
Measuring the Physical Activity of Seniors before and during COVID-19 Restrictions in the Czech Republic



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
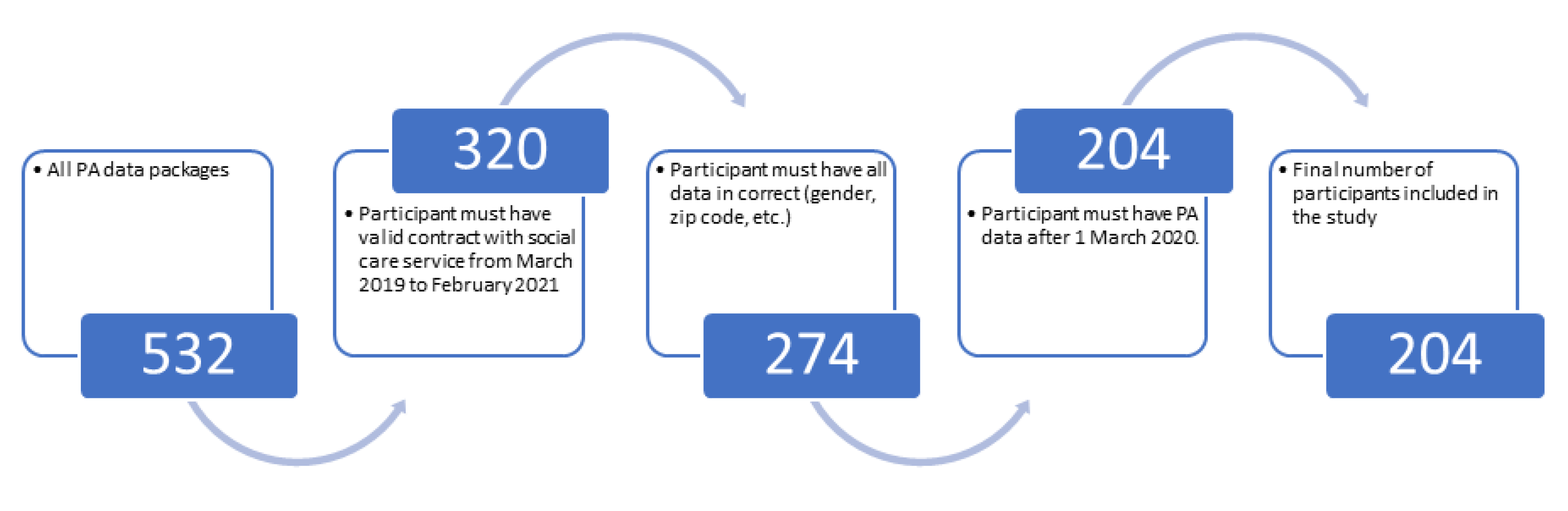
2.1.1. Data Filtering
2.1.2. Participant Statistics
2.2. Data Package
- The system has information about the battery; it knows when the device is put on the charger and when it is removed from it.
- The system monitors a “no motion alarm” in individual wear time (usually 7 am to 10 pm). If a device does not detect motion in a two-hour time window, then the caregiver will contact the user.
- The system monitors “long charging” in individual time (usually up to 8 am). If the battery device is over 98% and without motion, then the operator will contact the user.
- The system monitors “low battery” and “lost data”. Again, the caregiver will contact the user.
- There is regular training on the use of the equipment.
2.3. Statistical Analysis
2.4. Established Hypotheses
- Hypothesis 1 (H01). Participant PA in the pre-COVID period is the same as in the during-COVID period in general.
- Hypothesis 2 (H02). Male PA in the pre-COVID period is the same as in the during-COVID period in general.
- Hypothesis 3 (H03). Female PA in the pre-COVID period is the same as in the during-COVID period in general.
- Hypothesis 4 (H04). Participant physical activity in the pre-COVID period is the same as in the during-COVID period for every month.
- Hypothesis 5 (H05). The PA is the same for pre-COVID and during-COVID periods in a big city.
- Hypothesis 6 (H06). The PA of participants living in a small or big city is the same in the pre-COVID period.
- Hypothesis 7 (H07). The PA of participants living in a small or big city is the same in the during-COVID period.
- Hypothesis 8 (H08). For a participant living in a flat, is PA the same for a participant living in a house in the pre-COVID period.
- Hypothesis 9 (H09). For a participant living in a flat, is PA the same for a participant living in a house in the during-COVID period.
- Hypothesis 10 (H10). Physical activity in the pre-COVID and during-COVID periods is the same for a given age category.
- Hypothesis 11 (H11). BMI is correlated with average PA in the pre-COVID period.
- Hypothesis 12 (H12). BMI is correlated with average PA in the during-COVID period.
3. Results
3.1. Physical Activity in General
3.1.1. Physical Activity Evaluation
3.1.2. Physical Activity Calculation of the Rate of Decline
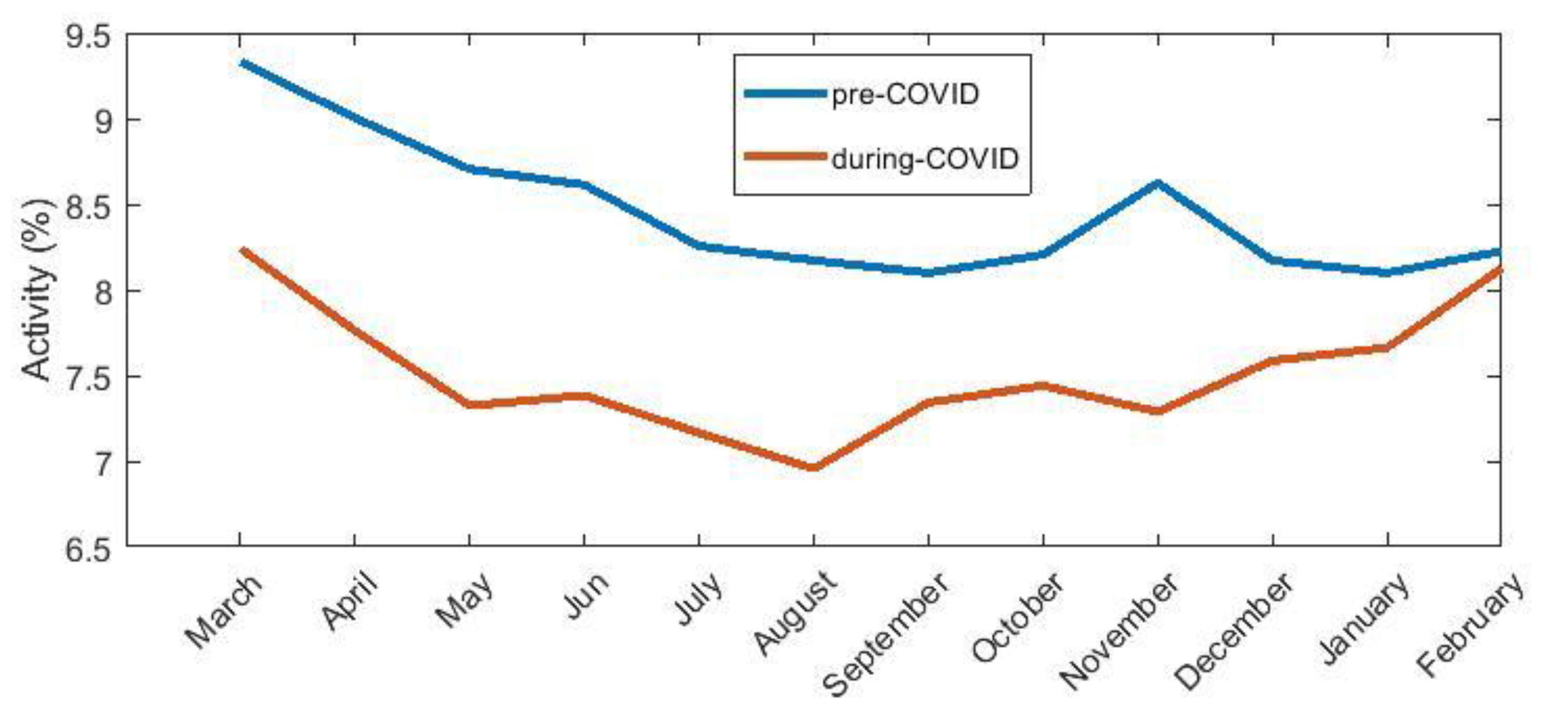
3.2. Physical Activity in Each Month
3.3. Physical Activity in Different City Size
3.4. Physical Activity in Different Households
3.5. Physical Activity in Different Age Groups
3.6. Correlation of BMI (Body Mass Index) with PAL
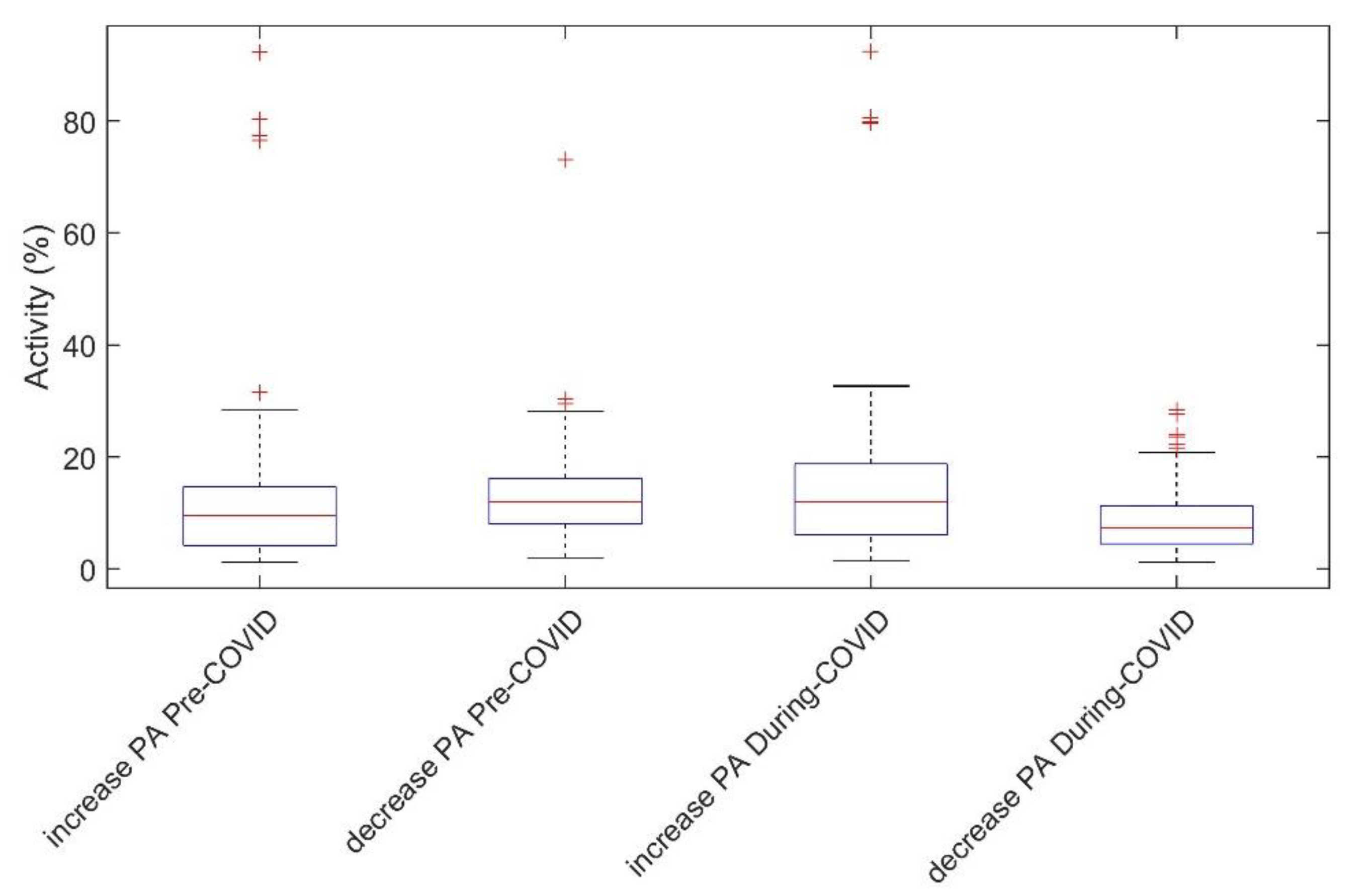
3.7. Variance of Physical Activity Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Physical Activity Package
- Client ID {number}
- Activity level in a 10-min window in the period 1 March 2019 to 29 February 2020 {number}
- Activity level in a 10-min window in the period 1 March 2020 to 28 February 2021 {number}
Appendix A.2. Client Information Package
- Client ID {number}
- Gender {text}
- Year of birth {number}
- Postcode of residence {number}
- Mobility Status {normal, low, with help, wheelchair}
- Housing Status {apartment, house}
- Height {number}
- Weight {number}
Appendix A.3. Number of Population in the Cities
- District code {number}
- City code {number}
- Name of municipality {text}
- Population total, males, females {number}
- Average age total, males, females {number}
Appendix A.4. ZIP Code List
- City name {text}
- ZIP code {number}
- Post name {text}
- District code {number}
- District name {text}
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Hypothesis | p-Value | p-Value for the First Group Normality Test | p-Value of the Second Group Normality Test | Test Type |
|---|---|---|---|---|
| H01 | 0.0000407 | 0.0558 (pre) | 0.4839 (during) | t-test |
| H02 | 0.0351 | 0.092 (pre) | 0.2268 (during) | t-test |
| H03 | 0.000279 | 0.0246 (pre) | 0.4113 (during) | Wilcox |
| H05 | 0.0003187 | 0.0029 (pre) | 0.1223 (during) | Wilcox |
| H06 | 0.9216 | 0.0029 (Big city) | 0.03804 (Small city) | Wilcox |
| H07 | 0.9981 | 0.1223 (Big city) | 0.3249 (Small city) | t-test |
| H08 | 0.5802 | 0.0218 (flat) | 0.132 (house) | Wilcox |
| H09 | 0.9982 | 0.008 (flat) | 0.5 (house) | Wilcox |
| H10 (<80) | 0.4713 | 0.3346 (pre) | 0.5 (during) | t-test |
| H10 (80–85) | 0.00137 | 0.0682 (pre) | 0.0178 (during) | Wilcox |
| H10 (86–90) | 0.0342 | 0.1599 (pre) | 0.5 (during) | t-test |
| H10 (>90) | 0.2342 | 0.0499 (pre) | 0.5 (during) | Wilcox |
| Month | p-Value | Normality Test Result Pre-COVID Group | Normality Test Result During-COVID Group | Test Type |
|---|---|---|---|---|
| January | 0.5143 | No | No | t-test |
| February | 0.8778 | No | No | t-test |
| March | 0.0272 | No | Yes | Wilcox |
| April | 0.000166 | No | No | Wilcox |
| May | 0.000221 | No | No | Wilcox |
| June | 0.0014 | No | No | t-test |
| July | 0.0124 | No | No | Wilcox |
| August | 0.0051 | No | No | Wilcox |
| September | 0.1718 | No | No | t-test |
| October | 0.0683 | No | No | Wilcox |
| November | 0.0011 | No | No | Wilcox |
| December | 0.4095 | No | No | Wilcox |
| Hypothesis | Mean | Std | Median | Interquartile | |||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-COVID | During-COVID | Pre-COVID | During-COVID | Pre-COVID | During-COVID | Pre-COVID | During-COVID | ||
| H01 | 8.8944 | 7.8846 | 12.0414 | 11.4569 | 6.3407 | 5.097 | 12.8576 | 11.3085 | |
| H02 | 9.5937 | 8.4228 | 5.5547 | 5.0809 | 9.4685 | 7.3391 | 6.9067 | 6.7901 | |
| H03 | 14.0388 | 12.4687 | 13.8464 | 13.5239 | 11.6287 | 9.5267 | 10.2819 | 10.1811 | |
| H05 | 11.4504 | 10.33 | 6.4578 | 6.8865 | 10.3775 | 8.7298 | 9.0502 | 8.0299 | |
| H06 + H07 | Big city | 11.4504 | 10.33 | 6.4578 | 6.8865 | 10.3775 | 8.7298 | 10.3775 | 8.0299 |
| Small city | 15.006 | 13.0793 | 17.2835 | 16.5888 | 11.0594 | 8.8027 | 11.1257 | 10.2064 | |
| H08 + H09 | Flat | 12.0011 | 10.5609 | 6.8931 | 7.1804 | 10.6546 | 8.6143 | 10.2723 | 9.6763 |
| House | 11.0172 | 9.6469 | 5.8998 | 5.3178 | 10.8687 | 9.9616 | 5.7273 | 7.0575 | |
| H10 (<80) | 12.21112 | 10.8139 | 16.7812 | 14.0844 | 8.4119 | 7.3049 | 7.9115 | 8.5652 | |
| H10 (80–85) | 11.9232 | 9.6699 | 6.8988 | 6.5215 | 11.0594 | 8.7298 | 9.3082 | 8.0688 | |
| H10 (86–90) | 15.1559 | 14.5726 | 15.2016 | 16.6061 | 12.7166 | 9.7711 | 8.6855 | 11.1537 | |
| H10 (>90) | 11.6059 | 10.2137 | 6.6508 | 7.5455 | 10.4028 | 8.3309 | 9.9492 | 9.4134 | |
| Hypothesis | R-Value |
|---|---|
| H11 | 0.004 |
| H12 | 0.121 |
References
- Puccinelli, P.; da Costa, T.; Seffrin, A.; de Lira, C.; Vancini, R.; Nikolaidis, P.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey: An internet-based survey. BMC Public Health 2021, 21, 425. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Breen, L.; Stokes, K.; Churchward-Venne, T.; Moore, D.; Baker, S.; Smith, K.; Atherton, P.; Phillips, S. Two Weeks of Reduced Activity Decreases Leg Lean Mass and Induces “Anabolic Resistance” of Myofibrillar Protein Synthesis in Healthy Elderly. J. Clin. Endocrinol. Metab. 2013, 98, 2604–2612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, A.; Kupelian, V.; Visser, M.; Simonsick, E.; Goodpaster, B.; Kritchevsky, S.; Tylavsky, F.; Rubin, S.; Harris, T. Strength, But Not Muscle Mass, Is Associated With Mortality in the Health, Aging and Body Composition Study Cohort. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Older Adults and COVID-19. In Proceedings of the CDC; U.S. Department of Health & Human Services: Washington, DC, USA, 2021.
- Suzuki, Y.; Maeda, N.; Hirado, D.; Shirakawa, T.; Urabe, Y. Physical Activity Changes and Its Risk Factors among Community-Dwelling Japanese Older Adults during the COVID-19 Epidemic: Associations with Subjective Well-Being and Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 6591. [Google Scholar] [CrossRef]
- Briguglio, M.; Giorgino, R.; Dell’Osso, B.; Cesari, M.; Porta, M.; Lattanzio, F.; Banfi, G.; Peretti, G. Consequences for the Elderly After COVID-19 Isolation: FEaR (Frail Elderly amid Restrictions). Front. Psychol. 2020, 11, 5. [Google Scholar] [CrossRef]
- Carriedo, A.; Cecchini, J.; Fernandez-Rio, J.; Méndez-Giménez, A. COVID-19, Psychological Well-being and Physical Activity Levels in Older Adults during the Nationwide Lockdown in Spain. Am. J. Geriatr. Psychiatry 2020, 28, 1146–1155. [Google Scholar] [CrossRef]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Sleep Quality and Physical Activity as Predictors of Mental Wellbeing Variance in Older Adults during COVID-19 Lockdown: ECLB COVID-19 International Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 4329. [Google Scholar] [CrossRef]
- Callow, D.; Arnold-Nedimala, N.; Jordan, L.; Pena, G.; Won, J.; Woodard, J.; Smith, J. The Mental Health Benefits of Physical Activity in Older Adults Survive the COVID-19 Pandemic. Am. J. Geriatr. Psychiatry 2020, 28, 1046–1057. [Google Scholar] [CrossRef]
- Richardson, D.; Duncan, M.; Clarke, N.; Myers, T.; Tallis, J. The influence of COVID-19 measures in the United Kingdom on physical activity levels, perceived physical function and mood in older adults: A survey-based observational study. J. Sports Sci. 2021, 39, 887–899. [Google Scholar] [CrossRef]
- Van Bakel, B.; Bakker, E.; de Vries, F.; Thijssen, D.; Eijsvogels, T. Impact of COVID-19 lockdown on physical activity and sedentary behaviour in Dutch cardiovascular disease patients. Neth. Heart J. 2021, 29, 273–279. [Google Scholar] [CrossRef]
- Pant, S.; Subedi, M. Impact of COVID-19 on the elderly. J. Patan Acad. Health Sci. 2020, 7, 32–38. [Google Scholar] [CrossRef]
- Linley, P.; Maltby, J.; Wood, A.; Osborne, G.; Hurling, R. Measuring happiness: The higher order factor structure of subjective and psychological well-being measures. Personal. Individ. Differ. 2009, 47, 878–884. [Google Scholar] [CrossRef]
- Roschel, H.; Artioli, G.; Gualano, B. Risk of Increased Physical Inactivity during COVID-19 Outbreak in Older People: A Call for Actions. J. Am. Geriatr. Soc. 2020, 68, 1126–1128. [Google Scholar] [CrossRef]
- WHO. Global Recommendations on Physical Activity for Health: Physical Activity for Health, 2nd ed.; World Health Organization: Geneva, Switzerland, 2010; ISBN 9789241599979. [Google Scholar]
- V01 Elders GPS Watch Tracker-Blue Idea Limited. Available online: http://www.blueideagps.com/index.php/EldergpswatchV01.html (accessed on 30 June 2021).
- Zákaznické výstupy—Česká Pošta. Available online: https://www.ceskaposta.cz/ke-stazeni/zakaznicke-vystupy#1 (accessed on 5 July 2021).
- Počet Obyvatel v Obcích. Available online: https://www.czso.cz/csu/czso/pocet-obyvatel-v-obcich-k-112021 (accessed on 5 July 2021).
- Buoite Stella, A.; Ajčević, M.; Furlanis, G.; Cillotto, T.; Menichelli, A.; Accardo, A.; Manganotti, P. Smart technology for physical activity and health assessment during COVID-19 lockdown. J. Sports Med. Phys. Fit. 2021, 61, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Sañudo, B.; Fennell, C.; Sánchez-Oliver, A. Objectively-Assessed Physical Activity, Sedentary Behavior, Smartphone Use, and Sleep Patterns Pre- and during-COVID-19 Quarantine in Young Adults from Spain. Sustainability 2020, 12, 5890. [Google Scholar] [CrossRef]
- Vetrovsky, T.; Frybova, T.; Gant, I.; Semerad, M.; Cimler, R.; Bunc, V.; Siranec, M.; Miklikova, M.; Vesely, J.; Griva, M.; et al. The detrimental effect of COVID-19 nationwide quarantine on accelerometer-assessed physical activity of heart failure patients. ESC Heart Fail. 2020, 7, 2093–2097. [Google Scholar] [CrossRef]
- Muriel, X.; Courel-Ibáñez, J.; Cerezuela-Espejo, V.; Pallarés, J. Training Load and Performance Impairments in Professional Cyclists during COVID-19 Lockdown. Int. J. Sports Physiol. Perform. 2021, 16, 735–738. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, H.; Potts, H.; Fisher, A. Physical Activity Behavior before, during, and after COVID-19 Restrictions: Longitudinal Smartphone-Tracking Study of Adults in the United Kingdom. J. Med. Internet Res. 2021, 23, 14. [Google Scholar] [CrossRef]
- Okely, J.; Corley, J.; Welstead, M.; Taylor, A.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.; Russ, T. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2021, 18, 210. [Google Scholar] [CrossRef]
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N.; et al. Relationships between changes in self-reported physical activity, sedentary behaviour and health during the coronavirus (COVID-19) pandemic in France and Switzerland. J. Sports Sci. 2021, 39, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Urzeala, C.; Duclos, M.; Chris Ugbolue, U.; Bota, A.; Berthon, M.; Kulik, K.; Thivel, D.; Bagheri, R.; Gu, Y.; Baker, J.; et al. COVID-19 lockdown consequences on body mass index and perceived fragility related to physical activity: A worldwide cohort study. Health Expect. 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- The Impact of Coronavirus on Global Activity. Available online: https://blog.fitbit.com/covid-19-global-activity/ (accessed on 26 July 2021).
- V Česku jsou tři lidé nakažení Koronavirem. Předtím byli v Itálii. In Proceedings of the ČT24; Česká televize: Praha, Czech, 2020.
- Vládní Usnesení Související s Bojem proti Epidemii Koronaviru. Available online: https://www.vlada.cz/cz/epidemie-koronaviru/dulezite-informace/vladni-usneseni-souvisejici-s-bojem-proti-epidemii-koronaviru---rok-2020-186999/ (accessed on 12 July 2021).
- Reilly, D.; McNeely, M.; Doerner, D.; Greenberg, D.; Staiger, T.; Geist, M.; Vedovatti, P.; Coffey, J.; Mora, M.; Johnson, T.; et al. Self-reported Exercise Tolerance and the Risk of Serious Perioperative Complications. Arch. Intern. Med. 1999, 159, 2185–2192. [Google Scholar] [CrossRef] [Green Version]
- Chapman, S.; Aslan, S.; Spence, J.; DeFina, L.; Keebler, M.; Didehbani, N.; Lu, H. Shorter term aerobic exercise improves brain, cognition, and cardiovascular fitness in aging. Front. Aging Neurosci. 2013, 5, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocca, A.; Brunese, M.; Cappuccio, M.; Scacchi, A.; Martucci, G.; Buondonno, A.; Perrotta, F.; Quarto, G.; Avella, P.; Amato, B. Impact of Physical Activity on Disability Risk in Elderly Patients Hospitalized for Mild Acute Diverticulitis and Diverticular Bleeding Undergone Conservative Management. Medicina 2021, 57, 360. [Google Scholar] [CrossRef]
- Aubertin-Leheudre, M.; Rolland, Y. The Importance of Physical Activity to Care for Frail Older Adults during the COVID-19 Pandemic. J. Am. Med. Dir. Assoc. 2020, 21, 973–976. [Google Scholar] [CrossRef]



| Group | Number | n (%) | |
|---|---|---|---|
| Gender | Male | 46 | 23 |
| Female | 158 | 77 | |
| Body | Weight ± SD | 79.54 ± 51.7 kg | |
| Height ± SD | 175.50 ± 8 cm | ||
| BMI ± SD | 25.80 ± 21.2 | ||
| Population | Weight in Big city ± SD | 81.10 ± 68.3 kg | |
| Weight in Small city ± SD | 72.33 ± 12.9 kg | ||
| Age in Big city ± SD | 84.26 ± 7.4 | ||
| Age in Small city ± SD | 84.31 ± 8.2 | ||
| Male | Weight ± SD | 79.54 ± 11.1 kg | |
| Height ± SD | 175.50 ± 6.4 cm | ||
| BMI ± SD | 25.80 ± 3.2 | ||
| Age ± SD | 84.80 ± 9.3 | ||
| Female | Weight ± SD | 76.50 ± 58.4 kg | |
| Height ± SD | 161.94 ± 5.5 cm | ||
| BMI ± SD | 29.23 ± 24 | ||
| Age ± SD | 84.22 ± 7.3 | ||
| Mobility | No problems | 55 | 27 |
| Small problems | 80 | 39 | |
| With help | 43 | 21 | |
| Wheelchair | 2 | 1 | |
| Not defined | 24 | 12 | |
| House | In house | 43 | 21 |
| In flat | 98 | 48 | |
| With family | 39 | 19 | |
| Not defined | 24 | 12 | |
| City size | Over than 100 k. (Big city) | 113 | 55 |
| Less than 100 k. (Small city) | 91 | 45 | |
| Age group | <80 | 44 | 22 |
| 80–85 | 49 | 24 | |
| 86–90 | 58 | 28 | |
| >90 | 53 | 26 | |
| Age | Average age | 84.55 | |
| Max age | 101 | ||
| Min age | 57 | ||
| Status | Number | (Percentage) | Age ± SD | PA Difference |
|---|---|---|---|---|
| PA has declined | 118 | 58% | 85.11 ± 7.37 | 5.49% |
| PA has increased | 86 | 42% | 83.98 ± 8.17 | 2.03% |
| Month | Pre-COVID | During-COVID | ||
|---|---|---|---|---|
| M | F | M | F | |
| April | 9.88 | 14.56 | 7.78 | 12.61 |
| May | 10.69 | 13.98 | 6.87 | 11.58 |
| Age Group (Years) | p-Value |
|---|---|
| <80 | 0.471 (α = 0.013) |
| 80–85 | 0.001 (α = 0.013) |
| 86–90 | 0.034 (α = 0.013) |
| >90 | 0.234 (α = 0.013) |
| Age Group (Years) | No Problems | Small Problems | With Help | Wheelchair | Not Defined |
|---|---|---|---|---|---|
| <80 | 18 | 12 | 6 | 1 | 7 |
| 80–85 | 15 | 38 | 9 | 1 | 2 |
| 86–90 | 13 | 20 | 13 | 0 | 11 |
| >90 | 9 | 10 | 15 | 0 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janovský, V.; Piorecký, M.; Včelák, J.; Mrissa, M. Measuring the Physical Activity of Seniors before and during COVID-19 Restrictions in the Czech Republic. Healthcare 2022, 10, 460. https://doi.org/10.3390/healthcare10030460
Janovský V, Piorecký M, Včelák J, Mrissa M. Measuring the Physical Activity of Seniors before and during COVID-19 Restrictions in the Czech Republic. Healthcare. 2022; 10(3):460. https://doi.org/10.3390/healthcare10030460
Chicago/Turabian StyleJanovský, Vít, Marek Piorecký, Jan Včelák, and Michael Mrissa. 2022. "Measuring the Physical Activity of Seniors before and during COVID-19 Restrictions in the Czech Republic" Healthcare 10, no. 3: 460. https://doi.org/10.3390/healthcare10030460