
Effects of Leisure-Time Physical Activity on Cognitive Reserve Biomarkers and Leisure Motivation in the Pre-Diabetes Elderly


Abstract
:1. Introduction
2. Methods
2.1. Participation
2.2. Measurement of Body Composition
2.3. Hematological Analysis
2.4. Leisure-Time Physical Activity
2.5. Questionnaire Test
2.6. Statistical Analysis
3. Results
3.1. Demographic Characteristics for Pre-Diabetes-Elderly-Only Questionnaire
3.2. LTPA Motivation and Stress
3.3. Change in Body Composition and Glycated Hemoglobin (HbA1c) Level after Intervention
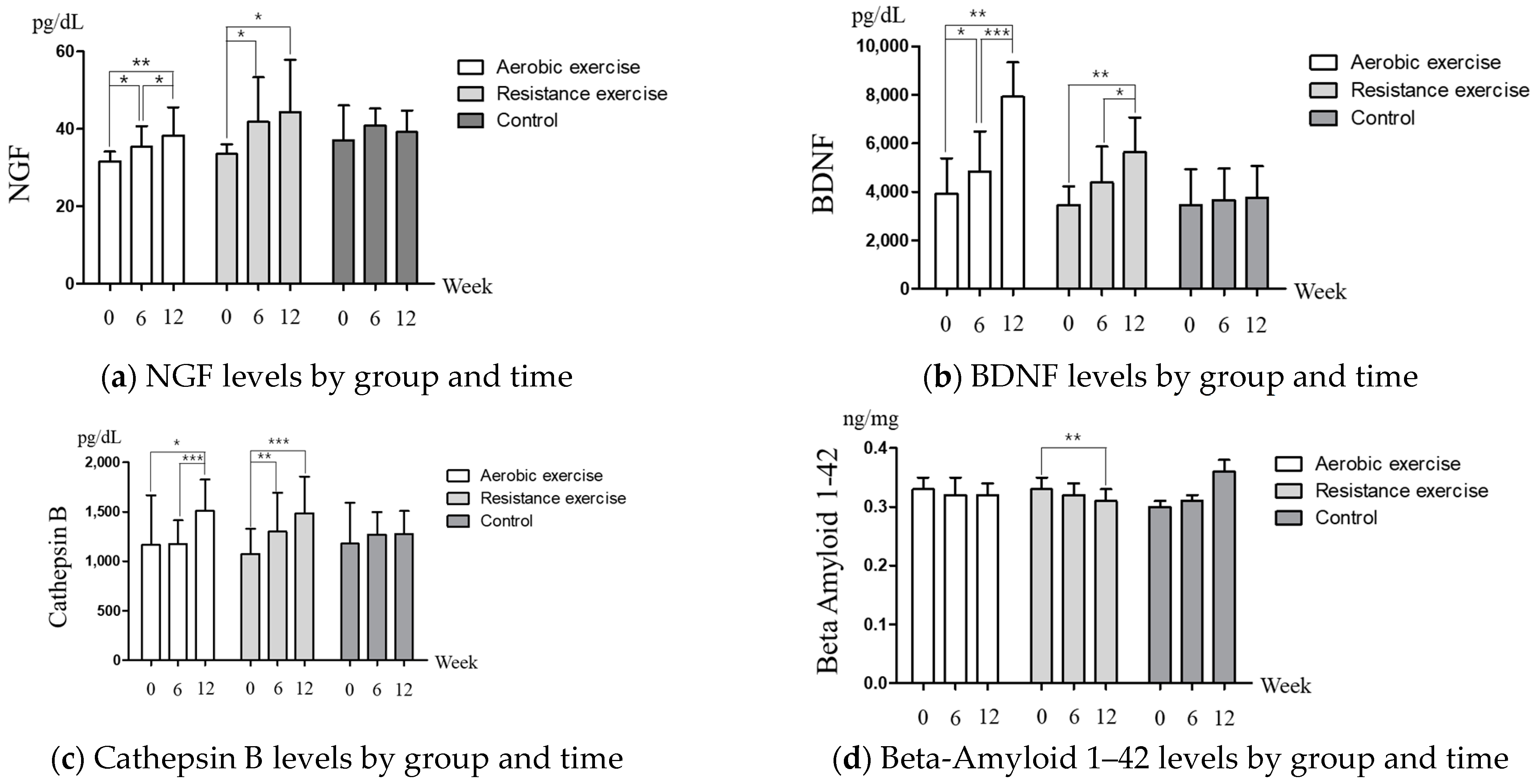
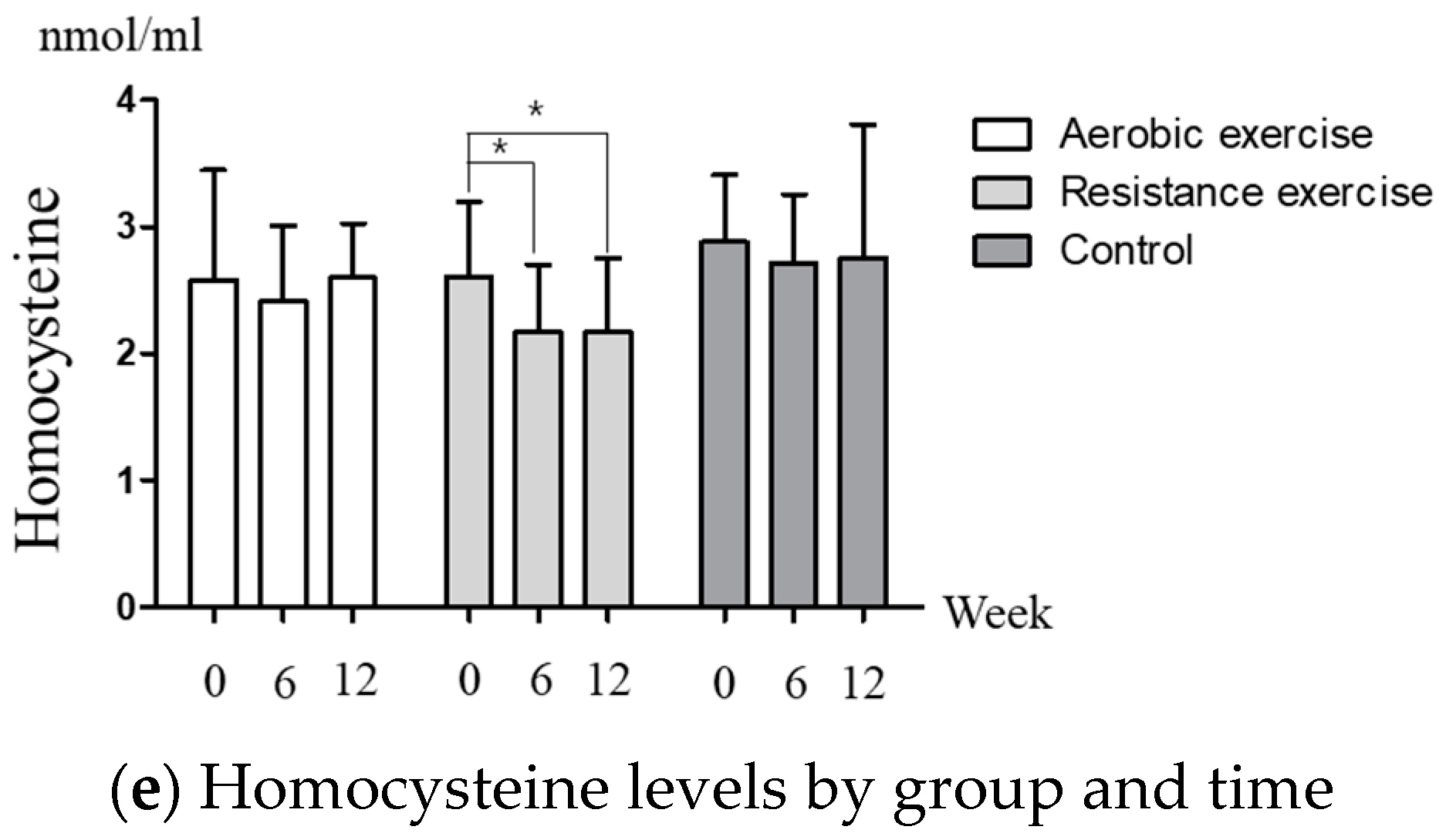
3.4. Change in Cognitive Reserve Biomarkers after Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, O.Y.; Song, J. The importance of BDNF and RAGE in diabetes-induced dementia. Pharmacol. Res. 2020, 160, 105083. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.; Beare, R.; Wang, W.; Callisaya, M.; Srikanth, V. Type 2 diabetes mellitus, brain atrophy, and cognitive decline. Neurology 2019, 92, e823–e830. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, B.J.; Hayward, G.C.; Fajardo, V.A.; MacPherson, R.E.K. Increased Prevalence of Obesity/Type 2 Diabetes and Lower Levels of Lithium in Rural Texas Counties May Explain Greater Alzheimer’s Disease Risk. J. Alzheimers Dis. 2018, 64, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Madhusudhanan, J.; Suresh, G.; Devanathan, V. Neurodegeneration in type 2 diabetes: Alzheimer’s as a case study. Brain Behav. 2020, 10, e01577. [Google Scholar] [CrossRef] [Green Version]
- Sastre, A.A.; Vernooij, R.W.; Harmand, M.G.; Martínez, G. Effect of the treatment of Type 2 diabetes mellitus on the development of cognitive impairment and dementia. Cochrane Database Syst. Rev. 2017, 6, CD003804. [Google Scholar]
- Stein, A.M.; Silva, T.M.V.; Coelho, F.G.M.; Arantes, F.J.; Costa, J.L.R.; Teodoro, E.; Santos-Galduróz, R.F. Physical exercise, IGF-1 and cognition A systematic review of experimental studies in the elderly. Dement. Neuropsychol. 2018, 12, 114–122. [Google Scholar] [CrossRef]
- Palmer, K.; Backman, L.; Winblad, B.; Fratiglioni, L. Mild cognitive impairment in the general population: Occurrence and progression to Alzheimer disease. Am. J. Geriatr. Psychiatry 2008, 16, 603–611. [Google Scholar] [CrossRef]
- Zhuang, Q.; Wu, L.; Ting, W.; Jie, L.; Zou, J.; Du, J. Negative emotions in community-dwelling adults with prediabetes and hypertension. J. Int. Med. Res. 2020, 48, 300060520918411. [Google Scholar] [CrossRef] [Green Version]
- Graham, E.; Au, B.; Schmitz, N. Depressive symptoms, prediabetes, and incident diabetes in older English adults. Int. J. Geriatr. Psychiatry 2017, 32, 1450–1458. [Google Scholar] [CrossRef]
- Katon, W.; Lyles, C.R.; Parker, M.M.; Karter, A.J.; Huang, E.S.; Whitmer, R.A. Association of depression with increased risk of dementia in patients with type 2 diabetes: The Diabetes and Aging Study. Arch. Gen. Psychiatry 2012, 69, 410–417. [Google Scholar]
- Oftedal, B.; Bru, E.; Karlsen, B. Motivation for diet and exercise management among adults with type 2 diabetes. Scand. J. Caring Sci. 2011, 25, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.S.; Guarnaccia, C.A. Self-determination theory and motivational interviewing interventions for type 2 diabetes prevention and treatment: A systematic review. J. Health Psychol. 2020, 25, 44–66. [Google Scholar] [CrossRef] [PubMed]
- Rowan, C.P.; Riddell, M.C.; Gledhill, N.; Jamnik, V.K. Aerobic Exercise Training Modalities and Prediabetes Risk Reduction. Med. Sci. Sports Exerc. 2017, 49, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Ma, X.; Xu, H.; Ruan, S.; Yuan, X. Comparing the effects of 12 months aerobic exercise and resistance training on glucose metabolism among prediabetes phenotype: A explorative randomized controlled trial. Prim. Care Diabetes 2021, 15, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Thaiyanto, J.; Sittichoke, C.; Phirom, K.; Sungkarat, S. Effects of Multicomponent Exercise on Cognitive Performance and Fall Risk in Older Women with Mild Cognitive Impairment. J. Nutr. Health Aging 2021, 25, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Shin, M.; Park, Y.; Won, S.Y.; Cho, K.S. Physical Exercise-Induced Myokines in Neurodegenerative Diseases. Int. J. Mol. Sci. 2021, 22, 5795. [Google Scholar] [CrossRef]
- Marinescu, I.; Enătescu, V.R.; Ghelase, S.M.; Marinescu, D. Neurobiological arguments for a pathogenic multifactorial disconnective model of cognitive disorders from Alzheimer’s disease in elderly people. Rom. J. Morphol. Embryol. 2017, 58, 1165–1173. [Google Scholar]
- Rooney, M.R.; Rawlings, A.M.; Pankow, J.S.; Tcheugui, J.B.E.; Coresh, J.; Sharrett, A.R.; Selvin, E. Risk of Progression to Diabetes Among Older Adults with Prediabetes. JAMA Intern. Med. 2021, 181, 511–519. [Google Scholar] [CrossRef]
- Vlachopoulos, S.P.; Katartzi, E.S.; Kontou, M.G.; Moustaka, F.C.; Goudas, M. The revised perceived locus of causality in physical education scale: Psychometric evaluation among youth. Psychol. Sport Exerc. 2011, 12, 583–592. [Google Scholar] [CrossRef]
- Song, Y.G.; Cheon, S.H. Examining Validation of Perceived Locus of Causality Scale(PLCS) for Physical Education. Korean Assoc. Sport Pedagog. 2014, 21, 81–101. [Google Scholar]
- Lee, E.S. Development of the Stress Questionnaire for KNHANES. Res. Rep. Korea Cent. Dis. Control Prev. 2010, 96, 1–103. [Google Scholar]
- Cox, A.E. Ullrich-French, S.; Sabiston, C. Using motivation regulations in a person-centered approach to examine the link between social physique anxiety in physical education and physical activity-related outcomes in adolescents. Psychol. Sport Exerc. 2013, 14, 461–467. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Song, Y.G. Association between Motivation Types and Anxiety in the Patients with Diabetes Mellitus. Korean J. Sport Psychol. 2021, 32, 69–80. [Google Scholar] [CrossRef]
- De Man, J.; Wouters, E.; Absetz, P.; Daivadanam, M.; Naggayi, G.; Kasujja, F.X.; Remmen, R.; Guwatudde, D.; Van Olmen, J. What motivates people with (pre) diabetes to move? Testing self-determination theory in rural Uganda. Front. Psychol. 2020, 11, 404. [Google Scholar] [CrossRef] [Green Version]
- De Man, J.; Kasujja, F.X.; Delobelle, P.; Annerstedt, K.S.; Alvesson, H.M.; Absetz, P.; Wouters, E.; Daivadanam, M.; Guwatudde, D.; Puoane, T.; et al. Motivational determinants of physical activity in disadvantaged populations with (pre) diabetes: A cross-cultural comparison. BMC Public Health 2022, 22, 1–13. [Google Scholar] [CrossRef]
- Russell-Williams, J.; Jaroudi, W.; Perich, T.; Hoscheidt, S.; Haj, M.E.; Moustafa, A.A. Mindfulness and meditation: Treating cognitive impairment and reducing stress in dementia. Rev. Neurosci. 2018, 29, 791–804. [Google Scholar] [CrossRef]
- Fiore, V.; De Rosa, A.; Falasca, P.; Marci, M.; Guastamacchia, E.; Licchelli, B.; Giagulli, V.A.; Pergola, G.D.; Poggi, A.; Triggiani, V. Focus on the correlations between alzheimer’s disease and type 2 diabetes. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 571–579. [Google Scholar] [CrossRef]
- Wijndaele, K.; Matton, L.; Duvigneaud, N.; Lefevre, J.; Bourdeaudhuij, I.D.; Duquet, W.; Thomis, M.; Philippaerts, R.M. Association between leisure time physical activity and stress, social support and coping: A cluster-analytical approach. Psychol. Sport Exerc. 2007, 8, 425–440. [Google Scholar] [CrossRef]
- Aldana, S.G.; Sutton, L.D.; Jacobson, B.H.; Quirk, M.G. Relationships between leisure time physical activity and perceived stress. Percept Mot. Skills 1996, 82, 315–321. [Google Scholar] [CrossRef]
- Biessels, G.J.; Strachan, M.W.J.; Visseren, F.L.J.; Kappelle, L.J.; Whitmer, R.A. Dementia and cognitive decline in type 2 diabetes and prediabetic stages: Towards targeted interventions. Lancet Diabetes Endocrinol. 2014, 2, 246–255. [Google Scholar] [CrossRef]
- Sundermann, E.E.; Thomas, K.R.; Bangen, K.J.; Weigand, A.J.; Eppig, J.S.; Edmonds, E.C.; Wong, C.G.; Bondi, M.W.; Delano-Wood, L. Prediabetes Is Associated with Brain Hypometabolism and Cognitive Decline in a Sex-Dependent Manner: A Longitudinal Study of Nondemented Older Adults. Front. Neurol. 2021, 12, 551975. [Google Scholar] [CrossRef] [PubMed]
- Cuello, A.C.; Pentz, R.; Hall, H. The Brain NGF Metabolic Pathway in Health and in Alzheimer’s Pathology. Front. Neurosci. 2019, 13, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beeri, M.S.; Sonnen, J. Brain BDNF expression as a biomarker for cognitive reserve against Alzheimer disease progression. Neurology 2016, 86, 702–703. [Google Scholar] [CrossRef]
- Nakanishi, H. Microglial cathepsin B as a key driver of inflammatory brain diseases and brain aging. Neural Regen Res. 2020, 15, 25–29. [Google Scholar] [CrossRef]
- Yaffe, K.; Weston, A.; Graff-Radford, N.R.; Satterfield, S.; Simonsick, E.M.; Younkin, S.G.; Younkin, L.H.; Kuller, L.; Ayonayon, H.N.; Ding, J.; et al. Association of plasma beta-amyloid level and cognitive reserve with subsequent cognitive decline. JAMA 2011, 305, 261–266. [Google Scholar] [CrossRef] [Green Version]
- De Luis, D.A.; Fernandez, N.; Arranz, M.; Aller, R.; Izaola, O. Total homocysteine and cognitive deterioration in people with type 2 diabetes. Diabetes Res. Clin. Pract. 2002, 55, 185–190. [Google Scholar] [CrossRef]
- Kim, B.; Kang, S. Regular Leisure-Time Physical Activity is Effective in Boosting Neurotrophic Factors and Alleviating Menopause Symptoms. Int. J. Environ. Res. Public Health 2020, 17, 8624. [Google Scholar] [CrossRef]
- Fernandes, M.S.; Ordônio, T.F.; Santos, G.C.J.; Santos, L.E.R.; Calazans, C.T.; Gomes, D.A.; Santos, T.M. Effects of Physical Exercise on Neuroplasticity and Brain Function: A Systematic Review in Human and Animal Studies. Neural Plast. 2020, 2020, 8856621. [Google Scholar] [CrossRef]
- La Rosa, A.D.; Solana, E.; Corpas, R.; Bartrés-Faz, D.; Pallàs, M.; Vina, J.; Sanfeliu, C.; Gomez-Cabrera, M.C. Long-term exercise training improves memory in middle-aged men and modulates peripheral levels of BDNF and Cathepsin B. Sci. Rep. 2019, 9, 3337. [Google Scholar] [CrossRef] [Green Version]
- Özbeyli, D.; Sarı, G.; Özkan, N.; Karademir, B.; Yüksel, M.; Kaya, Ö.T.Ç.; Çakır, Ö.K. Protective effects of different exercise modalities in an Alzheimer’s disease-like model. Behav. Brain Res. 2017, 328, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.J.; Tschakovsky, M.E. Exercise and circulating BDNF: Mechanisms of release and implications for the design of exercise interventions. Appl. Physiol. Nutr. Metab. 2018, 43, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.Y.; Becke, A.; Berron, D.; Becker, B.; Sah, N.; Benoni, G.; Janke, E.; Lubejko, S.T.; Greig, N.H.; Mattison, J.A.; et al. Running-Induced Systemic Cathepsin B Secretion Is Associated with Memory Function. Cell Metab. 2016, 24, 332–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firth, J.; Stubbs, B.; Vancampfort, D.; Schuch, F.; Lagopoulos, J.; Rosenbaum, S.; Ward, P.B. Effect of aerobic exercise on hippocampal volume in humans: A systematic review and meta-analysis. Neuroimage 2018, 166, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Stillman, C.M.; Lopez, O.L.; Becker, J.T.; Kuller, L.H.; Mehta, P.D.; Tracy, R.P.; Erickson, K.I. Physical activity predicts reduced plasma β amyloid in the Cardiovascular Health Study. Ann. Clin. Transl. Neurol. 2017, 4, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.M.; Peiffer, J.; Rainey-Smith, S.R. Exploring the relationship between physical activity, beta-amyloid and tau: A narrative review. Ageing Res. Rev. 2019, 50, 9–18. [Google Scholar] [CrossRef]
- Brown, B.M.; Peiffer, J.J.; Taddei, K.; Lui, J.K.; Laws, S.M.; Gupta, V.B.; Taddei, T.; Ward, V.K.; Rodrigues, M.A.; Burnham, S.; et al. Physical activity and amyloid-β plasma and brain levels: Results from the Australian Imaging, Biomarkers and Lifestyle Study of Ageing. Mol. Psychiatry 2013, 18, 875–881. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.H.; Almeida, O.P. Effect of Vitamin B Supplementation on Cognitive Function in the Elderly: A Systematic Review and Meta-Analysis. Drugs Aging 2019, 36, 419–434. [Google Scholar] [CrossRef]
- Deminice, R.; Ribeiro, D.F.; Frajacomo, F.T.T. The Effects of Acute Exercise and Exercise Training on Plasma Homocysteine: A Meta-Analysis. PLoS ONE 2016, 11, e0151653. [Google Scholar]
- Jakovljevic, B.; Gasic, B.; Kovacevic, P.; Rajkovaca, Z.; Kovacevic, T. Homocystein as a risk factor for developing complications in chronic renal failure. Mater. Socio-Med. 2015, 27, 95–98. [Google Scholar] [CrossRef] [Green Version]
- Joubert, L.M.; Manore, M.M. Exercise, nutrition, and homocysteine. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 341–361. [Google Scholar] [CrossRef] [PubMed]
- Antunes, H.K.M.; Mello, M.T.D.; Lemos, V.A.; Santos-Galduróz, R.F.; Galdieri, L.C.; Bueno, O.F.A.; Tufik, S.; D’Almeida, V. Aerobic physical exercise improved the cognitive function of elderly males but did not modify their blood homocysteine levels. Dement Geriatr. Cogn. Dis. Extra 2015, 5, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Malin, S.K.; Francois, M.E.; Eichner, N.Z.M.; Gilbertson, N.M.; Heiston, E.M.; Fabris, C.; Breton, M. Impact of short-term exercise training intensity on β-cell function in older obese adults with prediabetes. J. Appl. Physiol. 2018, 125, 1979–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, L.; Fang, Y.; Tang, L. Comparisons of different exercise interventions on glycemic control and insulin resistance in prediabetes: A network meta-analysis. BMC Endocr. Disord. 2021, 21, 181. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Park, K.M.; Sung, K.Y.; Yuan, Y.; Lim, S.T. Effect of Resistance Exercise on the Lipolysis Pathway in Obese Pre- and Postmenopausal Women. J. Pers. Med. 2021, 11, 874. [Google Scholar] [CrossRef]
- Wheeler, M.J.; Dempsey, P.C.; Grace, M.S.; Ellis, K.A.; Gardiner, P.A.; Green, D.J.; Dunstan, D.W. Sedentary behavior as a risk factor for cognitive decline? A focus on the influence of glycemic control in brain health. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2017, 3, 291–300. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Group | Mean ± SD | p-Value |
|---|---|---|---|
| Age (year) | Aerobic Exercise (n = 15) | 70.47 ± 5.57 | 0.123 |
| Resistance Exercise (n = 12) | 72.25 ± 5.07 | ||
| Control (n = 9) | 67.78 ± 2.33 | ||
| Height (cm) | Aerobic Exercise (n = 15) | 153.7 ± 4.73 | 0.134 |
| Resistance Exercise (n = 12) | 149.9 ± 6.30 | ||
| Control (n = 9) | 154.7 ± 6.50 | ||
| Weight (kg) | Aerobic Exercise (n = 15) | 62.45 ± 10.34 | 0.355 |
| Resistance Exercise (n = 12) | 57.32 ± 9.10 | ||
| Control (n = 9) | 59.52 ± 6.51 | ||
| BMI (kg/m2) | Aerobic Exercise (n = 15) | 26.50 ± 4.48 | 0.506 |
| Resistance Exercise (n = 12) | 25.37 ± 2.84 | ||
| Control (n = 9) | 24.86 ± 2.23 | ||
| Percent fat (%) | Aerobic Exercise (n = 15) | 38.33 ± 7.34 | 0.711 |
| Resistance Exercise (n = 12) | 38.19 ± 5.81 | ||
| Control (n = 9) | 36.32 ± 3.63 | ||
| SBP (mmHg) | Aerobic Exercise (n = 15) | 141.0 ± 14.09 | 0.684 |
| Resistance Exercise (n = 12) | 137.4 ± 9.92 | ||
| Control (n = 9) | 137.2 ± 10.28 | ||
| DBP (mmHg) | Aerobic Exercise (n = 15) | 68.33 ± 6.88 | 0.303 |
| Resistance Exercise (n = 12) | 72.17 ± 6.46 | ||
| Control (n = 9) | 70.78 ± 5.40 |
| (a) | |||
| Items Station | Exercise | Intensity | Time |
| 1 | Warm up | 10 min | |
| 2 | Vine step | HRR 55∼65% 250∼300 kcal/day | 40 min |
| 3 | Mambo | ||
| 4 | Twist | ||
| 5 | Bumb | ||
| 6 | Love repeat | ||
| 7 | Love trick | ||
| 8 | Walking | ||
| 9 | Cool down | 10 min | |
| (b) | |||
| Items Station | Exercise | Intensity | Time |
| 1 | Warm up | 10 min | |
| 2 | Squat | %RM 55∼65% 250∼300 kcal/day | 40 min |
| 3 | Lunge | ||
| 4 | Chest press | ||
| 5 | Vertical fly | ||
| 6 | Lat pull down | ||
| 7 | Long pull | ||
| 8 | Crunch | ||
| 9 | Cool down | 10 min | |
| Category | n | % | Variable | Category | n | % | |
|---|---|---|---|---|---|---|---|
| Gender | Male | 54 | 29.3 | LTPA Frequency | Fewer than 3 times a week | 101 | 54.9 |
| Female | 130 | 70.7 | |||||
| 3 or more times a week | 83 | 45.1 | |||||
| Age | 69.74 ± 10 | 184 | 100 | ||||
| Other disease | None | 66 | 35.9 | LTPA Amount | Less than 1 h | 134 | 72.8 |
| Hypertension | 88 | 47.8 | |||||
| Over 1 h | 50 | 27.2 | |||||
| Etc. | 30 | 16.3 | |||||
| Total | 184 | 100.0 | Total | 184 | 100.0 | ||
| Variable | Category | Minimum | Maximum | M ± SD |
|---|---|---|---|---|
| LTPA motivation | Integrated regulation | 1.00 | 7.00 | 5.03 ± 1.52 |
| Identified regulation | 1.00 | 7.00 | 5.49 ± 1.32 | |
| Introjected regulation | 1.00 | 6.50 | 3.72 ± 0.93 | |
| Extrinsic regulation | 1.00 | 7.00 | 3.15 ± 1.09 | |
| Stress | Burnout | 1.00 | 5.00 | 1.90 ± 0.94 |
| Depression | 1.00 | 5.00 | 1.69 ± 0.91 | |
| Anger | 1.00 | 5.00 | 1.64 ± 0.92 |
| Variable | 0 Week a | 6 Weeks b | 12 Weeks c | Post hoc | F-Value (p-Value) | |
|---|---|---|---|---|---|---|
| Weight (kg) | AE | 62.45 ± 10.35 | 61.84 ± 10.29 | 59.75 ± 9.19 | a > b > c | G: 0.935 (0.403) T: 19.254 (<0.001) G × T: 3.559 (0.011) |
| RE | 57.32 ± 9.10 | 57.12 ± 9.01 | 55.87 ± 7.14 | - | ||
| CG | 59.52 ± 6.51 | 58.58 ± 6.40 | 58.79 ± 6.61 | a > b | ||
| BMI (kg/m2) | AE | 26.50 ± 4.48 | 26.27 ± 4.53 | 25.34 ± 3.96 | a > b > c | G: 0.526 (0.596) T: 14.373 (<0.001) G × T: 3.774 (0.008) |
| RE | 25.37 ± 2.84 | 25.32 ± 2.83 | 24.87 ± 2.21 | - | ||
| CG | 24.86 ± 2.23 | 24.46 ± 2.25 | 24.57 ± 2.20 | a > b | ||
| Fat (%) | AE | 38.33 ± 7.34 | 37.93 ± 8.10 | 36.60 ± 7.52 | - | G: 0.199 (0.820) T: 34.508 (<0.001) G × T: 7.331 (<0.001) |
| RE | 38.19 ± 5.81 | 37.53 ± 6.69 | 35.27 ± 5.32 | a > b > c | ||
| CG | 36.32 ± 3.63 | 35.67 ± 3.38 | 35.90 ± 2.72 | a > b | ||
| SBP (mmHg) | AE | 141.0 ± 14.09 | 137.0 ± 12.72 | 133.27 ± 14.29 | a > c | G: 0.476 (0.626) T: 1.018 (0.367) G × T: 2.776 (0.034) |
| RE | 137.7 ± 9.92 | 137.6 ± 14.77 | 143.0 ± 11.79 | - | ||
| CG | 137.2 ± 10.28 | 135.9 ± 8.11 | 131.8 ± 7.92 | b > c | ||
| DBP (mmHg) | AE | 68.33 ± 6.88 | 68.67 ± 7.45 | 67.53 ± 7.34 | - | G: 2.298 (0.116) T: 0.128 (0.880) G × T: 0.835 (0.508) |
| RE | 72.17 ± 6.46 | 73.67 ± 12.30 | 75.08 ± 8.53 | - | ||
| CG | 70.78 ± 5.40 | 70.44 ± 5.90 | 68.56 ± 6.31 | - | ||
| HbA1c (%) | AE | 6.16 ± 0.29 | 6.09 ± 0.29 | 5.79 ± 0.40 | a > b > c | G: 0.449 (0.642) T: 17.255 (<0.001) G × T: 21.441 (<0.001) |
| RE | 6.08 ± 0.39 | 6.05 ± 0.33 | 5.61 ± 0.39 | a > b > c | ||
| CG | 5.84 ± 0.31 | 5.81 ± 0.41 | 6.08 ± 0.28 | a < b < c | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.-R.; Lim, S.-T. Effects of Leisure-Time Physical Activity on Cognitive Reserve Biomarkers and Leisure Motivation in the Pre-Diabetes Elderly. Healthcare 2022, 10, 737. https://doi.org/10.3390/healthcare10040737
Kim B-R, Lim S-T. Effects of Leisure-Time Physical Activity on Cognitive Reserve Biomarkers and Leisure Motivation in the Pre-Diabetes Elderly. Healthcare. 2022; 10(4):737. https://doi.org/10.3390/healthcare10040737
Chicago/Turabian StyleKim, Bo-Ram, and Seung-Taek Lim. 2022. "Effects of Leisure-Time Physical Activity on Cognitive Reserve Biomarkers and Leisure Motivation in the Pre-Diabetes Elderly" Healthcare 10, no. 4: 737. https://doi.org/10.3390/healthcare10040737