
Global Health Governance and Health Equity in the Context of COVID-19: A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives and Research Questions
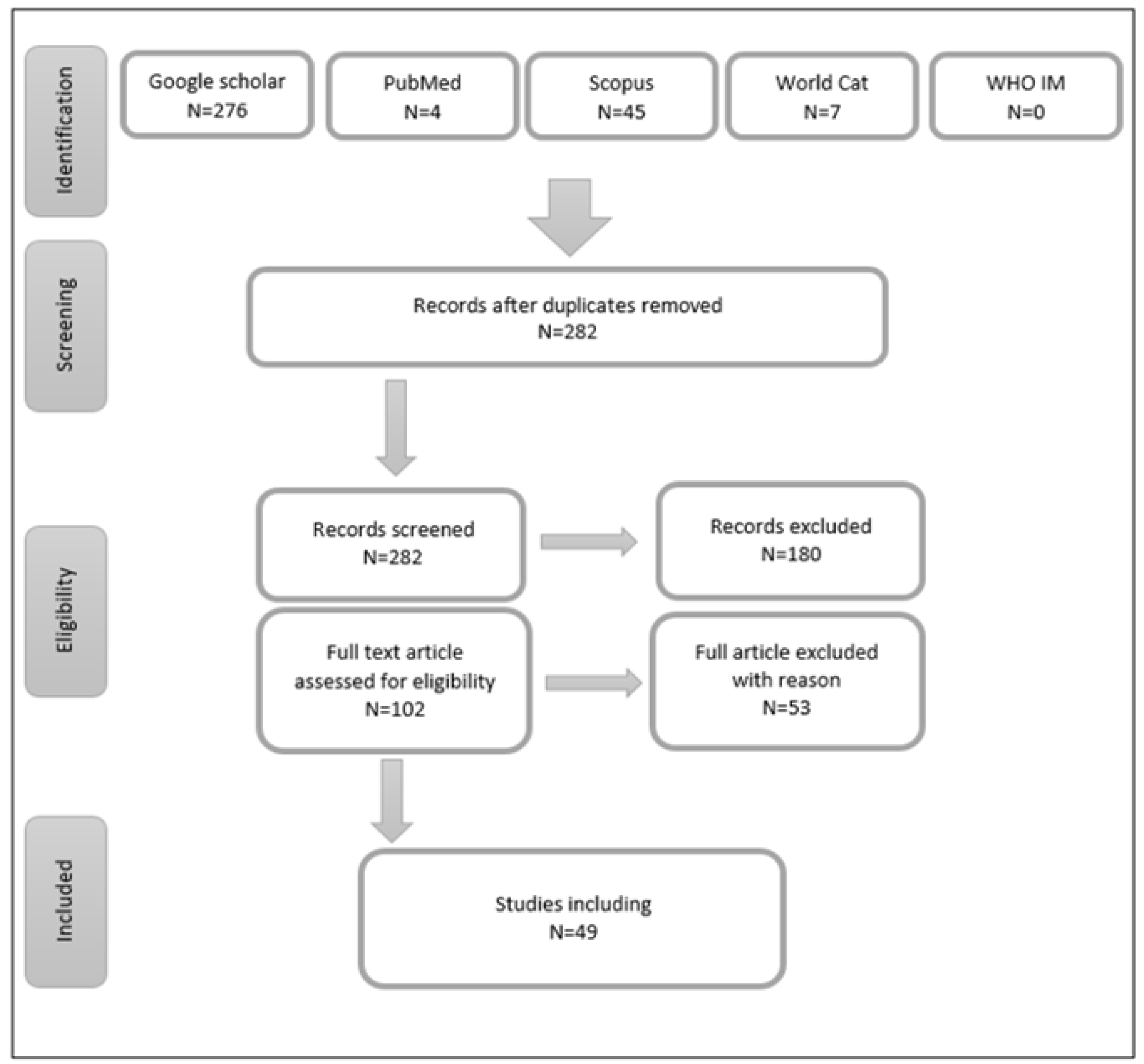
2.2. Relevant Studies Identification
2.3. Eligibility of Studies
- Written in English
- Published starting with the COVID-19 in 2019 up till October 2021
- The main focus is on global governance aspects that affect health equity
- Reports on health equity issue in the COVID-19 context
2.4. Charting of Data
2.5. Analysis and Results Reporting
3. Results
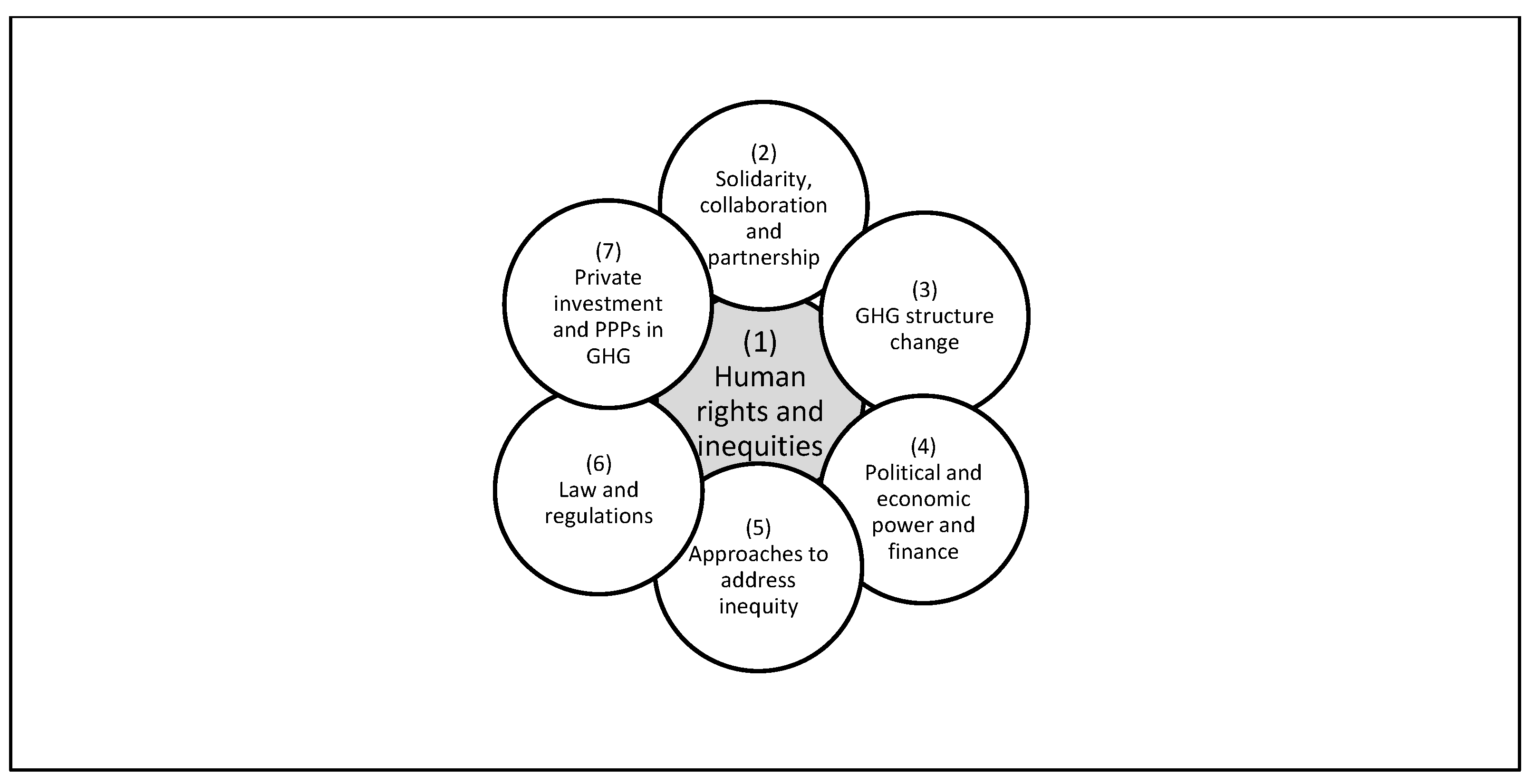
Identified Themes
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fidler, D.P. The Challenges of Global Health Governance; Council on Foreign Relations: New York, NY, USA, 2010; p. 3. [Google Scholar]
- Frenk, J.; Moon, S. Governance challenges in global health. N. Engl. J. Med. 2013, 368, 936–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyawo, O.; Viens, A.M. Rethinking the central role of equity in the global governance of pandemic response. J. Bioethical Inq. 2020, 17, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Chiriboga, D.; Garay, J.; Buss, P.; Madrigal, R.S.; Rispel, L.C. Health inequity during the COVID-19 pandemic: A cry for ethical global leadership. Lancet 2020, 395, 1690–1691. [Google Scholar] [CrossRef]
- Burström, B.; Tao, W. Social determinants of health and inequalities in COVID-19. Eur. J. Public Health 2020, 30, 617–618. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.; Abdool-Karim, Q.; Geng, E.; Goosby, E. How Will COVID-19 Transform Global Health Post-Pandemic? Defining Research and Investment Opportunities and Priorities; Public Library of Science: San Francisco, CA, USA, 2021. [Google Scholar]
- Gostin, L.O.; Moon, S.; Meier, B.M. Reimagining Global Health Governance in the Age of COVID-19; American Public Health Association: Washington, DC, USA, 2020. [Google Scholar]
- Singh, B.; Chattu, V.K. Prioritizing ‘equity’ in COVID-19 vaccine distribution through Global Health Diplomacy. Health Promot. Perspect. 2021, 11, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Kohler, J.C. The urgency of mutual collective accountability in Global Health Governance. Glob. Health Gov. 2021, 16, 38–41. [Google Scholar]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. JBI Evid. Implement 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Pūras, D.; de Mesquita, J.B.; Cabal, L.; Maleche, A.; Meier, B.M. The right to health must guide responses to COVID-19. Lancet 2020, 395, 1888–1890. [Google Scholar] [CrossRef]
- Jecker, N.S.; Wightman, A.G.; Diekema, D.S. Vaccine ethics: An ethical framework for global distribution of COVID-19 vaccines. J. Med. Ethics 2021, 47, 308–317. [Google Scholar] [CrossRef]
- Tandon, P. Ethical, public health, and economic dimensions of the inequitable global distribution of COVID-19 vaccines. Univ. Tor. Med. J. 2021, 98, 18–22. [Google Scholar]
- Lal, A.; Erondu, N.A.; Heymann, D.L.; Gitahi, G.; Yates, R. Fragmented health systems in COVID-19: Rectifying the misalignment between global health security and universal health coverage. Lancet 2021, 397, 61–67. [Google Scholar] [CrossRef]
- Beyrer, C.; Allotey, P.; Amon, J.J.; Baral, S.D.; Bassett, M.T.; Deacon, H.; Dean, L.T.; Fan, L.; Giacaman, R.; Gomes, C.; et al. Human rights and fair access to COVID-19 vaccines: The International AIDS Society–Lancet Commission on Health and Human Rights. Lancet 2021, 397, 1524–1527. [Google Scholar] [CrossRef]
- Osborne, R. In September 2020, the World Health Organization called for ‘equitable access to COVID-19 tools’ which included ‘the development, production and equitable access to COVID-19 tests, treatments and vaccines globally, while strengthening health systems’. What evidence is there of inequity of access so far in this pandemic? What is the role of national governments and of the WHO in this? Med. Confl. Surviv. 2021, 37, 187–196. [Google Scholar] [PubMed]
- Meier, B.M.; Cinà, M.M.; Gostin, L.O. Advancing human rights through Global Health Governance. In Foundations of Global Health and Human Rights; Gostin, L.O., Meier, B.M., Eds.; Oxford University Press: Oxford, UK, 2020; pp. 197–220. [Google Scholar]
- Wenham, C.; Davies, S.E. WHO runs the world–(not) girls: Gender neglect during global health emergencies. Int. Fem. J. Polit. 2021, 1–24. [Google Scholar] [CrossRef]
- Warsame, A.; Murray, J.; Gimma, A.; Checchi, F. The practice of evaluating epidemic response in humanitarian and low-income settings: A systematic review. BMC Med. 2020, 18, 315. [Google Scholar] [CrossRef] [PubMed]
- Storeng, K.T.; de Bengy Puyvallée, A.; Stein, F. COVAX and the rise of the ‘super public private partnership’ for global health. Glob. Public Health 2021, 1–17. [Google Scholar] [CrossRef]
- Storeng, K.T.; Fukuda-Parr, S.; Mahajan, M.; Venkatapuram, S. Digital Technology and the Political Determinants of Health Inequities: Special Issue Introduction. Glob. Policy 2021, 12, 5–11. [Google Scholar] [CrossRef]
- Paremoer, L.; Nandi, S.; Serag, H.; Baum, F. COVID-19 pandemic and the social determinants of health. BMJ 2021, 372, n129. [Google Scholar] [CrossRef]
- Patel, M.S.; Phillips, C.B. COVID-19 and the moral imagination. Lancet 2021, 397, 648–650. [Google Scholar] [CrossRef]
- Langran, I. Challenges to Global Health Governance from the International Trade in Organ Transplants: Time for a New Model? Glob. Gov. Rev. Multilater. Int. Organ. 2021, 27, 95–117. [Google Scholar] [CrossRef]
- Leung, J.Y.Y.; Yeung, S.L.A.; Lam, T.H.; Casswell, S. What lessons does the COVID-19 pandemic hold for global alcohol policy? BMJ Glob. Health 2021, 6, e006875. [Google Scholar] [CrossRef] [PubMed]
- Lou, L.; Wei, Y.; Wei, X. The construction and reconstruction of Global Health Governance system under public health emergencies. J. Glob. Policy Gov. 2020, 9, 97–116. [Google Scholar]
- D’Ambruoso, L.; Abbott, P.; Binagwaho, A. Building back fairer in public health policy requires collective action with and for the most vulnerable in society. BMJ Glob. Health 2021, 6, e005555. [Google Scholar] [CrossRef] [PubMed]
- Steven, D.; Williams, M. Governance and COVID-19: A background paper for the 2021 SDG 16 conference. Ment. Health Relig. Coping Am. Orthodox. Jews. J. Relig. Health 2020, 59, 2288–2301. [Google Scholar]
- Leidman, E.; Duca, L.M.; Omura, J.D.; Proia, K.; Stephens, J.W.; Sauber-Schatz, E.K. COVID-19 trends among persons aged 0–24 years—United States, March 1–December 12, 2020. Morb. Mortal Wkly Rep. 2021, 70, 88. [Google Scholar] [CrossRef]
- Shamasunder, S.; Holmes, S.M.; Goronga, T.; Carrasco, H.; Katz, E.; Frankfurter, R.; Keshavjee, S. COVID-19 reveals weak health systems by design: Why we must re-make global health in this historic moment. Glob. Public Health 2020, 15, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Tomson, G.; Causevic, S.; Ottersen, O.P.; Peterson, S.S.; Rashid, S.; Wanyenze, R.K.; Yamin, A.E. Solidarity and universal preparedness for health after COVID-19. BMJ 2021, 372, n59. [Google Scholar] [CrossRef] [PubMed]
- Olufadewa, I.; Adesina, M.; Ayorinde, T. Global health in low-income and middle-income countries: A framework for action. Lancet Glob. Health 2021, 9, e899–e900. [Google Scholar] [CrossRef]
- Persaud, A.; Bhugra, D.; Valsraj, K.; Bhavsar, V. Understanding geopolitical determinants of health. Bull. World Health Organ. 2021, 99, 166. [Google Scholar] [CrossRef] [PubMed]
- Van De Pas, R.; Widdowson, M.-A.; Ravinetto, R.; NS, P.; Ochoa, T.J.; Fofana, T.O.; Van Damme, W. COVID-19 vaccine equity: A health systems and policy perspective. SSRN 2021, 21, 25–36. [Google Scholar] [CrossRef]
- Chattu, V.K.; Aslanyan, G. Global Health Partnerships and Translation. Handbookof Global Health 2020, 1–33. [Google Scholar] [CrossRef]
- The Politics of Medicine: Power, Actors, and Ideas in the Making of Health. 2021. Available online: https://www.proquest.com/docview/2583438788?pq-origsite=gscholar&fromopenview=true (accessed on 6 December 2021).
- Baum, F.; Townsend, B.; Fisher, M.; Browne-Yung, K.; Freeman, T.; Ziersch, A.; Harris, P.; Friel, S. Creating political will for action on health equity: Practical lessons for public health policy actors. Int. J. Health Policy Manag. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kim, H. We need people’s WHO to solve vaccine inequity, and we need it now. BMJ Glob. Health 2021, 6, e006598. [Google Scholar] [CrossRef] [PubMed]
- Abed, Y.; Sahu, M.; Ormea, V.; Mans, L.; Lueddeke, G.; Laaser, U.; Hokama, T.; Goletic, R.; Eliakimu, E.; Dobe, M.; et al. Special Volume No. 1, 2021: The Global One Health Environment. South East Eur. J. Public Health SEEJPH 2021. [Google Scholar] [CrossRef]
- Plamondon, K.M. Equity at a time of pandemic. Health Promot. Int. 2021. [Google Scholar] [CrossRef]
- Ahen, F. From Ebola to COVID-19: What explains institutionalized manias and the ultimate preference for non-optimal solutions in Global Health Governance? Crit. Perspect Int. Bus. 2021. [Google Scholar] [CrossRef]
- Gupta, J.; Bavinck, M.; Ros-Tonen, M.; Asubonteng, K.; Bosch, H.; van Ewijk, E.; Hordijk, M.; van Leynseele, Y.; Cardozo, M.L.; Miedema, E.; et al. COVID-19, poverty and inclusive development. World Dev. 2021, 145, 105527. [Google Scholar] [CrossRef]
- Zwi, A.B. Development Trends and Assistance for Health. Glob Health Ethical Chall. 2020, 207. [Google Scholar]
- Kher, R.; Nair, A.S. The Case for a Global Healthcare Partnership. Available online: https://search.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/resource/en/covidwho-958819 (accessed on 5 December 2021).
- Ouimet, M.O.; Turcotte, P.L.; Rainville, L.C.; Abraham, Y.M.; Kaiser, D.; Badillo-Amberg, I. Public health and degrowth working synergistically: What leverage for public health. Vis. Sustain. 2021, 14, 99–116. [Google Scholar]
- Thoradeniya, T.; Jayasinghe, S. COVID-19 and future pandemics: A global systems approach and relevance to SDGs. Glob. Health 2021, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-L. Global health in a turbulence time: A commentary. Asian J. WTO Intl. Health Pol. 2020, 15, 27. [Google Scholar]
- Blinken, A.J.; Becerra, X. Strengthening Global Health Security and Reforming the International Health Regulations: Making the World Safer from Future Pandemics. JAMA 2021, 326, 1255–1256. [Google Scholar] [CrossRef] [PubMed]
- Gostin, L.O.; Karim, S.A.; Mason Meier, B. Facilitating access to a COVID-19 vaccine through global health law. J. Law Med. Ethics 2020, 48, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Gostin, L.O.; Monahan, J.T.; Kaldor, J.; DeBartolo, M.; Friedman, E.A.; Gottschalk, K.; Kim, S.C.; Alwan, A.; Binagwaho, A.; Burci, G.L.; et al. The legal determinants of health: Harnessing the power of law for global health and sustainable development. Lancet 2019, 393, 1857–1910. [Google Scholar] [CrossRef] [Green Version]
- Gostin, L.O.; Friedman, E.A. Imagining Global Health with Justice: Transformative Ideas for Health and Well-Being While Leaving No One Behind. Georget. Law J. 2019, 108, 1535. [Google Scholar]
- Rourke, M.; Eccleston-Turner, M.; Phelan, A.; Gostin, L. Policy opportunities to enhance sharing for pandemic research. Science 2020, 368, 716–718. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J.B.C.; Amor, Y.B.; Ergonul, O.; Figueroa, J.P.; Gilbert, S.; Gursel, M.; Hassanain, M.; Kang, G.; Kaslow, D.C.; Kim, J.H.; et al. Global public health security and justice for vaccines and therapeutics in the COVID-19 pandemic. EClinicalMedicine 2021, 39, 101053. [Google Scholar] [CrossRef] [PubMed]
- Meier, B.M.; Taylor, A.; Eccleston-Turner, M.; Habibi, R.; Sekalala, S.; Gostin, L.O. The World Health Organization in Global Health Law. J. Law Med. Ethics 2020, 48, 796–799. [Google Scholar] [CrossRef]
- Krikorian, G.; Torreele, E. We Cannot Win the Access to Medicines Struggle Using the Same Thinking That Causes the Chronic Access Crisis. Health Hum. Rights 2021, 23, 119. [Google Scholar]
- Dentico, N. The Breathing Catastrophe: COVID-19 and Global Health Governance. Development 2021, 64, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Stein, F. Risky business: COVAX and the financialization of global vaccine equity. Glob. Health 2021, 17, 112. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Characteristics N = 49 | Count (%) | ||||
|---|---|---|---|---|---|
| Year of publication | N | % | |||
| 2019 | 3 | 6.12% | |||
| 2020 | 14 | 28.57% | |||
| 2021 | 32 | 65.31% | |||
| Type of publication | |||||
| Journal article | Commentary | 8 | 42 | 85.71% | |
| Viewpoint | 1 | ||||
| Perspective | 1 | ||||
| Analytical | 22 | ||||
| Essay | 3 | ||||
| Review | 4 | ||||
| Systematic review | 1 | ||||
| Learning module | 1 | ||||
| Commission report | 1 | ||||
| Book chapter | 3 | 6.12% | |||
| Background paper | 1 | 2.04% | |||
| PhD Thesis | 1 | 2.04% | |||
| Discussion paper | 1 | 2.04% | |||
| Document | 1 | 2.04% | |||
| Discipline | |||||
| Medicine | 25 | ||||
| Bioethics and humanities | 1 | ||||
| Social sciences | 9 | ||||
| Development and policy | 1 | ||||
| Law and policy | 6 | ||||
| Communication | 1 | ||||
| Economics and political sciences | 2 | ||||
| Multidisciplinary | 4 | ||||
| Country | |||||
| Single country | 32 | 65.31% | |||
| UK | 4 | ||||
| USA | 9 | ||||
| Australia | 3 | ||||
| Taiwan | 1 | ||||
| Germany | 1 | ||||
| Italy | 1 | ||||
| Nigeria | 1 | ||||
| Canada | 5 | ||||
| Finland | 1 | ||||
| India | 1 | ||||
| China | 1 | ||||
| Netherlands | 1 | ||||
| Sri Lanka | 1 | ||||
| Norway | 2 | ||||
| Two or more countries | 13 | 26.53% | |||
| France, UK | 1 | ||||
| Norway, UK | 1 | ||||
| UK, US, Sweden | 1 | ||||
| Belgium, India, Guinea, Peru | 1 | ||||
| UK, Rwanda | 1 | ||||
| UK, USA, Lithuania, Kenya, Switzerland | 1 | ||||
| USA, Zimbabwe, Mexico, Belgium | 1 | ||||
| UK, USA, Kenya | 1 | ||||
| UK, Australia | 1 | ||||
| Australia, UK, USA | 1 | ||||
| Bangladesh, Sweden, Uganda, US | 1 | ||||
| New Zealand, Hong Kong | 1 | ||||
| US, South Africa, India, Australia | 1 | ||||
| Unidentified/commission/UN | 4 | 8.16% | |||
| Main Theme | N | % | ||
|---|---|---|---|---|
| 1 | Human rights and inequities | 11 | 22.49% | |
| Right to health and human rights | 3 | |||
| COVAX as a charitable PPP’s model to enhance equity | 1 | |||
| Digital technology role in enhancing equity, medical technology | 1 | |||
| Decolonizing GHG/right based approach | 1 | |||
| Inequity through different stages of vaccine | 1 | |||
| VALUES to consider in governing global vaccine distribution | 2 | |||
| Gender mainstreaming in IOs, in policy and response | 2 | |||
| 2 | Solidarity, collaboration, and partnership | 5 | 10.20% | |
| Solidarity through COVAX, technology transfer and voluntary license-sharing | 1 | |||
| Weak solidarity as a cause for inequity | 1 | |||
| GH partnership | 1 | |||
| Capacity bridging, collaboration, population-based health initiatives are needed to face inequity | 1 | |||
| Improving capacity in LMICs | 1 | |||
| 3 | GHG structure change | 9 | 18.37% | |
| Structural factors for health inequity | 1 | |||
| Many actors, no centralized authority, nor binding rules | 1 | |||
| Flexible governance, adequate financing, and evidence-based, collaborative | 1 | |||
| Justice and equity as the principle for GH practice | 1 | |||
| Unequal power relation/move some power to global south | 1 | |||
| Power, resources, and networks in GHG policy formulation | 1 | |||
| WHO—stronger independent structure to ensure equity | 2 | |||
| Inclusive multilateralism | 1 | |||
| 4 | Political and economic power and finance | 9 | 18.37% | |
| Political will and pro-equity policies | 2 | |||
| Centrality of power in GHG | 1 | |||
| Power and political economy/power as an access determinant to the vaccine | 4 | |||
| Quitting one-size-fits-all approach in equity, tends to prioritize the interests of HICs | 2 | |||
| 5 | Approaches to address inequity | 4 | 8.16% | |
| Multi-disciplinary effort is needed | 1 | |||
| Public health centrality in decision making | 1 | |||
| Global system approach | 1 | |||
| Mutual collective accountability | 1 | |||
| 6 | Law and regulations | 8 | 16.33% | |
| Health security and IHR to enhance equity | 1 | |||
| Role of law | 1 | |||
| Global intellectual property rules modification | 1 | |||
| Inequitable information sharing IS/international law for IS | 1 | |||
| Law capacity to advance GH justice | 1 | |||
| GH law reform | 3 | |||
| 7 | Private investment and PPPs in GHG | 3 | 6.12% | |
| Financial instrument for GHG—private investors renders GHG more secretive | 1 | |||
| Less PPP in GHG PPP causes inequity | 2 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kheir-Mataria, W.A.E.; El-Fawal, H.; Bhuiyan, S.; Chun, S. Global Health Governance and Health Equity in the Context of COVID-19: A Scoping Review. Healthcare 2022, 10, 540. https://doi.org/10.3390/healthcare10030540
Kheir-Mataria WAE, El-Fawal H, Bhuiyan S, Chun S. Global Health Governance and Health Equity in the Context of COVID-19: A Scoping Review. Healthcare. 2022; 10(3):540. https://doi.org/10.3390/healthcare10030540
Chicago/Turabian StyleKheir-Mataria, Wafa Abu El, Hassan El-Fawal, Shahjahan Bhuiyan, and Sungsoo Chun. 2022. "Global Health Governance and Health Equity in the Context of COVID-19: A Scoping Review" Healthcare 10, no. 3: 540. https://doi.org/10.3390/healthcare10030540