
A Comparison between Conventional and Extracorporeal Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Selection and Selection Criteria
2.2. Outcomes
2.3. Quality Assessment
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Quality
3.3. Summary of Studies
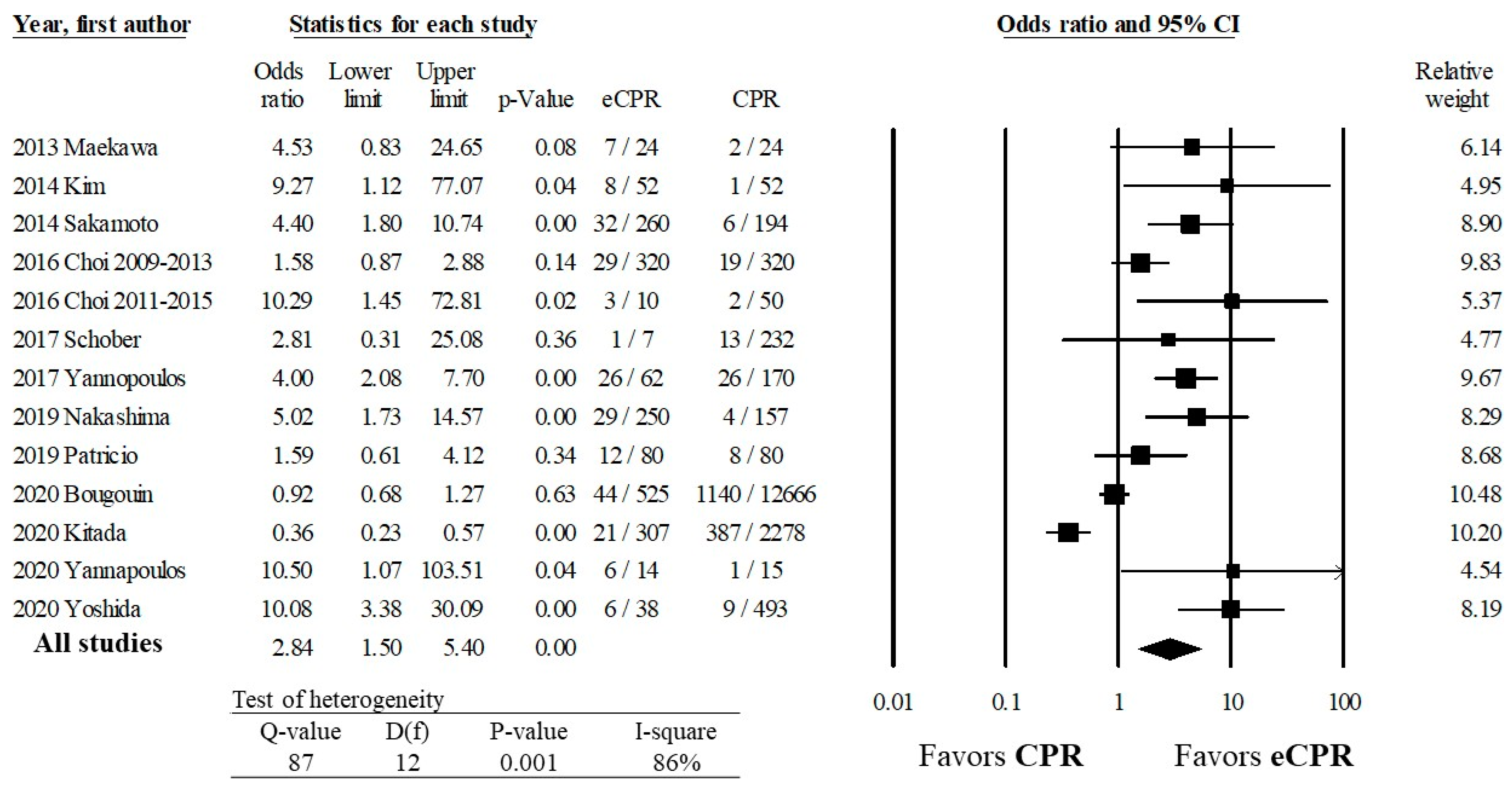
3.4. Primary Outcome: Any Favorable Outcome
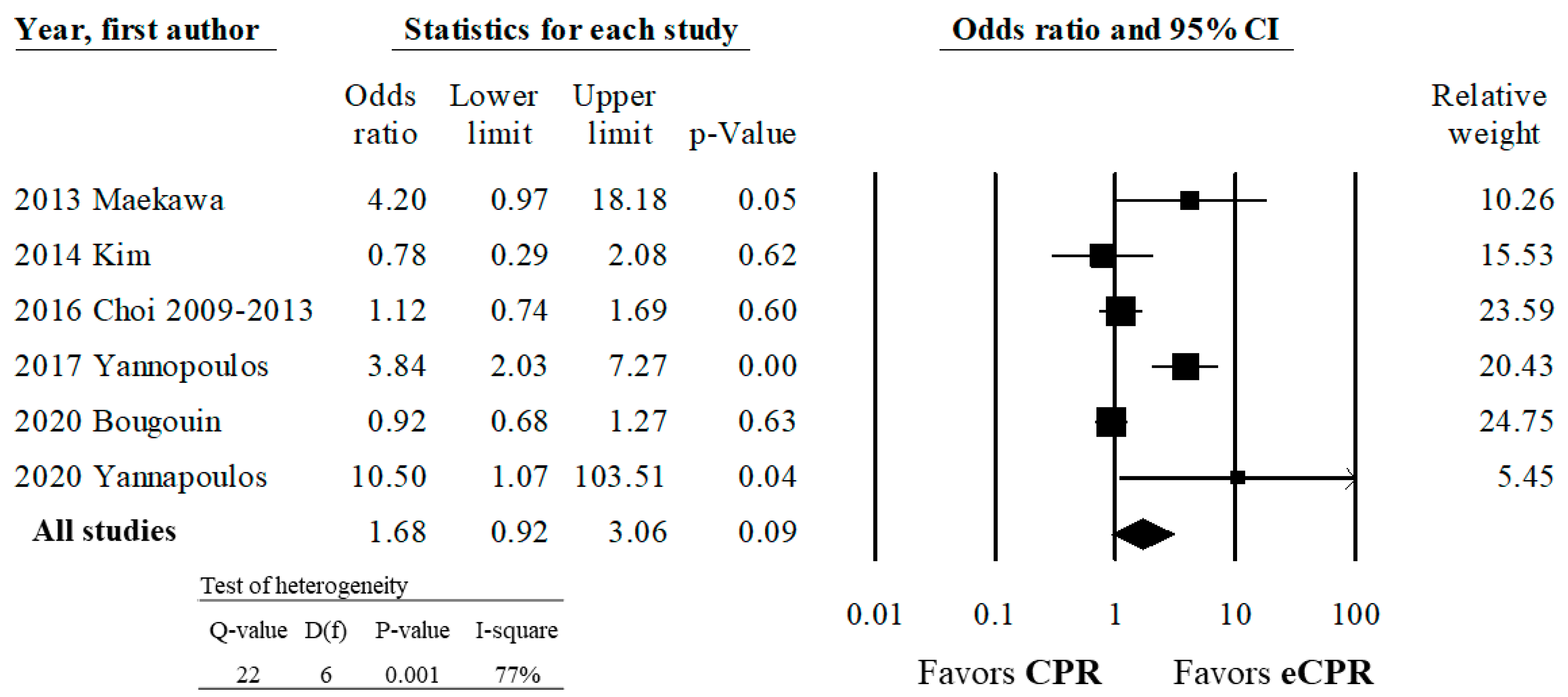
3.5. Sensitivity Analysis
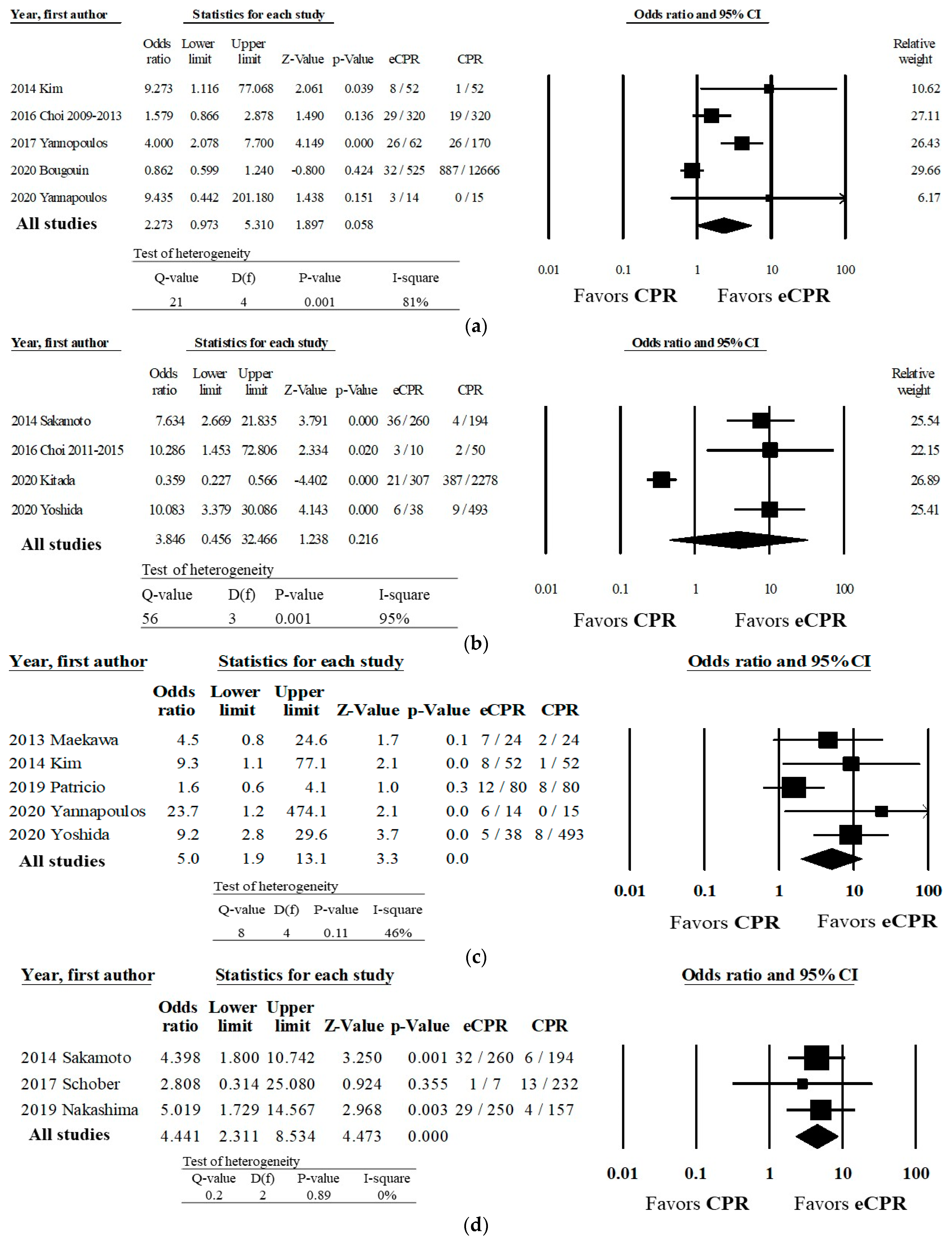
3.6. Subgroup Analysis
3.7. Secondary Outcomes
3.7.1. Survival to Hospital Discharge
3.7.2. Favorable Neurologic Outcomes
4. Discussion
4.1. Implications for Future Research
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Nakahara, S.; Tomio, J.; Ichikawa, M.; Nakamura, F.; Nishida, M.; Takahashi, H.; Morimura, N.; Sakamoto, T. Association of Bystander Interventions With Neurologically Intact Survival Among Patients With Bystander-Witnessed Out-of-Hospital Cardiac Arrest in Japan. JAMA 2015, 314, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, T.; Brady, W. The “Code Drugs in Cardiac Arrest”—The use of cardioactive medications in cardiac arrest resuscitation. Am. J. Emerg. Med. 2012, 30, 811–818. [Google Scholar] [CrossRef]
- Yan, S.; Gan, Y.; Jiang, N.; Wang, R.; Chen, Y.; Luo, Z.; Zong, Q.; Chen, S.; Lv, C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: A systematic review and meta-analysis. Crit. Care 2020, 24, 61. [Google Scholar] [CrossRef] [Green Version]
- Goto, Y.; Funada, A.; Goto, Y. Relationship Between the Duration of Cardiopulmonary Resuscitation and Favorable Neurological Outcomes After Out-of-Hospital Cardiac Arrest: A Prospective, Nationwide, Population-Based Cohort Study. J. Am. Heart Assoc. 2016, 5, e002819. [Google Scholar] [CrossRef] [Green Version]
- Squiers, J.J.; Lima, B.; DiMaio, J.M. Contemporary extracorporeal membrane oxygenation therapy in adults: Fundamental principles and systematic review of the evidence. J. Thorac. Cardiovasc. Surg. 2016, 152, 20–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yannopoulos, D.; Bartos, J.; Raveendran, G.; Walser, E.; Connett, J.; A Murray, T.; Collins, G.; Zhang, L.; Kalra, R.; Kosmopoulos, M.; et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): A phase 2, single centre, open-label, randomised controlled trial. Lancet 2020, 396, 1807–1816. [Google Scholar] [CrossRef]
- Downing, J.; Al Falasi, R.; Cardona, S.; Fairchild, M.; Lowie, B.; Chan, C.; Powell, E.; Pourmand, A.; Tran, Q.K. How effective is extracorporeal cardiopulmonary resuscitation (ECPR) for out-of-hospital cardiac arrest? A systematic review and meta-analysis. Am. J. Emerg. Med. 2021, 51, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Buick, J.E.; Drennan, I.R.; Scales, D.C.; Brooks, S.C.; Byers, A.; Cheskes, S.; Dainty, K.N.; Feldman, M.; Verbeek, P.R.; Zhan, C.; et al. Improving Temporal Trends in Survival and Neurological Outcomes After Out-of-Hospital Cardiac Arrest. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e003561. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Ruttmann, E.; Weissenbacher, A.; Ulmer, H.; Müller, L.; Höfer, D.; Kilo, J.; Rabl, W.; Schwarz, B.; Laufer, G.; Antretter, H.; et al. Prolonged extracorporeal membrane oxygenation-assisted support provides improved survival in hypothermic patients with cardiocirculatory arrest. J. Thorac. Cardiovasc. Surg. 2007, 134, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunne, B.; Christou, E.; Duff, O.; Merry, C. Extracorporeal-assisted rewarming in the management of accidental deep hypothermic cardiac arrest: A systematic review of the literature. Heart Lung. Circ. 2014, 23, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. Lancet 1975, 1, 480–484. [Google Scholar] [CrossRef]
- Ajam, K.; Gold, L.S.; Beck, S.S.; Damon, S.; Phelps, R.; Rea, T.D. Reliability of the Cerebral Performance Category to classify neurological status among survivors of ventricular fibrillation arrest: A cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2011, 19, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Metaanalyse. Published Online 2000. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 2 August 2019).
- Cummins, R.O.; Chamberlain, D.A.; Abramson, N.S.; Allen, M.; Baskett, P.J.; Becker, L.; Bossaert, L.; Delooz, H.H.; Dick, W.F.; Eisenberg, M.S. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: The Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991, 84, 960–975. [Google Scholar] [CrossRef] [Green Version]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Yannopoulos, D.; Bartos, J.; Raveendran, G.; Conterato, M.; Frascone, R.J.; Trembley, A.; John, R.; Connett, J.; Benditt, D.G.; Lurie, K.G.; et al. Coronary Artery Disease in Patients With Out-of- Hospital Refractory Ventricular Fibrillation Cardiac Arrest. J. Am. Coll. Cardiol. 2017, 70, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, T.; Morimura, N.; Nagao, K.; Asai, Y.; Yokota, H.; Nara, S.; Hase, M.; Tahara, Y.; Atsumi, T. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: A prospective observational study. Resuscitation 2014, 85, 762–768. [Google Scholar] [CrossRef]
- Bougouin, W.; Dumas, F.; Lamhaut, L.; Marijon, E.; Carli, P.; Combes, A.; Pirracchio, R.; Aissaoui, N.; Karam, N.; Deye, N.; et al. Extracorporeal cardiopulmonary resuscitation in out-of hospital cardiac arrest: A registry study. Eur. Heart J. 2020, 41, 1961–1971. [Google Scholar] [CrossRef]
- Choi, D.-H.; Kim, Y.-J.; Ryoo, S.M.; Sohn, C.H.; Ahn, S.; Seo, N.-W.; Lim, J.Y.; Kim, W.Y. Extracorporeal cardiopulmonary resuscitation among patients with out-of-hospital cardiac arrest. Clin. Exp. Emerg. Med. 2016, 3, 132–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, D.S.; Kim, T.; Ro, Y.S.; Ahn, K.O.; Lee, E.J.; Hwang, S.S.; Song, S.W.; Song, K.J.; Shin, S.D. Extracorporeal life support and survival after out-of-hospital cardiac arrest in a nationwide registry: A propensity score-matched analysis. Resuscitation 2016, 99, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Jung, J.S.; Park, J.H.; Park, J.S.; Hong, Y.S.; Lee, S.W. An optimal transition time to extracorporeal cardiopulmonary resuscitation for predicting good neurological outcome in patients with out-of-hospital cardiac arrest: A propensity-matched study. Crit. Care 2014, 18, 535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitada, M.; Kaneko, T.; Yamada, S.; Harada, M.; Takahashi, T. Extracorporeal cardiopulmonary resuscitation without target temperature management for out-of-hospital cardiac arrest patients prolongs the therapeutic time window: A retrospective analysis of a nationwide multicentre observational study in Japan. J. Intensive Care 2020, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, K.; Tanno, K.; Hase, M.; Mori, K.; Asai, Y. Extracorporeal Cardiopulmonary Resuscitation for Patients With Out-of-Hospital Cardiac Arrest of Cardiac Origin: A Propensity-Matched Study and Predictor Analysis. Crit. Care Med. 2013, 41, 1186–1196. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, T.; Noguchi, T.; Tahara, Y.; Nishimura, K.; Ogata, S.; Yasuda, S.; Onozuka, D.; Morimura, N.; Nagao, K.; Gaieski, D.F.; et al. Patients With Refractory Out-of-Cardiac Arrest and Sustained Ventricular Fibrillation as Candidates for Extracorporeal Cardiopulmonary Resuscitation—Prospective Multi-Center Observational Study. Circ. J. Off. J. Jpn. Circ. Soc. 2019, 83, 1011–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patricio, D.; Peluso, L.; Brasseur, A.; Lheureux, O.; Belliato, M.; Vincent, J.-L.; Creteur, J.; Taccone, F.S. Comparison of extracorporeal and conventional cardiopulmonary resuscitation: A retrospective propensity score matched study. Crit. Care 2019, 23, 27. [Google Scholar] [CrossRef] [Green Version]
- Schober, A.; Sterz, F.; Herkner, H.; Wallmueller, C.; Weiser, C.; Hubner, P.; Testori, C. Emergency extracorporeal life support and ongoing resuscitation: A retrospective comparison for refractory out-of-hospital cardiac arrest. Emerg. Med. J. 2017, 34, 277–281. [Google Scholar] [CrossRef]
- Yoshida, T.; Fujitani, S.; Wakatake, H.; Kitano, Y.; Yoshida, M.; Tsutsumi, K.; Masui, Y.; Taira, Y. Exploratory Observational Study of Extracorporeal Cardiopulmonary Resuscitation for Nonshockable Out-Of-Hospital Cardiac Arrest Occurring After an Emergency Medical Services Arrival: SOS-KANTO 2012 Study Report. J. Emerg. Med. 2020, 58, 375–384. [Google Scholar] [CrossRef]
- Riddersholm, S.; Kragholm, K.; Mortensen, R.N.; Hansen, S.M.; Wissenberg, M.; Lippert, F.K.; Torp-Pedersen, C.; Christiansen, C.F.; Rasmussen, B.S. Organ support therapy in the intensive care unit and return to work in out-of-hospital cardiac arrest survivors-A nationwide cohort study. Resuscitation 2018, 125, 126–134. [Google Scholar] [CrossRef]
- Sawyer, K.N.; Elmer, J. Measuring and improving outcomes that matter to patients after cardiac arrest. Resuscitation 2018, 125, A1–A2. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.; Zmudzki, F.; Burns, B.; Scott, S.; Gattas, D.; Reynolds, C.; Buscher, H.; Forrest, P. Cost effectiveness and quality of life analysis of extracorporeal cardiopulmonary resuscitation (ECPR) for refractory cardiac arrest. Resuscitation 2019, 139, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, Y.; Goto, R.; Atsumi, T.; Morimura, N.; Nagao, K.; Tahara, Y.; Asai, Y.; Yokota, H.; Ariyoshi, K.; Yamamoto, Y.; et al. Cost-effectiveness of extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest: A multi-centre prospective cohort study. Resuscitation 2020, 157, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Bharmal, M.I.; Venturini, J.M.; Chua, R.F.; Sharp, W.W.; Beiser, D.G.; Tabit, C.E.; Hirai, T.; Rosenberg, J.R.; Friant, J.; Blair, J.E.; et al. Cost-utility of extracorporeal cardiopulmonary resuscitation in patients with cardiac arrest. Resuscitation 2019, 136, 126–130. [Google Scholar] [CrossRef]
- Bonacchi, M.; Cabrucci, F.; Bugetti, M.; Dokollari, A.; Parise, O.; Sani, G.; Prifti, E.; Gelsomino, S. Outcomes’ predictors in Post-Cardiac Surgery Extracorporeal Life Support. An observational prospective cohort study. Int. J. Surg. 2020, 82, 56–63. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Publication Year | Sample Size (CPR/eCPR) | Location | Study Design | ECMO Cannulation Location a | Primary Outcome | Secondary Outcome(s) | Study Quality Rating |
|---|---|---|---|---|---|---|---|---|
| Bougouin et al. [21] | 2020 | 12,666/525 | France | Retrospective, Obs | - | Survival to hospital discharge | CPC 1 or 2 at hospital discharge | 8 |
| Choi et al. [22] | 2016 | 50/10 | Korea | Retrospective, Obs | - | CPC 1 or 2 at 1 month | Survival at 1 month | 7 |
| Choi et al. [23] | 2016 | 320/320 | Korea | Retrospective, Obs | - | CPC 1 or 2 at hospital discharge | Survival to hospital discharge | 8 |
| Kim et al. [24] | 2014 | 52/52 | Korea | Retrospective, Obs | ED, Cath Lab | CPC 1 or 2 at 3 months | Survival at 24 h, hospital discharge, and 3 months | 8 |
| Kitada et al. [25] | 2020 | 2278/307 | Japan | Retrospective, Obs | - | CPC 1 or 2 at 1 month | None | 9 |
| Maekawa et al. [26] | 2013 | 24/24 | Japan | Retrospective, Obs | - | CPC 1 or 2 at 3 months | None | 9 |
| Nakashima et al. [27] | 2019 | 157/250 | Japan | Retrospective, Obs | - | CPC 1 or 2 at 6 months | Survival at 6 months | 9 |
| Patricio et al. [28] | 2019 | 50/49 | Belgium | Retrospective, Obs | - | CPC 1 or 2 at 3 months; survival to ICU discharge * | None | 8 |
| Sakamoto et al. [20] | 2014 | 194/260 | Japan | Prospective, Obs | - | CPC 1 or 2 at 1 and 6 months | None | 7 |
| Schober et al. [29] | 2017 | 232/7 | Austria | Retrospective | ED | CPC 1 or 2 at 6 months | None | 8 |
| Yannopoulos et al. [19] | 2017 | 170/62 | USA | Prospective | Cath Lab | CPC 1 or 2 at discharge | CPC 1 or 2 at 3 months | 7 |
| Yannopoulos et al. [7] | 2020 | 15/15 | USA | RCT | Cath Lab | Survival to hospital discharge | Survival at 1, 3, and 6 months; CPC 1 or 2 at hospital discharge, 1, 3, 6 months | Low risk |
| Yoshida et al. [30] | 2020 | 493/38 | Japan | Retrospective | - | CPC 1 or 2 at 1, 3 months | Survival at 1, 3 months | 7 |
| Past Medical History | Arrest Etiology | Arrest Characteristics | Additional Treatments a | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Age b,c | Male N (%) | DM N (%) | HTN N (%) | HLD N (%) | CAD N (%) | ACS N (%) | PE N (%) | Arrhythmia N (%) | VT/VF N (%) | Witnessed N (%) | Bystander CPR N (%) | Time to Hospital (min) b | Low-Flow Time (min) d | ROSC N (%) | TTM N (%) | CABG, PCI N (%) |
| Bougouin et al. [21] | |||||||||||||||||
| CPR | 66 (16) | 8486 (67) | - | - | - | - | 196 (37) | 18 (3) | - | 3167 (25) | 9500 (75) | 6206 (49) | - | - | 4789 (38) | - | 966 (20) |
| ECPR | 50 (13) | 441 (84) | - | - | - | - | 194 (37) | 16 (3) | - | 357 (68) | 509 (97) | 425 (81) | - | - | - | - | 159 (54) |
| Choi et al. [22] | |||||||||||||||||
| CPR | 59 (12) | 38 (76) | - | - | - | - | - | - | - | 13 (26) | 50 (100) | 41 (82) | 19 (8) | - | 15 (30) | 10 (67) | 2 (13) |
| ECPR | 58 (6) | 7 (70) | - | - | - | - | - | - | - | 3 (30) | 10 (100) | 8 (80) | 14 (10) | - | - | 6 (60) | 5 (56) |
| Choi et al. [23] | |||||||||||||||||
| CPR e | 58 (6) | 259 (81) | - | - | - | - | - | - | - | 90 (28) | 234 (73) | 74 (32) | 19 (-) | 47 (-) | - | 34 (11) | - |
| ECPR | 56 (7) | 258 (81) | - | - | - | - | - | - | - | 93 (29) | 227 (71) | 96 (30) | 19 (-) | 54 (-) | - | 95 (30) | - |
| Kim et al. [24] | |||||||||||||||||
| CPR e | 55 (8) | 38 (73) | 6 (12) | 12 (23) | - | 11 (21) | 9 (17) | 1 (2) | 5 (10) | 29 (56) | 42 (81) | 16 (31) | - | 68 (-) | 20 (40) | 12 (60) | 3 (15) |
| ECPR | 53 (8) | 40 (77) | 11 (21) | 13 (25) | - | 15 (29) | 36 (69) | 2 (4) | 3 (6) | 31 (60) | 42 (81) | 22 (42) | - | 70 (-) | - | 14 (27) | 29 (56) |
| Kitada et al. [25] | |||||||||||||||||
| CPR | 76 (5) | 1457 (64) | - | - | - | - | - | - | - | - | - | 1002 (44) | - | - | - | - | - |
| ECPR | 60 (6) | 257 (84) | - | - | - | - | - | - | - | 215 (70) | - | 157 (51) | - | - | - | - | - |
| Maekawa et al. [26] | |||||||||||||||||
| CPR e | 58 (5) | 19 (79) | - | - | - | - | - | - | - | 14 (58) | 24 (100) | 14 (58) | 28 (3) | 52 (-) | - | - | - |
| ECPR | 56 (4) | 19 (79) | - | - | - | - | - | - | - | 13 (54) | 24 (100) | 13 (54) | 31(3) | 51 (-) | - | 9 (38) | 5 (21) |
| Nakashima et al. [27] | |||||||||||||||||
| CPR | 60 (5) | 139 (89) | - | - | - | - | 82 (52) | - | - | 157 (100) | 123 (78) | 68 (43) | 32 (4) | - | 48 (31) | 22 (46) | 16 (37) |
| ECPR | 58 (5) | 227 (91) | - | - | - | - | 163 (65) | - | - | 250 (100) | 183 (73) | 115 (46) | 32 (4) | 55 (5) | - | - | - |
| Patricio et al. [28] | |||||||||||||||||
| CPR | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 26 (52) | - | - |
| ECPR | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Sakamoto et al. [20] | |||||||||||||||||
| CPR | 58 (NR) | 172 (89) | - | - | - | - | 114 (59) | - | 27 (14) | 194 (100) | 151 (78) | 90 (46) | 31 (-) | - | - | - | - |
| ECPR | 56 (NR) | 235 (90) | - | - | - | - | 165 (64) | - | 42 (16) | 260 (100) | 186 (72) | 127 (49) | 30 (-) | - | - | 162 (63) | 97 (37) |
| Schober et al. [29] | |||||||||||||||||
| CPR | 60 (6) | 173 (75) | 44 (19) | 67 (29) | - | 65 (28) | - | - | - | 135 (58) | 204 (88) | 72 (31) | 56 (9) | 78 (-) | 89 (38) | 48 (55) | 11 (12) |
| ECPR | 46 (8) | 5 (71) | 0 (0) | 2 (28) | - | 1 (14) | - | - | - | 4 (57) | 6 (86) | 2 (28) | 42 (11) | 93 (-) | - | 3 (43) | 2 (28) |
| Yannopoulos et al. 2017 [19] | |||||||||||||||||
| CPR | 56 (7) | 124 (73) | 37 (22) | 63 (37) | 54 (32) | 24 (14) | - | - | - | 170 (100) | 131 (77) | 128 (75) | - | - | - | - | - |
| ECPR | 58 (10) | 44 (71) | 12 (19) | 30 (48) | 22 (36) | 6 (9) | - | - | - | 62 (100) | 50 (80) | 52 (84) | - | - | - | - | 46 (74) |
| Yannopoulos et al. 2020 [7] | |||||||||||||||||
| CPR | 58 (11) | 11 (73) | 3 (20) | 5 (33) | 2 (13) | 4 (27) | - | - | - | 15 (100) | 13 (87) | 12 (80) | 50 (-) | - | 2 (13) | 2 (100) | 2 (100) |
| ECPR | 59 (10) | 14 (93) | 3 (20) | 2 (13) | 1 (7) | 2 (13) | - | - | - | 15 (100) | 11 (73) | 13 (87) | 48 (-) | 59 (-) | - | 15 (100) | - |
| Yoshida et al. [30] | |||||||||||||||||
| CPR | 72 (16) | 307 (62) | - | - | - | - | 20 (4) | 10 (2) | - | 0 (0) | - | - | 16 (4) | - | - | - | - |
| ECPR | 61 (16) | 27 (71) | - | - | - | - | 8 (21) | 10 (26) | - | 0 (0) | - | - | 11 (5) | 39 (6) | - | - | - |
| Moderator Variables | Number of Studies | Odds Ratio (95% CI) | p-Value | Q-Value | D(f) | p-Value | I² | Between-Group Comparison p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| WHO region | AMR | 2 | 4.3 (2.3–8.1) | 0.001 | 0.63 | 1 | 0.43 | 0% | 0.001 |
| EURO | 3 | 0.99 (0.74–1.3) | 0.97 | 2 | 2 | 0.37 | 0% | ||
| WPR | 8 | 3.5 (1.2–9.9) | 0.02 | 67 | 7 | 0.001 | 90% | ||
| Sample size of ECPR group | <50 patients | 5 | 7.5 (3.6–15) | 0.001 | 2 | 4 | 0.81 | 0% | 0.014 |
| 51–100 patients | 3 | 3.1 (1.4–6.9) | 0.005 | 3 | 2 | 0.18 | 43% | ||
| >100 patients | 5 | 1.5 (0.7–3.3) | 0.34 | 41 | 4 | 0.001 | 90% | ||
| Categories of patient analysis | Matched | 4 | 2.0 (1.1–3.6) | 0.019 | 3.6 | 3 | 0.3 | 18% | 0.36 |
| Unmatched | 8 | 2.7 (1.1–6.6) | 0.24 | 77 | 7 | 0.001 | 91% | ||
| Randomized | 1 | 10.5 (1.06–100+) | 0.044 | NA | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfalasi, R.; Downing, J.; Cardona, S.; Lowie, B.-J.; Fairchild, M.; Chan, C.; Powell, E.; Pourmand, A.; Grazioli, A.; Tran, Q.K. A Comparison between Conventional and Extracorporeal Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 591. https://doi.org/10.3390/healthcare10030591
Alfalasi R, Downing J, Cardona S, Lowie B-J, Fairchild M, Chan C, Powell E, Pourmand A, Grazioli A, Tran QK. A Comparison between Conventional and Extracorporeal Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(3):591. https://doi.org/10.3390/healthcare10030591
Chicago/Turabian StyleAlfalasi, Reem, Jessica Downing, Stephanie Cardona, Bobbi-Jo Lowie, Matthew Fairchild, Caleb Chan, Elizabeth Powell, Ali Pourmand, Alison Grazioli, and Quincy K. Tran. 2022. "A Comparison between Conventional and Extracorporeal Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest: A Systematic Review and Meta-Analysis" Healthcare 10, no. 3: 591. https://doi.org/10.3390/healthcare10030591