
COVID-19 Pandemic Impact on Surgical Treatment Methods for Early-Stage Cervical Cancer: A Population-Based Study in Romania


 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Study Variables and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Peng, F. Patterns of metastases in cervical cancer: A population-based study. Int. J. Clin. Exp. Pathol. 2020, 13, 1615–1623. [Google Scholar] [PubMed]
- Hattori, S.; Yoshikawa, N.; Mogi, K.; Yoshida, K.; Yoshihara, M.; Tamauchi, S.; Ikeda, Y.; Yokoi, A.; Nishino, K.; Niimi, K.; et al. Significance of Concurrent Chemoradiotherapy as Primary Treatment in Patients with Metastatic Cervical Cancer. Curr. Oncol. 2021, 28, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, N.; Berek, J.; Cuello, M.; Fredes, M.C.; Denny, L.A.; Grenman, K.K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. New revised FIGO staging of cervical cancer. Abstract S020.2. Presented at the FIGO XXII World Congress of Gynecology and Obstetrics, Rio de Janeiro, Brazil, 14–19 October 2018. [Google Scholar] [CrossRef] [Green Version]
- Thomakos, N.; Trachana, S.-P.; Davidovic-Grigoraki, M.; Rodolakis, A. Less radical surgery for early-stage cervical cancer: To what extent do we justify it?—Our belief. Taiwan. J. Obstet. Gynecol. 2016, 55, 495–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swailes, A.L.; Gockley, A.; Phaëton, R.; Kesterson, J.P. The Wertheim hysterectomy: Development, modifications, and impact in the present day. Gynecol. Oncol. 2017, 145, 3–8. [Google Scholar] [CrossRef]
- Ekdahl, L.; Wallin, E.; Alfonzo, E.; Reynisson, P.; Lönnerfors, C.; Dahm-Kähler, P.; Falconer, H.; Persson, J. Increased Institutional Surgical Experience in Robot-Assisted Radical Hysterectomy for Early Stage Cervical Cancer Reduces Recurrence Rate: Results from a Nationwide Study. J. Clin. Med. 2020, 9, 3715. [Google Scholar] [CrossRef]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-COV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef]
- Yang, K.; Sheng, Y.; Huang, C.; Jin, Y.; Xiong, N.; Jiang, K.; Lu, H.; Liu, J.; Yang, J.; Dong, Y.; et al. Clinical characteristics, outcomes, and risk factors for mortality in patients with cancer and COVID-19 in Hubei, China: A multicentre, retrospective, cohort study. Lancet Oncol. 2020, 21, 904–913. [Google Scholar] [CrossRef]
- Russell, B.; Moss, C.; Palmer, K.; Sylva, R.; D’Souza, A.; Wylie, H.; Haire, A.; Cahill, F.; Steel, R.; Hoyes, A.; et al. COVID-19 Risk Factors for Cancer Patients: A First Report with Comparator Data from COVID-19 Negative Cancer Patients. Cancers 2021, 13, 2479. [Google Scholar] [CrossRef]
- Seth, G.; Sethi, S.; Bhattarai, S.; Saini, G.; Singh, C.; Aneja, R. SARS-CoV-2 Infection in Cancer Patients: Effects on Disease Outcomes and Patient Prognosis. Cancers 2020, 12, 3266. [Google Scholar] [CrossRef]
- Quaquarini, E.; Saltalamacchia, G.; Presti, D.; Caldana, G.; Tibollo, V.; Malovini, A.; Palumbo, R.; Teragni, C.M.; Balletti, E.; Mollica, L.; et al. Impact of COVID-19 Outbreak on Cancer Patient Care and Treatment: Data from an Outpatient Oncology Clinic in Lombardy (Italy). Cancers 2020, 12, 2941. [Google Scholar] [CrossRef] [PubMed]
- Ali, J.K.; Riches, J.C. The Impact of the COVID-19 Pandemic on Oncology Care and Clinical Trials. Cancers 2021, 13, 5924. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Elit, L.; Fyles, A.; Oliver, T.K.; Devries-Aboud, M.C.; Fung-Kee-Fung, M.; Members of the Gynecology Cancer Disease Site Group of Cancer Care Ontario’s Program in Evidence-Based Care. Follow-Up for Women after Treatment for Cervical Cancer. Curr. Oncol. 2010, 17, 65–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hata, M.; Koike, I.; Miyagi, E.; Numazaki, R.; Asai-Sato, M.; Kasuya, T.; Kaizu, H.; Matsui, T.; Hirahara, F.; Inoue, T. Radiation therapy for pelvic lymph node metastasis from uterine cervical cancer. Gynecol. Oncol. 2013, 131, 99–102. [Google Scholar] [CrossRef]
- Grigoraş, M.L.; Arghirescu, T.S.; Folescu, R.; Talpoş, I.C.; Gîndac, C.M.; Zamfir, C.; Cornianu, M.; Anghel, M.D.; Levai, C.M. Expression of E-cadherin in lung carcinoma, other than those with small cells (NSCLC). Romanian J. Morphol. Embryol. 2017, 58, 1317–1325. [Google Scholar]
- Wenzel, H.H.; Smolders, R.G.; Beltman, J.J.; Lambrechts, S.; Trum, H.W.; Yigit, R.; Zusterzeel, P.L.; Zweemer, R.P.; Mom, C.H.; Bekkers, R.L.; et al. Survival of patients with early-stage cervical cancer after abdominal or laparoscopic radical hysterectomy: A nationwide cohort study and literature review. Eur. J. Cancer 2020, 133, 14–21. [Google Scholar] [CrossRef]
- Li, Y.; Kong, Q.; Wei, H.; Wang, Y. Comparison of the complications between minimally invasive surgery and open surgical treatments for early-stage cervical cancer: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0253143. [Google Scholar] [CrossRef]
- Dobrescu, A.; Copaescu, C.; Zmeu, B.; Duta, C.; Bedreag, O.H.; Stoica, L.; Tarta, C.; Rogobete, A.F.; Lazar, F. Ghrelin Levels and Hunger Sensation after Laparoscopic Sleeve Gastrectomy Compared with Laparoscopic Greater Curvature Plication in Obese Patients. Clin. Lab. 2020, 66. [Google Scholar] [CrossRef]
- Velciov, S.; Gluhovschi, G.; Timar, R.; Gluhovschi, C.; Petrica, L.; Bob, F.; Bozdog, G.; Pricop, M.; Gluhovschi, A.; Cornianu, M.; et al. Urinary enzymatic markers (N-acetyl-beta-D-glucosaminidase) in assessing the tubulointerstitial compartment in chronic glomerulonephritis related to odontogenic foci. Wien. Klin. Wochenschr. 2015, 128, 102–108. [Google Scholar] [CrossRef]
- Siminel, M.A.; Neamţu, C.O.; DiŢescu, D.; Forţofoiu, M.C.; Comănescu, A.C.; Novac, M.B.; Neamţu, S.D.; Gluhovschi, A. Apert syndrome—Clinical case. Rom. J. Morphol. Embryol. 2017, 58, 277–280. [Google Scholar] [PubMed]
- Yan, D.-D.; Tang, Q.; Chen, J.-H.; Tu, Y.-Q.; Lv, X.-J. Prognostic value of the 2018 FIGO staging system for cervical cancer patients with surgical risk factors. Cancer Manag. Res. 2019, ume 11, 5473–5480. [Google Scholar] [CrossRef] [Green Version]
- Alessandrescu-Rusescu. National Institute for Maternal and Child Health. Active Early Detection of Cervical Cancer by Papanicolau Testing. Available online: https://www.insmc.ro/programe-de-sanatate/programe-de-sanatate-finantate-de-ms/programele-nationale-de-sanatate-privind-bolile-netransmisibile/programul-national-de-depistare-activa-precoce-a-cancerului-de-col-uterin/ (accessed on 10 December 2021).
- Gorun, F.; Motoi, S.; Malita, D.; Navolan, D.B.; Nemescu, D.; Olariu, T.R.; Craina, M.; Vilibic-Cavlek, T.; Ciohat, I.; Boda, D.; et al. Cytomegalovirus seroprevalence in pregnant women in the western region of Romania: A large-scale study. Exp. Ther. Med. 2020, 20, 2439–2443. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Mandelbaum, R.S.; Machida, H.; Purushotham, S.; Grubbs, B.H.; Roman, L.D.; Wright, J.D. Association of tumor differentiation grade and survival of women with squamous cell carcinoma of the uterine cervix. J. Gynecol. Oncol. 2018, 29, e91. [Google Scholar] [CrossRef] [PubMed]
- Michalas, S.; Rodolakis, A.; Voulgaris, Z.; Vlachos, G.; Giannakoulis, N.; Diakomanolis, E. Management of Early-Stage Cervical Carcinoma by Modified (Type II) Radical Hysterectomy. Gynecol. Oncol. 2002, 85, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, F.; Garbi, A. Change in practice in gynecologic oncology during the COVID-19 pandemic: A social media survey. Int. J. Gynecol. Cancer 2020, 30, 1101–1107. [Google Scholar] [CrossRef]
- Jouen, T.; Gauthier, T.; Azais, H.; Bendifallah, S.; Chauvet, P.; Fernandez, H.; Kerbage, Y.; Lavoue, V.; Lecointre, L.; Mimoun, C.; et al. The impact of the COVID-19 coronavirus pandemic on the surgical management of gynecological cancers: Analysis of the multicenter database of the French SCGP and the FRANCOGYN group. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102133. [Google Scholar] [CrossRef]
- Gupta, N.; Chauhan, A.S.; Prinja, S.; Pandey, A.K. Impact of COVID-19 on Outcomes for Patients With Cervical Cancer in India. JCO Glob. Oncol. 2021, 7, 716–725. [Google Scholar] [CrossRef]
- Kregting, L.M.; Kaljouw, S.; de Jonge, L.; Jansen, E.E.L.; Peterse, E.F.P.; Heijnsdijk, E.A.M.; van Ravesteyn, N.T.; Lansdorp-Vogelaar, I.; de Kok, I.M.C.M. Effects of cancer screening restart strategies after COVID-19 disruption. Br. J. Cancer 2021, 124, 1516–1523. [Google Scholar] [CrossRef]
- Matsuo, K.; Huang, Y.; Matsuzaki, S.; Ragab, O.M.; Roman, L.D.; Wright, J.D. Association between definitive chemoradiotherapy wait-time and survival in locally-advanced cervical cancer: Implications during the coronavirus pandemic. Gynecol. Oncol. 2021, 161, 414–421. [Google Scholar] [CrossRef]
- Matsuo, K.; Novatt, H.; Matsuzaki, S.; Hom, M.S.; Castaneda, A.V.; Licon, E.; Nusbaum, D.J.; Roman, L.D. Wait-time for hysterectomy and survival of women with early-stage cervical cancer: A clinical implication during the coronavirus pandemic. Gynecol. Oncol. 2020, 158, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.M.; Spencer, A.; Macdonald, S.; Dobson, L.; Haydock, E.; Burton, H.; Angelopoulos, G.; Martin-Hirsch, P.; Wood, N.J.; Thangavelu, A.; et al. Cervical cancer and COVID—An assessment of the initial effect of the pandemic and subsequent projection of impact for women in England: A cohort study. BJOG Int. J. Obstet. Gynaecol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Huang, Y.; Matsuzaki, S.; Deshpande, R.R.; Klar, M.; Roman, L.D.; Wright, J.D. Association between hysterectomy wait-time and all-cause mortality for micro-invasive cervical cancer: Treatment implications during the coronavirus pandemic. Arch. Gynecol. Obstet. 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables * | Pre-Pandemic (n = 340) | During Pandemic (n = 52) | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 38.6 ± 8.1 | 37.4 ± 8.6 | 0.324 |
| BMI, kg/m2 (mean ± SD) | 23.3 ± 4.4 | 23.8 ± 5.2 | 0.457 |
| Tumor size, n (%) | 0.248 | ||
| <2 cm | 133 (39.2%) | 16 (30.3%) | |
| ≥2 cm | 207 (60.8%) | 36 (69.2%) | |
| FIGO stage, n (%) | 0.047 | ||
| I | 135 (39.7%) | 11 (21.1%) | |
| II | 82 (24.1%) | 13 (25.0%) | |
| III | 76 (22.4%) | 18 (34.6%) | |
| IV | 47 (13.8%) | 10 (19.2%) | |
| Differentiation grade, n (%) | 0.942 | ||
| Grade 1 | 191 (56.2%) | 29 (55.7%) | |
| Grade 2 | 105 (30.9%) | 17 (32.7%) | |
| Grade 3 | 44 (12.9%) | 6 (11.6%) | |
| Histology | 0.755 | ||
| Squamous-cell | 268 (78.8%) | 40 (76.9%) | |
| Adenocarcinoma | 72 (21.2%) | 12 (23.1%) | |
| Outcomes | |||
| Change in treatment plan | 41 (12.1%) | 12 (23.1%) | 0.030 |
| Postponed surgery | 32 (9.4%) | 11 (21.2%) | 0.011 |
| Postponed radio-chemotherapy | 44 (12.9%) | 15 (28.8%) | 0.002 |
| ICU hospitalization | 23 (6.8%) | 6 (11.5%) | 0.220 |
| Mortality | 20 (5.9%) | 4 (7.7%) | 0.612 |
| Characteristics * | SARS-CoV-2 Negative (n = 128) | SARS-CoV-2 Positive (n = 32) | p-Value |
|---|---|---|---|
| Age, years | 38.0 ± 9.4 | 39.2 ± 9.1 | 0.516 |
| BMI, kg/m2 | 26.4 ± 3.5 | 27.8 ± 4.4 | 0.057 |
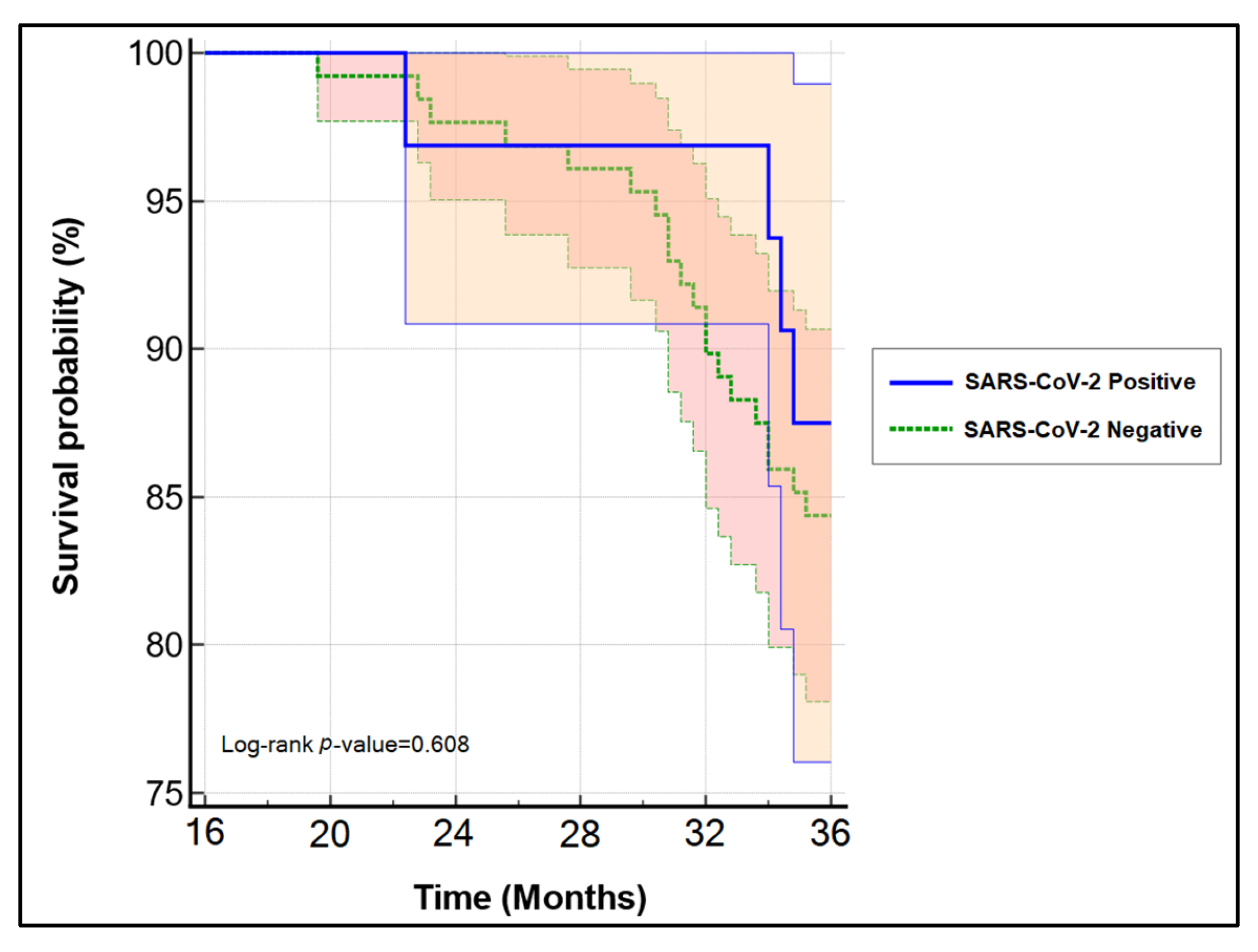
| Overall survival | 108 (84.4%) | 28 (87.5%) | 0.657 |
| DFS **, months, (median[IQR]) | 34 [31–36] | 33 [30–36] | 0.531 |
| Follow-up, months, (median[IQR]) | 34 [28–36] | 34 [29–36] | 0.948 |
| Surgical treatment type | 0.076 | ||
| Robot surgery | 16 (12.5%) | 8 (25.0%) | |
| Open surgery | 112 (87.5%) | 24 (75.0%) | |
| Tumor size | 0.871 | ||
| <2 cm | 50 (39.1%) | 12 (37.5%) | |
| ≥2 cm | 78 (60.9%) | 20 (62.5%) | |
| Lymph node involvement | 0.141 | ||
| 0 | 94 (73.4%) | 18 (56.3%) | |
| 1 | 12 (9.4%) | 6 (18.7%) | |
| >1 | 22 (17.2%) | 8 (25.0%) | |
| FIGO stage | 0.490 | ||
| IA2 | 40 (31.3%) | 8 (25.0%) | |
| IB1 | 88 (68.7%) | 24 (75.0%) | |
| Differentiation grade | 0.967 | ||
| Grade 1 | 74 (57.8%) | 18 (56.3%) | |
| Grade 2 | 40 (31.2%) | 10 (31.3%) | |
| Grade 3 | 14 (11.0%) | 4 (12.4%) | |
| Relapse (n = 38) | 0.868 | ||
| Local | 16 (12.4%) | 3 (9.4%) | |
| Regional | 8 (6.3%) | 2 (6.3%) | |
| Distant | 8 (6.3%) | 1 (3.2%) | |
| Total | 32 (25.0%) | 6 (18.8%) | |
| Histology | 0.223 | ||
| Squamous-cell | 111 (86.7%) | 25 (78.1%) | |
| Adenocarcinoma | 17 (13.3%) | 7 (21.9%) | |
| Adjuvant treatment | 0.762 | ||
| Radiotherapy-only | 20 (15.6%) | 8 (25.0%) | |
| Chemotherapy-only | 5 (3.9%) | 3 (9.4%) | |
| Radio-chemotherapy | 6 (4.7%) | 4 (12.4%) | |
| Clavien-Dindo scale | Classic surgery | Robotic surgery | 0.031 |
| No complications | 45 (35.2%) | 20 (62.5%) | |
| Score 1 | 52 (40.6%) | 8 (25.0%) | |
| Score 2 | 24 (18.8%) | 2 (6.25%) | |
| Score 3 | 7 (5.4%) | 2 (6.25%) |
| Factor | Odds Ratio | Confidence Interval | p-Value |
|---|---|---|---|
| Tumor Size (≥2 cm) | 1.8 | 1.4–2.5 | 0.022 |
| Relapse | 4.2 | 3.1–5.8 | <0.001 |
| High Grade | 5.1 | 3.3–7.2 | <0.001 |
| SARS-CoV-2 infection | 1.3 | 0.7–1.9 | 0.246 |
| Lymph Nodes (≥2) | 2.9 | 1.6–3.6 | 0.003 |
| Clavien–Dindo (≥3) | 1.5 | 0.9–1.9 | 0.085 |
| Change in treatment plan | 1.3 | 0.9–1.6 | 0.104 |
| Postponed surgery * | 1.1 | 0.8–1.3 | 0.417 |
| Postponed radio-chemotherapy * | 1.3 | 0.8–1.7 | 0.115 |
| First Author (Year) | Conclusions |
|---|---|
| Gupta et al. (2021) [30] | A 2.52% to 3.80% increase in cervical cancer-related deaths with treatment delays ranging from 9 weeks to 6 months. |
| Kregting et al. (2021) [31] | An increase of 2.0, 0.3, and 2.5 cancer deaths per 100,000 individuals in 10 years. |
| Matsuo et al. (2021) [32] | Wait-time of 6.1–9.8 weeks for cervical cancer treatment was not associated with increased risk of all-cause mortality compared to a wait-time of 6 weeks. |
| Matsuo et al. (2021) [33] | In women with early-stage cervical cancer, an 8-week delay for hysterectomy may not be related with short-term disease recurrence and shorter DFS. |
| Davies et al. (2022) [34] | Over the next 3 years, there is anticipated considerable rise in newly-diagnosed cervical cancer cases. Increased surgical capacity might alleviate this burden with no significant morbidity or mortality increase. |
| Matsuo et al. (2021) [35] | Postponing hysterectomy for 6–8 weeks is appropriate for women with early-stage cervical cancer in centers or areas with a high prevalence of COVID-19 illness and has no detrimental effect on survival. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popescu, A.; Craina, M.; Pantea, S.; Pirvu, C.; Radu, D.; Marincu, I.; Bratosin, F.; Bogdan, I.; Hosin, S.; Citu, C.; et al. COVID-19 Pandemic Impact on Surgical Treatment Methods for Early-Stage Cervical Cancer: A Population-Based Study in Romania. Healthcare 2022, 10, 639. https://doi.org/10.3390/healthcare10040639
Popescu A, Craina M, Pantea S, Pirvu C, Radu D, Marincu I, Bratosin F, Bogdan I, Hosin S, Citu C, et al. COVID-19 Pandemic Impact on Surgical Treatment Methods for Early-Stage Cervical Cancer: A Population-Based Study in Romania. Healthcare. 2022; 10(4):639. https://doi.org/10.3390/healthcare10040639
Chicago/Turabian StylePopescu, Alin, Marius Craina, Stelian Pantea, Catalin Pirvu, Daniela Radu, Iosif Marincu, Felix Bratosin, Iulia Bogdan, Samer Hosin, Cosmin Citu, and et al. 2022. "COVID-19 Pandemic Impact on Surgical Treatment Methods for Early-Stage Cervical Cancer: A Population-Based Study in Romania" Healthcare 10, no. 4: 639. https://doi.org/10.3390/healthcare10040639