
Burnout Syndrome among Staff at an Emergency Department during the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Instrument
3. Results
3.1. Sample Characteristics
3.2. Preliminary Analysis
3.3. Differences between the Professional Categories concerning Burnout Manifestations
3.4. Associations among the Study Variables
3.5. Gender Differences concerning Burnout Dimensions
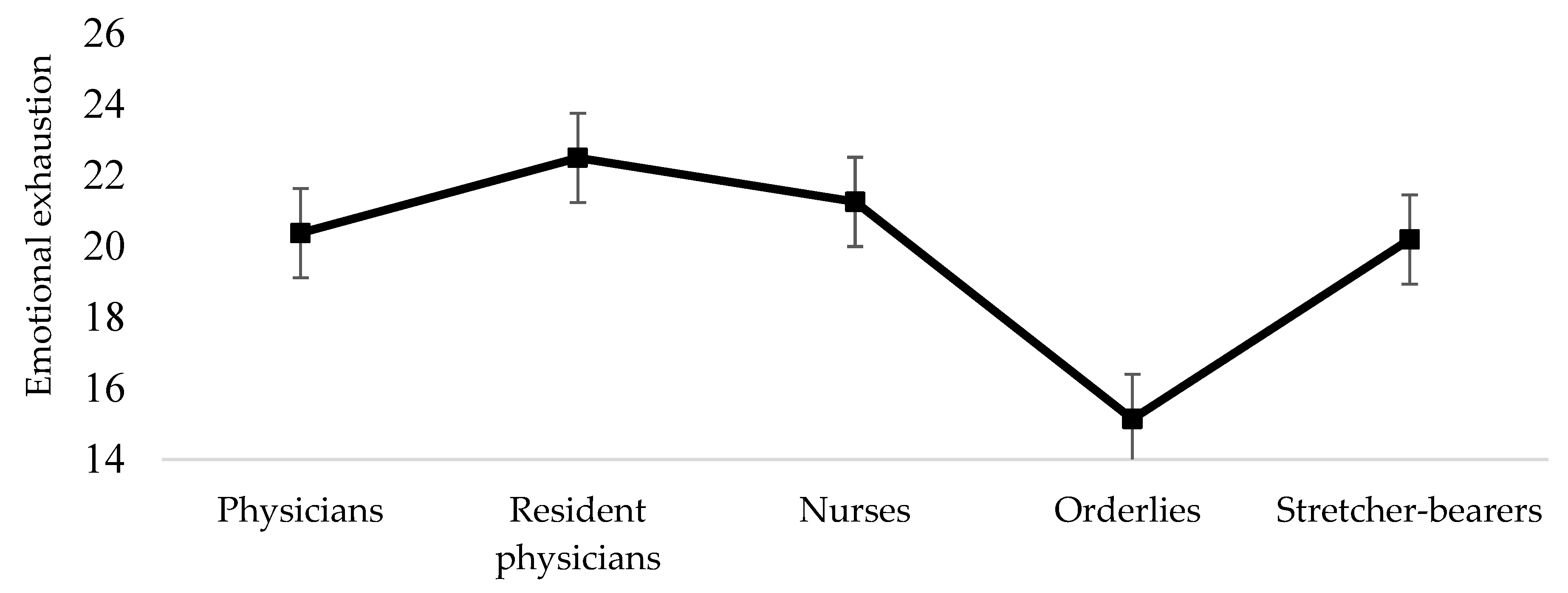
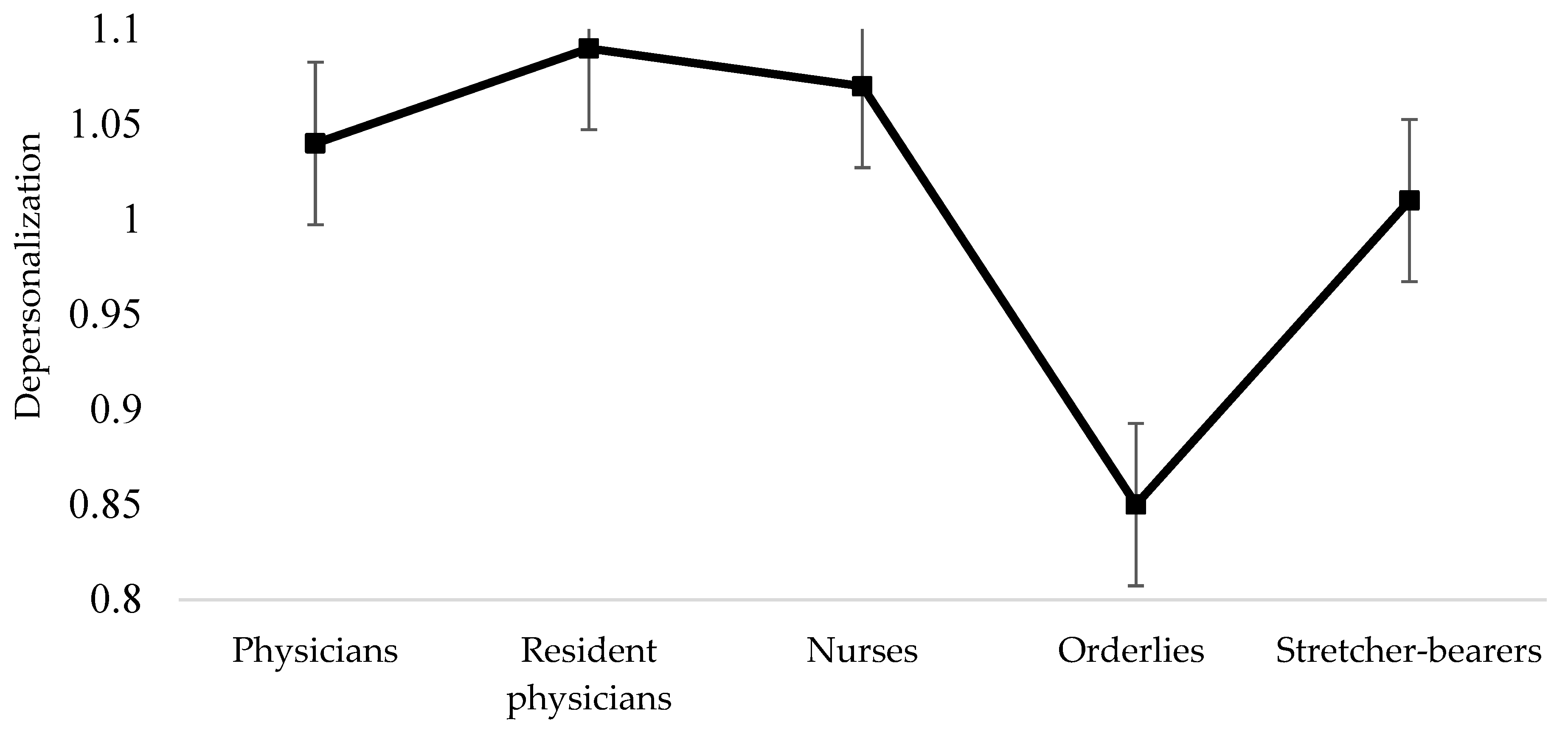
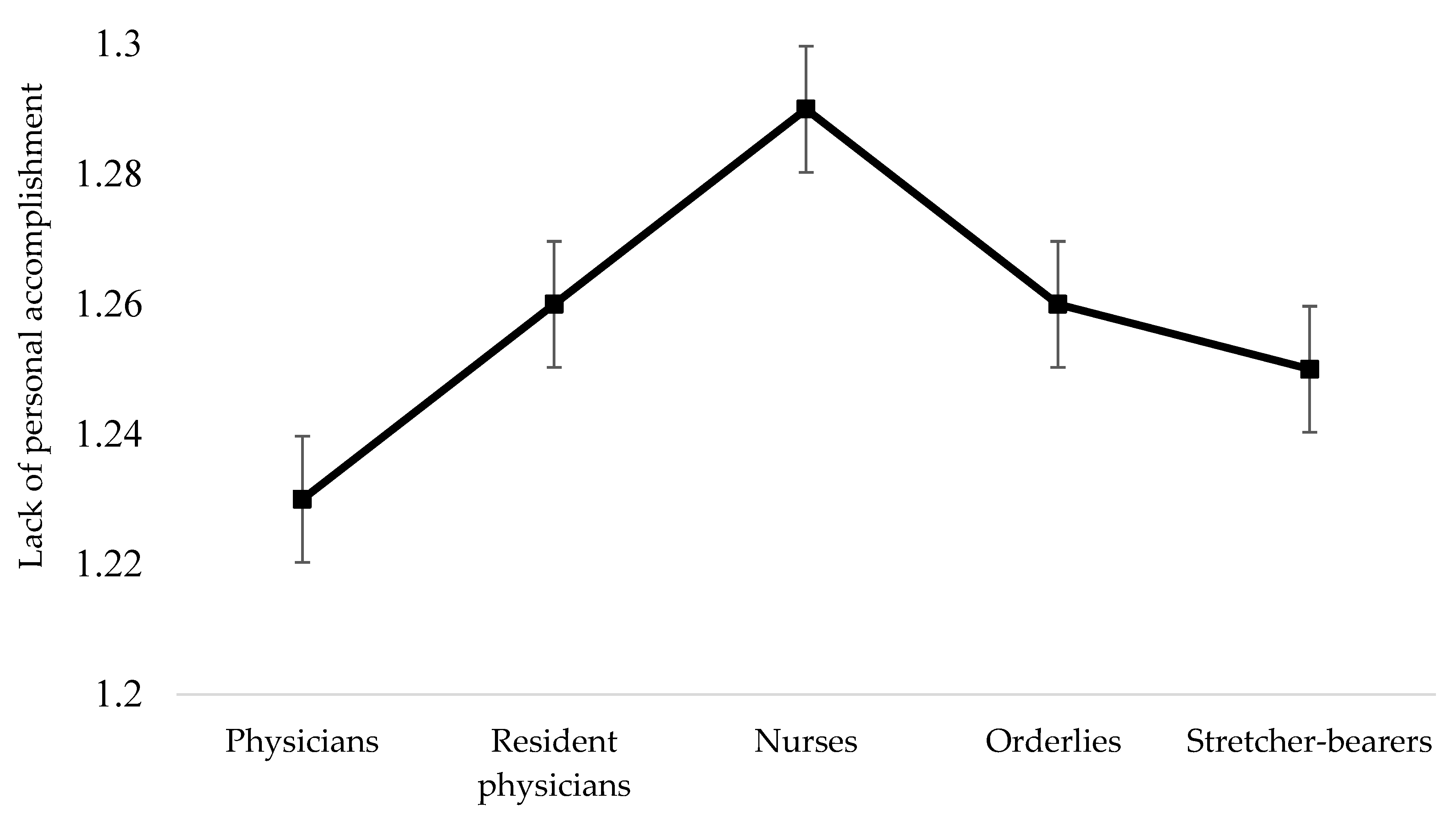
3.6. Differences among the Professional Categories concerning Burnout Dimensions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological adjustment of healthcare workers in Italy during the COVID-19 pandemic: Differences in stress, anxiety, depression, burnout, secondary trauma, and compassion satisfaction between frontline and non-frontline professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef] [PubMed]
- Dixon, E.; Murphy, M.; Wynne, R. A multidisciplinary, cross-sectional survey of burnout and wellbeing in emergency department staff during COVID-19. Australas. Emerg. Care 2022, (in press). [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.; Sullivan, V.; Weatherspoon, D.; Frazer, C. Comparison of Nurse Burnout, before and during the COVID-19 Pandemic. Nurs. Clin. N. Am. 2021, (in press). [Google Scholar] [CrossRef]
- Stehman, C.; Testo, Z.; Gershaw, R.; Kellogg, A. Burnout, Drop Out. West J. Emerg. Med. 2019, 20, 485–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyneel, A.; Smith, P.; Tack, J.; Pirson, M. Prevalence of burnout risk and factors associated with burnout risk among ICU nurses during the COVID-19 outbreak in French speaking Belgium. Intensive Crit. Care Nurs. 2021, 65, 103059. [Google Scholar] [CrossRef] [PubMed]
- Dimitriu, M.; Pantea-Stoian, A.; Smaranda, A.C.; Nica, A.A.; Carap, A.C.; Constantin, V.D.; Davitoiu, A.M.; Cirstoveanu, C.; Bacalbasa, N.; Bratu, O.G.; et al. Burnout syndrome in Romanian medical residents in time of the COVID-19 pandemic. Med. Hypotheses 2020, 144, 109972. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, M.A.; Sarwar, H. The Impact of COVID-19 on the Mental Health of Healthcare Professionals. J. Coll. Physicians Surg. Pak. 2020, 30 (Suppl. 2), S83. [Google Scholar]
- Sykes, C.; Borthwick, C.; Baker, E. Mental health and wellbeing in the medical profession. BMJ 2020, 368, m1211. [Google Scholar]
- WebMD. Doctors Suicide Rate Highest of Any Profession. 2018. Available online: https://www.webmd.com/mental-health/news/20180508/doctors-suicide-rate-highest-ofany-profession#1 (accessed on 20 June 2021).
- Shiu, C.; Chen, W.T.; Hung, C.C.; Huang, E.P.C.; Lee, T.S.H. COVID-19 stigma associates with burnout among healthcare providers: Evidence from Taiwanese physicians and nurses. J. Formos. Med. Assoc. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The relationship between burnout, depression, and anxiety: A systematic review and meta-analysis. Front. Psychol. 2019, 10, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mǎirean, C.; Turliuc, M.N. Predictors of vicarious trauma beliefs among medical staff. J. Loss Trauma 2013, 18, 414–428. [Google Scholar] [CrossRef]
- Măirean, C. Secondary traumatic stress and posttraumatic growth: Social support as a moderator. Soc. Sci. J. 2016, 53, 14–21. [Google Scholar] [CrossRef]
- Costea, F.; Sălceanu, M.; Staicu, I.M.; Andreescu, A.G. Burnout syndrome in the Emergency Department of the Central Military Emergency Hospital before and during the COVID-19 pandemic. Rom. J. Mil. Med. 2020, 124, 22–28. [Google Scholar]
- Anderson, N.; Pio, F.; Jones, P.; Selak, V.; Tan, E.; Beck, S.; Hamilton, S.; Rogan, A.; Yates, K.; Sagarin, M.; et al. Facilitators, barriers and opportunities in workplace wellbeing: A national survey of emergency department staff. Int. Emerg. Nurs. 2021, 57, 101046. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Arbuckle, J.L. IBM SPSS Amos 20.0 [Computer Program]; IBM: New York, NY, USA, 2011. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Marsaglia, G.; Tsang, W.W.; Wang, J. Evaluating Kolmogorov’s distribution. J. Stat. Softw. 2003, 8, 1–4. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 2013. [Google Scholar]
- Măirean, C. Emotion regulation strategies, secondary traumatic stress, and compassion satisfaction in healthcare providers. J. Psychol. 2016, 150, 961–975. [Google Scholar] [CrossRef] [PubMed]
- Burns, B. Caring for colleagues through debriefing. Kai Tiaki Nurs. N. Z. 2016, 22, 12–42. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | n | % | M | SD |
|---|---|---|---|---|
| Age | 37.72 | 7.90 | ||
| Gender | ||||
| Female | 71 | 73.2 | ||
| Male | 26 | 26.8 | ||
| Profession | ||||
| Physicians | 18 | 18.6 | ||
| Residential physicians | 14 | 14.4 | ||
| Nurses | 46 | 47.4 | ||
| Orderlies | 7 | 7.2 | ||
| Stretcher-bearers | 10 | 10.3 | ||
| Registrars | 2 | 2.1 |
| Burnout Manifestations | Total Sample (%) n = 97 | Physicians (%) n = 18 | Resident Physicians (%) n = 14 | Nurses (%) n = 46 | Orderlies (%) n = 7 | Stretcher-Bearers (%) n = 10 |
|---|---|---|---|---|---|---|
| Emotionally drained | 11.4 | 16.7 | 21.4 | 8.7 | 0 | 10 |
| Used up | 30.9 | 33.4 | 42.9 | 34.8 | 0 | 20 |
| Fatigued in the morning | 21.6 | 22.2 | 28.5 | 26 | 0 | 10 |
| Overwhelmed | 5.2 | 0 | 14.2 | 4.4 | 0 | 10 |
| Impersonal ‘objects’ | 2 | 0 | 14.2 | 0 | 0 | 0 |
| Frustrated | 6.2 | 0 | 7.1 | 10.9 | 0 | 0 |
| Full of energy * | 17.5 | 11.2 | 21.4 | 19.5 | 14.3 | 20 |
| Right solution * | 3.1 | 0 | 0 | 4.3 | 14.3 | 0 |
| Depression | 6.2 | 0 | 14.3 | 8.7 | 0 | 0 |
| Positive influence * | 14.4 | 5.6 | 7.1 | 17.4 | 42.9 | 0 |
| More callous | 12.3 | 16.7 | 14.3 | 13.1 | 0 | 10 |
| Lack of interest | 5.1 | 5.6 | 7.1 | 4.3 | 0 | 10 |
| Plans for the future * | 9.3 | 0 | 0 | 15.2 | 0 | 10 |
| Professional disillusions | 7.2 | 5.6 | 0 | 13 | 0 | 0 |
| Indifference | 11.4 | 5.6 | 14.2 | 15.2 | 0 | 10 |
| Tense | 7.2 | 5.6 | 7.1 | 8.7 | 0 | 10 |
| Work indifference | 7.2 | 0 | 21.4 | 6.5 | 0 | 10 |
| Want to isolate | 15.5 | 11.2 | 21.4 | 21.8 | 0 | 0 |
| Benevolent atmosphere * | 9.3 | 0 | 7.1 | 15.2 | 0 | 10 |
| Communicate easily * | 6.2 | 0 | 7.1 | 4.4 | 14.3 | 20 |
| Manage to do a lot * | 6.2 | 0 | 7.1 | 4.4 | 14.3 | 20 |
| Power limit | 56.7 | 55.5 | 42.9 | 58.7 | 71.4 | 60 |
| Optimism for the future * | 72.2 | 77.8 | 92.9 | 67.4 | 42.9 | 70 |
| Bankrupt | 6.2 | 11.1 | 0 | 6.7 | 0 | 0 |
| Burden on my shoulders | 7.2 | 16.7 | 7.1 | 6.5 | 0 | 0 |
| Burnout Manifestations | Total Sample M (SD) | Physicians M (SD) | Resident Physicians M (SD) | Nurses M (SD) | Orderlies M (SD) | Stretcher-Bearers M (SD) |
|---|---|---|---|---|---|---|
| Emotionally drained | 2.18 | 2.22 | 2.71 | 2.13 | 1.57 | 2.10 |
| Used up | 2.83 | 2.72 | 3.21 | 3.00 | 1.42 | 2.70 |
| Fatigued in the morning | 2.53 | 2.77 | 2.78 | 2.54 | 1.85 | 2.10 |
| Overwhelmed | 1.94 | 2.11 | 2.57 | 1.89 | 1.14 | 1.60 |
| Impersonal ‘objects’ | 1.84 | 1.83 | 2.00 | 1.89 | 1.42 | 1.80 |
| Frustrated | 1.82 | 1.61 | 1.92 | 2.00 | 1.00 | 1.80 |
| Full of energy * | 2.49 | 2.27 | 2.64 | 2.65 | 2.14 | 2.20 |
| Right solution * | 2.26 | 2.05 | 2.14 | 2.28 | 3.14 | 2.10 |
| Depression | 1.65 | 1.27 | 1.92 | 1.82 | 1.00 | 1.80 |
| Positive influence * | 2.61 | 2.11 | 2.64 | 2.73 | 3.14 | 2.30 |
| More callous | 2.15 | 2.50 | 2.42 | 2.13 | 1.28 | 1.90 |
| Lack of interest | 1.89 | 1.61 | 2.00 | 2.02 | 1.00 | 2.30 |
| Plans for the future * | 2.05 | 1.66 | 1.64 | 2.32 | 1.71 | 2.10 |
| Professional disillusions | 1.89 | 1.83 | 1.85 | 2.06 | 1.28 | 1.70 |
| Indifference | 2.11 | 1.83 | 2.21 | 2.30 | 1.57 | 2.00 |
| Tense | 1.93 | 1.94 | 2.14 | 1.93 | 1.14 | 2.10 |
| Work indifference | 1.87 | 1.5 | 2.21 | 2.08 | 1.00 | 1.60 |
| Want to isolate | 2.27 | 2.22 | 2.78 | 2.46 | 1.28 | 1.60 |
| Benevolent atmosphere * | 2.34 | 2.27 | 2.28 | 2.50 | 1.71 | 2.20 |
| Communicate easily * | 2.01 | 1.77 | 1.92 | 2.04 | 2.00 | 2.30 |
| Manage to do a lot * | 2.11 | 1.66 | 2.21 | 1.27 | 2.57 | 2.30 |
| Power limit | 3.79 | 3.38 | 3.35 | 3.93 | 4.42 | 4.00 |
| Optimism for the future * | 3.71 | 3.71 | 4.35 | 3.73 | 1.17 | 3.60 |
| Bankrupt | 1.53 | 1.72 | 1.50 | 1.52 | 1.00 | 1.60 |
| Burden on my shoulders | 1.95 | 2.33 | 1.85 | 1.89 | 1.57 | 2.00 |
| Burnout Dimensions | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Emotional exhaustion | 1 | |||
| 2. Depersonalization | 0.76 * | 1 | ||
| 3. Personal accomplishment | 0.43 * | 0.34 * | 1 | |
| 4. Age | −0.09 | −0.09 | −0.10 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corlade-Andrei, M.; Măirean, C.; Nedelea, P.; Grigorași, G.; Cimpoeșu, D. Burnout Syndrome among Staff at an Emergency Department during the COVID-19 Pandemic. Healthcare 2022, 10, 258. https://doi.org/10.3390/healthcare10020258
Corlade-Andrei M, Măirean C, Nedelea P, Grigorași G, Cimpoeșu D. Burnout Syndrome among Staff at an Emergency Department during the COVID-19 Pandemic. Healthcare. 2022; 10(2):258. https://doi.org/10.3390/healthcare10020258
Chicago/Turabian StyleCorlade-Andrei, Mihaela, Cornelia Măirean, Paul Nedelea, Gabriela Grigorași, and Diana Cimpoeșu. 2022. "Burnout Syndrome among Staff at an Emergency Department during the COVID-19 Pandemic" Healthcare 10, no. 2: 258. https://doi.org/10.3390/healthcare10020258