
Relationship of the Nigrostriatal Tract with the Motor Function and the Corticospinal Tract in Chronic Hemiparetic Stroke Patients: A Diffusion Tensor Imaging Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Motor Function Evaluation
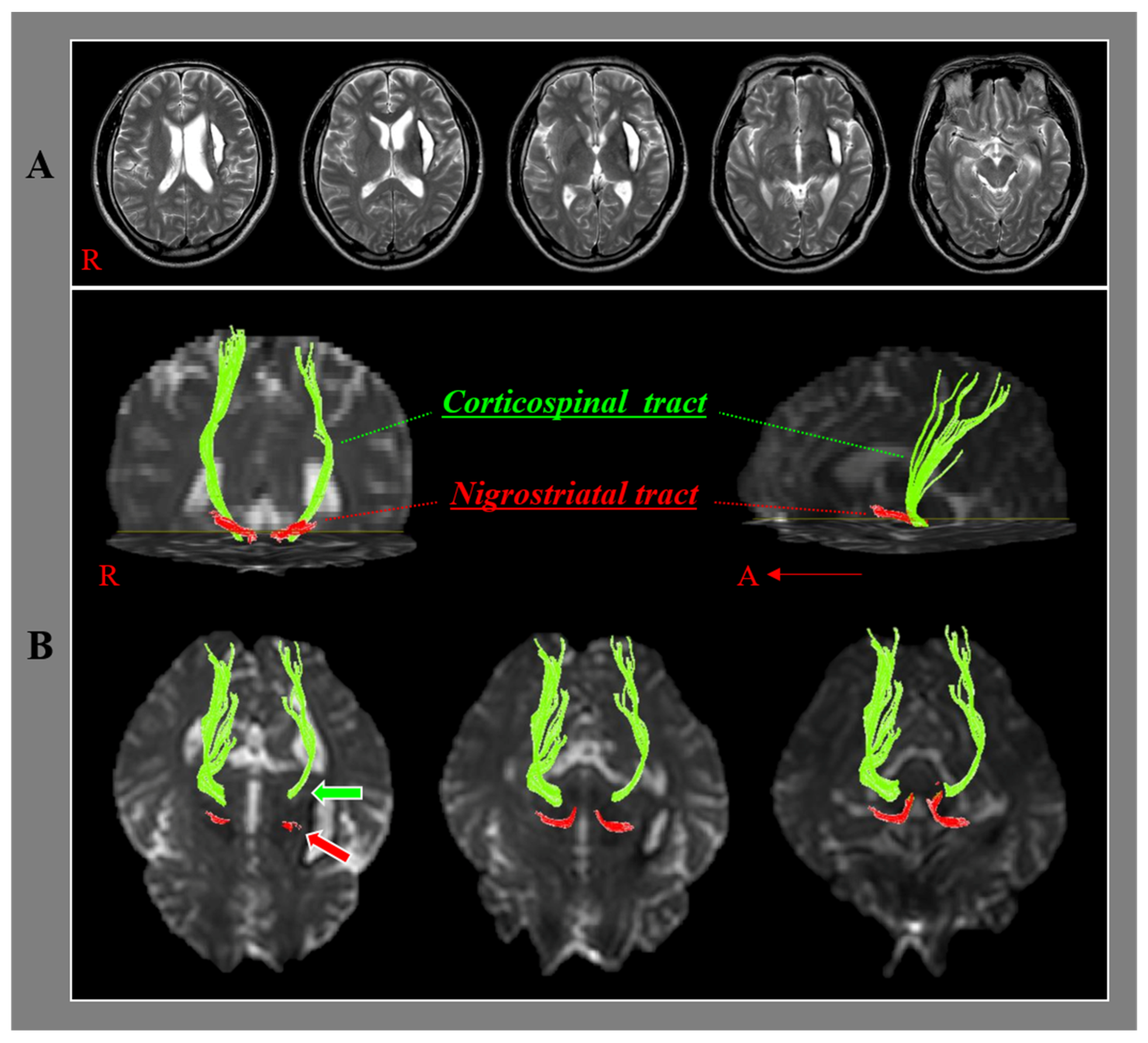
2.3. Diffusion Tensor Imaging and Tractography
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duncan, P.W.; Goldstein, L.B.; Matchar, D.; Divine, G.W.; Feussner, J. Measurement of motor recovery after stroke. Outcome assessment and sample size requirements. Stroke 1992, 23, 1084–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.H.; You, S.H.; Kwon, Y.H.; Hallett, M.; Lee, M.Y.; Ahn, S.H. Cortical reorganization associated lower extremity motor recovery as evidenced by functional MRI and diffusion tensor tractography in a stroke patient. Restor. Neurol. Neurosci. 2005, 23, 325–329. [Google Scholar] [PubMed]
- Cho, S.H.; Kim, D.G.; Kim, D.S.; Kim, Y.H.; Lee, C.H.; Jang, S.H. Motor outcome according to the integrity of the corticospinal tract determined by diffusion tensor tractography in the early stage of corona radiata infarct. Neurosci. Lett. 2007, 426, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Chang, C.H.; Lee, J.; Kim, C.S.; Seo, J.P.; Yeo, S.S. Functional role of the corticoreticular pathway in chronic stroke patients. Stroke 2013, 44, 1099–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puig, J.; Blasco, G.; Daunis-I-Estadella, J.; Thomalla, G.; Castellanos, M.; Figueras, J.; Remollo, S.; van Eendenburg, C.; Sanchez-Gonzalez, J.; Serena, J.; et al. Decreased corticospinal tract fractional anisotropy predicts long-term motor outcome after stroke. Stroke 2013, 44, 2016–2018. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H.; Kim, K.; Kim, S.H.; Son, S.M.; Jang, W.H.; Kwon, H.G. The relation between motor function of stroke patients and diffusion tensor imaging findings for the corticospinal tract. Neurosci. Lett. 2014, 572, 1–6. [Google Scholar] [CrossRef]
- Maraka, S.; Jiang, Q.; Jafari-Khouzani, K.; Li, L.; Malik, S.; Hamidian, H.; Zhang, T.; Lu, M.; Soltanian-Zadeh, H.; Chopp, M.; et al. Degree of corticospinal tract damage correlates with motor function after stroke. Ann. Clin. Transl. Neurol. 2014, 1, 891–899. [Google Scholar] [CrossRef]
- Jang, S.H.; Kim, D.H.; Kim, S.H.; Seo, J.P. The relation between the motor evoked potential and diffusion tensor tractography for the corticospinal tract in chronic hemiparetic patients with cerebral infarct. Somatosens. Mot. Res. 2017, 34, 134–138. [Google Scholar] [CrossRef]
- Yeo, S.S.; Jang, S.H.; Park, G.Y.; Oh, S. Effects of injuries to descending motor pathways on restoration of gait in patients with pontine hemorrhage. J. Stroke Cerebrovasc. Dis. 2020, 29, 104857. [Google Scholar] [CrossRef]
- Gong, Z.G.; Zhang, R.J.; Jiang, W.B.; Fu, Z.H. Integrity of the hand fibers of the corticospinal tract shown by diffusion tensor imaging predicts hand function recovery after hemorrhagic stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105447. [Google Scholar] [CrossRef]
- Ikemoto, S. Brain reward circuitry beyond the mesolimbic dopamine system: A neurobiological theory. Neurosci. Biobehav. Rev. 2010, 35, 129–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nambu, A. A new dynamic model of the cortico-basal ganglia loop. Prog. Brain Res. 2004, 143, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, A.V.; Freeze, B.S.; Parker, P.R.; Kay, K.; Thwin, M.T.; Deisseroth, K.; Kreitzer, A.C. Regulation of parkinsonian motor behaviours by optogenetic control of basal ganglia circuitry. Nature 2010, 466, 622–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravitz, A.V.; Kreitzer, A.C. Striatal mechanisms underlying movement, reinforcement, and punishment. Physiology 2012, 27, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Brooks, D.J.; Salmon, E.P.; Mathias, C.J.; Quinn, N.; Leenders, K.L.; Bannister, R.; Marsden, C.D.; Frackowiak, R.S. The relationship between locomotor disability, autonomic dysfunction, and the integrity of the striatal dopaminergic system in patients with multiple system atrophy, pure autonomic failure, and Parkinson’s disease, studied with PET. Brain 1990, 113 Pt 5, 1539–1552. [Google Scholar] [CrossRef] [PubMed]
- Kipps, C.M.; Duggins, A.J.; Mahant, N.; Gomes, L.; Ashburner, J.; McCusker, E.A. Progression of structural neuropathology in preclinical Huntington’s disease: A tensor based morphometry study. J. Neurol. Neurosurg. Psychiatry 2005, 76, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Obeso, J.A.; Rodriguez-Oroz, M.C.; Stamelou, M.; Bhatia, K.P.; Burn, D.J. The expanding universe of disorders of the basal ganglia. Lancet 2014, 384, 523–531. [Google Scholar] [CrossRef]
- Davidoff, R.A. The pyramidal tract. Neurology 1990, 40, 332–339. [Google Scholar] [CrossRef]
- Takakusaki, K.; Tomita, N.; Yano, M. Substrates for normal gait and pathophysiology of gait disturbances with respect to the basal ganglia dysfunction. J. Neurol. 2008, 255 (Suppl. 4), 19–29. [Google Scholar] [CrossRef]
- Jang, S.H. The corticospinal tract from the viewpoint of brain rehabilitation. J. Rehabil. Med. 2014, 46, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Awenowicz, P.W.; Porter, L.L. Local application of dopamine inhibits pyramidal tract neuron activity in the rodent motor cortex. J. Neurophysiol. 2002, 88, 3439–3451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosp, J.A.; Molina-Luna, K.; Hertler, B.; Atiemo, C.O.; Luft, A.R. Dopaminergic modulation of motor maps in rat motor cortex: An in vivo study. Neuroscience 2009, 159, 692–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Luna, K.; Pekanovic, A.; Rohrich, S.; Hertler, B.; Schubring-Giese, M.; Rioult-Pedotti, M.S.; Luft, A.R. Dopamine in motor cortex is necessary for skill learning and synaptic plasticity. PLoS ONE 2009, 4, e7082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosp, J.A.; Pekanovic, A.; Rioult-Pedotti, M.S.; Luft, A.R. Dopaminergic projections from midbrain to primary motor cortex mediate motor skill learning. J. Neurosci. 2011, 31, 2481–2487. [Google Scholar] [CrossRef] [Green Version]
- Vitrac, C.; Peron, S.; Frappe, I.; Fernagut, P.O.; Jaber, M.; Gaillard, A.; Benoit-Marand, M. Dopamine control of pyramidal neuron activity in the primary motor cortex via D2 receptors. Front. Neural Circuits 2014, 8, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cazorla, M.; Kang, U.J.; Kellendonk, C. Balancing the basal ganglia circuitry: A possible new role for dopamine D2 receptors in health and disease. Mov. Disord. 2015, 30, 895–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concha, L.; Gross, D.W.; Beaulieu, C. Diffusion tensor tractography of the limbic system. Am. J. Neuroradiol. 2005, 26, 2267–2274. [Google Scholar]
- Hong, J.H.; Son, S.M.; Jang, S.H. Somatotopic location of corticospinal tract at pons in human brain: A diffusion tensor tractography study. Neuroimage 2010, 51, 952–955. [Google Scholar] [CrossRef]
- Yeo, S.S.; Seo, J.P. The nigrostriatal tract between the substantia nigra and striatum in the human brain: A diffusion tensor tractography study. J. Korean Phys. Ther. 2020, 32, 388–390. [Google Scholar] [CrossRef]
- Jang, S.H.; Park, J.W.; Choi, B.Y.; Kim, S.H.; Chang, C.H.; Jung, Y.J.; Choi, W.H.; Seo, Y.S. Difference of recovery course of motor weakness according to state of corticospinal tract in putaminal hemorrhage. Neurosci. Lett. 2017, 653, 163–167. [Google Scholar] [CrossRef]
- Demeurisse, G.; Demol, O.; Robaye, E. Motor evaluation in vascular hemiplegia. Eur. Neurol. 1980, 19, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004, 23 (Suppl. 1), S208–S219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.J.; Korgaonkar, M.S.; Armstrong, L.V.; Eagles, S.; Williams, L.M.; Grieve, S.M. Tractography of the brainstem in major depressive disorder using diffusion tensor imaging. PLoS ONE 2014, 9, e84825. [Google Scholar] [CrossRef] [PubMed]
- Andica, C.; Kamagata, K.; Hatano, T.; Okuzumi, A.; Saito, A.; Nakazawa, M.; Ueda, R.; Motoi, Y.; Kamiya, K.; Suzuki, M.; et al. Neurite orientation dispersion and density imaging of the nigrostriatal pathway in Parkinson’s disease: Retrograde degeneration observed by tract-profile analysis. Parkinsonism Relat. Disord. 2018, 51, 55–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.H. Somatotopic arrangement and location of the corticospinal tract in the brainstem of the human brain. Yonsei Med. J. 2011, 52, 553–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunimatsu, A.; Aoki, S.; Masutani, Y.; Abe, O.; Hayashi, N.; Mori, H.; Masumoto, T.; Ohtomo, K. The optimal trackability threshold of fractional anisotropy for diffusion tensor tractography of the corticospinal tract. Magn. Reson. Med. Sci. 2004, 3, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.P.; Jang, S.H. Characteristics of corticospinal tract area according to pontine level. Yonsei Med. J. 2013, 54, 785–787. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef]
- Mori, S.; Crain, B.J.; Chacko, V.P.; van Zijl, P.C. Three-dimensional tracking of axonal projections in the brain by magnetic resonance imaging. Ann. Neurol. 1999, 45, 265–269. [Google Scholar] [CrossRef]
- Assaf, Y.; Pasternak, O. Diffusion tensor imaging (DTI)-based white matter mapping in brain research: A review. J. Mol. Neurosci. 2008, 34, 51–61. [Google Scholar] [CrossRef] [PubMed]
- De Groot, M.; Ikram, M.A.; Akoudad, S.; Krestin, G.P.; Hofman, A.; van der Lugt, A.; Niessen, W.J.; Vernooij, M.W. Tract-specific white matter degeneration in aging: The Rotterdam Study. Alzheimers Dement. 2015, 11, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Sakai, K.; Akazawa, K.; Yuen, S.; Nishimura, T. MR tractography: A review of its clinical applications. Magn. Reson. Med. Sci. 2009, 8, 165–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Patients | |
|---|---|
| Lesion side (right:left) | 18:25 |
| Mean duration to DTI (months) | 9.18 ± 8.72 |
| Motricity Index score | 55.95 ± 20.92 |
| Dependent Variable | Independent Variable | B | se | β | t | p | VIF |
|---|---|---|---|---|---|---|---|
| Motricity Index | Tract volume of NST | 0.144 | 0.062 | 0.356 | 2.328 | 0.03 * | 4.145 |
| Fractional anisotropy of CST | 31.640 | 22.898 | 0.144 | 1.382 | 0.18 | 1.919 | |
| Tract volume of CST | 0.019 | 0.006 | 0.449 | 2.902 | 0.01 * | 4.229 | |
| Adjusted R2 = 0.763 F = 45.998 p = 0.00 * | |||||||
| Step | Dependent Variable | Independent Variable | B | se | β | t | p | Adjusted R2 |
|---|---|---|---|---|---|---|---|---|
| 1 | Tract volume of CST | Tract volume of NST | 8.465 | 0.771 | 0.864 | 10.977 | 0.00 * | 0.740 |
| 2 | Motricity Index | Tract volume of NST | 0.340 | 0.034 | 0.839 | 9.881 | 0.00 * | 0.697 |
| 3 | Motricity Index | Tract volume of NST | 0.163 | 0.061 | 0.403 | 2.674 | 0.01 * | 0.757 |
| Tract volume of CST | 0.021 | 0.006 | 0.504 | 3.344 | 0.00 * | |||
| Sobel test Z = 3.34 * | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, S.H.; Cho, M.J. Relationship of the Nigrostriatal Tract with the Motor Function and the Corticospinal Tract in Chronic Hemiparetic Stroke Patients: A Diffusion Tensor Imaging Study. Healthcare 2022, 10, 731. https://doi.org/10.3390/healthcare10040731
Jang SH, Cho MJ. Relationship of the Nigrostriatal Tract with the Motor Function and the Corticospinal Tract in Chronic Hemiparetic Stroke Patients: A Diffusion Tensor Imaging Study. Healthcare. 2022; 10(4):731. https://doi.org/10.3390/healthcare10040731
Chicago/Turabian StyleJang, Sung Ho, and Min Jye Cho. 2022. "Relationship of the Nigrostriatal Tract with the Motor Function and the Corticospinal Tract in Chronic Hemiparetic Stroke Patients: A Diffusion Tensor Imaging Study" Healthcare 10, no. 4: 731. https://doi.org/10.3390/healthcare10040731