
Innovative Nutrition Education: A Color-Coded Tool for Individuals with Low Literacy Level

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
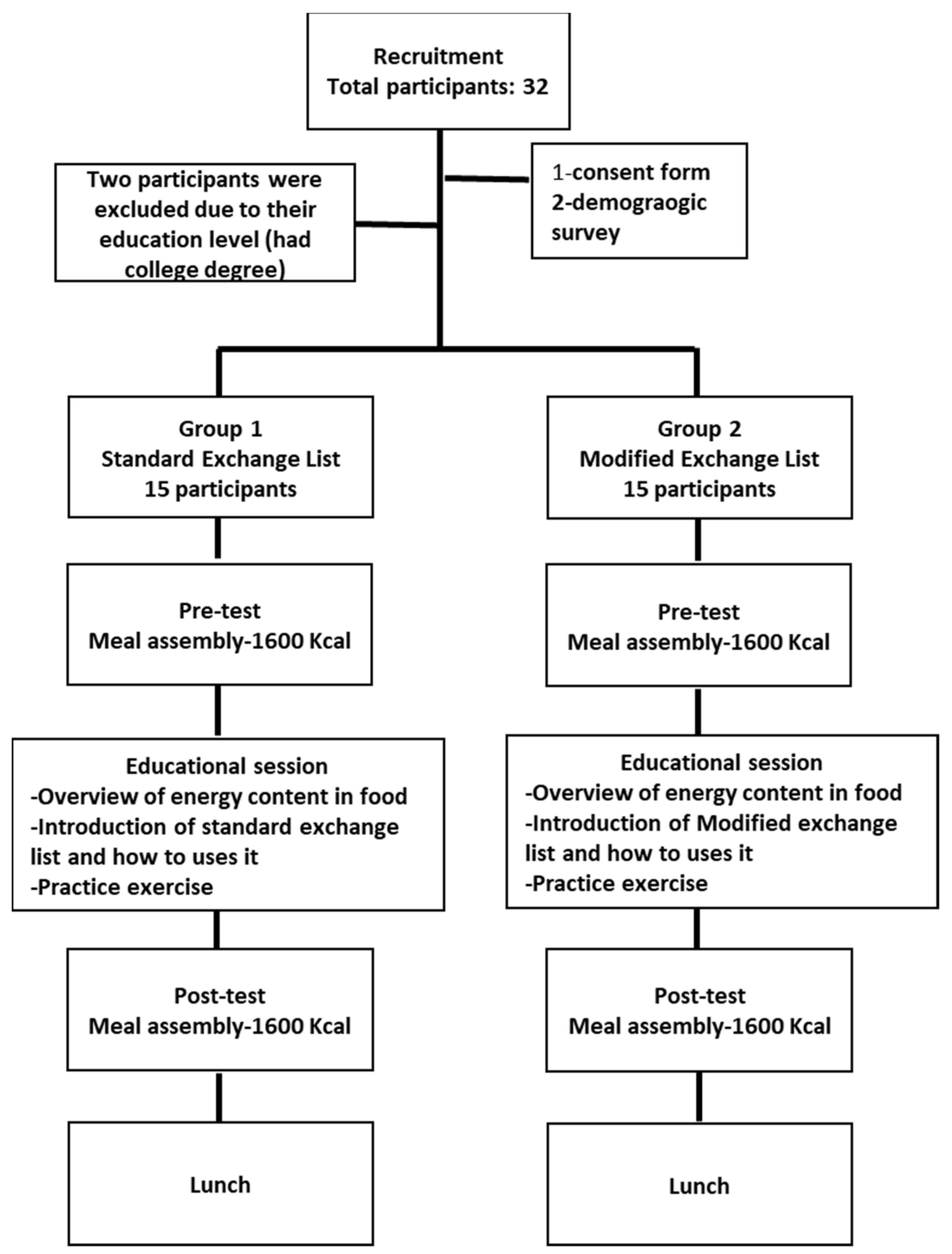
2.1. Study Participants
2.2. Intervention
2.2.1. Meal-Planning Training Using Standard Exchange Lists
2.2.2. Meal-Planning Training Using Modified Exchange Lists
2.2.3. Post-Test
2.3. Statistical Analysis
3. Results
4. Discussion
5. Limitations
Implications for Research and Practice
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kones, R.; Rumana, U. Cardiometabolic diseases of civilization: History and maturation of an evolving global threat: An update and call to action. Ann. Med. 2016, 49, 260–274. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 22 July 2020).
- Kelly, J.T.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.J.; Campbell, K.L.; Strippoli, G.F. Healthy Dietary Patterns and Risk of Mortality and ESRD in CKD: A Meta-Analysis of Cohort Studies. Clin. J. Am. Soc. Nephrol. 2016, 12, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Choose Your Foods: Food List for Diabetes; American Diabetes Association and Academy of Nutrition and Dietetics: Cleveland, OH, USA, 2014.
- Weeler, M.L.; Franz, M.; Barrier, F.; Holler, H.; Cronmiller, N.; Delahanty, L.M. Macronutriants and Energy Database for the 1995 Exchang Lists for Meal Planning: A Rational for Clinical Practice Decisions. J. Am. Diet. Soc. 1996, 96, 1167–1171. [Google Scholar] [CrossRef]
- Bawadi, H.A.; Naseem, M.; Al-Shwaiyat, R.F.; Tayyem, R.M.; Georgianna, T. Developing a food exchange list for Middle Eastern appetizers and desserts commonly consumed in Jordan. Nutr. Diet. 2009, 66, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.N.; Kalsoom, S.; Khan, A.A. Food exchange list and dietary management of non-communicable diseases in cultural perspective. Pak. J. Med. Sci. 2017, 33, 1273. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.C.A. Exchange list: A systematic review with emphasis on history and development of a meal-planning exchange list with cultural relevance. Eur. Int. J. Sci. Technol. 2017, 6, 6. [Google Scholar]
- Wheeler, M.L.; Daly, A.; Evert, A.; Franz, M.J.; Geil, P.; Holzmeister, L.A.; Kulkarni, K.; Loghmani, E.; Ross, T.A.; Woolf, P. Choose your foods: Exchange lists for diabetes, 2008: Description and guidelines for use. J. Am. Diet. Assoc. 2008, 108, 883–888. [Google Scholar] [CrossRef]
- Kendall, P.A.; Jason, G.R. Educating Patients with Diabetes: Comparison of Nutrient-based and Exchange Group Methods. J. Acad. Nutr. Diet. 1990, 90, 238. [Google Scholar] [CrossRef]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes: A systematic review of the literature. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Malloy-Weir, L.; Cooper, M. Health literacy, literacy, numeracy and nutrition label understanding and use: A scoping review of the literature. J. Hum. Nutr. Diet. 2016, 30, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Simply Put: A Guide for Creating Easy-to-Understand Materials [Booklet]; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2009.
- Bes-Rastrollo, M.; Sanchez-Villegas, A.; Gomez-Gracia, E.; Martinez, J.A.; Pajares, R.M.; Martinez-Gonzalez, M.A. Predictors of weight gain in a Mediterranean cohort: The Seguimiento Universidad de Navarra Study. Am. J. Clin. Nutr. 2006, 83, 362–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishida, C.; Uauy, R.; Kumanyika, S.; Shetty, P. The Joint WHO/FAO Expert Consultation on diet, nutrition and the prevention of chronic diseases: Process, product and policy implications. Public Health Nutr. 2004, 7, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations Office for the Coordination of Humantirian Affairs. Qatar|OCHA. Available online: https://www.unocha.org/middle-east-and-north-africa-romena/qataraheadofprint] (accessed on 18 June 2020).
- Migration Data Portal. Data on Migration and Health. Available online: https://migrationdataportal.org/themes/migration-and-health (accessed on 20 June 2020).
- Ang, J.W.; Chia, C.; Koh, C.J.; Chua, B.W.B.; Narayanaswamy, S.; Wijaya, L.; Chan, L.G.; Goh, W.L.; Vasoo, S. Healthcare-seeking behaviour, barriers and mental health of non-domestic migrant workers in Singapore. BMJ Glob. Health 2017, 2, e000213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Development, Planning, and Statistics. Measuring the Standard of Living in Qatar using Household Expenditure and Income Survey 2012/2013. 2015. Available online: https://www.psa.gov.qa/en/knowledge/ReportsandStudies/SolEn.pdf (accessed on 1 March 2016).
- The Healthy Eating Index; Center for Nutrition Policy and Promotion, US Department of Agriculture: Washington, DC, USA, 1995.
- Weinstein, S.J.; Vogt, T.M.; Gerrior, S.A. Healthy eating index scores are associated with blood nutrient concentrations in the third National Health and Nutrition Examination Survey. J. Am. Diet. Assoc. 2004, 104, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Speirs, K.E.; Messina, L.A.; Munger, A.L.; Grutzmacher, S.K. Health Literacy and Nutrition Behaviors among Low-Income Adults. J. Health Care Poor Underserved 2012, 23, 1082–1091. [Google Scholar] [CrossRef] [PubMed]
- Wolff, K.; Cavanaugh, K.; Malone, R.; Hawk, V.; Gregory, B.P.; Davis, D.; Wallston, K.; Rothman, R.L. The diabetes literacy and numeracy education toolkit (DLNET) materials to facilitate diabetes education and management in patients with low literacy and numeracy skills. Diabetes Educ. 2009, 35, 233–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nath, C. Literacy and Diabetes Self-Management: Low Literacy Affects Outcomes; Communication Is Key. Am. J. Nurs. 2016, 107, 43–49. Available online: http://0-www.jstor.org.mylibrary.qu.edu.qa/stable/40384539 (accessed on 1 March 2016). [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Standard | Modified | p-Value | |
|---|---|---|---|
| Age * | 31.1 ± 1.6 | 29.9 ± 1.1 | 0.4 † |
| Education ‡ | |||
| Primary | 3 (20) | 7 | 0.09 § |
| Middle | 2 (13.3) | 4 | |
| High | 10 (66.7) | 4 | |
| Income ‡ | |||
| 500–999 | 10 | 13 | 0.2 § |
| 1000–1499 | 5 | 2 | |
| Disease Status ‡ | |||
| Diseased | 4 | 5 | 0.7 § |
| Not Diseased | 11 | 10 | |
| Dietary Recommendations † | Pre-Intervention | p-Value | Post Intervention | p-Value | ||
|---|---|---|---|---|---|---|
| Standard | Modified | Standard | Modified | |||
| Frui t ≥ 1.6 cup | 9 (60) | 13 (86.6) | 0.1 | 10 (66.6) | 15 (100) | 0.02 |
| Protein ≥ 4.4 oz | 5 (33.3) | 7 (46.7) | 0.355 | 4 (26.7) | 10 (66.7) | 0.033 |
| Whole Grain > 2.4 oz | 0 (0) | 0 (0) | __ | 0 (0) | 0 (0) | __ |
| Refined Grain < 2.4 oz | 1 (6.6) | 2 (13.3) | 0.5 | 1 (6.6) | 4 (26.6) | 0.165 |
| Vegetables ≥ 2 cup | 4 (26.6) | 3 (20) | 0.5 | 5 (33.3) | 9 (60) | 0.1 |
| Dairy ≥ 2.4 cup | 1 (6.6) | 2 (13.3) | 0.5 | 0 (0) | 11 (73.3) | <0.001 |
| Saturated Fat < 10% | 11 (73.3) | 10 (66.6) | 0.5 | 10 (66.6) | 12 (80) | 0.3 |
| Total Calories 1520–1680 kcal | 2 (13.3) | 2 (13.3) | 0.701 | 1 (6.6) | 15 (100) | <0.001 |
| CHO 45–65% | 7 (46.6) | 9 (60) | 0.5 | 7 (46.6) | 12 (80) | <0.001 |
| Protein V | 15 (100) | 14 (93.3) | 0.5 | 15 (100) | 15 (100) | __ |
| Fat 20–35% | 7 (46.6) | 10 (66.6) | 0.231 | 9 (60) | 12 (80) | 0.213 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bawadi, H.; Al-Jayyousi, G.F.; Shabana, H.; Boutefnouchet, S.; Eljazzar, S.; Ismail, S. Innovative Nutrition Education: A Color-Coded Tool for Individuals with Low Literacy Level. Healthcare 2022, 10, 272. https://doi.org/10.3390/healthcare10020272
Bawadi H, Al-Jayyousi GF, Shabana H, Boutefnouchet S, Eljazzar S, Ismail S. Innovative Nutrition Education: A Color-Coded Tool for Individuals with Low Literacy Level. Healthcare. 2022; 10(2):272. https://doi.org/10.3390/healthcare10020272
Chicago/Turabian StyleBawadi, Hiba, Ghadir Fakhri Al-Jayyousi, Hala Shabana, Sana Boutefnouchet, Sereen Eljazzar, and Shrooq Ismail. 2022. "Innovative Nutrition Education: A Color-Coded Tool for Individuals with Low Literacy Level" Healthcare 10, no. 2: 272. https://doi.org/10.3390/healthcare10020272