
Common Pregnancy Complaints Can Lead to Motor Vehicle Collisions or Near-Miss Incidents


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
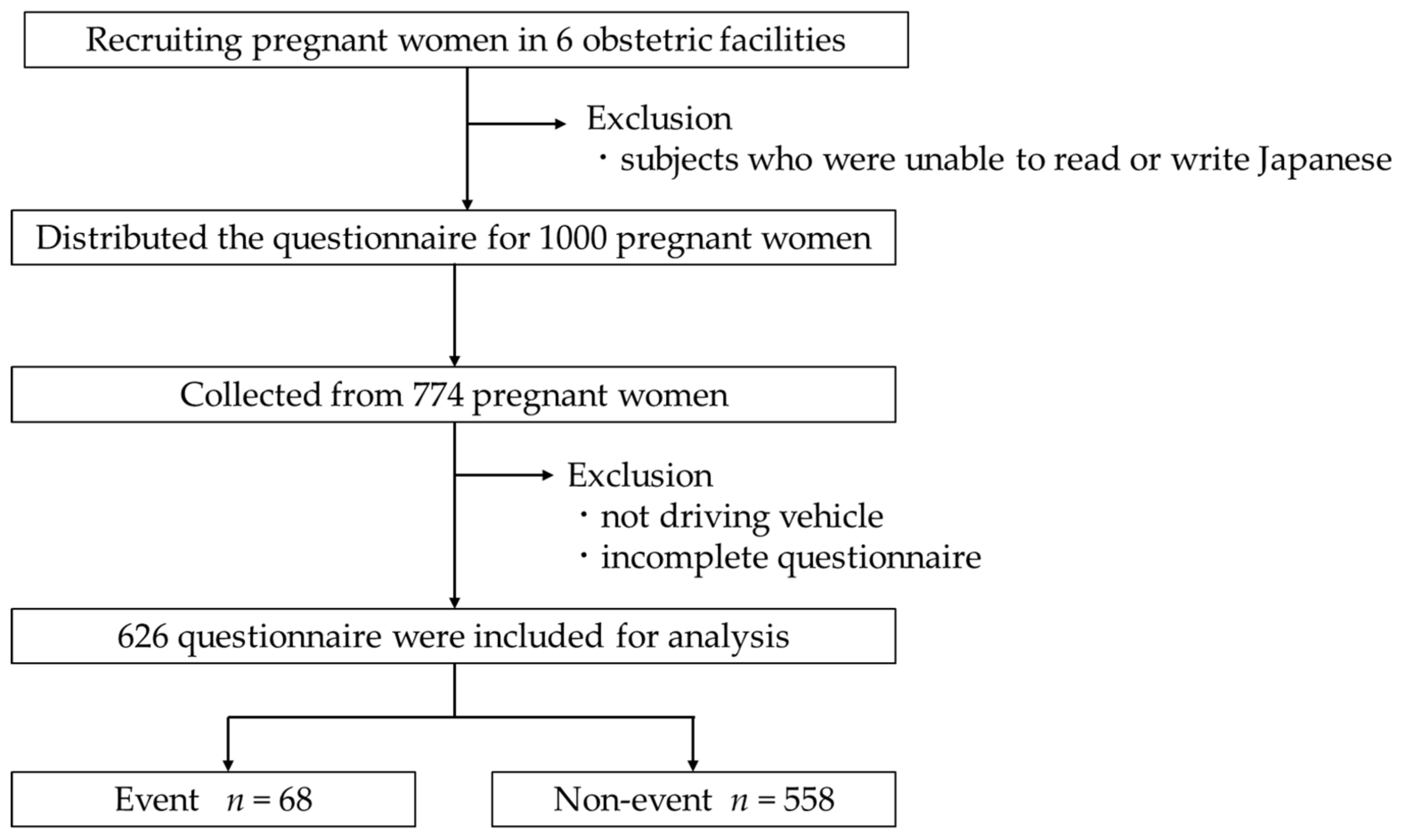
2.2. Study Participants

2.3. Survey
2.4. Questionnaire Items
- (1)
- Participant characteristics including age, height, weight, and body mass index (BMI).
- (2)
- Information about pregnancy: primipara or multipara, and gestational age.
- (3)
- Driving history.
- (4)
- Experience of an MVC or near-miss incident during pregnancy.
- (5)
- Frequency of common complaints in pregnancy. We asked participants to report their awareness of the following 18 items using a four-point scale (nothing: 1, almost none: 2, occasionally: 3, always: 4): compression of the stomach or abdomen; nausea; frequent urination; tension and cramps in the lower abdomen; taut or tingling breasts; stiff shoulder; pelvic pain; back or lower back pain; fatigue and cramp in the lower limbs; whole body malaise; strong drowsiness; irritability; depressed mood; distractedness; feeling of weakness; palpitations; hot flashes; itching.
2.5. Statistical Analysis
3. Results
3.1. Basic Subject Details
3.2. Comparison of the Frequency of Each Common Complaint in Pregnancy between the Two Groups
3.3. Relationship between Event Experiences and Common Complaints in Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. Department of Economic and Social Affairs Sustainable Development. Available online: https://sdgs.un.org/goals (accessed on 15 June 2021).
- Oda, S.; Inoue, K.; Sakakibara, T.; Nito, M.; Hasegawa, Y.; Mori, K.; Ibe, T.; Imamura, H.; Sakane, H.; Tsutsumi, S.; et al. Chapter 2 Demography. In Trends in National Health, Positive Indicators of Health and Welfare, 2nd ed.; Oda, S., Inoue, K., Sakakibara, T., Nito, M., Hasegawa, Y., Mori, K., Ibe, T., Imamura, H., Sakane, H., Tsutsumi, S., et al., Eds.; Japan Association for Health, Labour and Welfare Statistics: Tokyo, Japan, 2020; Volume 67, pp. 55–59. [Google Scholar]
- Redelmeier, D.A.; May, S.C.; Thiruchelvam, D.; Barrett, J.F. Pregnancy and the risk of a traffic crash. Can. Med. Assoc. J. 2014, 186, 742–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozawa, T.; Hagiwara, Y.; Kurosaki, M.; Teramoto, C.; Tanaka, G.; Ishikawa, K.; Morishima, M.; Watanabe, H. Traffic accidents involving pregnant women and seat belt use. Experience of three cases of traffic accidents involving pregnant women and a questionnaire survey of pregnant women. J. Jpn. Soc. Neonatol. 1996, 32, 204–207. (In Japanese) [Google Scholar]
- Hitosugi, M.; Kawato, H.; Udagawa, H.; Tokudome, S. Measures to improve the comfort of pregnant car occupants -A survey analysis of pregnant car drivers. J. Jpn. Soc. Occup. Disaster Med. 2011, 59, 85–89. (In Japanese) [Google Scholar]
- Morikawa, M.; Yamada, T.; Kato-Hirayama, E.; Nishikawa, A.; Watari, M.; Maeda, N.; Kogo, H.; Minakami, H. Seatbelt use and seat preference among pregnant women in Sapporo, Japan, in 2013. J. Obstet. Gynaecol. Res. 2016, 42, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Baba, M.; Miyama, G.; Sugiyama, D.; Hitosugi, M. Influence of workplace environment, working conditions and health status of taxi drivers on vehicle collisions or near-miss events. Ind. Health 2019, 57, 530–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chibber, R.; AI-Harmi, J.; Fouda, M.; EI-Saleh, E. Motor-vehicle injury in pregnancy and subsequent feto-maternal outcomes: Of grave concern. J. Matern.-Fetal Neonatal Med. 2015, 28, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, T.M. Nausea and vomiting of pregnancy: An obstetric syndrome. Am. J. Obstet. Gynecol. 2002, 186, S184–S189. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Dashe, J.S.; Hoffman, B.L.; Casey, B.M.; Spong, C.Y. (Eds.) Prenatal care. In Williams Obstetrics, 25th ed.; Mc Graw Hill: New York, NY, USA, 2018; pp. 157–179. [Google Scholar]
- Hall, H.; Cramer, H.; Sundberg, T.; Ward, L.; Adams, J.; Moore, C.; Sibbritt, D.; Lauche, R. The effectiveness of complementary manual therapies for pregnancy-related back and pelvic pain A systematic review with meta-analysis. Medicine 2016, 95, e4723. [Google Scholar] [CrossRef] [PubMed]
- Brunton, R.; Simpson, N.; Dryer, R. Pregnancy-related anxiety, perceived parental self-efficacy and the influence of parity and age. Int. J. Environ. Res. Public Health 2020, 17, 6709. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Dashe, J.S.; Hoffman, B.L.; Casey, B.M.; Spong, C.Y. (Eds.) Maternal physiology. In Williams Obstetrics, 25th ed.; Mc Graw Hill: New York, NY, USA, 2018; pp. 49–78. [Google Scholar]
- Chai, J.; Qu, W.; Sun, X.; Zhang, K.; Ge, Y. Negativity bias in dangerous drivers. PLoS ONE 2016, 11, e0147083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, S.; Hitosug, M.; Moriguchi, S.; Baba, M.; Tsujimura, S.; Takeda, A.; Takaso, M.; Nakamura, M. Comparison of motor vehicle collision injuries between pregnant and non-pregnant women: A nationwide collision data-based study. Healthcare 2021, 9, 1414. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total n = 626 | Event Group n = 68 | Non-Event Group n = 558 | p Value | ||
|---|---|---|---|---|---|
| Age (years) | Median (IQR) | 31.0 (28.0–35.0) | 32.0 (29.0–35.0) | 31.0 (28.0–35.0) | 0.599 |
| Min–Max | 18–44 | 22–41 | 18–44 | ||
| Height (cm) | Median (IQR) | 159.0 (155.0–162.0) | 158.0 (155.0–162.0) | 159.0 (155.0–162.0) | 0.628 |
| Min–Max | 140.0–180.0 | 140.0–180.0 | 143.0–172.0 | ||
| Weight before pregnancy (kg) | Median (IQR) | 51.0 (48.0–56.0) | 51.5 (47.0–57.0) | 51.0 (48.0–56.0) | 0.977 |
| Min–Max | 34.0–90.0 | 38.0–90.0 | 34.0–85.0 | ||
| Current weight (kg) | Median (IQR) | 56.1 (51.7–62.0) | 56.2 (51.0–63.0) | 56.0 (52.0–62.0) | 0.862 |
| Min–Max | 34.0–88.0 | 44.5–82.0 | 34.0–88.0 | ||
| BMI before pregnancy | Median (IQR) | 20.3 (19.0–22.2) | 20.6 (19.4–22.4) | 20.3 (18.9–22.1) | 0.516 |
| Min–Max | 14.0–37.0 | 16.4–37.0 | 14.0–33.2 | ||
| Gestational age (weeks) | Median (IQR) | 27.0 (20.0–33.0) | 29.0 (20.5–35.0) | 27.0 (20.0–33.0) | 0.111 |
| Min–Max | 6–41 | 6–40 | 7–41 | ||
| Driving history (years) | Median (IQR) | 11.0 (7.0–15.0) | 12.0 (7.5–14.0) | 11.0 (7.0–15.0) | 0.740 |
| Min–Max | 1–26 | 1–20 | 1–26 |
| Complaint | Frequency | Event n = 68 | % | Non-Event n = 558 | % | p Value |
|---|---|---|---|---|---|---|
| Compression of the stomach or abdomen | Low | 7 | 10.3 | 128 | 22.9 | 0.017 |
| High | 61 | 89.7 | 430 | 77.1 | ||
| Nausea | Low | 35 | 51.5 | 348 | 62.4 | 0.082 |
| High | 33 | 48.5 | 210 | 37.6 | ||
| Frequent urination | Low | 2 | 2.9 | 47 | 8.4 | 0.112 |
| High | 66 | 97.1 | 511 | 91.6 | ||
| Tension and cramps in the lower abdomen | Low | 10 | 14.7 | 173 | 31.0 | 0.005 |
| High | 58 | 85.3 | 385 | 69.0 | ||
| Taut or tingling breasts | Low | 35 | 51.5 | 317 | 56.8 | 0.402 |
| High | 33 | 48.5 | 241 | 43.2 | ||
| Stiff shoulder | Low | 23 | 33.8 | 230 | 41.2 | 0.241 |
| High | 45 | 66.2 | 328 | 58.8 | ||
| Pelvic pain | Low | 33 | 48.5 | 343 | 61.5 | 0.040 |
| High | 35 | 51.5 | 215 | 38.5 | ||
| Back or lower back pain | Low | 15 | 22.1 | 165 | 29.6 | 0.196 |
| High | 53 | 77.9 | 393 | 70.4 | ||
| Fatigue and cramp in the lower limbs | Low | 22 | 32.4 | 228 | 40.9 | 0.176 |
| High | 46 | 67.6 | 330 | 59.1 | ||
| Whole-body malaise | Low | 17 | 25.0 | 168 | 30.1 | 0.383 |
| High | 51 | 75.0 | 390 | 69.9 | ||
| Strong drowsiness | Low | 10 | 14.7 | 127 | 22.8 | 0.129 |
| High | 58 | 85.3 | 431 | 77.2 | ||
| Irritability | Low | 25 | 36.8 | 304 | 54.5 | 0.006 |
| High | 43 | 63.2 | 254 | 45.5 | ||
| Depressed mood | Low | 36 | 52.9 | 392 | 70.3 | 0.004 |
| High | 32 | 47.1 | 166 | 29.7 | ||
| Distractedness | Low | 24 | 35.3 | 309 | 55.4 | 0.002 |
| High | 44 | 64.7 | 249 | 44.6 | ||
| Feeling of weakness | Low | 39 | 57.4 | 352 | 63.1 | 0.357 |
| High | 29 | 42.6 | 206 | 36.9 | ||
| Palpitations | Low | 25 | 36.8 | 239 | 42.8 | 0.339 |
| High | 43 | 63.2 | 319 | 57.2 | ||
| Hot flashes | Low | 30 | 44.1 | 313 | 56.1 | 0.061 |
| High | 38 | 55.9 | 245 | 43.9 | ||
| Itching | Low | 38 | 55.9 | 347 | 62.2 | 0.313 |
| High | 30 | 44.1 | 211 | 37.8 |
| Complaints | Odds Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Tension and cramps in the lower abdomen | 2.414 | 1.198–4.868 | 0.014 |
| Distractedness | 1.849 | 1.072–3.189 | 0.027 |
| Irritability | 1.746 | 1.018–2.997 | 0.043 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsuchikawa, S.; Hanahara, K.; Tateoka, Y.; Hitosugi, M. Common Pregnancy Complaints Can Lead to Motor Vehicle Collisions or Near-Miss Incidents. Healthcare 2022, 10, 279. https://doi.org/10.3390/healthcare10020279
Tsuchikawa S, Hanahara K, Tateoka Y, Hitosugi M. Common Pregnancy Complaints Can Lead to Motor Vehicle Collisions or Near-Miss Incidents. Healthcare. 2022; 10(2):279. https://doi.org/10.3390/healthcare10020279
Chicago/Turabian StyleTsuchikawa, Sachi, Kyoko Hanahara, Yumiko Tateoka, and Masahito Hitosugi. 2022. "Common Pregnancy Complaints Can Lead to Motor Vehicle Collisions or Near-Miss Incidents" Healthcare 10, no. 2: 279. https://doi.org/10.3390/healthcare10020279