (0/47) | N/A | Mixed TMD | The upper arch rigid occlusal stabilization splint was worn by patients during night | N/A | Stabilometric force platform | Data were collected at baseline (T0) and after 6 months (T1). | The sway surface area decreased significantly after the occlusal guard placement with closed eyes (p= 0.012) but not with eyes open (p = 0.169). Likewise, the sway surface area decreased significantly in a dynamic lateral position with closed eyes (p = 0.018) and in the anteroposterior dynamic position with open eyes (p = 0.031). The mean sway length decreased significantly after the placement of the occlusal splint when participants were in a lateral position with open eyes (p = 0.025) and in the anteroposterior position with open eyes (p-value, 0.014). In conclusion, in female patients with TMD, the use of an occlusal splint is associated with a postural improvement evaluated by posturo-stabilometric tests. |
| Author and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
|---|---|---|---|---|---|---|---|---|---|
| Strini et al., 2009 [53] | N | N/A | N/A | N | Y | Y | Y | N | N |
| Baldini et al., 2012 [54] | N/A | N/A | N/A | N/A | Y | Y | N | Y | N/A |
| Walczynska-Dragon et al., 2014 [55] | N | Y | Y | Y | Y | Y | Y | Y | Y |
| De Giorgi et al., 2018 [56] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Oliveira et al., 2019 [57] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Kang et al., 2020 [58] | N | N/A | N/A | N | Y | Y | Y | Y | Y |
| El Zoghbi et al., 2021 [59] | N | N/A | N/A | N | Y | Y | N | Y | N |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrillo, M.; Marotta, N.; Giudice, A.; Calafiore, D.; Curci, C.; Fortunato, L.; Ammendolia, A.; de Sire, A. Effects of Occlusal Splints on Spinal Posture in Patients with Temporomandibular Disorders: A Systematic Review. Healthcare 2022, 10, 739. https://doi.org/10.3390/healthcare10040739
Ferrillo M, Marotta N, Giudice A, Calafiore D, Curci C, Fortunato L, Ammendolia A, de Sire A. Effects of Occlusal Splints on Spinal Posture in Patients with Temporomandibular Disorders: A Systematic Review. Healthcare. 2022; 10(4):739. https://doi.org/10.3390/healthcare10040739
Chicago/Turabian StyleFerrillo, Martina, Nicola Marotta, Amerigo Giudice, Dario Calafiore, Claudio Curci, Leonzio Fortunato, Antonio Ammendolia, and Alessandro de Sire. 2022. "Effects of Occlusal Splints on Spinal Posture in Patients with Temporomandibular Disorders: A Systematic Review" Healthcare 10, no. 4: 739. https://doi.org/10.3390/healthcare10040739