
Information Flow and Data Gaps in COVID-19 Recording and Reporting at National and Provincial Levels in Indonesia

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
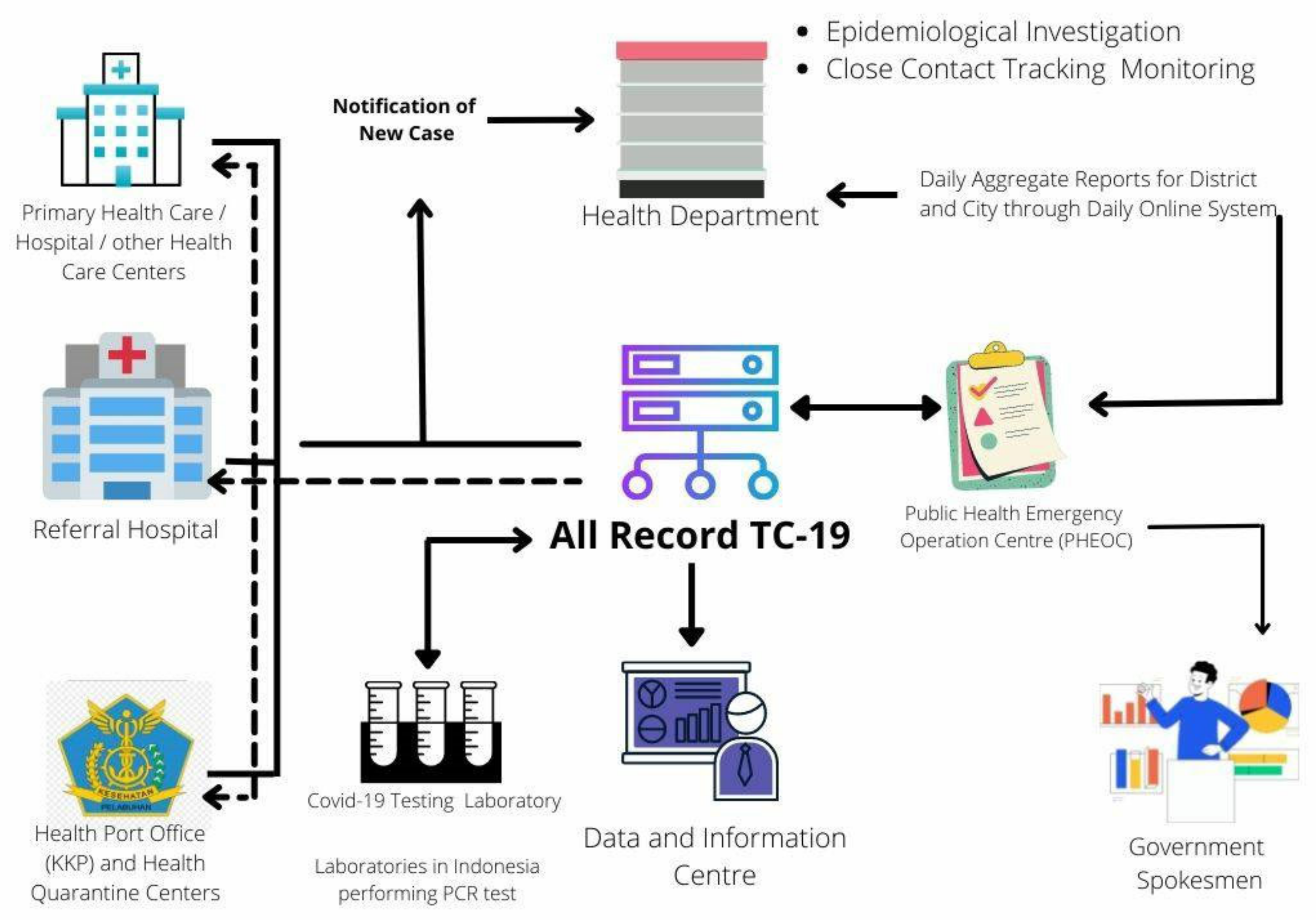
3.1. Information Flow of COVID-19 Recording and Reporting
3.1.1. Case Finding and Epidemiological Investigation Report
3.1.2. Aggregate Daily Reports
3.1.3. Processing and Analysis of Data
3.1.4. Data and Information Distribution
3.2. Comparison of Monitoring COVID-19 Incidence Data at Provincial and National Levels
4. Discussion
4.1. Finding of This Study
4.2. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zu, Z.Y.; Di Jiang, M.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancet, T. COVID-19: Fighting panic with information. Lancet 2020, 395, 537. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Gutierrez, B.; Mekaru, S.; Sewalk, K.; Goodwin, L.; Loskill, A.; Cohn, E.L.; Hswen, Y.; Hill, S.C.; Cobo, M.M.; et al. Epidemiological data from the COVID-19 outbreak, real-time case information. Sci. Data 2020, 7, 106. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, K.; Maher, J. Collecting Data. In The CDC Field Epidemiology Manual; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. [Google Scholar]
- Kazemi-Arpanahi, H.; Shanbehzadeh, M.; Mazhab-Jafari, K.; Haghiri, H. Coronavirus disease 2019 (COVID-19) surveillance system: Development of COVID-19 minimum data set and interoperable reporting framework. J. Educ. Health Promot. 2020, 9, 203. [Google Scholar] [CrossRef] [PubMed]
- Ågerfalk, P.J.; Conboy, K.; Myers, M.D. Information systems in the age of pandemics: COVID-19 and beyond. Eur. J. Inf. Syst. 2020, 29, 203–207. [Google Scholar] [CrossRef]
- Ibrahim, N.K. Epidemiologic surveillance for controlling COVID-19 pandemic: Types, challenges and implications. J. Infect. Public Health 2020, 13, 1630–1638. [Google Scholar] [CrossRef] [PubMed]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Arneson, D.; Elliott, M.; Mosenia, A.; Oskotsky, B.; Solodar, S.; Vashisht, R.; Zack, T.; Bleicher, P.; Butte, A.J.; Rudrapatna, V.A. COVIDCounties is an interactive real time tracker of the COVID19 pandemic at the level of US counties. Sci. Data 2020, 7, 405. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.; Susanto, H.; Kasim, M.F.; Nuraini, N.; Lestari, B.; Triany, D.; Widyastuti, W. Superspreading in early transmissions of COVID-19 in Indonesia. Sci. Rep. 2020, 10, 22386. [Google Scholar] [CrossRef] [PubMed]
- Satuan Tugas COVID-19. Peta Sebaran. Available online: https://covid19.go.id/peta-sebaran (accessed on 19 January 2021).
- Ministry of Health Republic of Indonesia. Guidelines For Prevention And Control Coronavirus Disease 2019 (COVID-19). In Number Hk.01.07/Menkes /413/2020; M.O.H.O.T.R.O. Editor: Jakarta, Indonesia, 2020. [Google Scholar]
- KawalCOVID-19. Kawal Informasi Seputar COVID-19 Secara Tepat Dan Akurat. 2021. Available online: https://datastudio.google.com/u/0/reporting/fda876a7-3eb2-4080-92e8-679c93d6d1bd/page/h6oVB (accessed on 7 July 2021).
- KawalCorona. Kawal Corona. 2021. Available online: https://kawalcorona.com/ (accessed on 7 July 2021).
- Ministry of Health. Peraturan Menteri Kesehatan Republik Indonesia Tentang Penyelenggaraan Surveilans Kesehatan; Ministry of Health: Jakarta, Indonesia, 2014.
- Ministry of Health. Keputusan Menteri Kesehatan Republik Indonesia Tentang Pedoman Pencegahan dan Pengendalian CORONA VIRUS DISEASE 2019 (COVID-19) Nomor HK.01.07/MENKES/413/2020. 2020. Available online: https://infeksiemerging.kemkes.go.id/download/KMK_No._HK.01.07-MENKES-413-2020_ttg_Pedoman_Pencegahan_dan_Pengendalian_COVID-19.pdf (accessed on 7 July 2021).
- Ministry of Health Republic of Indonesia. All Record TC-19. 2021. Available online: https://allrecord-tc19.kemkes.go.id (accessed on 19 January 2021).
- Pejabat Pengelola Informasi dan Dokumentasi Jakarta. Jakarta Tanggap COVID-19. Available online: https://corona.jakarta.go.id/id (accessed on 7 July 2021).
- Pusat Informasi & Koordinasi Provinsi Jawa Barat. Pusat Informasi dan Koordinati COVID-19. 2021. Available online: https://pikobar.jabarprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Jawa Tengah. Tanggap COVID-19 Provinsi Jawa Tengah. 2021. Available online: https://corona.jatengprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Jawa Timur. Jatim Tanggap COVID-19. 2021. Available online: http://infocovid19.jatimprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Sulawesi Selatan. Sulsel Tanggap COVID-19. 2021. Available online: https://covid19.sulselprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Kalimantan Timur. Kaltim Tanggap COVID-19. 2021. Available online: https://covid19.kaltimprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Riau. Riau Tanggap COVID-19. 2021. Available online: https://corona.riau.go.id (accessed on 7 July 2021).
- Tim IT Diskominfo Provinsi Sumatera Barat. Sumbar Tanggap Corona. 2021. Available online: https://corona.sumbarprov.go.id (accessed on 7 July 2021).
- Pemerintah Kota Tangerang. Data Situasi Virus Corona. 2021. Available online: https://covid19.tangerangkota.go.id (accessed on 7 July 2021).
- Pemerintah Provinsi Bali. Provinsi Bali Tanggap COVID-19. 2021. Available online: https://infocorona.baliprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Sumatera Utara. Sumut Tanggap COVID-19. 2021. Available online: https://covid19.sumutprov.go.id/ (accessed on 3 July 2021).
- Pemerintah Daerah Daerah Instimewa Yogyakarta. Yogyakarta Tanggap COVID-19. 2021. Available online: https://corona.jogjaprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Kalimantan Selatan. Kalsel Tanggap COVID-19. 2021. Available online: https://corona.kalselprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Papua. Papua COVID-19. 2021. Available online: https://covid19.papua.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Sumatera Selatan. Sumatera Selatan Tanggap COVID-19. 2021. Available online: http://corona.sumselprov.go.id (accessed on 7 July 2021).
- Pemerintah Provinsi Sulawesi Utara. Angka Kejadian di Sulawesi Utara. 2021. Available online: https://corona.sulutprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Kalimantan Tengah. Media Center Satuan Tugas COVID-19 Kalimantan Tengah. 2021. Available online: https://corona.kalteng.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Aceh. Aceh Tanggap COVID-19. 2021. Available online: https://covid19.acehprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Sulawesi Utara. Info COVID-19 Sultra. 2021. Available online: https://dinkes.sultraprov.go.id/info-covid-19-sultra/ (accessed on 7 July 2021).
- Pemerintah Provinsi Lampung. Website Informasi COVID-19 Provinsi Lampung. 2021. Available online: https://covid19.lampungprov.go.id/ (accessed on 7 July 2021).
- Gugus Tugas COVID-19 Kepulauan Riau. Kepulauan Riau Tanggap COVID-19. 2021. Available online: https://corona.kepriprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Nusa Tenggara Barat. Pemerintah Serius, Siap dan Mampu Menangani COVID-19. 2021. Available online: https://corona.ntbprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Papua Barat. Situasi Terkini Vovid-19 di Papua Barat. 2021. Available online: https://dinkes.papuabaratprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Maluku. Maluku Tanggap COVID-19. 2021. Available online: https://corona.malukuprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Kalimantan Utara. Pusat Informasi COVID-19 Provinsi Kalimantan Utara. 2021. Available online: https://coronainfo.kaltaraprov.go.id (accessed on 7 July 2021).
- Pemerintah Provinsi Sulawesi Tengah. Dinas Kesehatan Provinsi Sulawesi Tengah. 2021. Available online: https://dinkes.sultengprov.go.id/category/covid-19 (accessed on 7 July 2021).
- Tim-eGovernment Provinsi Bengkulu. Data Real Time COVID-19 Provinsi Bengkulu. 2021. Available online: https://covid19.bengkuluprov.go.id/databengkulu (accessed on 7 July 2021).
- Gugus Tugas COVID-19 Provinsi Gorontalo. Gorontalo Tanggap Darurat COVID-19. 2021. Available online: https://dinkes.gorontaloprov.go.id/covid-19/ (accessed on 7 July 2021).
- Pemerintah Provinsi Jambi. Jambi Siaga COVID-19. 2021. Available online: http://corona.jambiprov.go.id/v2/ (accessed on 7 July 2021).
- Pemerintah Provinsi Kalimantan Barat. Satu Data Kalbar. 2021. Available online: http://data.kalbarprov.go.id/ (accessed on 7 July 2021).
- Badan Penanggulangan Bencana Daerah Provinsi Kepulauan Bangka Belitung. Satgas COVID-19 Pusdalops BPBD. 2021. Available online: http://covid19.babelprov.go.id (accessed on 7 July 2021).
- PT Koridor Indomedia Persada. Maluku Utara Tanggap COVID-19. 2021. Available online: https://koridormalutnews.com/statistik-covid-19/ (accessed on 7 July 2021).
- Pemerintah Provinsi Nusa Tenggara Timur. Gugus Tugas Percepatan Penanganan COVID-19 NTT. 2021. Available online: http://www.covid19.nttprov.go.id/ (accessed on 7 July 2021).
- Pemerintah Provinsi Sulawesi Barat. Pantauan COVID-19 Prov Sulbar. 2021. Available online: https://covid19.sulbarprov.go.id/utama/data (accessed on 7 July 2021).
- Pemerintah Kabupaten Bangka. Pusat Informasi COVID-19 Kabupaten Bangka. 2021. Available online: https://covid19.bangka.go.id (accessed on 7 July 2021).
- Satgas Penanganan COVID-19 Kabupaten Bangka Barat. Pusat Informasi COVID-19 Kabupaten Bangka Barat. 2021. Available online: https://covid19.bangkabaratkab.go.id (accessed on 7 July 2021).
- Pemerintah Kabupaten Bangka Tengah. Update Informasi Kasus COVID-19 di Kabupaten Bangka Tengah 7 Juli 2021. 2021. Available online: https://bangkatengahkab.go.id/berita/detail/kominfo/update-informasi-kasus-covid19-di-kabupaten-bangka-tengah-07-juli-2021 (accessed on 7 July 2021).
- Gugus Tugas COVID-19 Kabupaten Bangka Selatan. Data COVID-19 Kab. Bangka Selatan. 2021. Available online: https://covid19.bangkaselatankab.go.id (accessed on 7 July 2021).
- Badan Penanggulangan Bencana Daerah Pangkalpinang. Update Data COVID-19 Kota Pangkalpinang. 2021. Available online: https://bpbd.pangkalpinangkota.go.id/berita/read/8/2020/update-data-covid-19-kota-pangkalpinang-per-tanggal-09-agustus-2020 (accessed on 7 July 2021).
- Dinas Kesehatan Kabupaten Belitung. Informasi Jumlah Pasien Terkait COVID-19 di Kabupaten Belitung. 2021. Available online: https://covid19.belitung.go.id (accessed on 7 July 2021).
- Pemerintah Kabupaten Belitung Timur. Pusat Informasi COVID-19 Belitung Timur. 2021. Available online: https://corona.belitungtimurkab.go.id (accessed on 7 July 2021).
- Badan Litbangkes Kementerian Kesehatan Republik Indonesia. Daftar Laboratorium Pemeriksa COVID-19. 2021. Available online: https://www.litbang.kemkes.go.id/laboratorium-pemeriksa-covid-19/ (accessed on 6 July 2021).
- Bona, M.F. Hanya 52% Lab Laporkan Hasil Tes PCR, DPR: Datanya Salah atau Kurang Koordinasi? 2021. Available online: https://www.beritasatu.com/kesehatan/779531/hanya-52-lab-laporkan-hasil-tes-pcr-dpr-datanya-salah-atau-kurang-koordinasi (accessed on 6 July 2021).
- Rahadi, P. Satgas COVID-19: Jangan Ada Lagi Data Terlambat. 2021. Available online: https://rri.co.id/nasional/peristiwa/963565/satgas-covid-19-jangan-ada-lagi-data-terlambat (accessed on 6 July 2021).
- Nugraheny, D.E. Satu Tahun Pandemi dan Persoalan Pencatatan Data COVID-19 yang Belum Terselesaikan. 2021. Available online: https://nasional.kompas.com/read/2021/03/02/10273881/satu-tahun-pandemi-dan-persoalan-pencatatan-data-covid-19-yang-belum?page=all (accessed on 6 July 2021).
- Nugraheny, D.E. Pencatatan Data COVID-19 Masih Ada yang Terlambat, Kemenkes Jelaskan Penyebabnya. 2021. Available online: https://nasional.kompas.com/read/2021/02/03/17194311/pencatatan-data-covid-19-masih-ada-yang-terlambat-kemenkes-jelaskan?page=all (accessed on 6 July 2021).
- Mantalean, V. Data COVID-19 Beda Jauh Dengan Kemenkes, Depok Berpegang Pada Data Real-Time. 2021. Available online: https://megapolitan.kompas.com/read/2021/01/07/13115951/data-covid-19-beda-jauh-dengan-kemenkes-depok-berpegang-pada-data-real (accessed on 6 July 2021).
- Callaghan, S.J.P. COVID-19 is a data science issue. Gene Expr. Patterns 2020, 1, 100022. [Google Scholar] [CrossRef] [PubMed]
- Kondilis, E.; Papamichail, D.; Gallo, V.; Benos, A. COVID-19 data gaps and lack of transparency undermine pandemic response. J. Public Health 2021, 43, e307–e308. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Oroz, M.; Pham, K.H.; Bullock, J.; Kirkpatrick, R.; Luccioni, A.; Rubel, S.; Wachholz, C.; Chakchouk, M.; Biggs, P.; Nguyen, T.; et al. Artificial intelligence cooperation to support the global response to COVID-19. Nat. Mach. Intell. 2020, 2, 295–297. [Google Scholar] [CrossRef]
- Naudé, W.; Vinuesa, R. Data deprivations, data gaps and digital divides: Lessons from the COVID-19 pandemic. Big Data Soc. 2021, 8. [Google Scholar] [CrossRef]
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]


{kind=link}
| No | Provinces | National Level (KawalCOVID-19 and KawalCorona Websites) [13,14] | Provincial Level | Difference | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive Cases | Cured Cases | Deaths | Positive Cases | Cured Cases | Deaths | References | Positive Cases | Cured Cases | Deaths | |||||
| 1 | DKI Jakarta | 610,303 | 501,083 | 8991 | 610,303 | 501,199 | 9042 | [18] | 0 | 0.00% | 116 | 0.02% | 51 | 0.57% |
| 2 | Jawa Barat (West Java) | 425,206 | 340,412 | 5712 | 425,206 | 340,412 | 5712 | [19] | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 3 | Jawa Tengah (Central Java) | 276,598 | 218,424 | 12,135 | 276,598 | 227,539 | 17,386 | [20] | 0 | 0.00% | 9115 | 4.17% | 5251 | 43.27% |
| 4 | Jawa Timur (East Java) | 184,624 | 157,489 | 13,293 | 184,624 | 158,640 | 13,601 | [21] | 0 | 0.00% | 1151 | 0.73% | 308 | 2.32% |
| 5 | Sulawesi Selatan (South Sulawesi) | 66,268 | 62,404 | 1004 | 65,738 | 62,331 | 996 | [22] | 530 | 0.81% | 73 | 0.12% | 8 | 0.80% |
| 6 | Kalimantan Timur (East Kalimantan) | 81,763 | 73,072 | 1957 | 81,006 | 72,758 | 1920 | [23] | 757 | 0.93% | 314 | 0.43% | 37 | 1.93% |
| 7 | Riau | 73,726 | 67,476 | 1996 | 73,706 | 67,457 | 1995 | [24] | 20 | 0.03% | 19 | 0.03% | 1 | 0.05% |
| 8 | Sumatera Barat (West Sumatera) | 54,187 | 48,228 | 1239 | 54,186 | 48,343 | 1243 | [25] | 1 | 0.00% | 115 | 0.24% | 4 | 0.32% |
| 9 | Banten | 60,672 | 50,271 | 1447 | 63,496 | 54,639 | 1625 | [26] | 2824 | 4.65% | 4368 | 8.69% | 178 | 12.30% |
| 10 | Bali | 52,828 | 48,233 | 1605 | 52,828 | 48,239 | 1605 | [27] | 0 | 0.00% | 6 | 0.01% | 0 | 0.00% |
| 11 | Sumatera Utara (North Sumatera) | 37,425 | 33,325 | 1218 | 37,425 | 33,323 | 1218 | [28] | 0 | 0.00% | 2 | 0.01% | 0 | 0.00% |
| 12 | Yogyakarta | 69,470 | 52,401 | 1810 | 68,100 | 51,601 | 1778 | [29] | 1 | 0.00% | 800 | 1.55% | 32 | 1.80% |
| 13 | Kalimantan Selatan (South Kalimantan) | 36,832 | 34,619 | 1084 | 36,832 | 34,619 | 1084 | [30] | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 14 | Papua | 21,276 | 11,687 | 213 | 23,818 | 22,165 | 469 | [31] | 2542 | 11.95% | 10,478 | 89.66% | 256 | 120.19% |
| 15 | Sumatera Selatan (South Sumatera) | 30,510 | 26,697 | 1540 | 30,152 | 26,559 | 1520 | [32] | 358 | 1.19% | 138 | 0.52% | 20 | 1.32% |
| 16 | Sulawesi Utara (North Sulawesi) | 16,921 | 15,460 | 562 | 16,773 | 15,447 | 560 | [33] | 148 | 0.88% | 13 | 0.08% | 2 | 0.36% |
| 17 | Kalimantan Tengah (Central Kalimantan) | 27,342 | 20,903 | 552 | 27,271 | 24,045 | 740 | [34] | 71 | 0.26% | 3142 | 15.03% | 188 | 34.06% |
| 18 | Aceh | 19,898 | 15,380 | 842 | 19,893 | 15,335 | 841 | [35] | 5 | 0.03% | 45 | 0.29% | 1 | 0.12% |
| 19 | Sulawesi Tenggara (Southeast Sulawesi) | 12,188 | 10,389 | 249 | 12,074 | 10,412 | 247 | [36] | 114 | 0.94% | 23 | 0.22% | 2 | 0.81% |
| 20 | Lampung | 23,622 | 19,058 | 1141 | 23,302 | 19,680 | 1273 | [37] | 320 | 1.37% | 622 | 3.26% | 132 | 11.57% |
| 21 | Kepulauan Riau (Riau Islands) | 29,456 | 23,751 | 623 | 28,848 | 23,363 | 626 | [38] | 608 | 2.11% | 388 | 1.66% | 3 | 0.48% |
| 22 | Nusa Tenggara Barat (West Nusa Tenggara) | 13,436 | 11,426 | 497 | 15,027 | 13,463 | 618 | [39] | 1591 | 11.84% | 2037 | 17.83% | 121 | 24.35% |
| 23 | Papua Barat (West Papua) | 12,557 | 9678 | 192 | 12,270 | 9631 | 191 | [40] | 287 | 2.34% | 47 | 0.49% | 1 | 0.52% |
| 24 | Maluku | 9952 | 7699 | 157 | 9952 | 7798 | 159 | [41] | 0 | 0.00% | 99 | 1.29% | 2 | 1.27% |
| 25 | Kalimantan Utara (North Kalimantan) | 13,982 | 12,271 | 207 | 13,827 | 12,587 | 210 | [42] | 155 | 1.11% | 316 | 2.58% | 3 | 1.45% |
| 26 | Sulawesi Tengah (Central Sulawesi) | 14,279 | 12,871 | 414 | 14,161 | 12,856 | 412 | [43] | 118 | 0.83% | 15 | 0.12% | 2 | 0.49% |
| 27 | Bengkulu | 11,306 | 9367 | 240 | 11,305 | 9186 | 234 | [44] | 1 | 0.01% | 181 | 1.97% | 6 | 2.56% |
| 28 | Gorontalo | 6112 | 5549 | 186 | 5997 | 5571 | 186 | [45] | 115 | 1.92% | 22 | 0.40% | 0 | 0.00% |
| 29 | Jambi | 13,617 | 11,884 | 288 | 13,511 | 11,826 | 284 | [46] | 106 | 0.78% | 58 | 0.49% | 4 | 1.41% |
| 30 | Kalimantan Barat (West Kalimantan) | 16,227 | 14,090 | 411 | 14,669 | 13,225 | 271 | [47] | 1558 | 10.62% | 865 | 6.54% | 140 | 51.66% |
| 31 | Bangka Belitung | 22,613 | 20,511 | 354 | 22,613 | 20,511 | 354 | [48] | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% |
| 32 | Maluku Utara (North Maluku) | 6230 | 4598 | 139 | 4414 | 4117 | 120 | [49] | 1816 | 41.14% | 481 | 11.68% | 19 | 15.83% |
| 33 | Nusa Tenggara Timur (East Nusa Tenggara) | 21,799 | 17,114 | 484 | 21,642 | 17,518 | 514 | [50] | 157 | 0.73% | 404 | 2.36% | 30 | 6.20% |
| 34 | Sulawesi Barat (West Sulawesi) | 6172 | 5568 | 126 | 5933 | 5505 | 122 | [51] | 239 | 4.03% | 63 | 1.14% | 4 | 3.28% |
| TOTAL | 2,379,397 | 1,973,388 | 62,908 | 2,377,500 | 2,001,900 | 69,156 | 1897 | 0.08% | 28,512 | 1.44% | 6248 | 9.93% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barsasella, D.; Iman, A.T.; Fadly, F.; Uddin, M.; Mohammed, A.; Shaik, T.; Saputra, H.; Malwade, S.; Dhar, E.; Zakiah; et al. Information Flow and Data Gaps in COVID-19 Recording and Reporting at National and Provincial Levels in Indonesia. Healthcare 2022, 10, 204. https://doi.org/10.3390/healthcare10020204
Barsasella D, Iman AT, Fadly F, Uddin M, Mohammed A, Shaik T, Saputra H, Malwade S, Dhar E, Zakiah, et al. Information Flow and Data Gaps in COVID-19 Recording and Reporting at National and Provincial Levels in Indonesia. Healthcare. 2022; 10(2):204. https://doi.org/10.3390/healthcare10020204
Chicago/Turabian StyleBarsasella, Diana, Arief Tarmansyah Iman, Fery Fadly, Mohy Uddin, Arshad Mohammed, Tazeem Shaik, Hermawan Saputra, Shwetambara Malwade, Eshita Dhar, Zakiah, and et al. 2022. "Information Flow and Data Gaps in COVID-19 Recording and Reporting at National and Provincial Levels in Indonesia" Healthcare 10, no. 2: 204. https://doi.org/10.3390/healthcare10020204