
Snoring Index and Neck Circumference as Predictors of Adult Obstructive Sleep Apnea

1
Department of Family Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi 622, Taiwan
2
Nature Dental Clinic, Nantou 545, Taiwan
3
Department of Urology, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi 622, Taiwan
4
Department of Family Medicine, Tainan Municipal Hospital (Managed by Show Chwan Medical Care Corporation), Tainan 701, Taiwan
*
Author to whom correspondence should be addressed.
Healthcare 2022, 10(12), 2543; https://doi.org/10.3390/healthcare10122543
Submission received: 26 October 2022
/
Revised: 12 December 2022
/
Accepted: 13 December 2022
/
Published: 15 December 2022
(This article belongs to the Topic Metabolism and Health)
Abstract
:Background. Snoring is the cardinal symptom of obstructive sleep apnea (OSA). The acoustic features of snoring sounds include intra-snore (including snoring index [SI]) and inter-snore features. However, the correlation between snoring sounds and the severity of OSA according to the apnea–hypopnea index (AHI) is still unclear. We aimed to use the snoring index (SI) and the Epworth Sleepiness Scale (ESS) to predict OSA and its severity according to the AHI among middle-aged participants referred for polysomnography (PSG). Methods. In total, 50 participants (mean age, 47.5 ± 12.6 years; BMI: 29.2 ± 5.6 kg/m2) who reported snoring and were referred for a diagnosis of OSA and who underwent a whole night of PSG were recruited. Results. The mean AHI was 30.2 ± 27.2, and the mean SI was 87.9 ± 56.3 events/hour. Overall, 11 participants had daytime sleepiness (ESS > 10). The correlation between SI and AHI (r = 0.33, p = 0.021) was significant. Univariate linear regression analysis showed that male gender, body mass index, neck circumference, ESS, and SI were associated with AHI. SI (β = 0.18, p = 0.004) and neck circumference (β = 2.40, p < 0.001) remained significantly associated with AHI by the multivariate linear regression model. Conclusion. The total number of snores per hour of sleep and neck circumference were positively associated with OSA among adults referred for PSG.
1. Introduction
Obstructive sleep apnea (OSA) syndrome is a serious sleep disorder causing excessive daytime sleepiness (EDS). The severe consequences of OSA include coronary artery diseases, diabetes mellitus, ischemic stroke, hypertension, psychiatric disorders, and all-cause mortality [1,2]. The prevalence of OSA in adults has substantially increased over the last two decades; a community-based study reported an overall prevalence of approximately 26% for mild-to-severe sleep-disordered breathing (apnea–hypopnea index [AHI] ≥ 5) among individuals aged 30–70 years, and approximately 17% of men and 9% of women aged 50–70 years had moderate-to-severe sleep-disordered breathing (AHI ≥ 15) [3].
Polysomnography (PSG) is the gold standard for the diagnosis of OSA and monitoring of snoring [4]. Under the current guidelines, AHI continues to be referred to as the primary measure of severity of OSA [5]. Severity is evaluated as follows: normal, AHI < 5; mild, 5 ≤ AHI < 15; moderate, 15 ≤ AHI < 30; and severe, AHI ≥ 30 [6]. However, PSG requires technical expertise and is labor-intensive and time-consuming. Furthermore, timely access is a problem for many patients, and single-night PSG measurement might lead to misclassification of the severity of OSA. A previous study reported that 93% of women and 82% of men with moderate-to-severe OSA did not receive a diagnosis through PSG [7]. Another study reported that the severity of OSA varies every night due to the influence of body position and rapid eye movement on sleep, and that higher variability was observed in less severe OSA [8,9]. An ideal approach to overcome this uncertainty in the severity of OSA would involve repeated measures; however, this is often not feasible owing to the inconvenience caused to participants in undergoing repeated PSG tests in a hospital or laboratory [10].
Several methods, including questionnaires and objective measures, can help determine the probability that a patient has OSA. For instance, snoring is the cardinal symptom of OSA and has been reported in 70–95% of patients with OSA [4,11]. However, the correlation between snoring and OSA is not conclusive. One systemic review reported that snoring is a relatively accurate, but not a strong and reliable, method for diagnosing OSA [12]. In addition, a systematic review reported that the clinical symptoms of nocturnal gasping and choking are the most reliable indicators of OSA, whereas snoring is not very specific [13]. However, other studies reported strong associations between the severity of snoring and OSA [14]. Snoring index (SI, the total number of snores per hour of sleep) is one of the acoustic features of snoring sounds used to predict the AHI, and is positively correlated with the AHI [15,16,17,18].
EDS is a key symptom in many patients with OSA, and the Epworth sleepiness scale (ESS) is a simple and convenient self-report questionnaire used to assess EDS among patients with OSA in a clinical setting [19]. The ESS uses an eight-item scale, with each item scored from 0 through 3, and the total ESS score ranges from 0 to 24 [20]. ESS scores > 10 represent EDS, and patients with EDS need to be evaluated for potential OSA [21].
PSG involves recording various physiological signals during sleep; snoring is one of these signals. The purpose of this current study was to explore the association between SI and the severity of OSA, according to the AHI, among patients referred for PSG.
2. Materials and Methods
2.1. Ethical Considerations
The study protocol was reviewed and approved by the institutional review board of the Tainan Municipal Hospital (Managed by Show Chwan Medical Care Corporation) (SCMH_IRB No: 1090508) and the Research Ethics Committee of the Buddhist Dalin Tzu Chi Hospital, Taiwan (No. B10901020).
2.2. Materials
Data Collection from PSG
The participants underwent PSG recording using the Embla N7000 System (Embla Inc., Broomfield, CO, USA) shown in Figure 1. The recorded data provided various physiological signals, including electrocardiographic, electroencephalographic, electrooculographic, and electromyographic signals, and oxygen saturation and respiratory airflow. AHI is defined as the average hourly number of apnea and hypopnea events, which are categorized according to severity, where 5 ≤ AHI < 15 is mild, 15 ≤ AHI < 30 is moderate, and AHI ≥ 30 is severe [5].
An external piezo-electric snoring sensor (Embla N7000 Systems; attachable) can be used with the system. When a snoring sensor is attached to a patient’s throat, it generates a signal in response to the vibrations produced during snoring. Relying on vibrations rather than actual sounds eliminates all artifacts associated with external noises (the recording procedures conducted in this study had been obeyed strictly by the same operator to our established standard operation protocol). The snoring signal is converted to an analog voltage that can be measured. The SI was defined as the vibration times per sleep hour.
All respiratory signals from the Embla N7000 system were imported into the system in European Data Format, and a new anonymized polygraphy file was created for each patient. This software automatically validated sections where the signals of the pressure cannula, sound signal, and saturation were present [22]. The formal reports from the PSG included AHI and SI.
2.3. Method
2.3.1. Design and Setting
Patients who reported snoring and were suspected of having OSA were referred for PSG test at a metropolitan regional teaching hospital in Taiwan between 1 January and 31 December 2021. Participants below 20 years of age were excluded. All patients provided written informed consent prior to enrolment.
2.3.2. Study Outcome
Snoring index (SI, the total number of snores per hour of sleep) from PSG, ESS, and demographic factors were collected to evaluate the independent factors associated with the apnea–hypopnea index, as the measures of OSA severity.
2.4. Statistical Analysis
Statistical analyses were conducted using R software version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). Two-sided p values < 0.05 were considered statistically significant. Continuous data are expressed as mean ± standard deviation (SD), and categorical variables are represented by frequency and percentage. The multivariate linear regression model was used to evaluate the independent factors associated with AHI.
3. Results
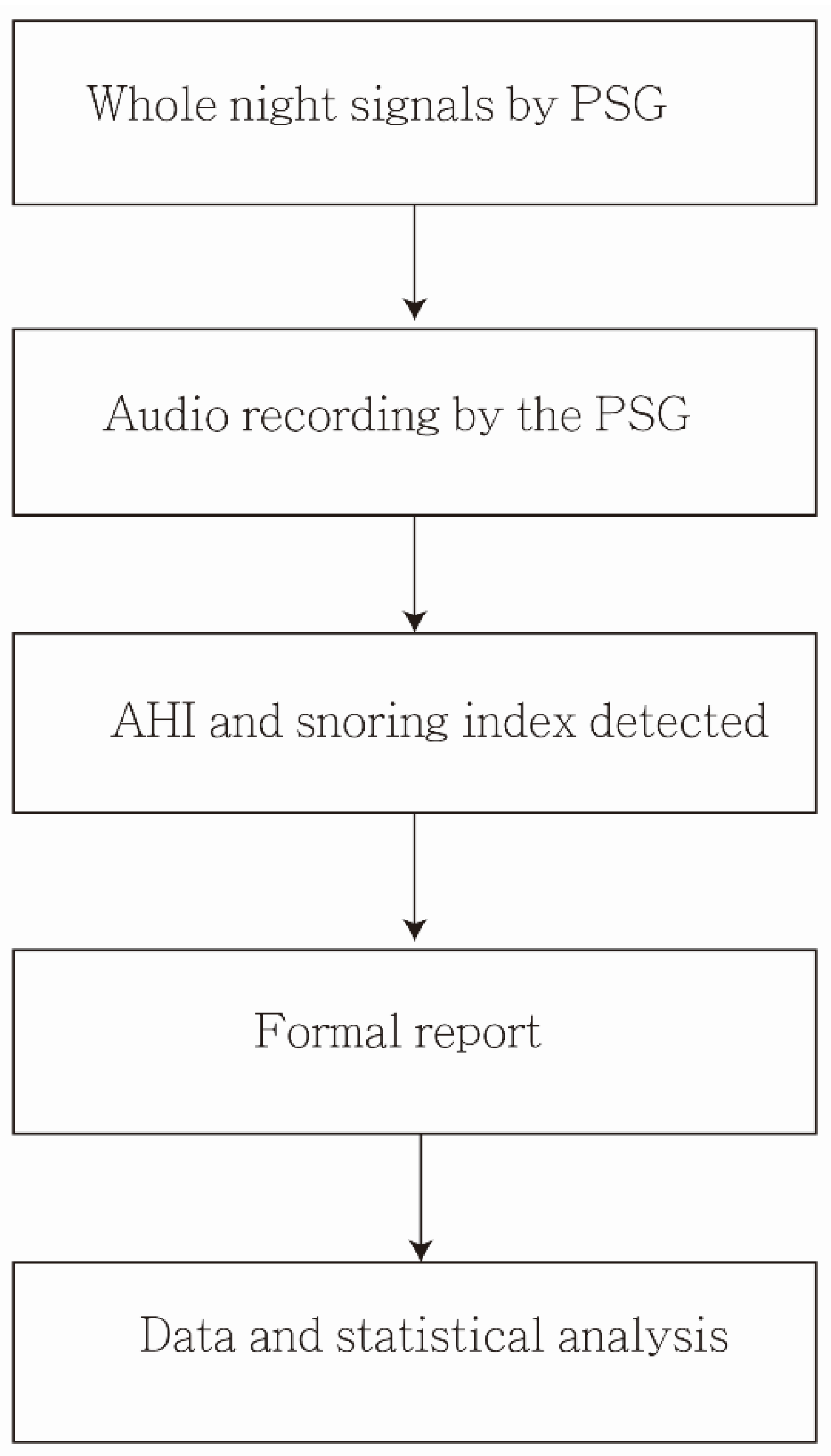
In total, 6 (12%) participants had primary snoring (AHI < 5), and 44 participants had OSA (AHI ≥ 5). The mean age of the participants was 47.5 ± 12.6 years, mean BMI was 29.2 ± 5.6 kg/m2, and mean neck circumference was 40.6 ± 5.3 cm. The mean SI was 87.9 ± 56.3 events/h, and the mean AHI was 30.2 ± 27.2. Eleven (22%) participants had EDS (ESS > 10). Additionally, values of BMI, neck circumference, and ESS were all higher in the AHI ≥ 5 group than the AHI < 5 group, which also reached statistical significance (p = 0.018, p = 0.013, and p = 0.037, respectively) (Table 1). The audio data handling and analysis was shown in Figure 2.
The mean SI for primary snoring (AHI < 5) was 89.28 ± 30.72 events/hour, and for mild, moderate, and severe OSA, it was 71.64 ± 48.07, 75.90 ± 39.99, and 106.30 ± 71.76 events/hour, respectively. No significant difference was observed in the SI by AHI score between the stratified four groups (p = 0.187) using ANOVA analysis (Table 2).
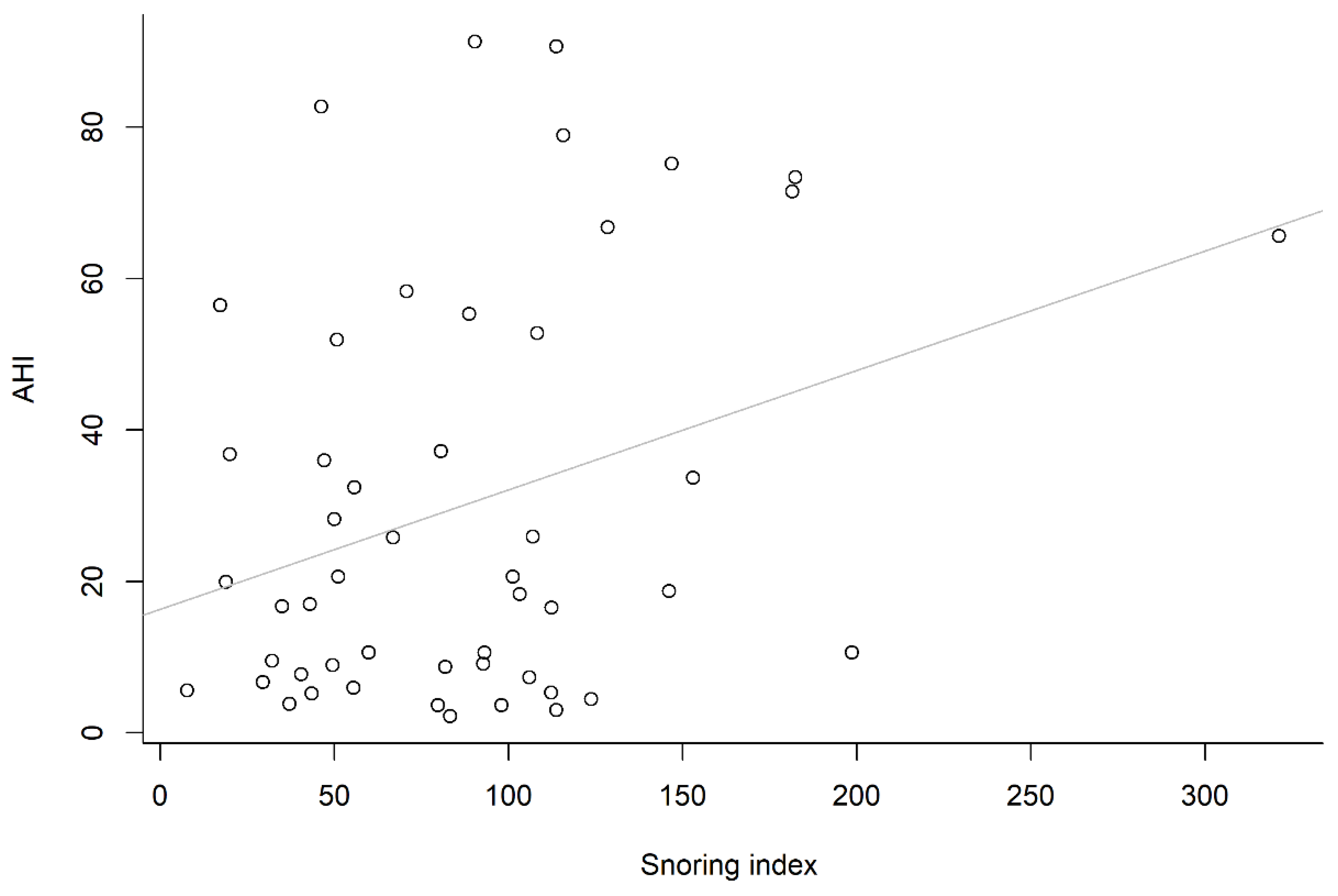
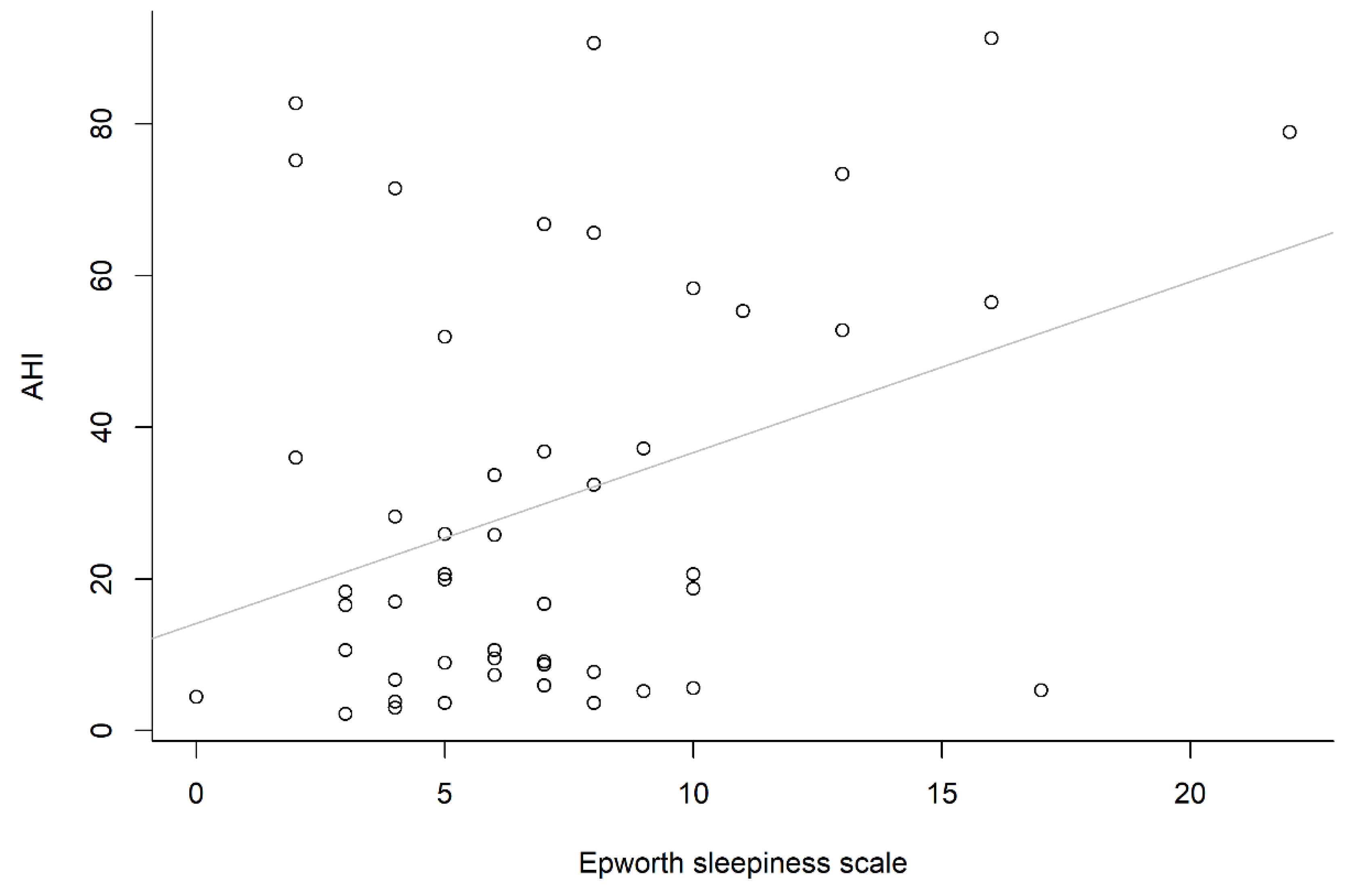
One reason for this might be the smaller number in each stratified group (n = 6, 14, 11 and 19, respectively), whereas the other might be that a higher mean value of SI was observed in the first (or fourth) group than either the second or third group. However, if we focused on the correlation between total SI and total AHI, a positively significant correlation (r = 0.33, p = 0.021) was demonstrated, and the correlation between the ESS and AHI was also significant (r = 0.35, p = 0.012). However, the correlation between the ESS and SI was not significant (r = 0.05, p = 0.717). The correlation between snoring index and apnea–hypopnea index is shown in Figure 3, and the correlation between Epworth sleepiness scale and apnea–hypopnea index is shown in Figure 4. Univariate analysis showed that gender, BMI, neck circumference, ESS, and SI were significant predictors of AHI (Table 3). Notably, a significantly positive correlation was found between neck circumference and BMI (r = 0.71, p < 0.001). Accordingly, collinearity of neck circumference and BMI has been concurred (both neck circumference and BMI were significant variables for AHI). Therefore, we shall only take one of the above variables (neck circumference or BMI) into account per multiple linear regression analysis (Model 1 or Model 2). Model 1 was better than Model 2 according to the adjusted R2 value (0.291 vs. 0.215). For each multiple linear regression analysis, only SI and neck circumference were significantly associated with AHI (Table 4).
4. Discussion
In the current study, SI and neck circumference were positively significantly correlated with AHI among adults referred for PSG. We suggested that the neck circumference for OSA might be a better parameter than BMI and ESS for OSA prediction.
The correlation between snoring and AHI has often been discussed in previous studies [10,12,13,14,15,16,17,18]. However, the findings have been inconclusive. One of the reasons for this might be the difficulty in the detection and identification of snoring. For example, Levartovsky et al. found the correlation between SI and AHI to be nonsignificant [18]. In that study, the acoustic signals were recorded using a noncontact directional microphone (RØDE, NTG-1, Silverwater, NSW, Australia) placed 1 m above the bed and connected to a digital audio recording device (Edirol R-4 Pro, Bellingham, WA, USA). Snoring was defined as breathing sound intensity > 50 dB, and SI was the total number of snores per hour of sleep. Wu found the correlation between SI and AHI to be significant [17]. In that study, the snoring burst index was defined as the number of snoring burst signal groups per hour of sleep. A burst signal group was defined as ≥3 successive bursts of signals with amplitudes exceeding the mean amplitude of all overnight snoring signals. In the current study, snoring measured through PSG and SI was defined as snoring events/h. The snoring sensor was attached to the patient’s throat, and a signal was generated in response to the vibrations that occurred during snoring. The snoring signal was then converted to an analog voltage that could be measured. We calculated the SI (total number of snores per sleep hour) from PSG data and found that the SI was correlated with AHI. The association between snoring and OSA according to the AHI is a very interesting issue for the study population and the investigators. Further study is warranted to investigate the detection of SI at home using similar measurements from PSG.
The ESS is often used clinically to assess subjective daytime sleepiness or sleep propensity in adults. The association between ESS and OSA has frequently been discussed, but no conclusion has been reached. Previous studies reported that ESS had only a poor to fair discriminatory ability to screen for OSA [20,23,24,25,26,27]. One study reported that ESS was associated with AHI among both men and women [28]. Moreover, another study reported that higher ESS item scores indicated a closer relationship with the corresponding AHI [29]. One of the possible explanations is the participant’s situational sleepiness, which influenced the results of the ESS [30]. In the current study, we found that although the correlation between ESS and AHI was significant for both men and women, it became nonsignificant after adjustments. This might be because ESS was associated with neck circumference and became nonsignificant, whereas neck circumference was a positive predictor of AHI. A previous cohort study reported that neck circumference was associated with ESS score among men [31].
Neck circumference, a proxy for upper body fat, has been shown to be associated with the risk factor for cardiovascular disease and metabolic syndrome [32,33]. In the current study, neck circumference was associated with AHI, and the mean neck circumference of middle-aged participants was 40.6 ± 5.3 cm. A previous study reported that neck circumference was a significant predictor of OSA; the neck circumference of the participants in that study was ≥17 inches [34].
A previous systemic review reported that BMI ≥ 25 kg/m2 was an important risk factor for OSA [35]. Another study showed that OSA was more common and more severe in Far East Asian men than in white men, although the value of mean BMI was lower in Far East Asian men (26.7 ± 3.8 kg/m2) than in white men (29.7 ± 5.8 kg/m2) [36]. In the current study, we found that BMI (29.2 ± 5.6 kg/m2) was a positive factor for AHI (p = 0.001) in univariate linear regression. A similar result was obtained if we used the factor of BMI to replace the neck circumference in multivariate linear regression analysis. The present study has some limitations. First, the sample size was small; only 50 participants (38 males; 12 females) were enrolled for analysis. Second, the sleep position of the participants could have affected the snoring signals. Third, the quality of the recorded signals was affected by sleep talk and sleep quality during the night. Finally, we found that individuals with primary snoring (AHI < 5) had higher SI than those with mild-to-moderate OSA (5 ≤ AHI < 30). One of the reasons could be the small number of participants (n = 6) diagnosed as having primary snoring. Further studies with more participants are warranted for a detailed investigation and to confirm our findings.
5. Conclusions
The mean number of snores per hour obtained from PSG and neck circumference were positively significantly correlated with AHI among adults. Further prospective and large-sample studies are warranted to confirm our results.
6. Patents
Predictors for OSA included snoring, male gender, older age, increased neck circumference, BMI, ESS, and a history of witnessed apneas [37]. In the current study, we suggested that the neck circumference for OSA might be a better parameter than BMI and ESS for OSA prediction.
Author Contributions
Conceptualization, J.-K.C., C.-M.L. and Y.-H.K.; Methodology, J.-K.C. and Y.-C.L.; Software, J.-K.C.; Validation, Y.-H.K. and J.-K.C.; Formal Analysis, J.-K.C.; Investigation, Y.-H.K. and J.-K.C.; Resources, Y.-H.K.; Data Curation, Y.-H.K.; Writing—Original Draft Preparation, Y.-H.K. and J.-K.C.; Writing—Review and Editing, J.-K.C., C.-M.L. and Y.-H.K.; Visualization, Y.-H.K.; Supervision, C.-M.L.; Project Administration, Y.-C.L.; Funding Acquisition, J.-K.C. J.-K.C. and C.-M.L. contributed equally. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, grant number DTCRD110(2)-E-06 and Buddhist Tzu Chi Medical Foundation, grant number TCMF-A 111-11.
Institutional Review Board Statement
The study protocol was reviewed and approved by the institutional review board of the Tainan Municipal Hospital (Managed by Show Chwan Medical Care Corporation) (SCMH_IRB No: 1090508) and the Research Ethics Committee of the Buddhist Dalin Tzu Chi Hospital, Taiwan (No. B10901020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sharafkhaneh, A.; Giray, N.; Richardson, P.; Young, T.; Hirshkowitz, M. Association of psychiatric disorders and sleep apnea in a large cohort. Sleep 2005, 28, 1405–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, N.S.; Wong, K.K.; Liu, P.Y.; Cullen, S.R.; Knuiman, M.W.; Grunstein, R.R. Sleep apnea as an independent risk factor for all-cause mortality: The Busselton Health Study. Sleep 2008, 31, 1079–1085. [Google Scholar] [PubMed] [Green Version]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–10014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abeyratne, U.R.; Wakwella, A.S.; Hukins, C. Pitch jump probability measures for the analysis of snoring sounds in apnea. Physiol. Meas. 2005, 6, 779–798. [Google Scholar] [CrossRef] [PubMed]
- Quan, S.F.; Gillin, J.C.; Littner, M.R.; Shepard, J.W. Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999, 22, 667–689. [Google Scholar]
- Epstein, L.J.; Kristo, D.; Strollo, P.J.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar]
- Young, T.; Evans, L.; Finn, L.; Palta, M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep 1997, 20, 705–706. [Google Scholar] [CrossRef]
- Eiseman, N.A.; Westover, M.B.; Ellenbogen, J.M.; Bianchi, M.T. The impact of body posture and sleep stages on sleep apnea severity in adults. J. Clin. Sleep Med. 2012, 8, 655–666A. [Google Scholar] [CrossRef]
- Stoberl, A.S.; Schwarz, E.I.; Haile, S.R.; Turnbull, C.D.; Rossi, V.A.; Stradling, J.R.; Kohler, M. Night-to-night variability of obstructive sleep apnea. J. Sleep Res. 2017, 26, 782–788. [Google Scholar] [CrossRef] [Green Version]
- Alakuijala, A.; Salmi, T. Predicting Obstructive Sleep Apnea with Periodic Snoring Sound Recorded at Home. J. Clin. Sleep Med. 2016, 12, 953–958. [Google Scholar] [CrossRef]
- Maimon, N.; Hanly, P.J. Does snoring intensity correlate with the severity of obstructive sleep apnea? J. Clin. Sleep Med. 2010, 6, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Lee, L.A.; Song, L.; Li, Y.; Peng, J.; Zhong, N.; Li, H.Y.; Zhang, X. Acoustic Analysis of Snoring in the Diagnosis of Obstructive Sleep Apnea Syndrome: A Call for More Rigorous Studies. J. Clin. Sleep Med. 2015, 11, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Myers, K.A.; Mrkobrada, M.; Simel, D.L. Does this patient have obstructive sleep apnea?: The Rational Clinical Examination systematic review. JAMA 2013, 310, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Sowho, M.; Sgambati, F.; Guzman, M.; Schneider, H.; Schwartz, A. Snoring: A source of noise pollution and sleep apnea predictor. Sleep 2020, 43, zsz305. [Google Scholar] [CrossRef] [PubMed]
- Alshaer, H.; Hummel, R.; Mendelson, M.; Marshal, T.; Bradley, T.D. Objective Relationship Between Sleep Apnea and Frequency of Snoring Assessed by Machine Learning. J. Clin. Sleep Med. 2019, 15, 463–470. [Google Scholar] [CrossRef]
- Jane, R.; Fiz, J.A.; Sola-Soler, J.; Mesquita, J.; Morera, J. Snoring analysis for the screening of Sleep Apnea Hypopnea Syndrome with a single-channel device developed using polysomnographic and snoring databases. Annu. Int. Conf. IEEE. Eng. Med. Biol. Soc. 2011, 2011, 8331–8333. [Google Scholar]
- Wu, H.T.; Pan, W.Y.; Liu, A.B.; Su, M.C.; Chen, H.R.; Tsai, I.T.; Lin, M.C.; Sun, C.K. Vibration signals of snoring as a simple severity predictor for obstructive sleep apnea. Clin. Respir. J. 2016, 10, 440–448. [Google Scholar] [CrossRef]
- Levartovsky, A.; Dafna, E.; Zigel, Y.; Tarasiuk, A. Breathing and Snoring Sound Characteristics during Sleep in Adults. J. Clin. Sleep Med. 2016, 12, 375–384. [Google Scholar] [CrossRef]
- Cho, Y.W.; Lee, J.H.; Son, H.K.; Lee, S.H.; Shin, C.; Johns, M.W. The reliability and validity of the Korean version of the Epworth sleepiness scale. Sleep Breath. 2011, 15, 377–384. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Johns, M.; Hocking, B. Daytime sleepiness and sleep habits of Australian workers. Sleep 1997, 20, 844–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glos, M.; Sabil, A.; Jelavic, K.S.; Schöbel, C.; Fietze, I.; Penzel, T. Characterization of Respiratory Events in Obstructive Sleep Apnea Using Suprasternal Pressure Monitoring. J. Clin. Sleep Med. 2018, 14, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, L.D.; Dolan, D.C. The Epworth sleepiness scale in the identification of obstructive sleep apnea. J. Nerv. Ment. Dis. 2008, 196, 429–431. [Google Scholar] [CrossRef] [PubMed]
- Borsini, E.; Blanco, M.; Schonfeld, S.; Ernst, G.; Salvado, A. Performance of Epworth Sleepiness Scale and tiredness symptom used with simplified diagnostic tests for the identification of sleep apnea. Sleep Sci. 2019, 12, 287–294. [Google Scholar]
- Randerath, W.; Bassetti, C.L.; Bonsignore, M.R.; Farre, R.; Ferini-Strambi, L.; Grote, L.; Hedner, J.; Kohler, M.; Martinez-Garcia, M.A.; Mihaicuta, S.; et al. Challenges and perspectives in obstructive sleep apnoea: Report by an ad hoc working group of the Sleep Disordered Breathing Group of the European Respiratory Society and the European Sleep Research Society. Eur. Respir. J. 2018, 52, 1702616. [Google Scholar] [CrossRef]
- Mediano, O.; Barcelo, A.; de la Pena, M.; Gozal, D.; Agustí, A.; Barbé, F. Daytime sleepiness and polysomnographic variables in sleep apnoea patients. Eur. Respir. J. 2007, 30, 110–113. [Google Scholar] [CrossRef] [Green Version]
- Sharkey, K.M.; Orff, H.J.; Tosi, C.; Harrington, D.; Roye, G.D.; Millman, R.P. Subjective sleepiness and daytime functioning in bariatric patients with obstructive sleep apnea. Sleep Breath. 2013, 17, 267–274. [Google Scholar] [CrossRef]
- Lipford, M.C.; Wahner-Roedler, D.L.; Welsh, G.A.; Mandrekar, J.; Thapa, P.; Olson, E.J. Correlation of the Epworth Sleepiness Scale and Sleep-Disordered Breathing in Men and Women. J. Clin. Sleep Med. 2019, 15, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Guo, Q.; Song, W.D.; Li, W.; Zeng, C.; Li, Y.H.; Mo, J.M.; Lu, Z.D.; Jiang, M. Weighted Epworth sleepiness scale predicted the apnea-hypopnea index better. Respir. Res. 2020, 21, 147. [Google Scholar] [CrossRef]
- Grewe, F.A.; Roeder, M.; Bradicich, M.; Schwarz, E.I.; Held, U.; Thiel, S.; Gaisl, T.; Sievi, N.A.; Kohler, M. Low repeatability of Epworth Sleepiness Scale after short intervals in a sleep clinic population. J. Clin. Sleep Med. 2020, 16, 757–764. [Google Scholar] [CrossRef]
- Cho, N.H.; Oh, T.J.; Kim, K.M.; Choi, S.H.; Lee, J.H.; Park, K.S.; Jang, H.C.; Kim, J.Y.; Lee, H.K.; Lim, S. Neck Circumference and Incidence of Diabetes Mellitus over 10 Years in the Korean Genome and Epidemiology Study (KoGES). Sci. Rep. 2015, 5, 18565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preis, S.R.; Massaro, J.M.; Hoffmann, U.; D’Agostino Sr, R.B.; Levy, D.; Robins, S.J.; Meigs, J.B.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Neck circumference as a novel measure of cardiometabolic risk: The Framingham Heart study. J. Clin. Endocrinol. Metab. 2010, 95, 3701–3710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stabe, C.; Vasques, A.C.; Lima, M.M.; Tambascia, M.A.; Pareja, J.C.; Yamanaka, A.; Geloneze, B. Neck circumference as a simple tool for identifying the metabolic syndrome and insulin resistance: Results from the Brazilian Metabolic Syndrome Study. Clin. Endocrinol. 2013, 78, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Earl, D.E.; Lakhani, S.S.; Loriaux, D.B.; Spector, A.R. Predictors of moderate to severe obstructive sleep apnea: Identification of sex differences. Sleep Breath. 2019, 23, 1151–1158. [Google Scholar] [CrossRef]
- Mitra, A.K.; Bhuiyan, A.R.; Jones, E.A. Association and Risk Factors for Obstructive Sleep Apnea and Cardiovascular Diseases: A Systematic Review. Diseases 2021, 9, 88. [Google Scholar] [CrossRef]
- Li, K.K.; Kushida, C.; Powell, N.B.; Riley, R.W.; Guilleminault, C. Obstructive sleep apnea syndrome: A comparison between Far-East Asian and white men. Laryngoscope 2000, 110, 1689–1693. [Google Scholar] [CrossRef]
- Ibrahim, A.S.; Almohammed, A.A.; Allangawi, M.H.; Sattar, H.A.A.A.; Mobayed, H.S.; Pannerselvam, B.; Philipose, M.V. Predictors of obstructive sleep apnea in snorers. Ann. Saudi Med. 2007, 27, 421–426. [Google Scholar] [CrossRef]
Figure 1.
PSG recording device: the Embla N7000 System.

Figure 2.
Block diagram of audio data handling and analysis.

Figure 3.
Positive correlation between snoring index and apnea–hypopnea index.

Figure 4.
Positive correlation between Epworth sleepiness scale and apnea–hypopnea index.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Demographic characteristics of participants.
| Variables | Value | AHI < 5 | AHI ≥ 5 | p |
|---|---|---|---|---|
| n (male/female) | 50 (38/12) | 16 (4/12) | 44 (34/10) | 0.621 |
| Age, year | 47.5 ± 12.6 | 47.8 ± 9.6 | 45.4 ± 13.0 | 0.663 |
| BMI | 29.2 ± 5.6 | 24.5 ± 4.3 | 29.8 ± 5.5 | 0.018 |
| Neck circumference, cm | 40.6 ± 5.3 | 36.5 ± 2.4 | 41.2 ± 5.3 | 0.013 |
| Hypertension, yes | 8 | 0 | 8 | 1 |
| Diabetes, yes | 0 | 0 | 0 | - |
| Operation for snore | 6 | 1 | 5 | 0.363 |
| Education level * | 0.217 | |||
| Graduate school | 7 | 0 | 7 | |
| College | 20 | 4 | 16 | |
| others | 12 | 0 | 12 | |
| ESS (score > 10) [daytime sleepiness] | 7.1 ± 4.3 | 4 ± 2.6 | 7.5 ± 4.3 | 0.037 |
| Snoring index, events/sleep hour | 87.9 ± 56.3 | 89.3 ± 30.7 | 87.7 ± 59.1 | 0.633 |
| AHI score | 30.2 ± 27.2 | 3.4 ± 0.8 | 33.8 ± 27.1 | <0.001 |
Abbreviation: AHI, apnea–hypopnea index; BMI, body mass index; ESS, Epworth sleepiness scale. Education level *, missing data n = 11.
Table 2.
Distribution of snoring index by the apnea–hypopnea index score.
| AHI < 5 | 5 ≤ AHI < 15 | 15 ≤ AHI < 30 | AHI ≥ 30 | p | |
|---|---|---|---|---|---|
| N | 6 | 14 | 11 | 19 | |
| Snoring index * | 89.28 ± 30.72 | 71.64 ± 48.07 | 75.90 ± 39.99 | 106.30 ± 71.76 | 0.187 |
Snoring index *: snoring events per sleep hour.
Table 3.
Univariate linear regression for the snoring index, Epworth sleepiness scale, and apnea–hypopnea index.
Table 3.
Univariate linear regression for the snoring index, Epworth sleepiness scale, and apnea–hypopnea index.
| Snoring Index | ESS | AHI | ||||
|---|---|---|---|---|---|---|
| Variable | β | p | β | p | β | p |
| Male vs. female | 4.39 | 0.816 | 1.15 | 0.424 | 18.86 | 0.035 |
| Age | −0.23 | 0.723 | −0.06 | 0.245 | −0.31 | 0.317 |
| BMI (kg/m2) | 2.26 | 0.114 | 0.22 | 0.045 | 2.13 | 0.001 |
| Neck circumference (cm) | −1.05 | 0.499 | 0.28 | 0.015 | 2.21 | 0.002 |
| ESS | 0.691 | 0.717 | 2.25 | 0.012 | ||
| Snoring index | - | 0.004 | 0.717 | 0.16 | 0.021 | |
| AHI | 0.67 | 0.021 | 0.06 | 0.012 | ||
Abbreviation: AHI, apnea–hypopnea index; BMI, body mass index; ESS, Epworth sleepiness scale.
Table 4.
Multiple linear regression for the apnea–hypopnea index.
| Covariates | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
|---|---|---|---|---|---|---|
| Intercept | −83.22 | −34.37 | −81.52 | −78.56 | −73.09 | −69.40 |
| (0.003) | (0.066) | (0.005) | (0.021) | (0.032) | (0.039) | |
| Snoring index, events/sleep hour | 0.18 | 0.12 | 0.17 | 0.17 | 0.15 | 0.14 |
| (0.004) | (0.072) | (0.012) | (0.013) | (0.033) | (0.043) | |
| Neck circumference, cm | 2.40 | 2.16 | 2.20 | 1.46 | 1.05 | |
| (<0.001) | (0.029) | (0.033) | (0.222) | (0.381) | ||
| Body mass index | 1.86 | 0.31 | 0.23 | 0.77 | 0.83 | |
| (0.005) | (0.735) | (0.830) | (0.505) | (0.465) | ||
| Age | −0.05 | 0.03 | 0.05 | |||
| (0.868) | (0.993) | (0.860) | ||||
| Gender male vs. female | 10.88 | 11.29 | ||||
| (0.239) | (0.215) | |||||
| ESS | 1.30 | |||||
| (0.123) | ||||||
| Adjusted R-squared | 0.291 | 0.215 | 0.277 | 0.261 | 0.268 | 0.292 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chiang, J.-K.; Lin, Y.-C.; Lu, C.-M.; Kao, Y.-H. Snoring Index and Neck Circumference as Predictors of Adult Obstructive Sleep Apnea. Healthcare 2022, 10, 2543. https://doi.org/10.3390/healthcare10122543
AMA Style
Chiang J-K, Lin Y-C, Lu C-M, Kao Y-H. Snoring Index and Neck Circumference as Predictors of Adult Obstructive Sleep Apnea. Healthcare. 2022; 10(12):2543. https://doi.org/10.3390/healthcare10122543
Chicago/Turabian StyleChiang, Jui-Kun, Yen-Chang Lin, Chih-Ming Lu, and Yee-Hsin Kao. 2022. "Snoring Index and Neck Circumference as Predictors of Adult Obstructive Sleep Apnea" Healthcare 10, no. 12: 2543. https://doi.org/10.3390/healthcare10122543
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.