
Association between Frequency of Going Out and Psychological Condition among Community-Dwelling Older Adults after the COVID-19 Pandemic in Japan

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
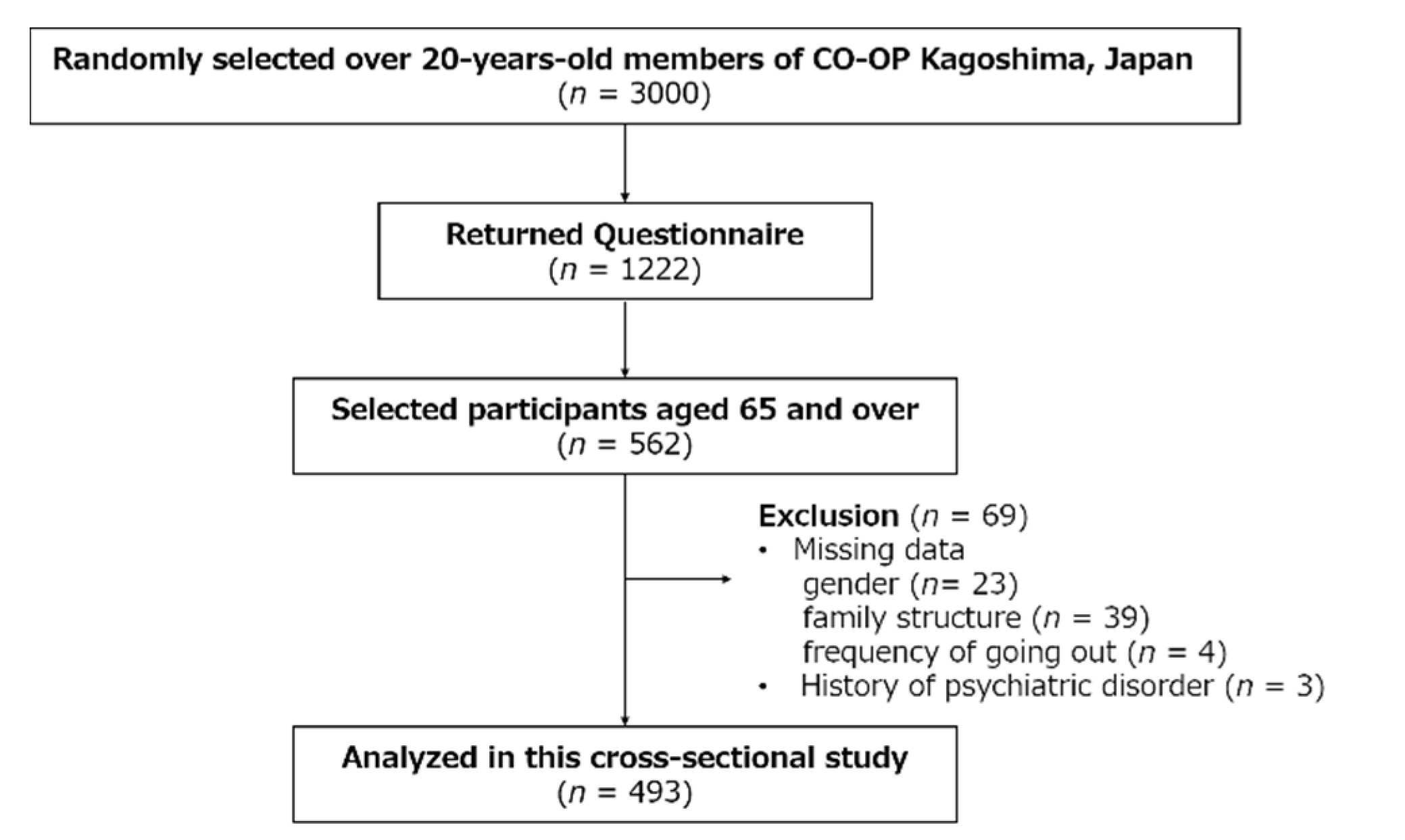
2.2. Participants
2.3. Measurements
2.3.1. Social Demographics and Baseline Characteristics
2.3.2. Changes in Frequency of Going Out
2.3.3. Psychological Condition Changes
2.4. Statistical Analysis
2.5. Ethical Consideration
2.6. Funding Sources
3. Results
3.1. Characteristics of the Participants and Summary of Questionnaire
3.2. Bivariate Statistics for Psychological Condition Changed since before the COVID-19 Pandemic
3.3. Association between FGO and Mental Condition Changed since before the COVID-19 Pandemic
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ren, L.-L.; Wang, Y.-M.; Wu, Z.-Q.; Xiang, Z.-C.; Guo, L.; Xu, T.; Jiang, Y.-Z.; Xiong, Y.; Li, Y.-J.; Li, X.-W.; et al. Identification of a novel coronavirus causing severe pneumonia in human: A descriptive study. Chin. Med. J. 2020, 133, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19, 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 16 May 2021).
- Prime Minister of Japan and His Cabinet. COVID-19 Declaration of a State of Emergency in Response to the Novel Coronavirus Disease (April 16) (Ongoing Topics). Available online: http://japan.kantei.go.jp/ongoingtopics/_00020.html (accessed on 16 May 2021).
- Saito, S.; Asai, Y.; Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Tsuzuki, S.; Ohmagari, N. First and second COVID-19 waves in Japan: A comparison of disease severity and characteristics. J. Infect. 2021, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-l.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Fisman, D.N.; Bogoch, I.; Lapointe-Shaw, L.; McCready, J.; Tuite, A.R. Risk Factors Associated with Mortality Among Residents with Coronavirus Disease 2019 (COVID-19) in Long-term Care Facilities in Ontario, Canada. JAMA Netw. Open 2020, 3, e2015957. [Google Scholar] [CrossRef]
- Ministry of Health. Labour and Welfare to the Citizens (COVID-19). Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00094.html (accessed on 16 May 2021).
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. Effect of the COVID-19 Epidemic on Physical Activity in Community-Dwelling Older Adults in Japan: A Cross-Sectional Online Survey. J. Nutr. Health Aging 2020, 24, 948–950. [Google Scholar] [CrossRef]
- Makizako, H.; Nakai, Y.; Shiratsuchi, D.; Akanuma, T.; Yokoyama, K.; Matsuzaki-Kihara, Y.; Yoshida, H. Perceived declining physical and cognitive fitness during the COVID-19 state of emergency among community-dwelling Japanese old-old adults. Geriatr. Gerontol. Int. 2021, 21, 364–369. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Skoog, I. COVID-19 and mental health among older people in Sweden. Int. Psychogeriatr. 2020, 32, 1173–1175. [Google Scholar] [CrossRef]
- Santini, Z.I.; Jose, P.E.; Cornwell, E.Y.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Meilstrup, C.; Madsen, K.R.; Koushede, V. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. Lancet Public Health 2020, 5, e62–e70. [Google Scholar] [CrossRef] [Green Version]
- Dura-Perez, E.; Goodman-Casanova, J.M.; Vega-Nuñez, A.; Guerrero-Pertiñez, G.; Varela-Moreno, E.; Garolera, M.; Quintana, M.; Cuesta-Vargas, A.; Barnestein-Fonseca, P.; Sánchez-Lafuente, C.G.; et al. Impact of the COVID-19 confinement on cognition and mental health and technology use among socially vulnerable older people: A retrospective cohort study. J. Med. Internet Res. 2021, 24, e30598. [Google Scholar] [CrossRef]
- McCarron, R.H.; Swann, P.; Artingstall, J.; Burn, A.-M.; Deakin, J.; Ellis, F.; Gandamaneni, P.K.; Griffith, J.; Ireland, A.; Leadbetter, J.; et al. Factors in Psychiatric Admissions: Before and During the COVID-19 Pandemic. Clin. Neuropsychiatry 2021, 18, 270–277. [Google Scholar] [CrossRef]
- Colucci, E.; Nadeau, S.; Higgins, J.; Kehayia, E.; Poldma, T.; Saj, A.; de Guise, E. COVID-19 lockdowns’ effects on the quality of life, perceived health and well-being of healthy elderly individuals: A longitudinal comparison of pre-lockdown and lockdown states of well-being. Arch. Gerontol. Geriatr. 2022, 99, 104606. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.-Q.; Li, L.; Zhong, B.-L. Prevalence of Insomnia Symptoms in Older Chinese Adults During the COVID-19 Pandemic: A Meta-Analysis. Front. Med. 2021, 8, 779914. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.S.; Bodner, E.V.; Allman, R.M. Measuring Life-Space Mobility in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2003, 51, 1610–1614. [Google Scholar] [CrossRef]
- Fujita, K.; Fujiwara, Y.; Kumagai, S.; Watanabe, S.; Yoshida, Y.; Motohashi, Y.; Shinkai, S. The frequency of going outdoors, and physical, psychological and social functioning among community-dwelling older adults. Nihon Koshu Eisei Zasshi 2004, 51, 168–180. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Oguma, Y.; Abe, Y.; Takayama, M.; Hara, A.; Urushihara, H.; Takebayashi, T. Behavioral changes and hygiene practices of older adults in Japan during the first wave of COVID-19 emergency. BMC Geriatr. 2021, 21, 137. [Google Scholar] [CrossRef]
- Zin, P.E.; Saw, Y.M.; Saw, T.N.; Cho, S.M.; Hlaing, S.S.; Noe, M.T.N.; Kariya, T.; Yamamoto, E.; Lwin, K.T.; Win, H.H.; et al. Assessment of quality of life among elderly in urban and peri-urban areas, Yangon Region, Myanmar. PLoS ONE 2020, 15, e0241211. [Google Scholar] [CrossRef]
- Park, K.-H.; Kim, A.-R.; Yang, M.-A.; Lim, S.-J.; Park, J.-H. Impact of the COVID-19 pandemic on the lifestyle, mental health, and quality of life of adults in South Korea. PLoS ONE 2021, 16, e0247970. [Google Scholar] [CrossRef]
- Ikeda, Y.; Ogawa, N.; Yoshiura, K.; Han, G.; Maruta, M.; Hotta, M.; Tabira, T. Instrumental Activities of Daily Living: The Processes Involved in and Performance of These Activities by Japanese Community-Dwelling Older Adults with Subjective Memory Complaints. Int. J. Environ. Res. Public Health 2019, 16, 2617. [Google Scholar] [CrossRef] [Green Version]
- Takatori, K.; Matsumoto, D.; Miyazaki, M.; Yamasaki, N.; Moon, J.-S. The difference between self-perceived and chronological age in the elderly may correlate with general health, personality and the practice of good health behavior: A cross-sectional study. Arch. Gerontol. Geriatr. 2019, 83, 13–19. [Google Scholar] [CrossRef]
- Motohashi, T.; Odaira, T.; Nakatsuji, Y.; Matsuura, K.; Mashiko, M.; Takata, A. Examining attitudes toward mutual support in daily life and their associated factors within a community-based integrated care system: Findings of the “Survey to Enrich the Lives of Miyamae Ward Residents”. Nihon Koshu Eisei Zasshi 2020, 67, 191–210. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Monma, T.; Takeda, F.; Noguchi, H.; Tamiya, N. Age and sex differences of risk factors of activity limitations in Japanese older adults. Geriatr. Gerontol. Int. 2016, 16, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D. Manual for the State-Trait Anxietry, Inventory. Consult. Psychol. 1970. Available online: http://www.med.uottawa.ca/courses/cmed6203/index_notes/stai.pdf (accessed on 16 May 2021).
- Yokoyama, K.; Araki, S.; Kawakami, N.; Tkakeshita, T. Production of the Japanese Edition of Profile of Mood States (POMS): Assessment of Reliability and Validity. Nihon Koshu Eisei Zasshi 1990, 37, 913–918. (In Japanese) [Google Scholar] [PubMed]
- Hashimoto, M.; Suzuki, M.; Hotta, M.; Nagase, A.; Yamamoto, Y.; Hirakawa, N.; Nagata, Y.; Satake, Y.; Suehiro, T.; Kanemoto, H.; et al. The Influence of the COVID-19 Outbreak on the Lifestyle of Older Patients with Dementia or Mild Cognitive Impairment Who Live Alone. Front. Psychiatry 2020, 11, 570580. [Google Scholar] [CrossRef] [PubMed]
- Hiroi, U. A Study on the Effect of Japanese-style lockdown on Self-restraint Request for COVID-19. J. City Plan. Inst. Jpn. 2020, 55, 902–909. [Google Scholar] [CrossRef]
- Daoust, J.-F. Elderly people and responses to COVID-19 in 27 Countries. PLoS ONE 2020, 15, e0235590. [Google Scholar] [CrossRef]
- Shimokihara, S.; Maruta, M.; Hidaka, Y.; Akasaki, Y.; Tokuda, K.; Han, G.; Ikeda, Y.; Tabira, T. Relationship of Decrease in Frequency of Socialization to Daily Life, Social Life, and Physical Function in Community-Dwelling Adults Aged 60 and Over after the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2573. [Google Scholar] [CrossRef]
- Pérez-Cano, H.J.; Moreno-Murguía, M.B.; Morales-López, O.; Crow-Buchanan, O.; English, J.A.; Lozano-Alcázar, J.; Somilleda-Ventura, S.A. Anxiety, depression, and stress in response to the coronavirus disease-19 pandemic. Cir. Cir. 2020, 88, 562–568. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Tsutsumimoto, K.; Lee, S.; Doi, T.; Nakakubo, S.; Hotta, R.; Suzuki, T. Social Frailty in Community-Dwelling Older Adults as a Risk Factor for Disability. J. Am. Med. Dir. Assoc. 2015, 16, 1003.e7–1003.e11. [Google Scholar] [CrossRef]
- Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Kurita, S.; Ishii, H.; Shimada, H. Associations Between Active Mobility Index and Disability. J. Am. Med. Dir. Assoc. 2021, in press. [Google Scholar] [CrossRef]
- Spaltenstein, J.; Bula, C.; Santos-Eggimann, B.; Krief, H.; Seematter-Bagnoud, L. Factors associated with going outdoors frequently: A cross-sectional study among Swiss community-dwelling older adults. BMJ Open 2020, 10, e034248. [Google Scholar] [CrossRef]
- Sasaki, N.; Kuroda, R.; Tsuno, K.; Kawakami, N. Exposure to media and fear and worry about COVID-19. Psychiatry Clin. Neurosci. 2020, 74, 501–502. [Google Scholar] [CrossRef]
- Japan Ministry of Health. Labour and Welfare the National Health and Nutrition Survey in Japan. 2019. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450171&tstat=000001041744&cycle=7&year=20190&month=0&tclass1=000001148507 (accessed on 16 May 2021).
- Gorenko, J.A.; Moran, C.; Flynn, M.; Dobson, K.; Konnert, C. Social Isolation and Psychological Distress Among Older Adults Related to COVID-19: A Narrative Review of Remotely-Delivered Interventions and Recommendations. J. Appl. Gerontol. 2021, 40, 3–13. [Google Scholar] [CrossRef]
- Ueki, H.; Furusawa, Y.; Iwatsuki-Horimoto, K.; Imai, M.; Kabata, H.; Nishimura, H.; Kawaoka, Y. Effectiveness of Face Masks in Preventing Airborne Transmission of SARS-CoV-2. mSphere 2020, 5, e00637-20. [Google Scholar] [CrossRef]
- Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Krznaric, Z.; Nitzan, D.; Pirlich, M.; Singer, P.; The ESPEN Council. ESPEN expert statements and practical guidance for nutritional management of individuals with SARS-CoV-2 infection. Clin. Nutr. 2020, 39, 1631–1638. [Google Scholar] [CrossRef]


{kind=link}
| Factor a | ||||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| uneasiness about the information in the mass media | 0.66 | 0.09 | 0.02 | −0.14 | −0.38 | −0.12 | 0.02 | 0.19 |
| increased nervousness | 0.66 | 0.03 | −0.06 | 0.22 | −0.05 | 0.08 | −0.32 | −0.05 |
| increased restlessness | 0.64 | −0.01 | −0.09 | −0.09 | 0.15 | 0.15 | −0.11 | 0.01 |
| anxiety | 0.51 | −0.10 | 0 | 0.09 | 0.01 | −0.07 | 0.42 | −0.13 |
| mental fatigue | 0.04 | 0.80 | 0.11 | −0.19 | −0.15 | 0.13 | −0.11 | 0.04 |
| sleeplessness | −0.05 | 0.74 | −0.04 | 0.37 | 0.01 | −0.29 | −0.03 | −0.01 |
| depressed | 0.27 | 0.33 | −0.04 | 0.18 | 0.29 | −0.12 | 0.15 | 0.02 |
| emotional instability | 0.05 | 0.31 | 0.04 | −0.27 | 0.27 | 0.22 | 0.12 | −0.26 |
| anxiousness to meet people | −0.10 | 0.09 | 0.83 | 0.16 | −0.1 | 0 | 0 | 0.02 |
| anxiousness to go outside | −0.04 | −0.09 | 0.76 | 0.04 | 0.06 | −0.13 | 0.25 | 0.10 |
| being angry when someone is not wearing a mask | 0.05 | 0.25 | 0.45 | −0.03 | 0.11 | 0.20 | −0.21 | −0.06 |
| does not trust what others say | 0.10 | −0.10 | 0.10 | 0.80 | 0.05 | 0.11 | −0.08 | −0.07 |
| increased carelessness | −0.10 | 0.15 | 0.08 | 0.60 | −0.16 | 0.29 | 0.09 | −0.03 |
| frustration | −0.14 | −0.12 | −0.01 | −0.01 | 0.87 | −0.01 | −0.09 | −0.01 |
| mental stress | 0.19 | 0.09 | 0.02 | −0.15 | 0.41 | −0.08 | 0.23 | 0.13 |
| bradyphrenia | −0.01 | 0 | −0.04 | 0.17 | 0.07 | 0.74 | −0.12 | 0.07 |
| afraid of rumors | 0.32 | −0.18 | 0.08 | 0.13 | −0.2 | 0.5 | 0.15 | −0.11 |
| increased amnesia | −0.17 | 0.23 | −0.26 | 0.08 | −0.18 | 0.35 | 0.34 | 0.09 |
| worry about not being able to see family | −0.15 | −0.09 | 0.07 | −0.03 | −0.04 | −0.06 | 0.82 | −0.15 |
| not smiling as much as before | −0.04 | 0.03 | 0.05 | −0.04 | 0.02 | 0.28 | 0.41 | 0.19 |
| anorexia | 0.01 | 0.08 | 0.06 | −0.17 | −0.11 | −0.05 | −0.13 | 0.81 |
| unmotivated | 0.04 | −0.13 | 0 | 0.17 | 0.32 | 0.24 | −0.02 | 0.6 |
| Characteristic | Overall, n = 493 | Increased/Unchanged FGO, n = 149 | Decreased FGO, n = 344 | ES | p-Value |
|---|---|---|---|---|---|
| Age † | 73.6 (7.0) | 75.17 (7.25) | 72.92 (6.72) | 0.326 | 0.001 a |
| Gender ‡ | 0.108 | 0.024 b | |||
| male | 68 (14%) | 29 (19%) | 39 (11%) | ||
| female | 425 (86%) | 120 (81%) | 305 (89%) | ||
| Family structure ‡ | 0.019 | 0.666 b | |||
| living alone | 126 (26%) | 40 (27%) | 86 (25%) | ||
| living with family | 367 (74%) | 109 (73%) | 258 (75%) | ||
| Number of underlying diseases § | 1 (0–7) | 1 (0–7) | 1 (0–6) | 0.771 c |
| Question Items | Overall, n = 493 † | Increased/Unchanged FGO, n = 149 † | Decreased FGO, n = 344 † | ES | p-Value |
|---|---|---|---|---|---|
| General psychological condition | |||||
| Mental stress | 0.172 | <0.001 | |||
| yes | 141 (29%) | 25 (17%) | 116 (34%) | ||
| Mental fatigue | 0.155 | <0.001 | |||
| yes | 79 (16%) | 11 (7.4%) | 68 (20%) | ||
| Frustration | 0.112 | 0.024 | |||
| yes | 25 (5.1%) | 2 (1.3%) | 23 (6.7%) | ||
| Unmotivated | 0.148 | 0.002 | |||
| yes | 93 (19%) | 15 (10%) | 78 (23%) | ||
| Depressed | 0.058 | 0.253 | |||
| yes | 57 (12%) | 13 (8.7%) | 44 (13%) | ||
| Bradyphrenia | 0.074 | 0.141 | |||
| yes | 42 (8.5%) | 8 (5.4%) | 34 (9.9%) | ||
| Sleeplessness | 0.079 | 0.111 | |||
| yes | 55 (11%) | 11 (7.4%) | 44 (13%) | ||
| Anorexia | 0.068 | 0.206 | |||
| yes | 20 (4.1%) | 3 (2.0%) | 17 (4.9%) | ||
| Emotional instability | 0.001 | 0.988 | |||
| yes | 10 (2.0%) | 3 (2.0%) | 7 (2.0%) | ||
| Anxiety | 0.079 | 0.111 | |||
| yes | 55 (11%) | 11 (7.4%) | 44 (13%) | ||
| Not smiling as much as before | 0.197 | <0.001 | |||
| yes | 90 (18%) | 10 (6.7%) | 80 (23%) | ||
| Increased amnesia | 0.043 | 0.426 | |||
| yes | 56 (11%) | 20 (13%) | 36 (10%) | ||
| Increased carelessness | 0.017 | 0.853 | |||
| yes | 33 (6.7%) | 9 (6.0%) | 24 (7.0%) | ||
| Increased restlessness | 0.002 | 0.965 | |||
| yes | 13 (2.6%) | 4 (2.7%) | 9 (2.6%) | ||
| Increased nervousness | 0.022 | 0.799 | |||
| yes | 23 (4.7%) | 8 (5.4%) | 15 (4.4%) | ||
| COVID-19 pandemic-related psychological condition | |||||
| Anxiousness to go outside | 0.219 | <0.001 | |||
| yes | 140 (28%) | 20 (13%) | 120 (35%) | ||
| Anxiousness to meet people | 0.084 | 0.084 | |||
| yes | 83 (17%) | 18 (12%) | 65 (19%) | ||
| Worry about not being able to see family | 0.062 | 0.218 | |||
| yes | 69 (14%) | 16 (11%) | 53 (15%) | ||
| Uneasiness about the information in the mass media | 0.014 | 0.562 | |||
| yes | 92 (19%) | 25 (17%) | 67 (19%) | ||
| Afraid of rumors | 0.032 | 0.725 | |||
| yes | 35 (7.1%) | 12 (8.1%) | 23 (6.7%) | ||
| Does not trust what others say | 0.024 | 0.180 | |||
| yes | 14 (2.8%) | 7 (4.7%) | 7 (2.0%) | ||
| Being angry when someone is not wearing a mask | 0.074 | 0.010 | |||
| yes | 72 (15%) | 12 (8.1%) | 60 (17%) |
| Crude Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|
| Wald χ2 | OR (95% CI) | p-Value | Wald χ2 | OR (95% CI) | p-Value | |
| Mental stress | ||||||
| no a | - | - | - | - | - | - |
| yes | 3.94 | 1.69 (1.01–2.84) | 0.047 | 3.07 | 1.60 (0.95–2.70) | 0.080 |
| Mental fatigue | ||||||
| no a | - | - | - | - | - | - |
| yes | 4.90 | 2.23 (1.10–4.53) | 0.027 | 3.89 | 2.05 (1.00–4.20) | 0.049 |
| Frustration | ||||||
| no a | - | - | - | - | - | - |
| yes | 3.18 | 3.96 (0.87–18.00) | 0.074 | 2.99 | 3.80 (0.84–17.28) | 0.084 |
| Unmotivated | ||||||
| no a | - | - | - | - | - | - |
| yes | 4.10 | 1.91 (1.02–3.57) | 0.043 | 3.59 | 1.84 (0.98–3.47) | 0.058 |
| Not smiling as much as before | ||||||
| no a | - | - | - | - | - | - |
| yes | 8.85 | 2.98 (1.45–6.11) | 0.003 | 10.80 | 3.43 (1.65–7.16) | 0.001 |
| Anxiousness to go outside | ||||||
| no a | - | - | - | - | - | - |
| yes | 15.78 | 3.00 (1.74–5.15) | <0.001 | 13.17 | 2.75 (1.59–4.74) | <0.001 |
| Being angry when someone is not wearing a mask | ||||||
| no a | - | - | - | - | - | - |
| yes | 1.37 | 1.52 (0.75–3.08) | 0.242 | 1.93 | 1.66 (0.81–3.40) | 0.165 |
| Gender | ||||||
| Female a | - | - | - | - | - | - |
| Male | - | - | - | 2.18 | 0.65 (0.36–1.15) | 0.140 |
| Age | - | - | - | 7.78 | 0.96 (0.93–0.99) | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimokihara, S.; Maruta, M.; Akasaki, Y.; Ikeda, Y.; Han, G.; Kamasaki, T.; Tokuda, K.; Hidaka, Y.; Akasaki, Y.; Tabira, T. Association between Frequency of Going Out and Psychological Condition among Community-Dwelling Older Adults after the COVID-19 Pandemic in Japan. Healthcare 2022, 10, 439. https://doi.org/10.3390/healthcare10030439
Shimokihara S, Maruta M, Akasaki Y, Ikeda Y, Han G, Kamasaki T, Tokuda K, Hidaka Y, Akasaki Y, Tabira T. Association between Frequency of Going Out and Psychological Condition among Community-Dwelling Older Adults after the COVID-19 Pandemic in Japan. Healthcare. 2022; 10(3):439. https://doi.org/10.3390/healthcare10030439
Chicago/Turabian StyleShimokihara, Suguru, Michio Maruta, Yasuaki Akasaki, Yuriko Ikeda, Gwanghee Han, Taishiro Kamasaki, Keiichiro Tokuda, Yuma Hidaka, Yoshihiko Akasaki, and Takayuki Tabira. 2022. "Association between Frequency of Going Out and Psychological Condition among Community-Dwelling Older Adults after the COVID-19 Pandemic in Japan" Healthcare 10, no. 3: 439. https://doi.org/10.3390/healthcare10030439