
Caring for Patients in Need of Palliative Care: Is This a Mission for Acute Care Hospitals? Key Questions for Healthcare Professionals


Abstract
:1. Introduction
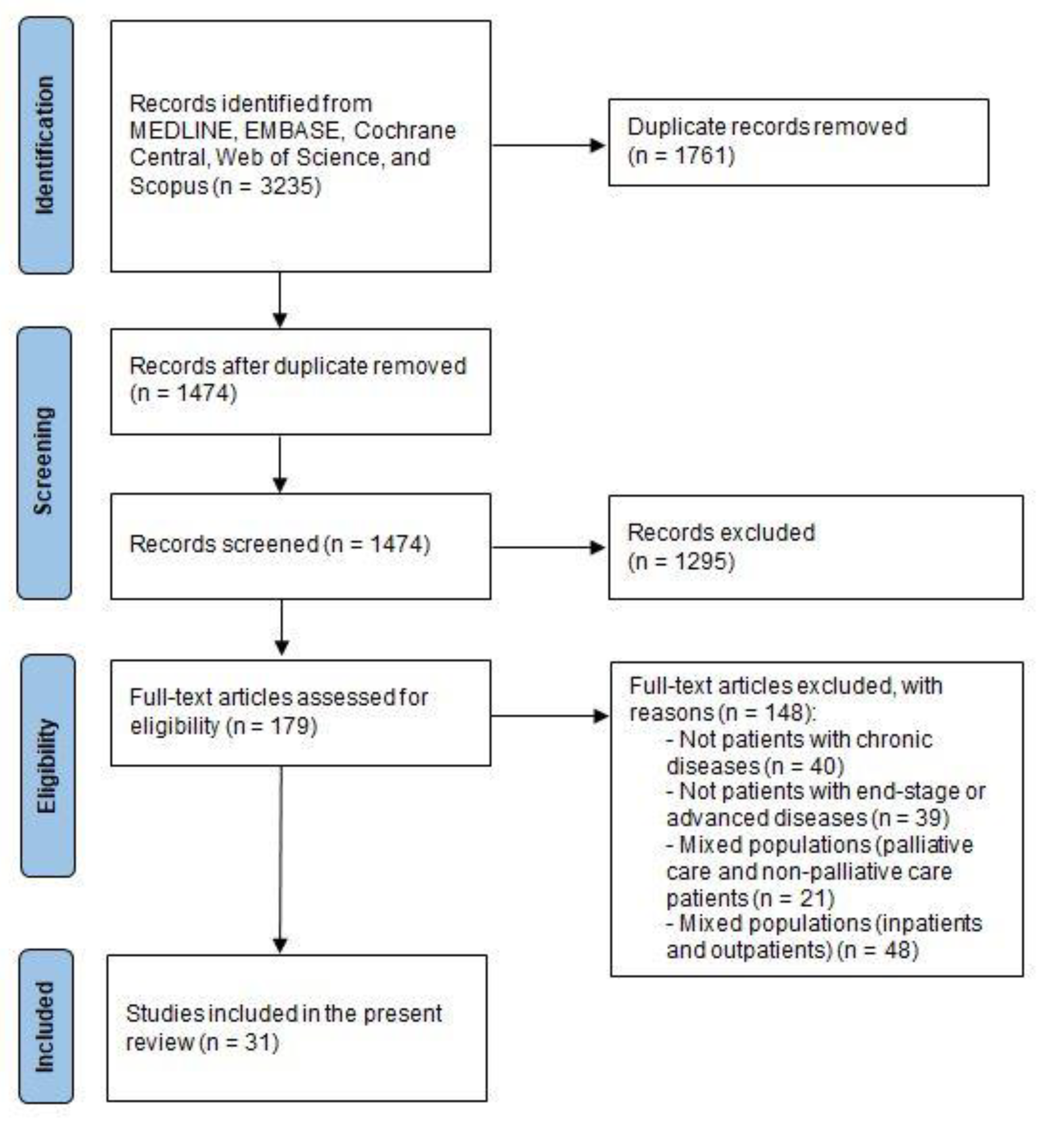
2. Methods
Search Strategy
3. Results
3.1. Who Are People with Serious Chronic Diseases?
3.1.1. Chronic Diseases
3.1.2. Chronic Disease-Focused Discussion
3.2. Why People with Serious Chronic Diseases Were Admitted in Acute Care Hospitals?
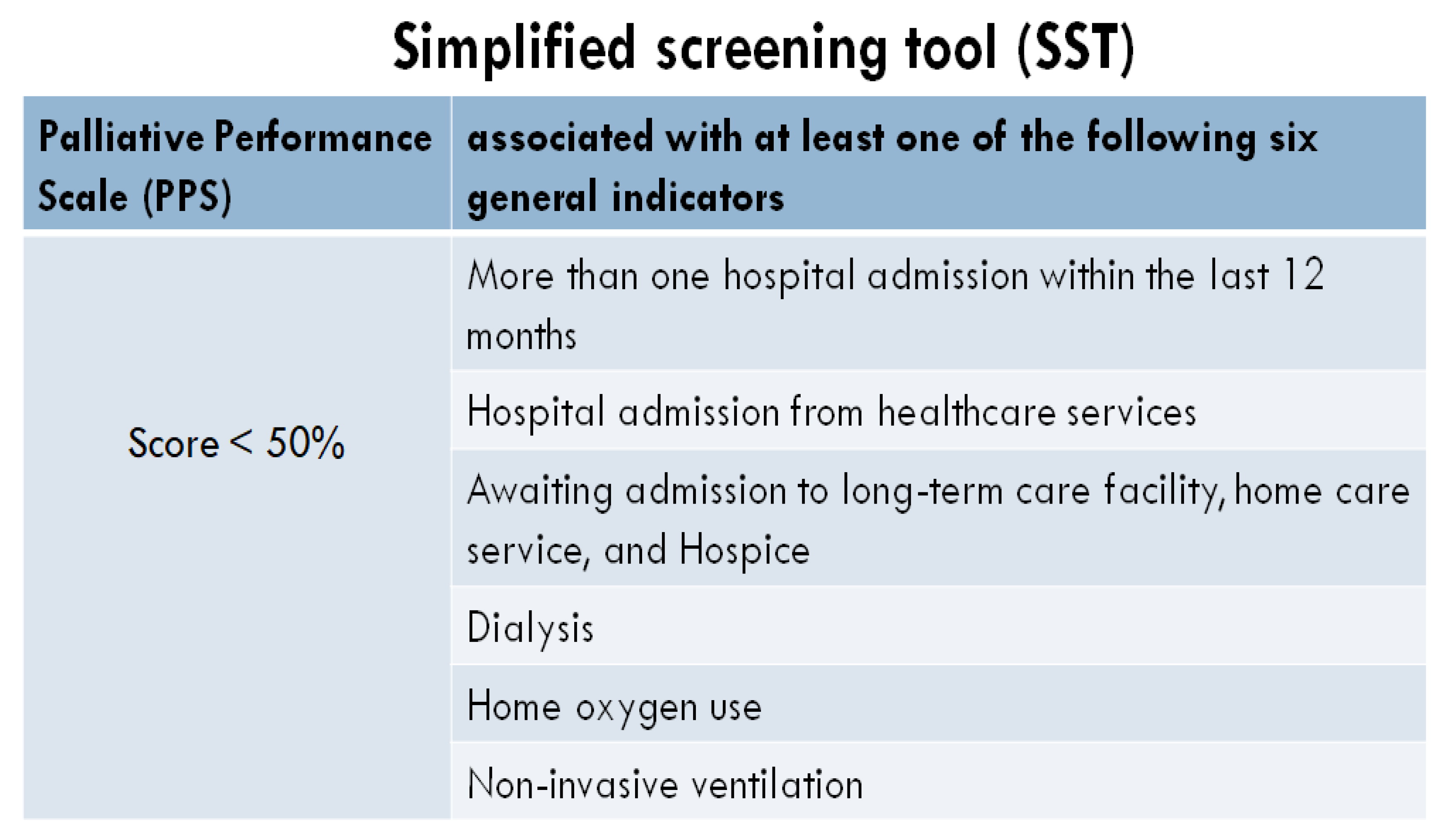
3.3. When People with Serious Chronic Diseases Should Be Considered Palliative Care Patients?
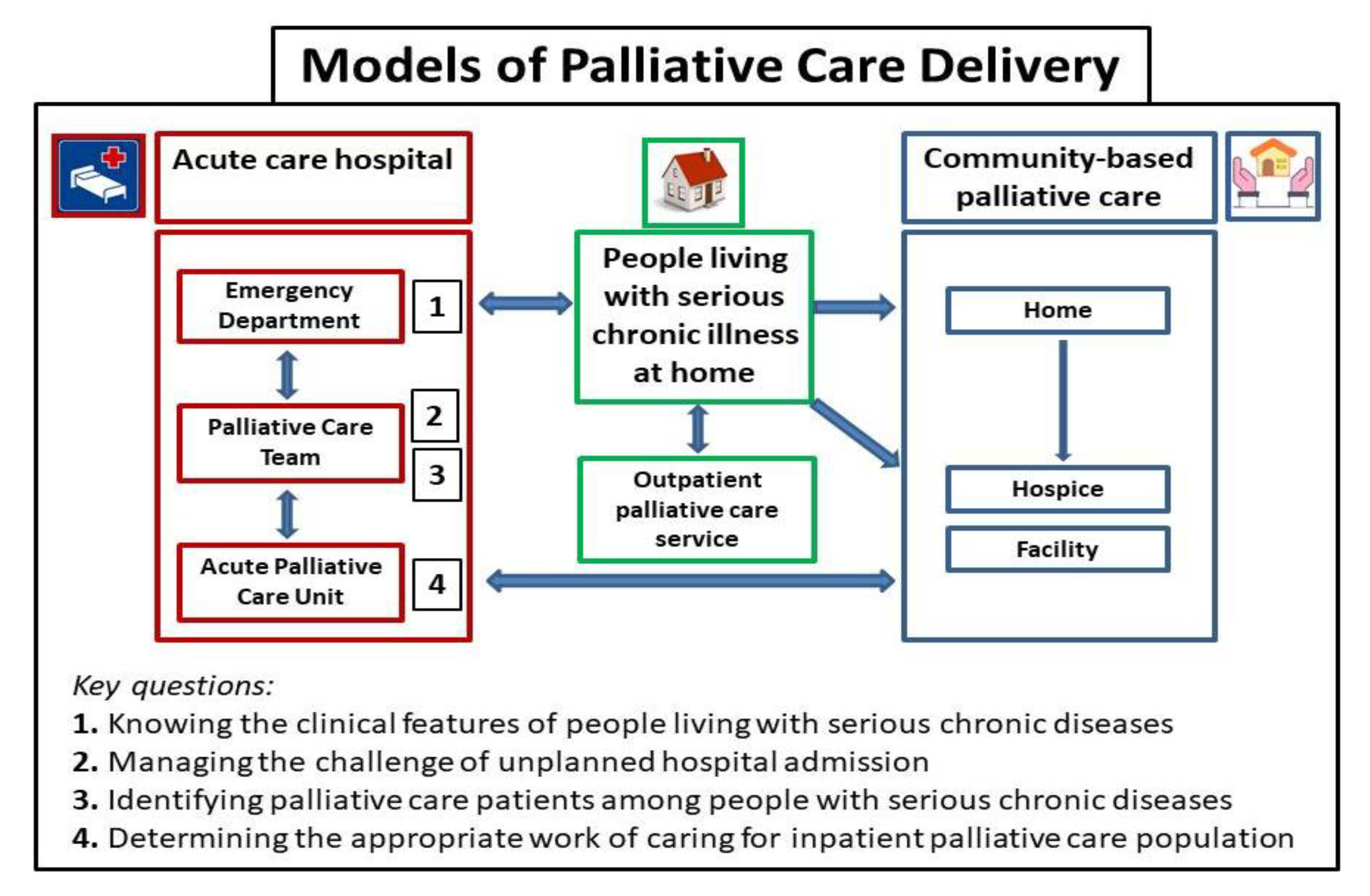
3.4. How Acute Care Hospital Should Plan the Work of Caring for This Palliative Care Population?
4. Limitations of the Study
5. Future Directions for Palliative Care Research
5.1. Research
5.2. Interventions
5.3. Education
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statements
Conflicts of Interest
References
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. World Report on Ageing and Health; World Health Organisation: Geneva, Switzerland, 2015; ISBN 978-92-4-156504-2. Available online: www.who.int (accessed on 5 November 2021).
- Goldsbury, D.E.; O’Connell, D.L.; Girgis, A.; Wilkinson, A.; Phillips, J.L.; Davidson, P.M.; Ingham, J.M. Acute hospital-based services used by adults during the last year of life in New South Wales, Australia: A population-based retrospective cohort study. BMC Health Serv. Res. 2015, 15, 537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, A.K.; McCarthy, E.; Weber, E.; Cenzer, I.S.; Boscardin, J.; Fisher, J.; Covinsky, K. Half of older Americans seen in emergency department in last month of life; most admitted to hospital, and many die there. Health Aff. 2012, 31, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Bekelman, J.E.; Halpern, S.D.; Blankart, C.R.; Bynum, J.P.; Cohen, J.; Fowler, R.; Kaasa, S.; Kwietniewski, L.; Melberg, H.O.; Onwuteaka-Philipsen, B.; et al. Comparison of Site of Death, Health Care Utilization, and Hospital Expenditures for Patients Dying with Cancer in 7 Developed Countries. JAMA 2016, 315, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Wallace, E.M.; Cooney, M.C.; Walsh, J.; Conroy, M.; Twomey, F. Why do palliative care patients present to the emergency department? Avoidable or unavoidable? Am. J. Hosp. Palliat. Care 2013, 30, 253–256. [Google Scholar] [CrossRef]
- Barbera, L.; Taylor, C.; Dudgeon, D. Why do patients with cancer visit the emergency department near the end of life? CMAJ 2010, 182, 563–568. [Google Scholar] [CrossRef] [Green Version]
- Higginson, I.J.; Addington-Hall, J.M. Palliative care needs to be provided on basis of needs rather than diagnosis. BMJ 1999, 318, 123. [Google Scholar] [CrossRef] [Green Version]
- Kelly, A.S.; Morrison, R.S. Palliative care for the seriously ill. N. Engl. J. Med. 2015, 373, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Solano, J.P.; Gomes, B.; Higginson, I.J. A comparison of symptom prevalence in far advanced cancer, AIDS, heart disease, chronic obstructive pulmonary disease and renal disease. J. Pain Symptom Manag. 2006, 31, 58–69. [Google Scholar] [CrossRef]
- Weissman, D.E.; Meier, D.E. Identifying patients in need of a palliative care assessment in the hospital setting: A consensus report from the Center to Advance Palliative Care. J. Palliat. Med. 2011, 14, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Prognostic Indicator Guidance (PIG). The National GSF Centre’s guidance for clinicians to support earlier recognition of patients nearing the end of life. In The Gold Standards Framework Centre In End of Life Care CIC, 6th ed.; Royal College of General Practioners: London, UK, December 2016; Available online: www.goldstandardsframework.org.uk (accessed on 5 November 2021).
- Società Italiana di Anestesia, Analgesia, Rianimazione e Terapia Intensiva (SIAARTI). Grandi Insufficienze D’Organo “End Stage”: Cure Intensive o Cure Palliative? ‘Documento Condiviso’ per una Pianificazione Delle Scelte di Cura. 2013. Available online: www.siaarti.it/News/grandi-insufficienze-organo-end-stage-cure-intensive-o-cure-palliative.aspx (accessed on 5 November 2021).
- Glare, P.A.; Chow, K. Validation of a simple screening tool for identifying unmet palliative care needs in patients with cancer. J. Oncol. Pract. 2015, 11, e81–e86. [Google Scholar] [CrossRef] [PubMed]
- Cotogni, P.; De Luca, A.; Evangelista, A.; Filippini, C.; Gili, R.; Scarmozzino, A.; Ciccone, G.; Brazzi, L. A simplified screening tool to identify seriously ill patients in the Emergency Department for referral to a palliative care team. Minerva Anestesiol 2017, 83, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Davidson, P.M.; Macdonald, P.S.; Newton, P.J. The use of hospital-based services by heart failure patients in the last year of life: A discussion paper. Heart Fail. Rev. 2019, 24, 199–207. [Google Scholar] [CrossRef]
- Gore, J.M.; Brophy, C.J.; Greenstone, M.A. How well do we care for patients with end stage chronic obstructive pulmonary disease (COPD)? A comparison of palliative care and quality of life in COPD and lung cancer. Thorax 2000, 55, 1000–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, D.H.; Udris, E.M.; Fihn, S.D.; McDonell, M.B.; Curtis, J.R. Differences in health care utilization at the end of life among patients with chronic obstructive pulmonary disease and patients with lung cancer. Arch. Intern. Med. 2006, 166, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.N.; Howard, E.P.; Steel, K.; Schreiber, R.; Fries, B.E.; Lipsitz, L.A.; Goldman, B. Predicting risk of hospital and emergency department use for home care elderly persons through a secondary analysis of cross-national data. BMC Health Serv. Res. 2014, 14, 519. [Google Scholar] [CrossRef] [Green Version]
- Lovasik, B.P.; Zhang, R.; Hockenberry, J.M.; Schrager, J.D.; Pastan, S.O.; Mohan, S.; Patzer, R.E. Emergency Department Use and Hospital Admissions Among Patients with End-Stage Renal Disease in the United States. JAMA Intern. Med. 2016, 176, 1563–1565. [Google Scholar] [CrossRef]
- Javaud, N.; Bonnin, L.; Lapostolle, F.; Boubaya, M.; Bardis, A.; Dufau, R.; Ghazali, A.; Reuter, P.G.; Pateron, D.; Adnet, F. Prognosis of cirrhotic patients admitted to Emergency Departments: A multicenter study. Am. J. Emerg. Med. 2019, 37, 1317–1321. [Google Scholar] [CrossRef]
- Harris, M.; Fry, M. The utilisation of one district hospital emergency department by people with Parkinson’s disease. Australas. Emerg. Nurs. J. 2017, 20, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.K.; Fisher, J.; Schonberg, M.A.; Pallin, D.J.; Block, S.D.; Forrow, L.; Phillips, R.S.; McCarthy, E.P. Am I doing the right thing? Provider perspectives on improving palliative care in the emergency department. Ann. Emerg. Med. 2009, 54, 86–93.e1. [Google Scholar] [CrossRef]
- Henson, L.A.; Higginson, I.J.; Gao, W.; Build Care. What factors influence emergency department visits by patients with cancer at the end of life? Analysis of a 124,030 patient cohort. Palliat. Med. 2018, 32, 426–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moens, K.; Higginson, I.J.; Harding, R.; Euro Impact. Are there differences in the prevalence of palliative care-related problems in people living with advanced cancer and eight non-cancer conditions? A systematic review. J. Pain Symptom Manag. 2014, 48, 660–677. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, S.C.; Wesker, W.; Kruitwagen, C.; de Haes, H.C.; Voest, E.E.; de Graeff, A. Symptom prevalence in patients with incurable cancer: A systematic review. J. Pain Symptom Manag. 2007, 34, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Bruera, E.; Kuehn, N.; Miller, M.J.; Selmser, P.; Macmillan, K. The Edmonton Symptom Assessment System (ESAS): A simple method for the assessment of palliative care patients. J. Palliat. Care 1991, 7, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Bruera, E. The Edmonton Symptom Assessment System 25 Years Later: Past, Present, and Future Developments. J. Pain Symptom Manag. 2017, 53, 630–643. [Google Scholar] [CrossRef] [Green Version]
- Modonesi, C.; Scarpi, E.; Maltoni, M.; Derni, S.; Fabbri, L.; Martini, F.; Sansoni, E.; Amadori, D. Impact of palliative care unit admission on symptom control evaluated by the Edmonton Symptom Assessment System. J. Pain Symptom Manag. 2005, 30, 367–373. [Google Scholar] [CrossRef]
- Murray, S.A.; Kendall, M.; Boyd, K.; Sheikh, A. Illness trajectories and palliative care. BMJ 2005, 330, 1007–1011. [Google Scholar] [CrossRef] [Green Version]
- Siegel, M.; Biegelow, S. Palliative care symptom management in the emergency department: The ABC’s of symptom management for the emergency physician. J. Emerg. Med. 2017, 54, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Batiste, X.; Martínez-Muñoz, M.; Blay, C.; Espinosa, J.; Contel, J.C.; Ledesma, A. Identifying needs and improving palliative care of chronically ill patients: A community-oriented, population-based, public-health approach. Curr. Opin. Support. Palliat. Care 2012, 6, 371–378. [Google Scholar] [CrossRef]
- Van Mechelen, W.; Aertgeerts, B.; De Ceulaer, K.; Thoonsen, B.; Vermandere, M.; Warmenhoven, F.; Van Rijswijk, E.; De Lepeleire, J. Defining the palliative care patient: A systematic review. Palliat. Med. 2013, 27, 197–208. [Google Scholar] [CrossRef]
- Lunney, J.R.; Lynn, J.; Foley, D.J.; Lipson, S.; Guralnik, J.M. Patterns of functional decline at the end of life. JAMA 2003, 289, 2387–2392. [Google Scholar] [CrossRef] [Green Version]
- Gardiner, C.; Ingleton, C.; Gott, M.; Ryan, T. Exploring the transition from curative care to palliative care: A systematic review of the literature. BMJ Support. Palliat. Care 2011, 1, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, C.; Gott, M.; Ingleton, C.; Seymour, J.; Cobb, M.; Noble, B.; Bennett, M.; Ryan, T. Extent of palliative care need in the acute hospital setting: A survey of two acute hospitals in the UK. Palliat. Med. 2013, 27, 76–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotogni, P.; De Luca, A.; Saini, A.; Brazzi, L. Unplanned hospital admissions of palliative care patients: A great challenge for internal and emergency medicine physicians. Intern. Emerg. Med. 2017, 12, 569–571. [Google Scholar] [CrossRef]
- Gott, M.; Gardiner, C.; Ingleton, C.; Cobb, M.; Noble, B.; Bennett, M.I.; Seymour, J. What is the extent of potentially avoidable admissions amongst hospital inpatients with palliative care needs? BMC Palliat. Care 2013, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, C.; Swami, N.; Krzyzanowska, M.; Hannon, B.; Leighl, N.; Oza, A.; Moore, M.; Rydall, A.; Rodin, G.; Tannock, I.; et al. Early palliative care for patients with advanced cancer: A cluster-randomised controlled trial. Lancet 2014, 383, 1721–1730. [Google Scholar] [CrossRef]
- Vanbutsele, G.; Pardon, K.; Van Belle, S.; Surmont, V.; De Laat, M.; Colman, R.; Eecloo, K.; Cocquyt, V.; Geboes, K.; Deliens, L. Effect of early and systematic integration of palliative care in patients with advanced cancer: A randomized controlled trial. Lancet Oncol. 2018, 19, 394–404. [Google Scholar] [CrossRef]
- Murray, S.A.; Kendall, M.; Mitchell, G.; Moine, S.; Amblàs-Novellas, J.; Boyd, K. Palliative care from diagnosis to death. BMJ Support. Palliat. Care 2017, 7, 122–127. [Google Scholar] [CrossRef]
- Gómez-Batiste, X.; Murray, S.A.; Thomas, K.; Blay, C.; Boyd, K.; Moine, S.; Gignon, M.; Van den Eynden, B.; Leysen, B.; Wens, J.; et al. Comprehensive and Integrated Palliative Care for People with Advanced Chronic Conditions: An Update From Several European Initiatives and Recommendations for Policy. J. Pain Symptom Manag. 2017, 53, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Gott, M.; Ingleton, C.; Bennett, M.I.; Gardiner, C. Transitions to palliative care in acute hospitals in England: Qualitative study. BMJ 2011, 342, 1773. [Google Scholar] [CrossRef] [Green Version]
- Fry, M.; Fitzpatrick, L.; Considine, J.; Shaban, R.Z.; Curtis, K. Emergency department utilisation among older people with acute and/or chronic conditions: A multi-centre retrospective study. Int. Emerg. Nurs. 2018, 37, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Lowery, D.S.; Quest, T.E. Emergency medicine and palliative care. Clin. Geriatr. Med. 2015, 31, 295–303. [Google Scholar] [CrossRef] [PubMed]
- DeVader, T.E.; Jeanmonod, R. The effect of education in hospice and palliative care on emergency medicine residents’ knowledge and referral patterns. J. Palliat. Med. 2012, 1, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Boyd, K.; Murray, S.A. Recognising and managing key transitions in end of life care. BMJ 2010, 341, c4863. [Google Scholar] [CrossRef] [PubMed]
- Kinzbrunner, B.M. Ethical dilemmas in hospice and palliative care. Support. Care Cancer 1995, 3, 28–36. [Google Scholar] [CrossRef]
- Manfredi, P.L.; Morrison, R.S.; Morris, J.; Goldhirsch, S.L.; Carter, J.M.; Meier, D.E. Palliative care consultations: How do they impact the care of hospitalized patients? J. Pain Symptom Manag. 2000, 20, 166–173. [Google Scholar] [CrossRef]
- Pan, C.X.; Morrison, R.S.; Meier, D.E.; Natale, D.K.; Goldhirsch, S.L.; Kralovec, P.; Cassel, C.K. How prevalent are hospital-based palliative care programs? Status report and future directions. J. Palliat. Med. 2001, 4, 315–324. [Google Scholar] [CrossRef]
- Ferrell, B.R.; Twaddle, M.L.; Melnick, A.; Meier, D.E. National Consensus Project Clinical Practice Guidelines for Quality Palliative Care Guidelines, 4th Edition. J. Palliat. Med. 2018, 21, 1684–1689. [Google Scholar] [CrossRef]
- Wu, F.M.; Newman, J.M.; Lasher, A.; Brody, A.A. Effects of initiating palliative care consultations in the emergency department on inpatient length of stay. J. Palliat. Med. 2013, 16, 1362–1367. [Google Scholar] [CrossRef]
- Grudzen, C.R.; Richardson, L.D.; Johnson, P.N.; Hu, M.; Wang, B.; Ortiz, J.M.; Kistler, E.A.; Chen, A.; Morrison, R.S. Emergency department-initiated palliative care in advanced cancer: A randomized clinical trial. JAMA Oncol. 2016, 2, 591–598. [Google Scholar] [CrossRef] [Green Version]
- George, N.; Phillips, E.; Zaurova, M.; Song, C.; Lamba, S.; Grudzen, C. Palliative Care Screening and Assessment in the Emergency Department: A Systematic Review. J. Pain Symptom Manag. 2016, 51, 108–119.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, N.; Bowman, J.; Aaronson, E.; Ouchi, K. Past, present, and future of palliative care in emergency medicine in the USA. Acute Med. Surg. 2020, 7, e497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haun, M.W.; Estel, S.; Rücker, G.; Friederich, H.C.; Villalobos, M.; Thomas, M.; Hartmann, M. Early palliative care for adults with advanced cancer. Cochrane Database Syst. Rev. 2017, 6, CD011129. [Google Scholar] [CrossRef] [PubMed]
- Dy, S.M.; Shugarman, L.R.; Lorenz, K.A.; Mularski, R.A.; Lynn, J. RAND-Southern California Evidence-Based Practice Center. A systematic review of satisfaction with care at the end of life. J. Am. Geriatr. Soc. 2008, 56, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Morrison, R.S. Health care system factors affecting end-of-life care. J. Palliat. Med. 2005, 8, S79–S87. [Google Scholar] [CrossRef] [PubMed]
- Back, A.L.; Li, Y.F.; Sales, A.E. Impact of palliative care case management on resource use by patients dying of cancer at a Veterans Affairs medical center. J. Palliat. Med. 2005, 8, 26–35. [Google Scholar] [CrossRef]
- Brumley, R.; Enguidanos, S.; Jamison, P.; Seitz, R.; Morgenstern, N.; Saito, S.; McIlwane, J.; Hillary, K.; Gonzalez, J. Increased satisfaction with care and lower costs: Results of a randomized trial of in-home palliative care. J. Am. Geriatr. Soc. 2007, 55, 993–1000. [Google Scholar] [CrossRef]
- Gade, G.; Venohr, I.; Conner, D.; McGrady, K.; Beane, J.; Richardson, R.H.; Williams, M.P.; Liberson, M.; Blum, M.; Della Penna, R. Impact of an inpatient palliative care team: A randomized control trial. J. Palliat. Med. 2008, 11, 180–190. [Google Scholar] [CrossRef]
- Klinedinst, R.; Kornfield, Z.N.; Hadler, R.A. Palliative Care for Patients with Advanced Heart Disease. J. Cardiothorac. Vasc. Anesth. 2019, 33, 833–843. [Google Scholar] [CrossRef]
- Hui, D.; Bruera, E. Models of Palliative Care Delivery for Patients with Cancer. J. Clin. Oncol. 2020, 38, 852–865. [Google Scholar] [CrossRef]
- Eti, S.; O’Mahony, S.; McHugh, M.; Guilbe, R.; Blank, A.; Selwyn, P. Outcomes of the acute palliative care unit in an academic medical centre. Am. J. Hosp. Palliat. Med. 2014, 31, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Hui, D.; Chisholm, G.B.; Kwon, J.H.; San Miguel, M.T.; Allo, J.A.; Yennurajalingam, S.; Frisbee-Hume, S.E.; Bruera, E. Characteristics and outcomes of patients admitted to an acute palliative care unit from the emergency centre. J. Pain Symptom Manag. 2014, 47, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Elsayem, A.; Palla, S.; De La Cruz, M.; Li, Z.; Yennurajalingam, S.; Bruera, E. Discharge outcomes and survival of patients with advanced cancer admitted to an acute palliative care unit at a comprehensive cancer centre. J. Palliat. Med. 2010, 13, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Cotogni, P.; De Luca, A.; Saini, A.; Brazzi, L. Trying to prolong life no matter what, or to dignify it till the end: The dilemma of modern medicine: Reply. Intern. Emerg. Med. 2018, 13, 627–628. [Google Scholar] [CrossRef] [PubMed]
- Hasson, F.; Nicholson, E.; Muldrew, D.; Bamidele, O.; Payne, S.; McIlfatrick, S. International palliative care research priorities: A systematic review. BMC Palliat. Care 2020, 19, 16. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Keyword | Question | Comments |
|---|---|---|
| Chronic diseases | Who are people with serious chronic diseases? |
|
| Unplanned hospital admission | Why people with serious chronic diseases were admitted in acute care hospitals? |
|
| Palliative care patient | When people with serious chronic diseases should be considered PC patients? |
|
| Hospital care | How acute care hospital should plan the work of caring for this PC population? |
|
| Heart failure | NYHA class IV ≥1 admission within the last 6 months Hypotension and/or fluid retention Dependency from intravenous medications Poor response to cardiac resynchronization therapy Cachexia | Dementia | Unable to walk without assistance, urinary and fecal incontinence, no consistently meaningful conversation Considerable assistance required Urinary tract infection, pressures sores (stage 3–4), recurrent fever Reduced oral intake, cachexia, aspiration pneumonia |
| Respiratory failure | >70 years Forced Expiratory Volume in the first sec <30% predicted Dyspnea scale grade of ≥3/Dependency from oxygen use ≥1 admission within the last 12 months Cachexia Considerable assistance required | Stroke | NIH Stroke Score ≥20 for left and ≥15 for right stroke Onset of headache + nausea/vomiting within 6 hCT scan showing a middle cerebral artery stroke ≥50% >75 years, history of ictus, fever, atrial fibrillation Conjugate deviation of the eyes Early reduced level of consciousness |
| Liver failure | Reduced oral intake, cachexia, aspiration pneumonia Deemed ineligible for transplantation Model for end-stage liver disease (MELD) score >25 Refractory ascites, spontaneous peritonitis, recurrent variceal bleeding, hepatorenal syndrome, hepatic encephalopathy | Parkinson’s disease | Decreasing response to treatments/medications Considerable assistance required Less controlled disease (increasing ‘off’ periods) Dyskinesias, mobility problems, falls Dysphagia (moderate/severe), psychiatric signs |
| Renal failure | >75 years Advanced cancer, heart or lung failure, vegetative state, dementia, cachexia | Amyotrophic lateral sclerosis | Patient/family requests for information/help about disease/symptoms Pain requiring high dosages of analgesics Need for a feeding tube Dyspnea or hypoventilation with vital capacity <50% Loss of function in at least two body regions Communication difficulties Weakness Cognitive difficulties Recurrent infections Dysphagia, cachexia, aspiration pneumonia |
| Cancer | Uncontrolled symptoms Moderate-to-severe cancer-related distress Metastatic solid tumors, central nervous system metastasis ECOG ≥3 or Karnofsky Performance Status <50 Persistent hypercalcemia, delirium, superior vena cava syndrome, spinal cord compression Cachexia Malignant effusions Palliative stenting or venting gastrostomy Patient/family concerns about disease/decision-making Patient/family requests for palliative care |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cotogni, P.; De Luca, A. Caring for Patients in Need of Palliative Care: Is This a Mission for Acute Care Hospitals? Key Questions for Healthcare Professionals. Healthcare 2022, 10, 486. https://doi.org/10.3390/healthcare10030486
Cotogni P, De Luca A. Caring for Patients in Need of Palliative Care: Is This a Mission for Acute Care Hospitals? Key Questions for Healthcare Professionals. Healthcare. 2022; 10(3):486. https://doi.org/10.3390/healthcare10030486
Chicago/Turabian StyleCotogni, Paolo, and Anna De Luca. 2022. "Caring for Patients in Need of Palliative Care: Is This a Mission for Acute Care Hospitals? Key Questions for Healthcare Professionals" Healthcare 10, no. 3: 486. https://doi.org/10.3390/healthcare10030486