
Smartphone-Based Visual Inspection with Acetic Acid: An Innovative Tool to Improve Cervical Cancer Screening in Low-Resource Setting

 ,
,  , and
, and
Abstract
:1. Introduction
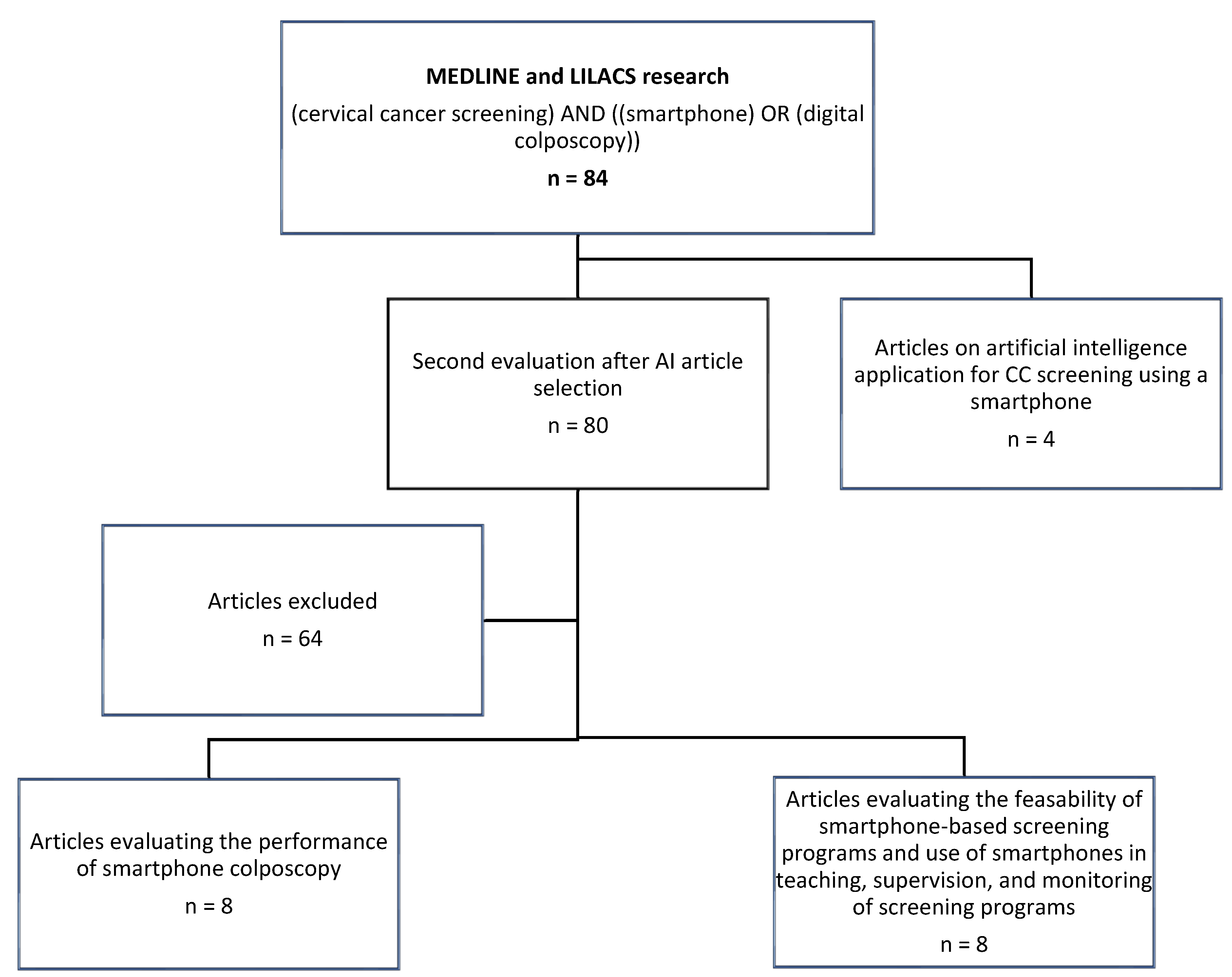
2. Methodology
3. Visual Inspection with Acetic Acid (VIA): Strengths and Limitations
4. VIA-Enhanced with Digital Imaging
5. Performance for CIN2+ Diagnosis
6. On-Site Training and Supervision
7. Off-Site Mentorship
8. Data Registration and Monitoring
9. Artificial Intelligence: A Vision of the Future
10. Conclusions and Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Globocan. Globocan 2020: New Global Cancer Data. Available online: https://www.uicc.org/news/globocan-2020-new-global-cancer-data (accessed on 29 December 2021).
- World Health Organisation. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem. Available online: https://www.who.int/publications/i/item/9789240014107 (accessed on 29 December 2021).
- World Health Organisation. Guidelines for Screening and Treatment of Precancerous Lesions for Cervical Cancer Prevention. Available online: http://www.who.int/reproductivehealth/publications/cancers_screening_and_treatment_of_precancerous_lesions/en/ (accessed on 29 December 2021).
- Cubie, H.A.; Campbell, C. Cervical cancer screening—The challenges of complete pathways of care in low-income countries: Focus on Malawi. Womens Health 2020, 16, 1745506520914804. [Google Scholar] [CrossRef] [PubMed]
- Firnhaber, C.; Mao, L.; Levin, S.; Faesen, M.; Lewis, D.A.; Goeieman, B.J.; Swarts, A.J.; Rakhombe, N.; Michelow, P.M.; Williams, S.; et al. Evaluation of a cervicography-based program to ensure quality of visual inspection of the cervix in HIV-infected women in Johannesburg, South Africa. J. Low. Genit. Tract Dis. 2015, 19, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Manga, S.; Parham, G.; Benjamin, N.; Nulah, K.; Sheldon, L.K.; Welty, E.; Ogembo, J.G.; Bradford, L.; Sando, Z.; Shields, R.; et al. Cervical cancer screening in cameroon: Interobserver agreement on the interpretation of digital cervicography results. J. Low. Genit. Tract Dis. 2015, 19, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Sankaranarayanan, R.; Budukh, A.M.; Rajkumar, R. Effective screening programmes for cervical cancer in low—And middle-income developing countries. Bull. World Health Organ. 2001, 79, 954–962. [Google Scholar] [PubMed]
- Goel, A.; Gandhi, G.; Batra, S.; Bhambhani, S.; Zutshi, V.; Sachdeva, P. Visual inspection of the cervix with acetic acid for cervical intraepithelial lesions. Int. J. Gynaecol. Obstet. 2005, 88, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, R.A.; Santesso, N.; Khatib, R.; Mustafa, A.A.; Wiercioch, W.; Kehar, R.; Gandhi, S.; Chen, Y.; Cheung, A.; Hopkins, J.; et al. Systematic reviews and meta-analyses of the accuracy of HPV tests, visual inspection with acetic acid, cytology, and colposcopy. Int. J. Gynaecol. Obstet. 2016, 132, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Control of cancer of the cervix uteri. A WHO meeting. Bull World Health Organ 1986, 64, 607–618. [Google Scholar]
- World Health Organisation. Comprehensive Cervical Cancer Control: A Guide to Essential Practice—Second Edition. Available online: https://www.who.int/reproductivehealth/publications/cancers/cervical-cancer-guide/en/ (accessed on 29 December 2021).
- Parham, G.P.; Mwanahamuntu, M.H.; Pfaendler, K.S.; Sahasrabuddhe, V.V.; Myung, D.; Mkumba, G.; Kapambwe, S.; Mwanza, B.; Chibwesha, C.; Hicks, M.L.; et al. eC3—A modern telecommunications matrix for cervical cancer prevention in Zambia. J. Low. Genit. Tract. Dis. 2010, 14, 167–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Castro Hillmann, E.; Moreira Bacha, O.; Roy, M.; Paris, G.; Berbiche, D.; Nizard, V.; Lopes Ramos, J.G. Cervical Digital Photography: An Alternative Method to Colposcopy. J. Obstet. Gynaecol. Can. 2019, 41, 1099–1107. [Google Scholar] [CrossRef]
- De Vuyst, H.; Claeys, P.; Njiru, S.; Muchiri, L.; Steyaert, S.; De Sutter, P.; Van Marck, E.; Bwayo, J.; Temmerman, M. Comparison of pap smear, visual inspection with acetic acid, human papillomavirus DNA-PCR testing and cervicography. Int. J. Gynaecol. Obstet. 2005, 89, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Bateman, A.C.; Katundu, K.; Mwanahamuntu, M.H.; Kapambwe, S.; Sahasrabuddhe, V.V.; Hicks, M.L.; Chi, B.H.; Stringer, J.S.; Parham, G.P.; Chibwesha, C.J. The burden of cervical pre-cancer and cancer in HIV positive women in Zambia: A modeling study. BMC Cancer 2015, 15, 541. [Google Scholar] [CrossRef] [Green Version]
- Ricard-Gauthier, D.; Wisniak, A.; Catarino, R.; van Rossum, A.F.; Meyer-Hamme, U.; Negulescu, R.; Scaringella, S.; Jinoro, J.; Vassilakos, P.; Petignat, P. Use of smartphones as adjuvant tools for cervical cancer screening in low-resource settings. J. Low. Genit. Tract Dis. 2015, 19, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Gallay, C.; Girardet, A.; Viviano, M.; Catarino, R.; Benski, A.C.; Tran, P.L.; Ecabert, C.; Thiran, J.P.; Vassilakos, P.; Petignat, P. Cervical cancer screening in low-resource settings: A smartphone image application as an alternative to colposcopy. Int. J. Womens Health 2017, 9, 455–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, P.L.; Benski, C.; Viviano, M.; Petignat, P.; Combescure, C.; Jinoro, J.; Herinianasolo, J.L.; Vassilakos, P. Performance of Smartphone-Based Digital Images for Cervical Cancer Screening in a Low-Resource Context. Int. J. Technol. Assess Health Care 2018, 34, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Mungo, C.; Osongo, C.O.; Ambaka, J.; Randa, M.A.; Samba, B.; Ochieng, C.A.; Barker, E.; Guliam, A.; Omoto, J.; Cohen, C.R. Feasibility and Acceptability of Smartphone-Based Cervical Cancer Screening Among HIV-Positive Women in Western Kenya. JCO. Glob. Oncol. 2021, 7, 686–693. [Google Scholar] [CrossRef]
- Goldstein, A.; Goldstein, L.S.; Lipson, R.; Bedell, S.; Wang, J.; Stamper, S.A.; Brenner, G.; Goldstein, G.R.; O’Keefe, K.D.; O’Keefe, S.C.; et al. Assessing the feasibility of a rapid, high-volume cervical cancer screening programme using HPV self-sampling and digital colposcopy in rural regions of Yunnan, China. BMJ Open 2020, 10, e035153. [Google Scholar] [CrossRef] [Green Version]
- Thay, S.; Goldstein, A.; Goldstein, L.S.; Govind, V.; Lim, K.; Seang, C. Prospective cohort study examining cervical cancer screening methods in HIV-positive and HIV-negative Cambodian Women: A comparison of human papilloma virus testing, visualization with acetic acid and digital colposcopy. BMJ Open 2019, 9, e026887. [Google Scholar] [CrossRef] [Green Version]
- Urner, E.; Delavy, M.; Catarino, R.; Viviano, M.; Meyer-Hamme, U.; Benski, A.C.; Jinoro, J.; Heriniainasolo, J.L.; Undurraga, M.; De Vuyst, H.; et al. A Smartphone-based approach for triage of human papillomavirus-positive sub-saharan african women: A prospective study. JMIR Mhealth Uhealth 2017, 5, e72. [Google Scholar] [CrossRef]
- Catarino, R.; Vassilakos, P.; Scaringella, S.; Undurraga-Malinverno, M.; Meyer-Hamme, U.; Ricard-Gauthier, D.; Matute, J.C.; Petignat, P. Smartphone Use for Cervical Cancer Screening in Low-Resource Countries: A Pilot Study Conducted in Madagascar. PLoS ONE 2015, 10, e0134309. [Google Scholar] [CrossRef] [Green Version]
- Silkensen, S.L.; Schiffman, M.; Sahasrabuddhe, V.; Flanigan, J.S. Is It Time to Move Beyond Visual Inspection With Acetic Acid for Cervical Cancer Screening? Glob. Health Sci. Pract. 2018, 6, 242–246. [Google Scholar] [CrossRef] [Green Version]
- Asgary, R.; Cole, H.; Adongo, P.; Nwameme, A.; Maya, E.; Adu-Amankwah, A.; Barnett, H.; Adanu, R. Acceptability and implementation challenges of smartphone-based training of community health nurses for visual inspection with acetic acid in Ghana: mHealth and cervical cancer screening. BMJ Open 2019, 9, e030528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeates, K.E.; Sleeth, J.; Hopman, W.; Ginsburg, O.; Heus, K.; Andrews, L.; Giattas, M.R.; Yuma, S.; Macheku, G.; Msuya, A.; et al. Evaluation of a Smartphone-Based Training Strategy Among Health Care Workers Screening for Cervical Cancer in Northern Tanzania: The Kilimanjaro Method. J. Glob. Oncol. 2016, 2, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Negulescu, R.A.; Catarino, R.; De Vuyst, H.; Undurraga-Malinverno, M.; Meyer-Hamme, U.; Alec, M.; Campana, A.; Vassilakos, P.; Petignat, P. Web-based instrument to assess skills in visual inspection of the cervix among healthcare providers. Int. J. Gynaecol. Obstet. 2016, 134, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Sanghvi, H.; Limpaphayom, K.K.; Plotkin, M.; Charurat, E.; Kleine, A.; Lu, E.; Eamratsameekool, W.; Palanuwong, B. Cervical cancer screening using visual inspection with acetic acid: Operational experiences from Ghana and Thailand. Reprod Health Matters 2008, 16, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Asgary, R.; Staderini, N.; Mthethwa-Hleta, S.; Lopez Saavedra, P.A.; Garcia Abrego, L.; Rusch, B.; Marie Luce, T.; Rusike Pasipamire, L.; Ndlangamandla, M.; Beideck, E.; et al. Evaluating smartphone strategies for reliability, reproducibility, and quality of VIA for cervical cancer screening in the Shiselweni region of Eswatini: A cohort study. PLoS Med. 2020, 17, e1003378. [Google Scholar] [CrossRef]
- Yeates, K.; Erwin, E.; Mtema, Z.; Magoti, F.; Nkumbugwa, S.; Yuma, S.; Hopman, W.M.; Ferguson, A.; Oneko, O.; Macheku, G.; et al. Smartphone-Enhanced Training, QA, Monitoring, and Evaluation of a Platform for Secondary Prevention of Cervical Cancer: Opportunities and Challenges to Implementation in Tanzania. JCO Glob. Oncol. 2020, 6, 1114–1123. [Google Scholar] [CrossRef]
- Quercia, K.; Tran, P.L.; Jinoro, J.; Herniainasolo, J.L.; Viviano, M.; Vassilakos, P.; Benski, C.; Petignat, P. A Mobile Health Data Collection System for Remote Areas to Monitor Women Participating in a Cervical Cancer Screening Campaign. Telemed. J. E. Health 2018, 24, 277–282. [Google Scholar] [CrossRef]
- Sharma, D.; Rohilla, L.; Bagga, R.; Srinivasan, R.; Jindal, H.A.; Sharma, N.; Kankaria, A.; Jamir, L.; Suri, V.; Singh, R.K.; et al. Feasibility of implementing cervical cancer screening program using smartphone imaging as a training aid for nurses in rural India. Public Health Nurs. 2018, 35, 526–533. [Google Scholar] [CrossRef]
- Asgary, R.; Adongo, P.B.; Nwameme, A.; Cole, H.V.; Maya, E.; Liu, M.; Yeates, K.; Adanu, R.; Ogedegbe, O. mHealth to Train Community Health Nurses in Visual Inspection With Acetic Acid for Cervical Cancer Screening in Ghana. J. Low Genit. Tract. Dis. 2016, 20, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Peterson, C.W.; Rose, D.; Mink, J.; Levitz, D. Real-Time Monitoring and Evaluation of a Visual-Based Cervical Cancer Screening Program Using a Decision Support Job Aid. Diagnostics 2016, 6, 20. [Google Scholar] [CrossRef] [Green Version]
- Fokom Domgue, J.; Baker, E.; Manjuh, F.; Lopez, M.; Welty, T.; Schmeler, K.M.; The Cameroon Cervical Cancer Prevention ECHO Collaborative Group. Connecting frontline providers in Africa with distant experts to improve patients’ outcomes through Project ECHO: A successful experience in Cameroon. Int. J. Gynecol. Cancer 2019, 29, 1446–1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, S.; Isaac, R.; Finkel, M.; Evans, J.; Grant, L.; Paul, B.; Weller, D. Mobile technology and cancer screening: Lessons from rural India. J. Glob. Health 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Fink, C.; Blum, A.; Buhl, T.; Mitteldorf, C.; Hofmann-Wellenhof, R.; Deinlein, T.; Stolz, W.; Trennheuser, L.; Cussigh, C.; Deltgen, D.; et al. Diagnostic performance of a deep learning convolutional neural network in the differentiation of combined naevi and melanomas. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Sounderajah, V.; Martin, G.; Ting, D.S.W.; Karthikesalingam, A.; King, D.; Ashrafian, H.; Darzi, A. Diagnostic accuracy of deep learning in medical imaging: A systematic review and meta-analysis. NPJ Digit. Med. 2021, 4, 65. [Google Scholar] [CrossRef]
- Miyagi, Y.; Takehara, K.; Miyake, T. Application of deep learning to the classification of uterine cervical squamous epithelial lesion from colposcopy images. Mol. Clin. Oncol. 2019, 11, 583–589. [Google Scholar] [CrossRef]
- Xue, P.; Tang, C.; Li, Q.; Li, Y.; Shen, Y.; Zhao, Y.; Chen, J.; Wu, J.; Li, L.; Wang, W.; et al. Development and validation of an artificial intelligence system for grading colposcopic impressions and guiding biopsies. BMC Med. 2020, 18, 406. [Google Scholar] [CrossRef]
- Peng, G.; Dong, H.; Liang, T.; Li, L.; Liu, J. Diagnosis of cervical precancerous lesions based on multimodal feature changes. Comput. Biol. Med. 2021, 130, 104209. [Google Scholar] [CrossRef]
- Li, Y.; Liu, Z.H.; Xue, P.; Chen, J.; Ma, K.; Qian, T.; Zheng, Y.; Qiao, Y.L. GRAND: A large-scale dataset and benchmark for cervical intraepithelial Neoplasia grading with fine-grained lesion description. Med. Image. Anal. 2021, 70, 102006. [Google Scholar] [CrossRef]
- Xue, Z.; Novetsky, A.P.; Einstein, M.H.; Marcus, J.Z.; Befano, B.; Guo, P.; Demarco, M.; Wentzensen, N.; Long, L.R.; Schiffman, M.; et al. A demonstration of automated visual evaluation of cervical images taken with a smartphone camera. Int. J. Cancer 2020, 147, 2416–2423. [Google Scholar] [CrossRef]
- Kudva, V.; Prasad, K.; Guruvare, S. Andriod Device-Based Cervical Cancer Screening for Resource-Poor Settings. J. Digit Imaging 2018, 31, 646–654. [Google Scholar] [CrossRef]
- Bae, J.K.; Roh, H.J.; You, J.S.; Kim, K.; Ahn, Y.; Askaruly, S.; Park, K.; Yang, H.; Jang, G.J.; Moon, K.H.; et al. Quantitative Screening of Cervical Cancers for Low-Resource Settings: Pilot Study of Smartphone-Based Endoscopic Visual Inspection After Acetic Acid Using Machine Learning Techniques. JMIR Mhealth Uhealth 2020, 8, e16467. [Google Scholar] [CrossRef] [PubMed]
- Vinals, R.; Vassilakos, P.; Rad, M.S.; Undurraga, M.; Petignat, P.; Thiran, J.P. Using dynamic features for automatic cervical precancer detection. Diagnostics 2021, 11, 716. [Google Scholar] [CrossRef] [PubMed]
- Rossman, A.H.; Reid, H.W.; Pieters, M.M.; Mizelle, C.; von Isenburg, M.; Ramanujam, N.; Huchko, M.J.; Vasudevan, L. Digital Health Strategies for Cervical Cancer Control in Low- and Middle-Income Countries: Systematic Review of Current Implementations and Gaps in Research. J. Med. Internet Res. 2021, 23, e23350. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Population | Intervention and Device | Outcome and Results | Strengths and Weaknesses |
|---|---|---|---|---|
| Mungo et al., 2021 [19] | Western Kenya 25–49 y HIV-positive n = 164 * | D-VIA images taken by nonphysicians. Samsung J8; three off-site expert colposcopists assessed images. | Outcome: performance to detect CIN2+ (off-site) and acceptability of D-VIA. Results: Se ranging from 21.4% (95% CI, 0.06 to 0.43) to 35.7% (95% CI, 0.26 to 0.46). Sp between 85.5% (95% CI, 0.81 to 0.90) to 94.9% (95% CI, 0.92 to 0.98). 99.4% of women were comfortable with the use of a smartphone. | Comment: low sensitivity, very good acceptability. Strengths: histology as reference standard. Limitations: HIV population. |
| Goldstein et al., 2019 [20] | China (rural Yunnan areas) 35–65 y n = 216 * | VIA and digital images. Samsung Galaxy J5 Pro (mobile ODT system). | Outcome: performance to detect CIN1 and CIN2+ Results: Se: NR, Sp: NR. | Comment: accuracy of D-VIA to differentiate between CIN1 and CIN2+ Strengths: histology as reference standard. Limitations: low observed prevalence of HPV (6%), small number of CIN2+ (n = 15). |
| Thay et al., 2019 [21] | Cambodia 30–49 y n= 250 HPV-positive = 56 ** | VIA and digital images. Samsung Galaxy J5 Pro (mobile ODT system). | Outcome: differentiation between CIN1 and CIN2+. Results: Se: NR, Sp: NR. | Comment: accuracy of D-VIA to differentiate between CIN1 and CIN2+. Strengths: histology as reference standard (but only in case of CIN2+ suspicion). Limitations: study setting in an urban hospital, results might not be applicable to rural regions, few CIN2+ lesion (n = 4). |
| Tran et al., 2018 [18] | Madagascar 30–69 y n = 125 * | Forty-five gynecologists (different levels of expertise) assessed D-VIA images. Smartphone Galaxy S4/S5. | Outcome: performance to detect CIN2+. Results: Se 71.3% (95% CI 67–75.7); Sp 62.4% (95% CI 57.5–67.4) | Comment: visual assessment demonstrated relatively high Se. Strengths: histology as reference standard. Limitations: small sample size (19 CIN2+). |
| Gallay et al., 2017 [17] | Madagascar 30–65 y n= 56 * | Four clinicians assessed D-VIA images and classified them in an app called “Exam”. Smartphone Galaxy S4/S5. | Outcome: evaluation of image quality and inter-observer agreement. Results: adequate quality for visual assessment in 93.3% of cases. Moderate inter-observer agreement, with kappa value = 0.45 (0.23–0.56). | Comment: small study, designed only for quality of images. Limitations: no histology for diagnosis confirmation. |
| Urner et al., 2017 [22] | Madagascar 30–69 y n = 187 * | Fifteen clinician evaluated D-VIA images (off-site). Samsung Galaxy S4/S5. | Outcome: performance in the detection of CIN2+. Results: Se 94.1% (95%CI 81.6–98.3); Sp 50.4% (95%CI 35.9–64.8). | Comment: Se to detect CIN2+ lesion better than generally reported. Strengths: histology as reference. Limitations: small sample size and limited number of CIN2+ (n = 14). |
| Catarino et al., 2015 [23] | Madagascar 30–65 y n = 137 * | Comparison of VIA (on-site) and D-VIA (off-site). Samsung Galaxy S4/S5. | Outcome: performance to detect CIN2+ and inter-observer agreement. Results on-sites: Se 66.7% (95%CI 30–90.3); Sp 85.7% (95%CI 76.7–91.6). Results off-site: Se 66.7% (95%CI 30–90.3); Sp 82.3% (95%CI72.4–89.1). Moderate to poor inter-observer agreement: kappa 0.28. | Comment: higher Sp than generally reported, demonstration that off-site assessment is feasible. Strengths: histology as reference Limitations: 30.7% drop-out rate, small sample size |
| Ricard-Gauthier et al., 2015 [16] | Madagascar 30–65 y n = 122 * | Comparison of VIA and D-VIA (on-site) and D-VIA (off-site). Samsung Galaxy S4. | Outcome: performance to detect CIN 2+. Results on-site: Se 28.6% (95%CI 3.7–71%), Sp 87.2% (95%CI 77.7–93.7%). Results off-site: Se ranging from 42.9 (95%CI 9.9–81.6) to 85.7% (95%CI 42.1–99.6); Sp from 48.1 (95% CI 38.5–59.7) to 79.2% (95%CI 68.5–87.6). | Comment; Off-site assessment feasible, lower Se for on-site assessment than reported in literature. Strengths: histology as reference. Limitations: 27.9% drop-out rate, small sample size |
| Studies | Population | Intervention | Results, Comment |
|---|---|---|---|
| Asgary et al., 2020 [29] | Eswatini 25–49 y n = 247 HPV status = NR HIV-positive = 128 * | Smartphone-based VIA screening program, standard VIA training, refresher course, and 6-month mHealth mentorship. | Results: agreement 100% for positive cases and 95.7% for negative; kappa 0.74, then 0.64 after 3 months and 0.79 after 6 months, |
| Yeates et al., 2020 [30] | Tanzania >24 y n = 10,545 HPV status = NR HIV-positive = 2561 ** | Smartphone-enhanced VIA platform (SEVIA) for “real-time secure sharing of cervical images”. Follow-up of the mean VIA+ rates after implementation of SEVIA. Evaluation of VIA images by providers and reviewers. | Results: VIA+ rates increased from 4 to 6.2% after implementation of SEVIA. Provider-Reviewer concordance rate = 90% over the 1-year period. Comment: SEVIA allows enhanced quality of visual inspection, training, real-time data acquisition, monitoring, and evaluation. |
| Asgary et al., 2019 [25] | Ghana mean age = 33.8 y n = 21 HPV status = NR | Providers’ perceptions and experiences: 15 nurses, 1 nurse supervisor, 1 expert reviewer. | Comment: cervical images provided peer-to-peer learning opportunities, better trust of patients, targeted education, and improvement of adherence, as well as implementation of quality control. |
| Quercia et al., 2018 [31] | Madagascar 30–65 y n= 151 HPV status = NR | Registration of cervical cancer screening program data onto a secure web-based platform, for monitoring purposes. Quality of data evaluation. | Results: less than 0.02% of key data missing. Comment: small group. Helps for real-time monitoring, but impact on women follow-up not assessed. |
| Sharma et al., 2018 [32] | India Mean age = 38.79 y n = 180 HPV status = NR | Assessment of nurses’ judgment for diagnosis of cervical pre-cancerous lesions using smartphone images. | Results: moderate nurse-expert agreement, kappa 0.45. Comment: appropriately trained nurses can reliably conduct screening. Real-time expert feedback might improve reporting. |
| Asgary et al., 2016 [33] | Ghana 25–45 y n = 169 HPV status = NR | Providers completed a 2-week on-site training in VIA, followed by a 3-month VIA training supported by text messaging by an expert reviewer (real-time feedback). Comparison of agreement rates for VIA+. | Results: total agreement rate, 95%, average agreement rate between each provider and expert reviewer 89.6%. Kappa 0.67 |
| Peterson et al., 2016 [34] | Kenya Age = NR n = 824 HPV status = NR | Training of providers using pictures taken. Decision support “Job Aid tool” included in the mobile application (MobileODT system) for diagnosis and treatment. | Results: 12.6% pre-cancerous lesions, 0.7% suspected cancer. Comment: deployment of the “EVA System” allows monitoring of clinical decisions made by nurses. Help of “Job Aid” decision support for treatment and gives more confidence to providers. |
| Yeates et al., 2016 [26] | Tanzania 25–49 y n = 1072 HPV status = NR | Training providers to perform D-VIA with real-time support from regional experts, images sent through a smartphone application. | Feasibility of smartphone camera to perform “Enhanced VIA” and level of agreement between trainee and expert over time (agreement 96.8%), Response timing (real-time), 1–5 min 48.4% and <10 min 60% of the time. |
| Studies | Population | Objective | Device | Intervention | Results |
|---|---|---|---|---|---|
| Kudva et al., 2018 [44] | India >24 y n = 102 | Develop a decision support system for cervical cancer screening with an inbuilt image processing algorithm. | Android device with a camera of 13 Mpx. | 102 images Reference = expert evaluation. | Accuracy 97.9%, Se 99.0%, Sp 97.1%, AUC NR. |
| Bae et al., 2020 [45] | South Korea, >20 y n = 20 | Develop a new cervical cancer screening technique and implement a machine-learning algorithm using images taken during VIA with a smartphone-based endoscope. | Smartphone-based endoscope. | 40 images (2 per patient). Expert evaluation vs AI. Reference = histopathology. | Accuracy 78.3%, Se 75.8%, Sp 80.3%, AUC 0.805. Clinicians’ mean accuracy 77.5%, Se 62.5%, Sp 100%, AUC NR. |
| Xue Z. et al., 2020 [43] | Various countries >18 y n = 3221 | Evaluate accuracy of automated visual evaluation (AVE) on smartphone images. | MobileODT system (smartphone with lens). | 7587 images. Reference = expert evaluation | Accuracy NR, Se NR, Sp NR, AUC 0.87 (95% CI 0.81–0.92). |
| Viñals et al., 2021 [46] | Cameroon, Switzerland 30–49 y n = 44 | Development of a smartphone-based algorithm to detect cervical precancer from the dynamic features (dynamics of aceto-whitening). | Samsung Galaxy S5 | 44 dynamic images; Expert evaluation vs. AI. Reference = histology | AI accuracy 89%, Se 90%, Sp 87%, AUC NR. Clinicians’ mean accuracy 71%, Se 68%, Sp 78%, AUC NR. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sami, J.; Lemoupa Makajio, S.; Jeannot, E.; Kenfack, B.; Viñals, R.; Vassilakos, P.; Petignat, P. Smartphone-Based Visual Inspection with Acetic Acid: An Innovative Tool to Improve Cervical Cancer Screening in Low-Resource Setting. Healthcare 2022, 10, 391. https://doi.org/10.3390/healthcare10020391
Sami J, Lemoupa Makajio S, Jeannot E, Kenfack B, Viñals R, Vassilakos P, Petignat P. Smartphone-Based Visual Inspection with Acetic Acid: An Innovative Tool to Improve Cervical Cancer Screening in Low-Resource Setting. Healthcare. 2022; 10(2):391. https://doi.org/10.3390/healthcare10020391
Chicago/Turabian StyleSami, Jana, Sophie Lemoupa Makajio, Emilien Jeannot, Bruno Kenfack, Roser Viñals, Pierre Vassilakos, and Patrick Petignat. 2022. "Smartphone-Based Visual Inspection with Acetic Acid: An Innovative Tool to Improve Cervical Cancer Screening in Low-Resource Setting" Healthcare 10, no. 2: 391. https://doi.org/10.3390/healthcare10020391