Most Common Long COVID Physical Symptoms in Working Age Adults Who Experienced Mild COVID-19 Infection: A Scoping Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identifying Relevant Studies
2.2. Search Strategy
2.3. Study Selection
2.4. Charting the Data
2.5. Collating, Summarising and Reporting
3. Results
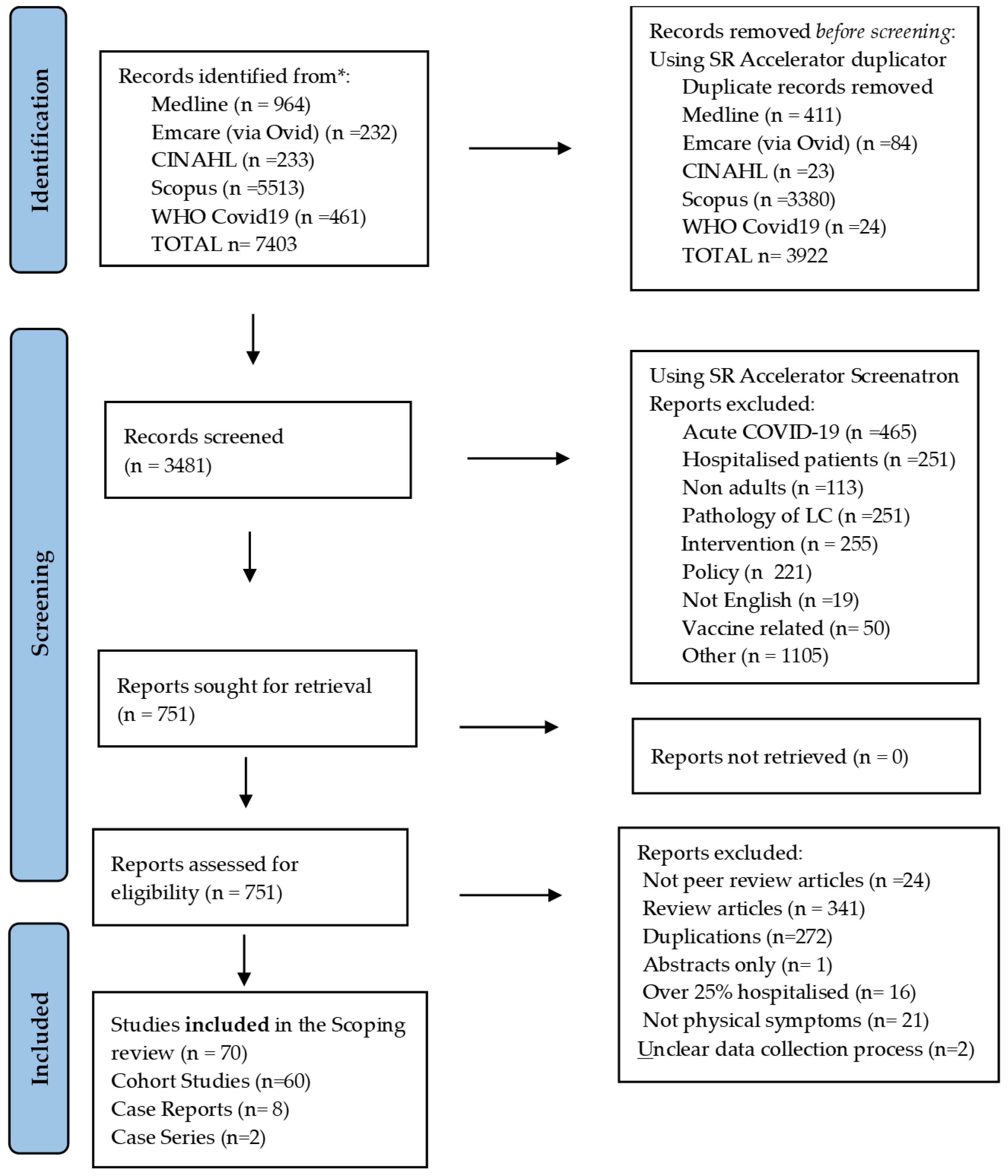
3.1. Study Selection and Characteristics
3.2. Description of Included Studies
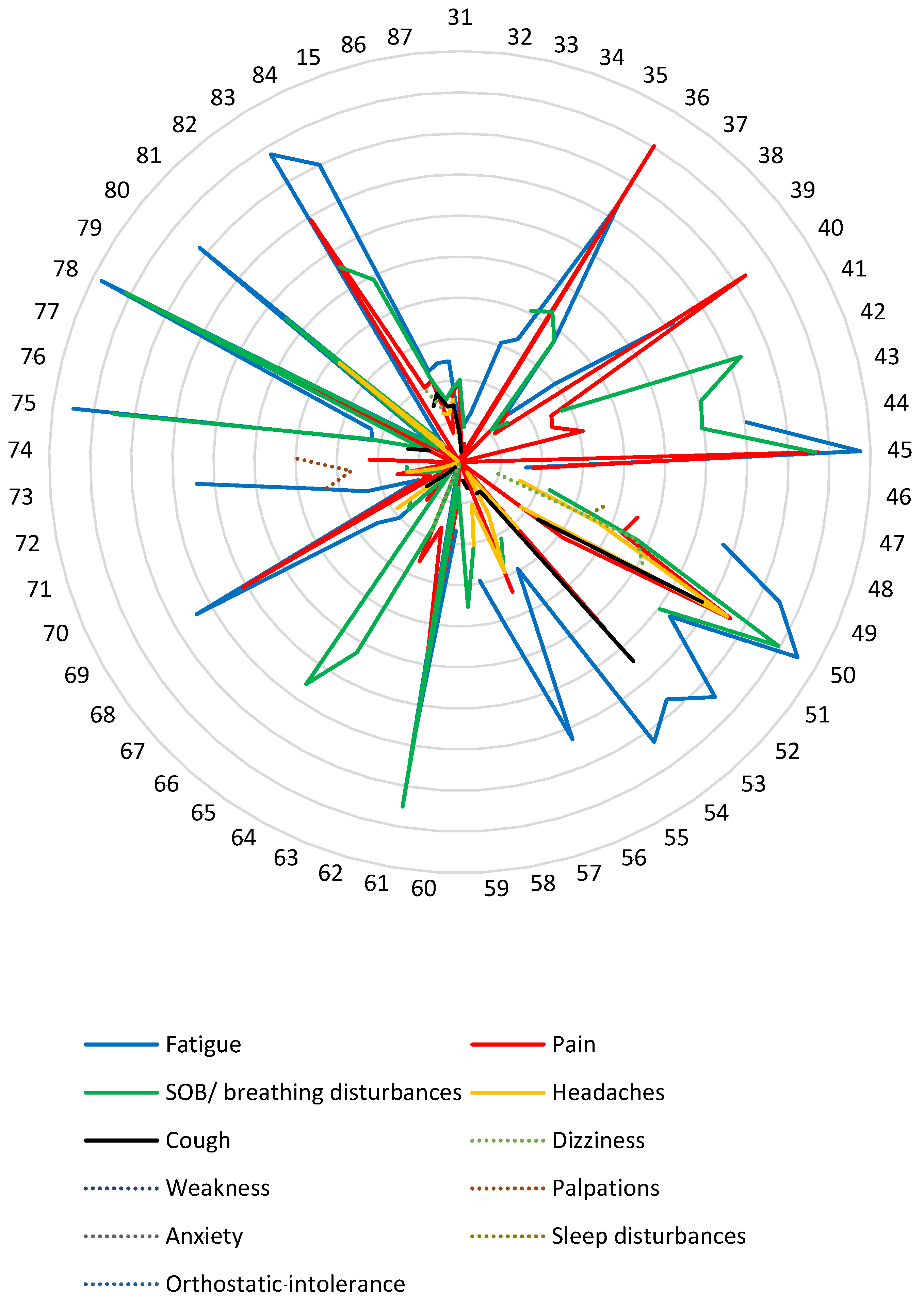
3.3. Description of the Physical Symptoms of Long COVID from the Cohort Studies

4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus COVID-19 Dashboard. Available online: https://covid19.who.int (accessed on 8 December 2021).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Aouissi, H.A.; Kechebar, M.S.A.; Ababsa, M.; Roufayel, R.; Neji, B.; Petrisor, A.-I.; Hamimes, A.; Epelboin, L.; Ohmagari, N. The Importance of Behavioral and Native Factors on COVID-19 Infection and Severity: Insights from a Preliminary Cross-Sectional Study. Healthcare 2022, 10, 1341. [Google Scholar] [CrossRef] [PubMed]
- Arsenault, C.; Gage, A.; Kim, M.K.; Kapoor, N.R.; Akweongo, P.; Amponsah, F.; Aryal, A.; Asai, D.; Awoonor-Williams, J.K.; Ayele, W.; et al. COVID-19 and resilience of healthcare systems in ten countries. Nat. Med. 2022, 28, 1314–1324. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Ayenigbara, I.O.; Adegboro, J.S.; Ayenigbara, G.O.; Adeleke, O.R.; Olofintuyi, O.O. The challenges to a successful COVID-19 vaccination programme in Africa. Germs 2021, 11, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Marshall, M. The four most urgent questions about long COVID. Nature 2021, 594, 168–170. [Google Scholar] [CrossRef]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus, 6 October 2021. Available online: https://apps.who.int/iris/handle/10665/345824 (accessed on 6 January 2022).
- Mahase, E. COVID-19: What do we know about “long covid”? BMJ 2020, 370, m2815. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19 2020. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 6 January 2022).
- van Kessel, S.A.; Olde Hartman, T.C.; Lucassen, P.L.; van Jaarsveld, C.H. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam Pract. 2022, 39, 159–167. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Carson, G. Long Covid Forum Group Research priorities for Long Covid: Refined through an international multi-stakeholder forum. BMC Med. 2021, 19, 84. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Foer, D.; MacPhaul, E.; Lo, Y.-C.; Bates, D.W.; Zhou, L. PASCLex: A comprehensive post-acute sequelae of COVID-19 (PASC) symptom lexicon derived from electronic health record clinical notes. J. Biomed. Inform. 2021, 125, 103951. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. International Classification of Functioning, Disability and Health: ICF. World Health Organization. 2001. Available online: https://apps.who.int/iris/handle/10665/42407 (accessed on 6 January 2022).
- Reuschke, D.; Houston, D. The impact of Long COVID on the UK workforce. Appl. Econ. Lett. 2022, 8, 1–5. [Google Scholar]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Negro, F.D.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Rose, E.B.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network—United States, March–June 2020. Morb. Mortal Wkly. Rep. 2020, 69, 993. [Google Scholar] [CrossRef] [PubMed]
- Vaes, A.W.; Machado, F.V.; Meys, R.; Delbressine, J.M.; Goertz, Y.M.; Van Herck, M.; Houben-Wilke, S.; Franssen, F.M.; Vijlbrief, H.; Spies, Y.; et al. Care Dependency in Non-Hospitalized Patients with COVID-19. J. Clin. Med. 2020, 9, 2946. [Google Scholar] [CrossRef]
- Antipova, A. Analysis of the COVID-19 impacts on employment and unemployment across the multi-dimensional social disadvantaged areas. Soc. Sci. Humanit. Open 2021, 4, 100224. [Google Scholar] [CrossRef]
- Stiglitz, J.E. The proper role of government in the market economy: The case of the post-COVID recovery. J. Gov. Econ. 2021, 1, 100004. [Google Scholar] [CrossRef]
- Neves, M.T.; de Matos, L.V.; Vasques, A.C.; Sousa, I.E.; Ferreira, I.; Peres, S.; Jesus, S.; Fonseca, C.; Mansinho, K. COVID-19 and aging: Identifying measures of severity. SAGE Open Med. 2021, 9, 20503121211027462. [Google Scholar] [CrossRef]
- Office for National Statistics. Working Age Population: Gov.UK. 2020. Available online: https://www.ethnicity-facts-figures.service.gov.uk/uk-population-by-ethnicity/demographics/working-age-population/latest#full-page-history (accessed on 6 January 2022).
- Song, Y.; Yang, Y.; Yu, J.; Zhao, Z. The Post-COVID-19 Economic Policy Uncertainty and the Effectiveness of Monetary Policy: Evidence from China. Front. Public Health 2021, 9, 771364. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative research synthesis: Methodological guidance for systematic reviewers utilizing meta-aggregation. JBI Evid. Implement. 2015, 13, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.; Glasziou, P.; Del Mar, C.; Bannach-Brown, A.; Stehlik, P.; Scott, A.M. A full systematic review was completed in 2 weeks using automation tools: A case study. J. Clin. Epidemiol. 2020, 121, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Swift, J.A.; Glazebrook, C.; Macdonald, I. Validation of a brief, reliable scale to measure knowledge about the health risks associated with obesity. Int. J. Obes. 2005, 30, 661–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; Di Cristanziano, V.; Osebold, L.; et al. Post-COVID syndrome in non-hospitalised patients with COVID-19: A longitudinal prospective cohort study. Lancet Reg. Health-Eur. 2021, 6, 100122. [Google Scholar] [CrossRef]
- Bakılan, F.; Gökmen, I.G.; Ortanca, B.; Uçan, A.; Güvenç, E.; Mutlu, F.; Gökmen, H.M.; Ekim, A. Musculoskeletal symptoms and related factors in postacute COVID-19 patients. Int. J. Clin. Pr. 2021, 75, e14734. [Google Scholar] [CrossRef] [PubMed]
- Barizien, N.; Le Guen, M.; Russel, S.; Touche, P.; Huang, F.; Vallée, A. Clinical characterization of dysautonomia in long COVID-19 patients. Sci. Rep. 2021, 11, 14042. [Google Scholar] [CrossRef]
- Bastola, A.; Nepal, R.; Shrestha, B.; Maharjan, K.; Shrestha, S.; Chalise, B.; Neupane, J. Persistent Symptoms in Post-COVID-19 Patients Attending Follow-Up OPD at Sukraraj Tropical and Infectious Disease Hospital (STIDH), Kathmandu, Nepal. Trop. Med. Infect. Dis. 2021, 6, 113. [Google Scholar] [CrossRef]
- Aly, M.A.E.G.; Saber, H.G. Long COVID and chronic fatigue syndrome: A survey of elderly female survivors in Egypt. Int. J. Clin. Pr. 2021, 75, e14886. [Google Scholar] [CrossRef]
- Bierle, D.M.; Aakre, C.A.; Grach, S.L.; Salonen, B.R.; Croghan, I.T.; Hurt, R.T.; Ganesh, R. Central Sensitization Phenotypes in Post Acute Sequelae of SARS-CoV-2 Infection (PASC): Defining the Post COVID Syndrome. J. Prim. Care Community Health 2021, 12, 21501327211030826. [Google Scholar] [CrossRef]
- Bell, M.L.; Catalfamo, C.J.; Farland, L.V.; Ernst, K.C.; Jacobs, E.T.; Klimentidis, Y.C.; Jehn, M.; Pogreba-Brown, K. Post-acute sequelae of COVID-19 in a non-hospitalized cohort: Results from the Arizona CoVHORT. PLoS ONE 2021, 16, e0254347. [Google Scholar] [CrossRef] [PubMed]
- Bliddal, S.; Banasik, K.; Pedersen, O.B.; Nissen, J.; Cantwell, L.; Schwinn, M.; Tulstrup, M.; Westergaard, D.; Ullum, H.; Brunak, S.; et al. Acute and persistent symptoms in non-hospitalized PCR-confirmed COVID-19 patients. Sci. Rep. 2021, 11, 13153. [Google Scholar] [CrossRef] [PubMed]
- Blomberg, B.; Mohn, K.G.-I.; Brokstad, K.A.; Zhou, F.; Linchausen, D.W.; Hansen, B.-A.; Lartey, S.; Onyango, T.B.; Kuwelker, K.; Sævik, M.; et al. Long COVID in a prospective cohort of home-isolated patients. Nat. Med. 2021, 27, 1607–1613. [Google Scholar] [CrossRef] [PubMed]
- Boesl, F.; Audebert, H.; Endres, M.; Prüss, H.; Franke, C. A Neurological Outpatient Clinic for Patients with Post-COVID-19 Syndrome—A Report on the Clinical Presentations of the First 100 Patients. Front. Neurol. 2021, 12, 738405. [Google Scholar] [CrossRef]
- Buoite Stella, A.; Furlanis, G.; Frezza, N.A.; Valentinotti, R.; Ajcevic, M.; Manganotti, P. Autonomic dysfunction in post-COVID patients with and witfhout neurological symptoms: A prospective multidomain observational study. J. Neurol. 2021, 12, 587–596. [Google Scholar] [CrossRef]
- Danesh, V.; Arroliga, A.C.; Bourgeois, J.A.; Widmer, A.J.; McNeal, M.J.; McNeal, T.M. Post-acute sequelae of COVID-19 in adults referred to COVID recovery clinic services in an integrated health system in Texas. Bayl. Univ. Med. Cent. Proc. 2021, 34, 645–648. [Google Scholar] [CrossRef]
- Davin-Casalena, B.; Lutaud, R.; Scronias, D.; Guagliardo, V.; Verger, P. French General Practitioners Frequently See Patients with Long-COVID. J. Am. Board Fam. Med. 2021, 34, 1010–1013. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. eClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Dennis, A.; Wamil, M.; Alberts, J.; Oben, J.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Brady, M.; Hishmeh, L.; et al. Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: A prospective, community-based study. BMJ Open 2021, 11, e048391. [Google Scholar] [CrossRef]
- Gaber, T.A.-Z.K.; Ashish, A.; Unsworth, A. Persistent post-covid symptoms in healthcare workers. Occup. Med. 2021, 71, 144–146. [Google Scholar] [CrossRef]
- Ganesh, R.; Ghosh, A.K.; Nyman, M.A.; Croghan, I.T.; Grach, S.L.; Anstine, C.V.; Salonen, B.R.; Hurt, R.T. PROMIS Scales for Assessment of Persistent Post-COVID Symptoms: A Cross Sectional Study. J. Prim. Care Community Health 2021, 12, 21501327211030413. [Google Scholar] [CrossRef] [PubMed]
- González-Andrade, F. Post-COVID-19 conditions in Ecuadorian patients: An observational study. Lancet Reg. Health-Am. 2021, 5, 100088. [Google Scholar] [CrossRef] [PubMed]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized COVID-19 “long haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef] [PubMed]
- Goërtz, Y.M.J.; van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542–2020. [Google Scholar] [CrossRef]
- Heightman, M.; Prashar, J.; Hillman, T.E.; Marks, M.; Livingston, R.; Ridsdale, H.A.; Roy, K.; Bell, R.; Zandi, M.; McNamara, P.; et al. Post-COVID-19 assessment in a specialist clinical service: A 12-month, single-centre, prospective study in 1325 individuals. BMJ Open Respir. Res. 2021, 8, e001041. [Google Scholar] [CrossRef]
- Herck, M.V.; Goërtz, Y.M.J.; Houben-Wilke, S.; Machado, F.V.C.; Meys, R.; Delbressine, J.M.; Vaes, A.W.; Burtin, C.; Posthuma, R.; Frannsen, F.M.E.; et al. Severe fatigue in long COVID: Follow-up study in members of online long COVID support groups. J. Med. Internet Res. 2021, 23, e30274. [Google Scholar] [CrossRef]
- Holmes, E.; Wist, J.; Masuda, R.; Lodge, S.; Nitschke, P.; Kimhofer, T.; Loo, R.L.; Begum, S.; Boughton, B.; Yang, R.; et al. Incomplete Systemic Recovery and Metabolic Phenoreversion in Post-Acute-Phase Nonhospitalized COVID-19 Patients: Implications for Assessment of Post-Acute COVID-19 Syndrome. J. Proteome Res. 2021, 20, 3315–3329. [Google Scholar] [CrossRef]
- Hossain, M.A.; Hossain, K.M.A.; Saunders, K.; Uddin, Z.; Walton, L.M.; Raigangar, V.; Sakel, M.; Shafin, R.; Kabir, F.; Faruqui, R.; et al. Prevalence of Long COVID symptoms in Bangladesh: A prospective Inception Cohort Study of COVID-19 survivors. BMJ Glob. Health 2021, 6, e006838. [Google Scholar] [CrossRef]
- Jacobson, K.B.; Rao, M.; Bonilla, H.; Subramanian, A.; Hack, I.; Madrigal, M.; Singh, U.; Jagannathan, P.; Grant, P. Patients with Uncomplicated Coronavirus Disease 2019 (COVID-19) Have Long-Term Persistent Symptoms and Functional Impairment Similar to Patients with Severe COVID-19: A Cautionary Tale During a Global Pandemic. Clin. Infect. Dis. 2021, 73, e826–e829. [Google Scholar] [CrossRef]
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int. J. Clin. Pract. 2021, 75, e13746. [Google Scholar] [CrossRef]
- Kashif, A.; Chaudhry, M.; Fayyaz, T.; Abdullah, M.; Malik, A.; Anwer, J.M.A.; Inam, S.H.A.; Fatima, T.; Iqbal, N.; Shoaib, K. Follow-up of COVID-19 recovered patients with mild disease. Sci. Rep. 2021, 11, 13414. [Google Scholar] [CrossRef] [PubMed]
- Kayaaslan, B.; Eser, F.; Kalem, A.K.; Kaya, G.; Kaplan, B.; Kacar, D.; Hasanoglu, I.; Coskun, B.; Guner, R. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J. Med. Virol. 2021, 93, 6566–6574. [Google Scholar] [CrossRef] [PubMed]
- Lund, L.C.; Hallas, J.; Nielsen, H.; Koch, A.; Mogensen, S.H.; Brun, N.C.; Christiansen, C.F.; Thomsen, R.W.; Pottegård, A. Post-acute effects of SARS-CoV-2 infection in individuals not requiring hospital admission: A Danish population-based cohort study. Lancet Infect Dis. 2021, 21, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Mady, A.F.; Abdelfattah, R.A.; Kamel, F.M.; Naiem, A.S.M.A.; AbdelGhany, W.M.; Abdelaziz, A.O. Predictors of Long COVID 19 Syndrome. Egypt. J. Hosp. Med. 2021, 85, 3604–3608. [Google Scholar] [CrossRef]
- Mahmoud, M.H.; Alghamdi, F.A.; Alghamdi, G.A.; Alkhotani, L.A.; Alrehaili, M.A.; El-Deeb, D.K. Study of Post-COVID-19 Syndrome in Saudi Arabia. Cureus 2021, 13, 17787. [Google Scholar] [CrossRef] [PubMed]
- Matta, J.; Wiernik, E.; Robineau, O.; Carrat, F.; Touvier, M.; Severi, G.; de Lamballerie, X.; Blanché, H.; Deleuze, J.; Gouraud, C. Association of Self-reported COVID-19 Infection and SARS-CoV-2 Serology Test Results with Persistent Physical Symptoms among French Adults during the COVID-19 Pandemic. JAMA Intern. Med. 2021, 182, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Mittal, C.; Mishra, A.; Jain, S.; Gautam, N.S. Post covid-19 symptoms: A neglected domain. Indian J. Community Health 2021, 33, 325–328. [Google Scholar] [CrossRef]
- Mohamed-Hussein, A.A.R.; Amin, M.T.; Makhlouf, H.A.; Galal, I.; Abd-Elaal, H.K.; Abdeltawab, D.; Kholief, K.M.S.; Hashem, M.K. Non-hospitalised COVID-19 patients have more frequent long COVID-19 symptoms. Int. J. Tuberc. Lung Dis. 2021, 25, 732–737. [Google Scholar] [CrossRef]
- Munker, D.; Veit, T.; Barton, J.; Mertsch, P.; Mümmler, C.; Osterman, A.; Khatamzas, E.; Barnikel, M.; Hellmuth, J.C.; Münchhoff, M.; et al. Pulmonary function impairment of asymptomatic and persistently symptomatic patients 4 months after COVID-19 according to disease severity. Infection 2021, 50, 157–168. [Google Scholar] [CrossRef]
- Naik, S.; Haldar, S.N.; Soneja, M.; Mundadan, N.G.; Garg, P.; Mittal, A.; Desai, D.; Trilangi, P.K.; Chakraborty, S.; Begam, N.N.; et al. Post COVID-19 sequelae: A prospective observational study from Northern India. Drug Discov. Ther. 2021, 15, 254–260. [Google Scholar] [CrossRef]
- Nehme, M.; Braillard, O.; Chappuis, F.; Courvoisier, D.S.; Guessous, I.; on behalf of the CoviCare Study Team*. Prevalence of Symptoms More Than Seven Months after Diagnosis of Symptomatic COVID-19 in an Outpatient Setting. Ann. Intern. Med. 2021, 174, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Ordinola Navarro, A.; Cervantes-Bojalil, J.; Cobos Quevedo, O.D.J.; Avila Martínez, A.; Hernández-Jiménez, C.A.; Pérez Álvarez, E.; Gil, A.G.; Amaro, A.L.P.; Vera-Lastra, O.; Luis, B.A.L. Decreased quality of life and spirometric alterations even after mild-moderate COVID-19. Respir. Med. 2021, 181, 106391. [Google Scholar] [CrossRef]
- Orrù, G.; Bertelloni, D.; Diolaiuti, F.; Mucci, F.; Di Giuseppe, M.; Biella, M.; Gemignani, A.; Ciacchini, R.; Conversano, C. Long-COVID Syndrome? A Study on the Persistence of Neurological, Psychological and Physiological Symptoms. Healthcare 2021, 9, 575. [Google Scholar] [CrossRef] [PubMed]
- Peghin, M.; Palese, A.; Venturini, M.; De Martino, M.; Gerussi, V.; Graziano, E.; Bontempo, G.; Marrella, F.; Tommasini, A.; Fabris, M.; et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin. Microbiol. Infect. 2021, 27, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Steig, B.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands: A Longitudinal Study Among Nonhospitalized Patients. Clin. Infect. Dis. 2020, 73, e4058–e4063. [Google Scholar] [CrossRef] [PubMed]
- Sahanic, S.; Tymoszuk, P.; Ausserhofer, D.; Rass, V.; Pizzini, A.; Nordmeyer, G.; Hüfner, K.; Kurz, K.; Weber, P.M.; Sonnweber, T.; et al. Phenotyping of acute and persistent COVID-19 features in the outpatient setting: Exploratory analysis of an international cross-sectional online survey. Clin. Infect. Dis. 2021, 26, ciab978. [Google Scholar]
- Ezzat, M.M.; Elsherif, A.A. Prevalence of fatigue in patients post COVID-19. Eur. J. Mol. Clin. Med. 2021, 8, 1330–1340. [Google Scholar]
- Shouman, K.; Vanichkachorn, G.; Cheshire, W.P.; Suarez, M.D.; Shelly, S.; Lamotte, G.J.; Sandroni, P.; Benarroch, E.E.; Berini, S.E.; Cutsforth-Gregory, J.K.; et al. Autonomic dysfunction following COVID-19 infection: An early experience. Clin. Auton. Res. 2021, 31, 385–394. [Google Scholar] [CrossRef]
- Sivan, M.; Parkin, A.; Makower, S.; Greenwood, D.C. Post-COVID syndrome symptoms, functional disability, and clinical severity phenotypes in hospitalized and nonhospitalized individuals: A cross-sectional evaluation from a community COVID rehabilitation service. J. Med. Virol. 2021, 15, 15. [Google Scholar] [CrossRef]
- Skala, M.; Svoboda, M.; Kopecky, M.; Kocova, E.; Hyrsl, M.; Homolac, M.; Chrobok, V.; Bostik, P.; Fajfr, M.; Prasil, P.; et al. Heterogeneity of post-COVID impairment: Interim analysis of a prospective study from Czechia. Virol. J. 2021, 18, 73. [Google Scholar] [CrossRef]
- Søraas, A.; Kalleberg, K.T.; Dahl, J.A.; Søraas, C.L.; Myklebust, T.; Axelsen, E.; Lind, A.; Bævre-Jensen, R.; Jørgensen, S.B.; Istre, M.S.; et al. Persisting symptoms three to eight months after non-hospitalized COVID-19, a prospective cohort study. PLoS ONE 2021, 16, e0256142. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Sultana, S.; Islam, M.T.; Salwa, M.; Hossain, S.M.Z.; Hasan, N.; Masum, A.A.; Khan, A.H.; Khan, M.H.; Haque, M.A. Duration and Risk Factors of Post-COVID Symptoms Following Recovery Among the Medical Doctors in Bangladesh. Cureus 2021, 13, 15351. [Google Scholar] [CrossRef] [PubMed]
- Tabacof, L.; Tosto-Mancuso, J.; Wood, J.; Cortes, M.; Kontorovich, A.; McCarthy, D.; Rizk, D.; Rozanski, G.; Breyman, E.; Nasr, L.; et al. Post-acute COVID-19 Syndrome Negatively Impacts Physical Function, Cognitive Function, Health-Related Quality of Life, and Participation. Am. J. Phys. Med. Rehabil. 2021, 101, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Tran, V.T.; Riveros, C.; Clepier, B.; Desvarieux, M.; Collet, C.; Yordanov, Y.; Ravaud, P. Development and validation of the long covid symptom and impact tools, a set of patient-reported instruments constructed from patients’ lived experience. Clin. Infect. Dis. 2021, 29, 29. [Google Scholar]
- Vanichkachorn, G.; Newcomb, R.; Cowl, C.T.; Murad, M.H.; Breeher, L.; Miller, S.; Trenary, M.; Neveau, D.; Higgins, S. Post–COVID-19 Syndrome (Long Haul Syndrome): Description of a Multidisciplinary Clinic at Mayo Clinic and Characteristics of the Initial Patient Cohort. Mayo Clin. Proc. 2021, 96, 1782–1791. [Google Scholar] [CrossRef]
- Yomogida, K.; Zhu, S.; Rubino, F.; Figueroa, W.; Balanji, N.; Holman, E. Post-Acute Sequelae of SARS-CoV-2 Infection Among Adults Aged >=18 Years—Long Beach, California, April 1-December 10, 2020. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 1274–1277. [Google Scholar] [CrossRef]
- Aeschlimann, F.A.; Misra, N.; Hussein, T.; Panaioli, E.; Soslow, J.H.; Crum, K.; Steele, J.M.; Huber, S.; Marcora, S.; Brambilla, P.; et al. Myocardial involvement in children with post-COVID multisystem inflammatory syndrome: A cardiovascular magnetic resonance based multicenter international study—The CARDOVID registry. J. Cardiovasc. Magn. Reson. 2021, 23, 140. [Google Scholar] [CrossRef]
- Wanga, V.; Chevinsky, J.R.; Dimitrov, L.V.; Gerdes, M.E.; Whitfield, G.P.; Bonacci, R.A.; Nji, M.A.M.; Hernandez-Romieu, A.C.; Rogers-Brown, J.S.; McLeod, T.; et al. Long-term symptoms among adults tested for SARS-CoV-2—United States, January 2020–April 2021. Morb. Mortal Wkly. Rep. 2021, 70, 1235. [Google Scholar] [CrossRef] [PubMed]
- Estiri, H.; Strasser, Z.H.; Brat, G.A.; Semenov, Y.R.; Patel, C.J.; Murphy, S.N.; Aaron, J.R.; Agapito, G.; Albayrak, A.; Alessiani, M.; et al. Evolving phenotypes of non-hospitalized patients that indicate long COVID. BMC Med. 2021, 19, 249. [Google Scholar] [CrossRef] [PubMed]
- Machado, F.V.C.; Meys, R.; Delbressine, J.M.; Vaes, A.W.; Goërtz, Y.M.J.; van Herck, M.; Houben-Wilke, S.; Boon, G.J.A.M.; Barco, S.; Burtin, C.; et al. Construct validity of the Post-COVID-19 Functional Status Scale in adult subjects with COVID-19. Health Qual. Life Outcomes 2021, 19, 40. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, K.J.; Vestergaard, J.M.; Schlunssen, V.; Bonde, J.P.; Kaspersen, K.A.; Biering, K.; Carstensen, O.; Greve, T.; Hansen, K.K.; Dalbøge, A.; et al. Day-by-day symptoms following positive and negative PCR tests for SARS-CoV-2 in non-hospitalized healthcare workers: A 90-day follow-up study. Int. J. Infect. Dis. 2021, 1, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Balan, S.; Beauchamps, L.; Gonzales-Zamora, J.A.; Vu, C.; Amoros, A.; Quiroz, T.; Stevenson, M.; Sharkey, M.; Andrews, D.M.; Abbo, L. Recovery does not always signal the end of the battle: A case of post SARS-CoV-2 multisystem inflammatory syndrome in an adult. IDCases 2021, 24, e01067. [Google Scholar] [CrossRef]
- Feghali, K.; Atallah, J.; Norman, C. Manifestations of thyroid disease post COVID-19 illness: Report of Hashimoto thyroiditis, Graves’ disease, and subacute thyroiditis. J. Clin. Transl. Endocrinol. Case Rep. 2021, 22, 100094. [Google Scholar] [CrossRef]
- Johansson, M.; Stahlberg, M.; Runold, M.; Nygren-Bonnier, M.; Nilsson, J.; Olshansky, B.; Bruchfeld, J.; Fedorowski, A. Long-Haul Post-COVID-19 Symptoms Presenting as a Variant of Postural Orthostatic Tachycardia Syndrome: The Swedish Experience. JACC Case Rep. 2021, 3, 573–580. [Google Scholar] [CrossRef]
- Kakamad, F.H.; Mahmood, S.O.; Rahim, H.M.; Abdulla, B.A.; Abdullah, H.O.; Othman, S.; Mohammed, S.H.; Kakamad, S.H.; Mustafa, S.M.; Salih, A.M. Post covid-19 invasive pulmonary Aspergillosis: A case report. Int. J. Surg. Case Rep. 2021, 82, 105865. [Google Scholar] [CrossRef]
- Lechien, J.R.; Hervochon, R.; Hans, S. Post-COVID-19 Kawasaki-Like Syndrome. Ear. Nose Throat J. 2021; 1455613211006011, Advance online publication. [Google Scholar] [CrossRef]
- McWilliam, M.; Samuel, M.; Alkufri, F.H. Neuropathic pain post-COVID-19: A case report. BMJ Case Rep. 2021, 14, e243459. [Google Scholar] [CrossRef]
- Morris, D.; Patel, K.; Rahimi, O.; Sanyurah, O.; Iardino, A.; Khan, N. ANCA vasculitis: A manifestation of Post-COVID-19 Syndrome. Respir. Med. Case Rep. 2021, 34, 101549. [Google Scholar] [CrossRef]
- Omololu, A.; Ojelade, B.; Ajayi, O.; Adesomi, T.; Alade, O.; Adebisi, S.; Nwadike, V. “Long COVID”: A case report of persistent symptoms in a patient with prolonged SARS-CoV-2 shedding for over 110 days. SAGE Open Med. Case Rep. 2021, 9, 2050313X211015494. [Google Scholar] [CrossRef] [PubMed]
- Taribagil, P.; Creer, D.; Tahir, H. ‘Long COVID’ syndrome. BMJ Case Rep. 2021, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Vera-Lastra, O.; Lucas-Hernández, A.; Ruiz-Montiel, J.E.; Gonzalez-Rodriguez, V.R.; Pineda-Galindo, L.F. Myopericarditis as a Manifestation of Long COVID Syndrome. Cureus 2021, 13, 19449. [Google Scholar] [CrossRef]
- Becker, R.; Möser, S.; Moser, N.; Glauser, D. Survey Participation in the Time of Corona. Surv. Res. Methods 2022, 16, 61–74. [Google Scholar] [CrossRef]
- Weir, W.; Speight, N. ME/CFS: Past, Present and Future. Healthcare; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2021. [Google Scholar]
- Petersen, E.L.; Goßling, A.; Adam, G.; Aepfelbacher, M.; Behrendt, C.-A.; Cavus, E.; Cheng, B.; Fischer, N.; Gallinat, J.; Kühn, S.; et al. Multi-organ assessment in mainly non-hospitalized individuals after SARS-CoV-2 infection: The Hamburg City Health Study COVID programme. Eur. Heart J. 2022, 43, 1124–1137. [Google Scholar] [CrossRef] [PubMed]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef] [Green Version]
- van Loenhout, J.A.; van Tiel, H.H.; van den Heuvel, J.; Vercoulen, J.H.; Bor, H.; van der Velden, K.; Paget, W.J.; Hautvast, L.A. Serious long-term health consequences of Q-fever and Legionnaires’ disease. J. Infect. 2014, 68, 527–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorowski, A. Postural orthostatic tachycardia syndrome: Clinical presentation, aetiology and management. J. Intern. Med. 2018, 285, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.M.; Wong, J.G.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.-M.; Wong, P.-C.; Tsang, K.W.; Chua, S.E. Stress and Psychological Distress among SARS Survivors 1 Year after the Outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.H.-B.; Wing, Y.-K.; Yu, M.W.-M.; Leung, C.-M.; Ma, R.C.; Kong, A.P.; So, W.Y.; Fong, S.Y.Y.; Lam, S. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: Long-term follow-up. Arch. Intern. Med. 2009, 169, 2142–2147. [Google Scholar] [CrossRef] [Green Version]
- Kumar, I.; Prakash, A.; Ranjan, M.; Chakrabarti, S.S.; Shukla, R.C.; Verma, A. Short-term follow-up HRCT Chest of COVID-19 survivors and association with persistent dyspnea. Egypt. J. Radiol. Nucl. Med. 2021, 52, 227. [Google Scholar] [CrossRef]
- Fu, Q.; Levine, B.D. Exercise and non-pharmacological treatment of POTS. Auton. Neurosci. 2018, 215, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Pasanen, T.; Tolvanen, S.; Heinonen, A.; Kujala, U.M. Exercise therapy for functional capacity in chronic diseases: An overview of meta-analyses of randomised controlled trials. Br. J. Sports Med. 2017, 51, 1459–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVID-19: Censorship and Misinformation having ‘Devastating’ Impact on Global Health Crisis [Press Release]. 2021. Available online: https://www.amnesty.org.uk/press-releases/covid-19-censorship-and-misinformation-having-devastating-impact-global-health (accessed on 15 January 2022).
- Menachemi, N.; Collum, T.H. Benefits and drawbacks of electronic health record systems. Risk Manag. Health Policy 2011, 4, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5-6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2021, 76, 405–407. [Google Scholar] [CrossRef]
- Elkan, M.; Dvir, A.; Zaidenstein, R.; Keller, M.; Kagansky, D.; Hochman, C.; Koren, R. Patient-Reported Outcome Measures After Hospitalization During the COVID-19 Pandemic: A Survey Among COVID-19 and Non-COVID-19 Patients. Int. J. Gen. Med. 2021, 14, 4829–4836. [Google Scholar] [CrossRef]
- Horowitz, E.; Abadi-Korek, I.; Shani, M.; Shemer, J. EQ-5D as a generic measure of health-related quality of life in Israel: Reliability, validity and responsiveness. Isr. Med. Assoc. J. IMAJ 2010, 12, 715–720. [Google Scholar]
- Roth, P.H.; Gadebusch-Bondio, M. The contested meaning of “long COVID”—Patients, doctors, and the politics of subjective evidence. Soc. Sci. Med. 2022, 292, 114619. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Pain | Insomnia |
| Anxiety | Pain in extremities |
| Depression | Paresthesia |
| Fatigue | Peripheral edema |
| Joint pain | Palpations |
| Shortness of breath | Diarrhea |
| Head aches | Itching |
| Nauseaand or vomiting | Erythema |
| Myalgia | Lower urinary tract symptoms |
| Gastroesophageal reflux | Lymphadenopathy |
| Cough | Edema |
| Back pain | Weight gain |
| stress | Sino-nasal congestion |
| Fever | Pain in throat |
| Swelling | Abnormal gait |
| Bleeding | Respiratory distress |
| Weight loss | Visual changes |
| Abdominal pain | Chills |
| Dizziness or vertigo | Urinary incontinence |
| Chest pain | Sleep apnea |
| Weakness | Confusion |
| Constipation | Hearing loss |
| Skin lesions | Problems with taste and smell |
| Wheezing | Difficulty in swallowing |
| Rash | Loss of appetite |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Papers which discussed patients with long COVID (and all synonyms as described in the search term section) | |
| >75% of the participants in the study were non hospitalised | >25% of participants were hospitalised |
| >75% of the participant were between the ages of 18–65 | Participants were <16 or >65 years |
| Primary research | Not primary research (i.e., reviews) |
| Physical signs and symptoms | Primarily reporting cognitive, psychological, or social signs and symptoms |
| Data could be clearly extracted | Data that could not be clearly extracted |
| Population was clearly defined | Population was not clearly defined |
| Papers written in English | Papers not written in English |
| Symptom | Number of Studies Reporting Symptom/Total Number of Studies (%) | Number of Patients with Symptom/Total Number of Patients |
|---|---|---|
| Fatigue | 51/55 (92.7%) | 21,129/162,282 |
| Shortness of Breath (SOB) | 45/55 (81.8%) | 23,109/162,282 |
| Chest Pain | 29/55 (52.7%) | 10,463/162,282 |
| Cough | 27/55 (49%) | 4678/162,282 |
| Headaches | 26/55 (42%) | 17,991/162,282 |
| Muscle Ache | 24/55 (43.6%) | 8284/162,282 |
| Joint Pain | 19/55 (34.5%) | 6778/162,282 |
| Sleep Disturbances | 11/55 (20%) | 6778/162,282 |
| Dizziness | 10/55 (18.1%) | 4285/162,282 |
| Palpation | 9/55 (16.3%) | 3261/162,282 |
| Anxiety | 8/55 (14.5%) | 173/162,282 |
| Muscle and joint pain | 8/55 (14.5%) | 7534/162,282 |
| Weakness | 2/55 (3.6%) | 3236/162,282 |
| Back pain | 2/55 (3.6%) | 4429/162,282 |
| Orthostatic Intolerance | 1/55 (1.18%) | 16/162,282 |
| Characteristics | Relevant Studies | |
|---|---|---|
| Percentage of females Number of studies with over 75% women | 64.48% 8 studies | [31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85] [35,38,44,50,52,69,78,83] |
| Mean age | 43.5 years (mean) | [15,34,35,38,40,41,42,45,47,48,49,50,51,52,54,55,56,57,61,62,64,65,67,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84] |
| Median age | 47 years (median) | [31,32,33,36,39,58,59,60,66] |
| Mean % of population were smokers with long COVID | 23.7% | [32,35,37,38,40,45,56,60,61,64,65,68,70,70,71,75,77,82] |
| Author/Country/Year | Condition Described as Part of the Long COVID Syndrome | Sample Size | Study Design |
|---|---|---|---|
| Balan, et al., USA 2021 [91] | Multisystem inflammatory sequelae. | 1 male | Case report |
| Feghali, USA 2021 [92] | Hashimoto thyroiditis, Graves’ disease, and subacute thyroiditis | 3 females | Case series |
| Johansson, Sweden, 2021 [93] | POTS—Postural Orthostatic Tachcardia Syndrome | 2 females, 1 male | Case series |
| Kakamad, Iraq, 2021 [94] | Pulmonary fungal infection | 1 male | Case report |
| Lechien, France, 2021 [95] | Kawasaki-Like Syndrome | 1 male | Case report |
| McWilliam UK, 2021 [96] | Neuropathic pain | 1 male | Case report |
| Morris, D., USA, 2021 [97] | ANCA vasculitis | 1 male | Case report |
| Omololu, Nigeria, 2021 [98] | Persistent symptoms post COVID-19 | 1 male | Case report |
| Taribagil., et al., UK, 2021 [99] | Presentation of a patient with long COVID | 1 female | Case report |
| Vera-Lastra, et al., Mexico, 2021 [100] | Fluctuating symptoms of myopericarditis | 1 male | Case Report |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kokolevich, Z.M.; Crowe, M.; Mendez, D.; Biros, E.; Reznik, J.E. Most Common Long COVID Physical Symptoms in Working Age Adults Who Experienced Mild COVID-19 Infection: A Scoping Review. Healthcare 2022, 10, 2577. https://doi.org/10.3390/healthcare10122577
Kokolevich ZM, Crowe M, Mendez D, Biros E, Reznik JE. Most Common Long COVID Physical Symptoms in Working Age Adults Who Experienced Mild COVID-19 Infection: A Scoping Review. Healthcare. 2022; 10(12):2577. https://doi.org/10.3390/healthcare10122577
Chicago/Turabian StyleKokolevich, Zoe Mass, Melissa Crowe, Diana Mendez, Erik Biros, and Jacqueline Elise Reznik. 2022. "Most Common Long COVID Physical Symptoms in Working Age Adults Who Experienced Mild COVID-19 Infection: A Scoping Review" Healthcare 10, no. 12: 2577. https://doi.org/10.3390/healthcare10122577