
Measurements of Tear Evaporation Rate in Subjects with Refractive Errors Using a Portable Evaporimeter

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
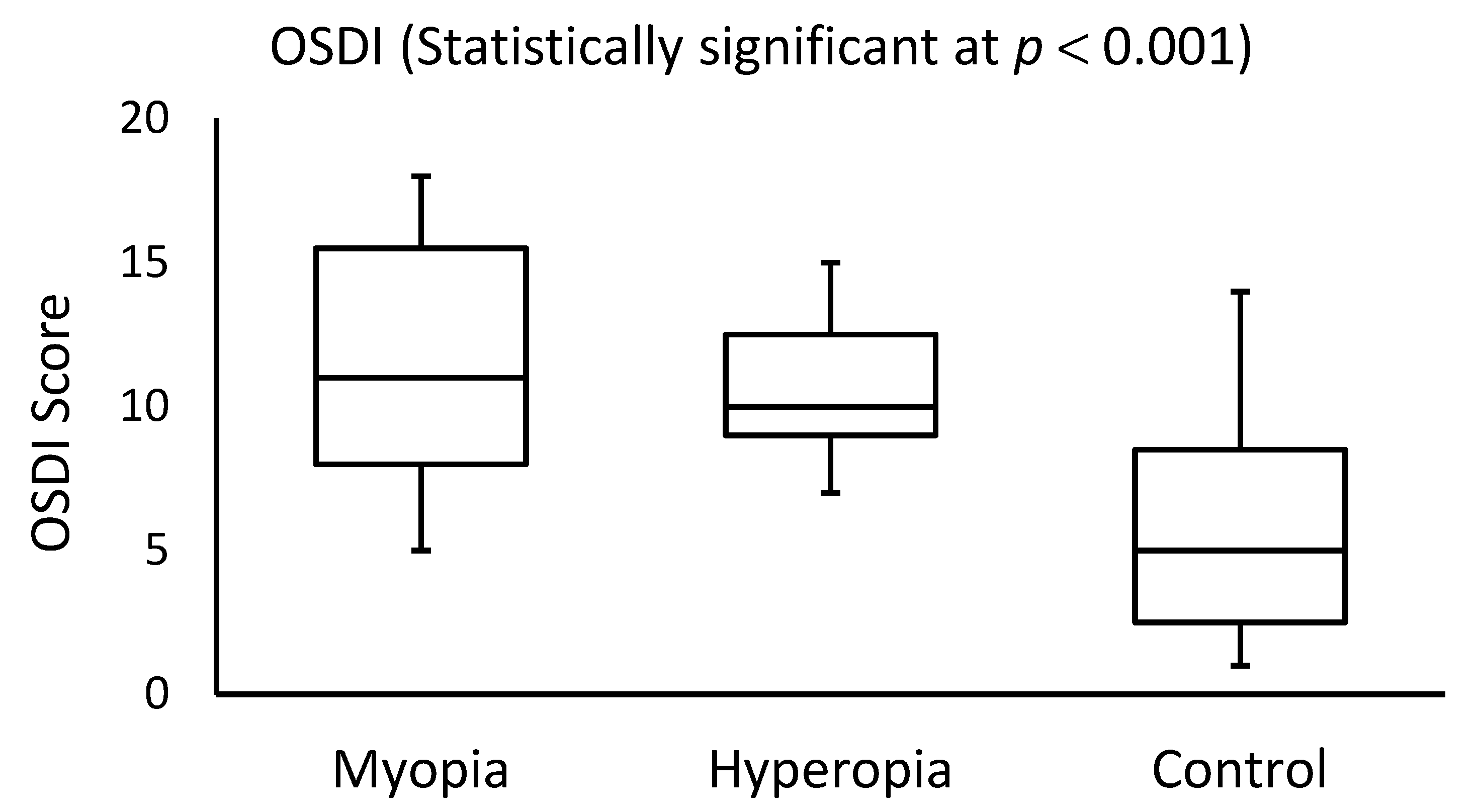
2.2. OSDI
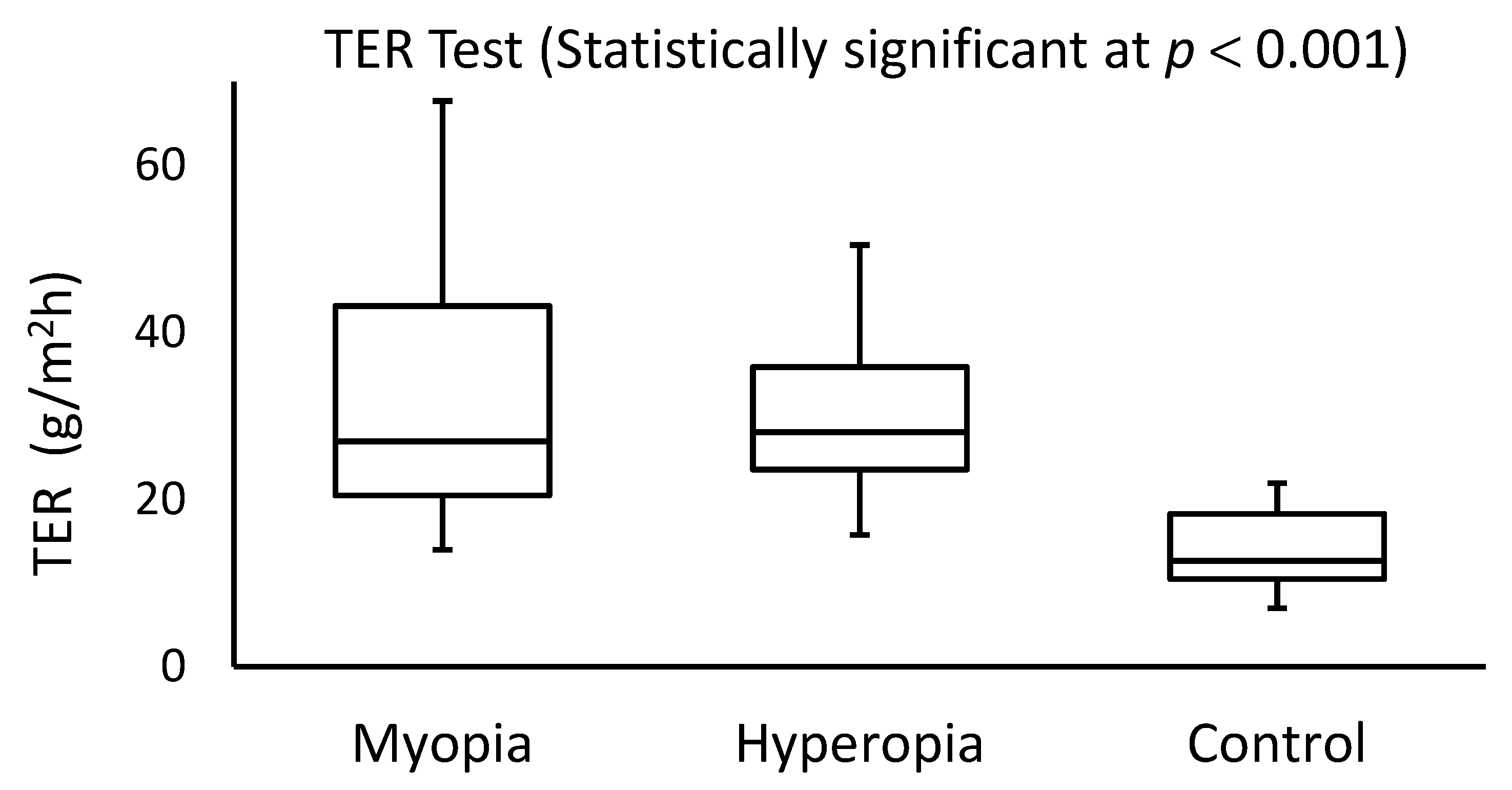
2.3. TER Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harb, E.N.; Wildsoet, C.F. Origins of refractive errors: Environmental and genetic factors. Annu. Rev. Vis. Sci. 2009, 5, 47–72. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, K.S.; Leasher, J.; Bourne, R.R.; Flaxman, S.R.; Jonas, J.B.; Keeffe, J.; Limburg, H.; Pesudovs, K.; Price, H.; White, R.A.; et al. Global vision impairment and blindness due to uncorrected refractive error, 1990–2010. Optom. Vis. Sci. 2016, 93, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Fotouhi, A.; Yekta, A.; Pakzad, R.; Ostadimoghaddam, H.; Khabazkhoob, M. Global and regional estimates of prevalence of refractive errors: Systematic review and meta-analysis. J. Curr. Ophthalmol. 2000, 30, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.; Anker, S.; Bobier, W.; Braddick, O.; Durden, K.; Nardini, M.; Watson, P. Normal emmetropization in infants with spectacle correction for hyperopia. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3726–3731. [Google Scholar]
- The COMET Group. Myopia stabilization and associated factors among participants in the Correction of Myopia Evaluation Trial (COMET). Investig. Ophthalmol. Vis. Sci. 2013, 54, 7871–7883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abd Almajeed, R.H.A.; Elawad, M.E. The effect of spherical refractive error on tear volume. Al-Basar Int. J. Ophthalmol. 2017, 4, 104–108. [Google Scholar] [CrossRef]
- Fahmy, R.M.; Aldarwesh, A. Correlation between dry eye and refractive error in Saudi young adults using noninvasive Keratograph 4. Indian J. Ophthalmol. 2018, 66, 653–654. [Google Scholar] [CrossRef]
- Dhungel, D.; Shrestha, G.S. Visual symptoms associated with refractive errors among Thangka artists of Kathmandu valley. BMC Ophthalmol. 2017, 17, 258. [Google Scholar] [CrossRef] [Green Version]
- Shimazaki, K. Definition and diagnostic criteria of dry eye disease: Historical overview and future directions. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES7–DES12. [Google Scholar] [CrossRef] [Green Version]
- Willcox, M.D.P.; Argüeso, P.; Georgiev, G.A. TFOS DEWS II tear film report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.-K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II definition and classification report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- DEWS Definition and Classification. The definition and classification of dry eye disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop. Ocul. Surf. 2007, 5, 75–92. [Google Scholar] [CrossRef]
- Bron, A.J.; Tiffany, J.M. The contribution of meibomian disease to dry eye. Ocul. Surf. 2004, 2, 149–165. [Google Scholar] [CrossRef]
- King-Smith, P.E.; Ramamoorthy, P.; Braun, R.J.; Nichols, J.J. Tear film images and breakup analyzed using fluorescent quenching. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6003–6011. [Google Scholar] [CrossRef]
- Siddique, J.I.; Braun, R.J. Tear film dynamics with evaporation, osmolarity and surfactant transport. Appl. Math. Model. 2015, 39, 255–269. [Google Scholar] [CrossRef]
- Chhadva, P.; Goldhardt, R.; Galor, A. Meibomian gland disease: The role of gland dysfunction in dry eye disease. Ophthalmology 2017, 124, S20–S26. [Google Scholar] [CrossRef]
- Kulovesi, P.; Rantamaki, A.H.; Holopainen, J.M. Surface properties of artificial tear film lipid layers: Effects of wax esters. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4448–4454. [Google Scholar] [CrossRef] [Green Version]
- DEWS Epidemiology. The epidemiology of dry eye disease: Report of the Epidemiology Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 93–107. [Google Scholar] [CrossRef]
- Ghislandi, G.M.; Lima, G.C. Comparative study between phenol red thread test and the Schirmer’s test in the diagnosis of dry eyes syndrome. Rev. Bras. Oftalmol. 2016, 75, 438–442. [Google Scholar] [CrossRef]
- Masmali, M.A.; Alanazi, S.A.; Almagren, B.; El-Hiti, G.A. Assessment of the tear film in normal eye subjects after consumption of a single dose of hot peppermint drink. Clin. Optom. 2019, 11, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Masmali, A.; Alrabiah, S.; Alharbi, A.; El-Hiti, G.A.; Almubrad, T. Investigation of tear osmolarity using the TearLab Osmolarity System in normal adults in Saudi Arabia. Eye Contact Lens 2014, 40, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Abusharaha, A.; Alturki, A.A.; Alanazi, S.A.; Fagehi, R.; Al-Johani, N.; El-Hiti, G.A.; Masmali, A.M. Assessment of tear-evaporation rate in thyroid-gland patients. Clin. Ophthalmol. 2019, 13, 131–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alanazi, S.A.; Abusharha, A.; Fagehi, R.; Alsaqr, A.M.; El-Hiti, G.A.; Alahmari, R.A.; Alenazi, F.A.; Alnassar, K.M.A.; Masmali, A.M. Assessment of the tear evaporation rate in chronic smokers using Delfin VapoMeter. Int. J. Ophthalmol. Vis. Sci. 2019, 4, 37–41. [Google Scholar] [CrossRef]
- Mathers, W.D.; Binarao, G.; Petroll, M. Ocular water evaporation and the dry eye: A new measuring device. Cornea 1992, 12, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Tsubota, K.; Yamada, M. Tear evaporation from the ocular surface. Investig. Ophthalmol Vis. Sci. 1992, 33, 2942–2950. [Google Scholar]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [Green Version]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Ridder, W.H., 3rd; Tomlinson, A.; Huang, J.F.; Li, J. Impaired visual performance in patients with dry eye. Ocul. Surf. 2011, 9, 42–55. [Google Scholar] [CrossRef]
- Schein, O.D.; Tielsch, J.M.; Muñoz, B.; Bandeen-Roche, K.; West, S. Relation between signs and symptoms of dry eye in the elderly: A population-based perspective. Ophthalmology 1997, 104, 1395–1401. [Google Scholar] [CrossRef]
- McMonnies, C.W. Tear instability importance, mechanisms, validity and reliability of assessment. J. Optom. 2018, 11, 203–210. [Google Scholar] [CrossRef]
- Potvin, R.; Makari, S.; Rapuano, C.J. Tear film osmolarity and dry eye disease: A review of the literature. Clin. Ophthalmol. 2015, 9, 2039–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, E.; Endo, K.; Suzuki, A.; Fujikura, Y.; Matsumoto, Y.; Tsubota, K. Tear evaporation dynamics in normal subjects and subjects with obstructive meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2003, 44, 33–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Čiumbaraitė, R.; Liutkevičienė, R. Refractive errors characteristic of the patients at the Children’s Ophthalmology Outpatient Department of Kauno klinikos Hospital (Lithuanian University of Health Sciences) from 1 January 2012 to 31 December 2012. Acta Med. Litu. 2017, 24, 83–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Li, S.; Zhou, J.; Liu, C.; Xu, M. Relationship between lipid layer thickness, incomplete blinking rate and tear film instability in patients with different myopia degrees after small-incision lenticule extraction. PLoS ONE 2020, 15, e0230119. [Google Scholar] [CrossRef] [PubMed]
- Ilhan, N.; Ilhan, O.; Ayhan Tuzcu, E.A.; Daglioglu, M.C.; Coskun, M.; Parlakfikirer, N.; Keskin, U. Is there a relationship between pathologic myopia and dry eye syndrome? Cornea 2014, 33, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Abusharha, A.A.; Yami, A.A.; Alsreea, K.; Fagehi, R.; Alsaqr, A.; Alanazi, S.; Masmali, A. Repeatability and reproducibility of tear film evaporation rate measurement using a new closed-chamber evaporimeter. Open Ophthalmol. J. 2021, 15, 117–121. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Mean ± SD or Median (IQR) | ||
|---|---|---|---|
| Myopia (N = 25) | Hyperopia (N = 25) | Control (N = 25) | |
| Age (year) | 28.8 ± 6.8 | 27.7 ± 5.5 | 23.6 ± 2.6 |
| OSDI | 11.0 (7.5) | 10.0 (3.5) | 5.0 (6.0) |
| TER (g/m2h) | 27.0 (22.7) | 28.3 (11.8) | 12.7 (7.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fagehi, R.; El-Hiti, G.A.; Alsubaie, M.H.; Abusharha, A.; Alanazi, M.A.; Masmali, A.M.; Almubrad, T. Measurements of Tear Evaporation Rate in Subjects with Refractive Errors Using a Portable Evaporimeter. Healthcare 2022, 10, 405. https://doi.org/10.3390/healthcare10020405
Fagehi R, El-Hiti GA, Alsubaie MH, Abusharha A, Alanazi MA, Masmali AM, Almubrad T. Measurements of Tear Evaporation Rate in Subjects with Refractive Errors Using a Portable Evaporimeter. Healthcare. 2022; 10(2):405. https://doi.org/10.3390/healthcare10020405
Chicago/Turabian StyleFagehi, Raied, Gamal A. El-Hiti, Mushawwat H. Alsubaie, Ali Abusharha, Mana A. Alanazi, Ali M. Masmali, and Turki Almubrad. 2022. "Measurements of Tear Evaporation Rate in Subjects with Refractive Errors Using a Portable Evaporimeter" Healthcare 10, no. 2: 405. https://doi.org/10.3390/healthcare10020405