
Information Security Behavior in Health Information Systems: A Review of Research Trends and Antecedent Factors
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Data Items and Synthesis
3. Results
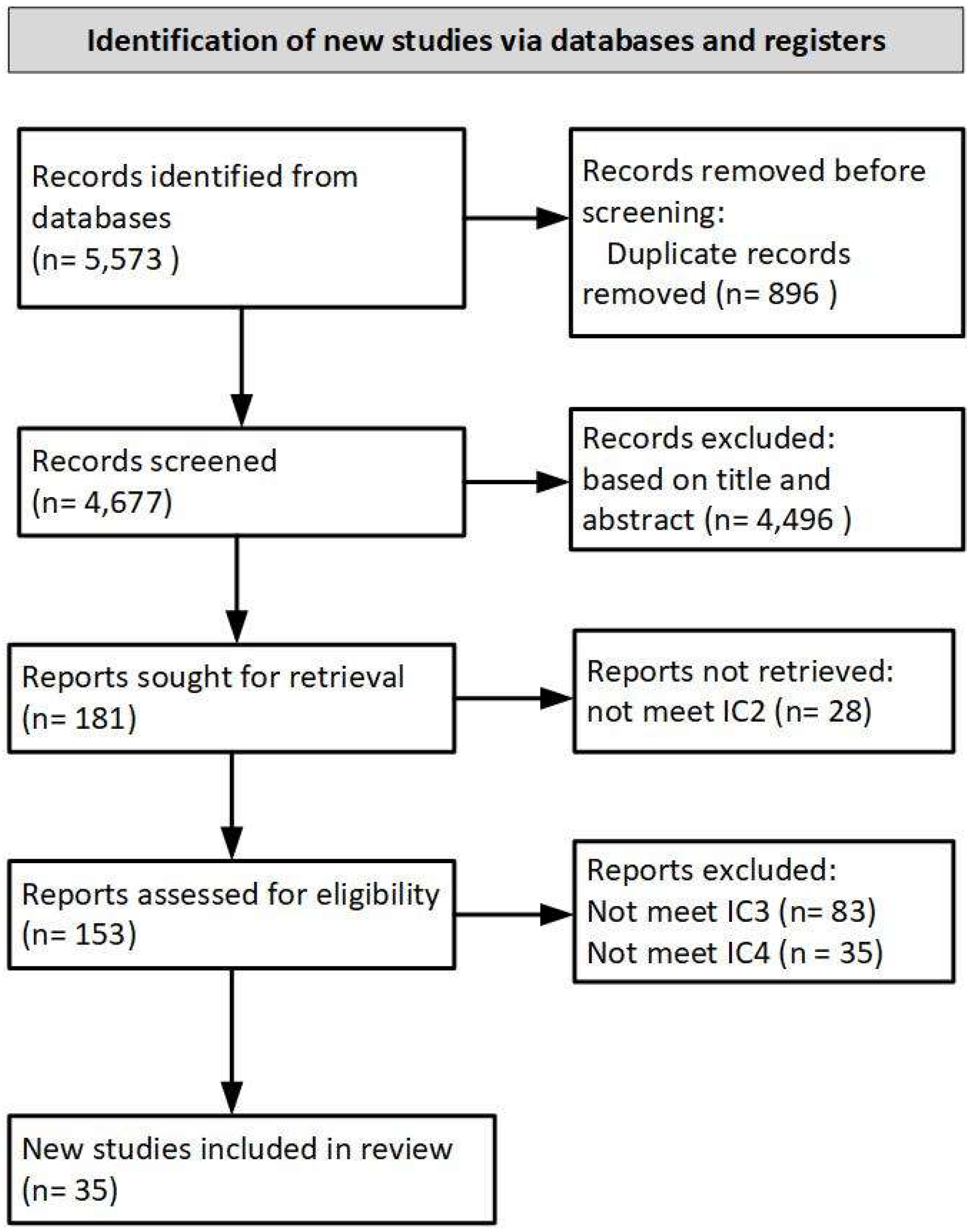
3.1. Study Selection
3.2. Study Characteristics
3.3. Security Threat Model
3.4. Antecedent Factors of Security Behavior
3.4.1. Individual Factors
3.4.2. Organizational Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humaidi, N.; Balakrishnan, V. Indirect effect of management support on users’ compliance behaviour towards information security policies. Health Inf. Manag. J. 2018, 47, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Sardi, A.; Rizzi, A.; Sorano, E.; Guerrieri, A. Cyber Risk in Health Facilities: A Systematic Literature Review. Sustainability 2020, 12, 7002. [Google Scholar] [CrossRef]
- Mathews, A.W.; Yadron, D. Health Insurer Anthem Hit by Hackers. Available online: https://www.wsj.com/articles/health-insurer-anthem-hit-by-hackers-1423103720 (accessed on 8 January 2020).
- Weise, E. Massive Breach at Health Care Company Anthem Inc. Available online: https://www.usatoday.com/story/tech/2015/02/04/health-care-anthem-hacked/22900925/ (accessed on 8 January 2020).
- Info Security. Eight NHS Laptops—One with 8.6 m Patient Records—Go Missing. Available online: https://www.infosecurity-magazine.com/news/eight-nhs-laptops-one-with-86m-patient-records-go/ (accessed on 8 January 2020).
- CBC. LifeLabs Pays Ransom after Cyberattack Exposes Information of 15 Million Customers in B.C. and Ontario. Available online: https://www.cbc.ca/news/canada/british-columbia/lifelabs-cyberattack-15-million-1.5399577 (accessed on 8 January 2020).
- Kwang, K. Singapore Health System Hit by ‘Most Serious BREACH of Personal Data’ in Cyberattack; PM Lee’s Data Targeted. Available online: https://www.channelnewsasia.com/news/singapore/singhealth-health-system-hit-serious-cyberattack-pm-lee-target-10548318 (accessed on 8 January 2020).
- Yusof, N. Personal Data of 808,000 Blood Donors Compromised for Nine Weeks; HSA Lodges Police Report. Available online: https://www.todayonline.com/singapore/personal-data-808000-blood-donors-compromised-nine-weeks-hsa-lodges-police-report (accessed on 8 January 2020).
- HIPAA. Journal Analysis of 2018 Healthcare Data Breaches. Available online: https://www.hipaajournal.com/analysis-of-healthcare-data-breaches/ (accessed on 21 December 2019).
- Agaku, I.T.; Adisa, A.O.; Ayo-yusuf, O.A.; Connolly, G.N. Concern about security and privacy, and perceived control over collection and use of health information are related to withholding of health information from healthcare providers. J. Am. Med. Inform. Assoc. 2014, 21, 374–378. [Google Scholar] [CrossRef] [Green Version]
- Box, D.; Pottas, D. A model for information security compliant behaviour in the healthcare context. Procedia Technol. 2014, 16, 1462–1470. [Google Scholar] [CrossRef] [Green Version]
- Coventry, L.; Branley, D. Cybersecurity in healthcare: A narrative review of trends, threats and ways forward. Maturitas 2018, 113, 48–52. [Google Scholar] [CrossRef]
- Roer, K.; Petrič, G.; Eriksen, A.; Huisman, J.; Smothers, R.L.; Carpenter, P. Measure to Improve: Security Culture Report 2020. 2020. Available online: https://www.knowbe4.com/hubfs/Security-Culture-Report.pdf (accessed on 10 November 2020).
- ISO 27799; Health Informatics—Information Security Management in Health Using ISO/IEC 27002. International Standard Organization: Geneva, Switzerland, 2016.
- Williams, P.A.H. In a “trusting” environment, everyone is responsible for information security. Inf. Secur. Tech. Rep. 2008, 13, 207–215. [Google Scholar] [CrossRef]
- Dimkov, T.; Pieters, W.; Hartel, P. Laptop Theft: A Case Study on the Effectiveness of Security Mechanisms in Open Organizations. In Proceedings of the 17th ACM Conference on Computer and Communication Security, Chicago, IL, USA, 4–8 October 2010; pp. 666–668. [Google Scholar] [CrossRef]
- Laric, M.V.; Pitta, D.A.; Katsanis, L.P. Consumer concerns for healthcare information privacy: A comparison of US and Canadian perspectives. Res. Healthc. Financ. Manag. 2009, 12, 93–111. [Google Scholar]
- Sittig, D.F.; Singh, H. Legal, Ethical, and Financial Dilemmas in Electronic Health Record Adoption and Use. Pediatrics 2011, 127, e1042–e1047. [Google Scholar] [CrossRef] [Green Version]
- Chaet, D.; Clearfield, R.; Sabin, J.E.; Skimming, K. Ethical practice in Telehealth and Telemedicine. J. Gen. Intern. Med. 2017, 32, 1136–1140. [Google Scholar] [CrossRef] [Green Version]
- Layman, E.J. Ethical issues and the electronic health record. Health Care Manag. 2008, 27, 165–176. [Google Scholar] [CrossRef]
- de Roulet, D.; Scherrer, J.-R. Technical means for securing health information. Int. J. Biomed. Comput. 1996, 43, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Alumaran, S.; Bella, G.; Chen, F. The role and impact of cultural dimensions on information systems security in Saudi Arabia National Health Service. Int. J. Comput. Appl. 2015, 112, 21–28. [Google Scholar]
- Kolkowska, E.; Karlsson, F.; Hedström, K. Towards analysing the rationale of information security non-compliance: Devising a Value-Based Compliance analysis method. J. Strateg. Inf. Syst. 2017, 26, 39–57. [Google Scholar] [CrossRef] [Green Version]
- Hedström, K.; Kolkowska, E.; Karlsson, F.; Allen, J.P. Value conflicts for information security management. J. Strateg. Inf. Syst. 2011, 20, 373–384. [Google Scholar] [CrossRef]
- Fernández-Alemán, J.L.; Sánchez-Henarejos, A.; Toval, A.; Sánchez-García, A.B.; Hernández-Hernández, I.; Fernandez-Luque, L. Analysis of health professional security behaviors in a real clinical setting: An empirical study. Int. J. Med. Inform. 2015, 84, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Brady, J.W. Securing health care: Assessing factors that affect HIPAA security compliance in academic medical centers. In Proceedings of the 2011 44th Hawaii International Conference on System Sciences, Kauai, HI, USA, 4–7 January 2011; IEEE: Piscataway, NJ, USA, 2011; Volume 44, pp. 1–10. [Google Scholar] [CrossRef]
- Shahani, A. The Black Market for Stolen Health Care Data. Available online: https://www.npr.org/sections/alltechconsidered/2015/02/13/385901377/the-black-market-for-stolen-health-care-data (accessed on 8 January 2020).
- Rinehart-Thompson, L.A. Introduction to Health Information Privacy and Security, 2nd ed.; American Health Information Management Association (AHIMA): Chicago, IL, USA, 2018; ISBN 978-1-58426-588-7. [Google Scholar]
- Ashford, W. Most Healthcare Organisations Have Been Breached, Report Shows. Available online: https://www.computerweekly.com/news/252436215/Most-healthcare-organisations-have-been-breached-report-shows (accessed on 21 December 2019).
- Verizon. 2019 Verizon Data Breach Investigation Report; Verizon: New York, NY, USA, 2019. [Google Scholar]
- Verizon. Protected Health Information Data Breach Report. Available online: https://enterprise.verizon.com/resources/reports/protected_health_information_data_breach_report.pdf (accessed on 21 December 2019).
- Van Deursen, N.; Buchanan, W.J.; Duff, A. Monitoring information security risks within health care. Comput. Secur. 2013, 37, 31–45. [Google Scholar] [CrossRef]
- Albarrak, A.I. Evaluation of users information security practices at King Saud University hospitals. Glob. Bus. Manag. Res. 2011, 3, 1–6. [Google Scholar]
- Bulgurcu, B.; Cavusoglu, H. Benbasa Information security policy compliance: An empirical study of rationality-based beliefs and information security awareness. MIS Q. 2010, 34, 523–548. [Google Scholar] [CrossRef] [Green Version]
- Guo, K.H. Security-related behavior in using information systems in the workplace: A review and synthesis. Comput. Secur. 2013, 32, 242–251. [Google Scholar] [CrossRef]
- Da Veiga, A.; Eloff, J.H.P. A framework and assessment instrument for information security culture. Comput. Secur. 2010, 29, 196–207. [Google Scholar] [CrossRef]
- Padayachee, K. Taxonomy of compliant information security behavior. Comput. Secur. 2012, 31, 673–680. [Google Scholar] [CrossRef]
- Rezaeibagha, F.; Win, K.T.; Susilo, W. A systematic literature review on security and privacy of electronic health record systems: Technical perspectives. Health Inf. Manag. J. 2013, 44, 23–38. [Google Scholar] [CrossRef]
- Fernández-Alemán, J.L.; Señor, I.C.; Ángel, P.; Lozoya, O.; Toval, A. Security and privacy in electronic health records: A systematic literature review. J. Biomed. Inform. J. 2013, 46, 541–562. [Google Scholar] [CrossRef]
- Alhogail, A.; Mirza, A. Information security culture: A definition and a literature review. In Proceedings of the 2014 World Congress on Computer Applications and Information Systems, WCCAIS, Hammamet, Tunisia, 17–19 January 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 1–7. [Google Scholar] [CrossRef]
- Karlsson, F.; Åström, J.; Karlsson, M. Information security culture—State-of-the-art review between 2000 and 2013. Inf. Comput. Secur. 2015, 23, 246–285. [Google Scholar] [CrossRef]
- Lebek, B.; Uffen, J.; Breitner, M.H.; Neumann, M.; Hohler, B. Employees’ information security awareness and behavior: A literature review. In Proceedings of the Annual Hawaii International Conference on System Sciences, Wailea, Maui, 7–10 January 2013; pp. 2978–2987. [Google Scholar] [CrossRef]
- Glaspie, H.W.; Karwowski, W. Human Factors in Information Security Culture: A Literature Review. In Advance in Intelligent Systems and Computing; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; Volume 593, pp. 269–280. [Google Scholar] [CrossRef]
- Nasir, A.; Arshah, R.A.; Hamid, M.R.A.; Fahmy, S. An analysis on the dimensions of information security culture concept: A review. J. Inf. Secur. Appl. 2019, 44, 12–22. [Google Scholar] [CrossRef]
- Mahfuth, A.; Yussof, S.; Abu Baker, A.; Ali, N. A Systematic Literature Review: Information Security Culture. In Proceedings of the International Conference on Research and Innovation in Information Systems (ICRIIS), Seoul, Republic of Korea, 16–17 July 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Lebek, B.; Uffen, J.; Neumann, M.; Hohler, B.; Breitner, M.H. Information security awareness and behavior: A theory-based literature review. Manag. Res. Rev. 2014, 37, 1049–1092. [Google Scholar] [CrossRef] [Green Version]
- Sherif, E.; Furnell, S.; Clarke, N. An identification of variables influencing the establishment of information security culture. In Human Aspects of Information Security, Privacy, and Trust. HAS 2015; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2015; Volume 9190, pp. 436–448. [Google Scholar] [CrossRef]
- Page, B.B. Exploring organizational culture for information security in healthcare organizations: A literature review. In Proceedings of the Portland International Conference on Management of Engineering and Technology (PICMET 2017), Portland, OR, USA, 9–13 July 2017. [Google Scholar] [CrossRef]
- Yeng, P.K.; Szekeres, A.; Yang, B.; Snekkenes, E.A. Mapping the psychosocialcultural aspects of healthcare professionals’ information security practices: Systematic mapping study. JMIR Hum. Factors 2021, 8, e17604. [Google Scholar] [CrossRef] [PubMed]
- Liginlal, D.; Sim, I.; Khansa, L. Paul Fearn HIPAA Privacy Rule compliance: An interpretive study using Norman’s action theory. Comput. Secur. 2012, 31, 206–220. [Google Scholar] [CrossRef]
- Pathania, A.; Rasool, G. Investigating power styles and behavioural compliance for effective hospital administration: An application of AHP. Int. J. Health Care Qual. Assur. 2019, 32, 958–977. [Google Scholar] [CrossRef]
- von Solms, B.; von Solms, R. Cybersecurity and information security—What goes where? Inf. Comput. Secur. 2018, 26, 2–9. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 89. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handayani, P.W.; Hidayanto, A.N.; Budi, I. User acceptance factors of hospital information systems and related technologies: Systematic review. Inform. Health Soc. Care 2018, 43, 401–426. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Aliyu, A.; Evans, M.; Luo, C. Health Care Cybersecurity Challenges and Solutions Under the Climate of COVID-19: Scoping Review. J. Med. Internet Res. 2021, 23, e21747. [Google Scholar] [CrossRef]
- Alanazi, S.T.; Anbar, M.; Ebad, S.A.; Karuppayah, S.; Al-Ani, H.A. Theory-based model and prediction analysis of information security compliance behavior in the Saudi healthcare sector. Symmetry 2020, 12, 1544. [Google Scholar] [CrossRef]
- Dong, K.; Ali, R.F.; Dominic, P.D.D.; Ali, S.E.A. The effect of organizational information security climate on information security policy compliance: The mediating effect of social bonding towards healthcare nurses. Sustainability 2021, 13, 2800. [Google Scholar] [CrossRef]
- World Population Review. Developing Countries. Available online: https://worldpopulationreview.com/country-rankings/developing-countries (accessed on 30 March 2022).
- Jalali, M.S.; Bruckes, M.; Westmattelmann, D.; Schewe, G. Why employees (still) click on phishing links: Investigation in hospitals. J. Med. Internet Res. 2022, 22, e16775. [Google Scholar] [CrossRef]
- Johnston, A.C.; Warkentin, M. Information privacy compliance in the healthcare industry. Inf. Manag. Comput. Secur. 2008, 16, 5–19. [Google Scholar] [CrossRef] [Green Version]
- Mussa, C.; Cohen, M. Prudent access control behavioral intention: Instrument development and validation in a healthcare environment. In Proceedings of the Americas Conference on Information Systems (AMCIS), Chicago, IL, USA, 15–17 August 2013; Volume 19, pp. 2820–2830. [Google Scholar]
- Samhan, B. Security behaviors of healthcare providers using HIT outside of work: A technology threat avoidance perspective. In Proceedings of the International Conference on Information and Communication Systems, (ICICS), Irbid, Jordan, 4–6 April 2017; IEEE: Piscataway, NJ, USA, 2017; Volume 8, pp. 342–347. [Google Scholar] [CrossRef]
- Park, E.H.; Kim, J.; Wiles, L.L.; Park, Y.S. Factors affecting intention to disclose patients’ health information. Comput. Secur. 2018, 87, 101340. [Google Scholar] [CrossRef]
- Alexandrou, A.; Chen, L.-C. A security risk perception model for the adoption of mobile devices in the healthcare industry. Secur. J. 2019, 32, 410. [Google Scholar] [CrossRef]
- Kessler, S.R.; Pindek, S.; Kleinman, G.; Andel, S.A.; Spector, P.E. Information security climate and the assessment of information security risk among healthcare employees. Health Inform. J. 2020, 26, 461–473. [Google Scholar] [CrossRef] [PubMed]
- Tazkarji, M.Y. The Effect of Patient Centeredness on Nurses’ Security Policy Compliance. In Proceedings of the AMCIS 2020, Virtual Conference, 10–14 August 2020. [Google Scholar]
- Sarkar, S.; Vance, A.; Ramesh, B.; Demestihas, M.; Wu, D.T. The influence of professional subculture on information security policy violations: A field study in a healthcare context. Inf. Syst. Res. 2020, 31, 1240–1259. [Google Scholar] [CrossRef]
- Kuo, K.M.; Ma, C.C.; Alexander, J.W. How do patients respond to violation of their information privacy? Health Inf. Manag. J. 2014, 43, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.-C.; Kuo, K.-M.; Alexander, J.W. A survey-based study of factors that motivate nurses to protect the privacy of electronic medical records. BMC Med. Inform. Decis. Mak. 2015, 16, 13. [Google Scholar] [CrossRef]
- Sher, M.-L.; Talley, P.C.; Yang, C.-W.; Kuo, K.-M. Compliance with electronic medical records privacy policy: An empirical investigation of hospital information technology staff. Inq. J. Health Care Organ. Provis. Financ. 2017, 54. [Google Scholar] [CrossRef] [Green Version]
- Sher, M.-L.; Talley, P.C.; Cheng, T.-J.; Kuo, K.-M. How can hospitals better protect the privacy of electronic medical records? Perspectives from staff members of health information management departments. Health Inf. Manag. J. 2017, 46, 87–95. [Google Scholar] [CrossRef]
- Kuo, K.; Talley, P.C.; Lin, D.M. Hospital Staff’s Adherence to Information Security Policy: A Quest for the Antecedents of Deterrence Variables. Inq. J. Health Care Organ. Provis. Financ. 2021, 58. [Google Scholar] [CrossRef]
- Humaidi, N.; Balakrishnan, V. The Moderating effect of working experience on health information system security policies compliance behaviour. Malays. J. Comput. Sci. 2015, 28, 70–92. [Google Scholar]
- Humaidi, N.; Balakrishnan, V.; Shahrom, M. Exploring user’s compliance behavior towards Health Information System security policies based on extended Health Belief Model. In Proceedings of the 2014 IEEE Conference on e-Learning, e-Management and e-Services (IC3e), Hawthorne, VIC, Australia, 10–12 December 2014; pp. 30–35. [Google Scholar] [CrossRef]
- Yang, C.G.; Lee, H.J. A study on the antecedents of healthcare information protection intention. Inf. Syst. Front. 2016, 18, 253–263. [Google Scholar] [CrossRef]
- Park, E.H.; Kim, J.; Park, Y.S. The role of information security learning and individual factors in disclosing patients’ health information. Comput. Secur. 2017, 65, 64–76. [Google Scholar] [CrossRef]
- Lee, E.; Seomun, G. Structural model of the healthcare information security behavior of nurses applying protection motivation theory. Int. J. Environ. Res. Public Health 2021, 18, 2084. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, E.H.; Park, Y.S.; Chun, K.H.; Wiles, L.L. Prosocial rule breaking on health information security at healthcare organisations in South Korea. Inf. Syst. J. 2022, 32, 164–191. [Google Scholar] [CrossRef]
- Foth, M. Factors influencing the intention to comply with data protection regulations in hospitals: Based on gender differences in behaviour and deterrence. Eur. J. Inf. Syst. 2016, 25, 91–109. [Google Scholar] [CrossRef]
- Foth, M.; Schusterschitz, C.; Flatscher-Thöni, M. Technology acceptance as an influencing factor of hospital employees’ compliance with data-protection standards in Germany. J. Public Health 2012, 20, 253–268. [Google Scholar] [CrossRef]
- Altamimi, S.; Renaud, K.; Storer, T. “I do it because they do it”: Social-Neutralisation in Information Security Practices of Saudi Medical. In Risks and Security of Internet and Systems. CRiSIS 2019; Kallel, S., Cuppens, F., Cuppens-Boulahia, N., Hadj Kacem, A., Eds.; Springer Nature Switzerland: Hammamet, Tunisia, 2020; Volume 1, pp. 227–243. [Google Scholar] [CrossRef] [Green Version]
- Coventry, L.; Branley-Bell, D.; Sillence, E.; Magalini, S.; Mari, P.; Magkaranaraki, A.; Anastasopoulou, K. Cyber-Risk in Healthcare: Exploring Facilitators and Barriers to Secure Behaviour. In HCI for Cybersecurity, Privacy and Trust. HCII 2020; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2020; pp. 105–122. ISBN 9783030503093. [Google Scholar] [CrossRef]
- Box, D.; Pottas, D. Improving information security behaviour in the healthcare context. Procedia Technol. 2013, 9, 1093–1103. [Google Scholar] [CrossRef] [Green Version]
- Fauzi, M.A.; Yeng, P.; Yang, B.; Rachmayani, D. Examining the link between stress level and cybersecurity practices of hospital staff in Indonesia. In Proceedings of the 16th International Conference on Availability, Reliability and Security, Vienna, Austria, 17–20 August 2021; pp. 1–8. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Straub, D.W.; Welke, R.J. Coping with Systems Risk: Security Planning Models for Management Decision Making1. MIS Q. 1998, 22, 441–469. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Herath, T.; Rao, H.R. Encouraging information security behaviors in organizations: Role of penalties, pressures and perceived effectiveness. Decis. Support Syst. 2009, 47, 154–165. [Google Scholar] [CrossRef]
- Davis, F.D. Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Samy, G.N.; Ahmad, R.; Ismail, Z. Security threats categories in healthcare information systems. Health Inform. J. 2010, 16, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Bakkar, M.; Alazab, A. Information Security: Definitions, Threats and Management in Dubai Hospitals Context. In Proceedings of the 2019 Cybersecurity and Cyberforensics Conference (CCC), Melbourne, Australia, 8–9 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 152–159. [Google Scholar] [CrossRef]
- Landry, J.P.; Pardue, J.H.; Johnsten, T.; Campbell, M.; Landry, J.; Pardue, H.; Campbell, M. A Threat Tree for Health Information Security and Privacy A Threat Tree for Health Information Security and Privacy. In Proceedings of the AMCIS 2011, Detroit, MI, USA, 4–8 August 2011. [Google Scholar]
- Kuppusamy, P.; Samy, G.N.; Maarop, N.; Magalingam, P.; Kamaruddin, N.; Shanmugam, B.; Perumal, S. Systematic Literature Review of Information Security Compliance Behaviour Theories. In Journal of Physics: Conference Series; Universiti Teknologi Malaysia: Kuala Lumpur, Malaysia, 2020; Volume 1551. [Google Scholar] [CrossRef]
- Pollini, A.; Callari, T.C.; Tedeschi, A.; Ruscio, D.; Save, L.; Chiarugi, F.; Guerri, D. Leveraging human factors in cybersecurity: An integrated methodological approach. Cogn. Technol. Work 2022, 24, 371–390. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.W. A protection motivation theory of fear appeals and attitude change1. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, P.; Dharanikota, S.; Mirzaei, T. The role of patient engagement in patient-centric health information exchange (HIE) initiatives: An empirical study in the United States. Inf. Technol. People, 2021; ahead of printing. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Country | Frequency | Citation |
|---|---|---|---|
| Developed country | United States | 11 | [26,50,60,61,62,63,64,65,66,67,68] |
| Taiwan | 5 | [69,70,71,72,73] | |
| Republic of Korea | 4 | [1,58,74,75] | |
| Germany | 4 | [76,77,78,79] | |
| Malaysia | 2 | [80,81] | |
| Saudi Arabia | 2 | [57,82] | |
| Norway | 1 | [49] | |
| Spain | 1 | [25] | |
| Ireland | 1 | [83] | |
| Italy | 1 | [83] | |
| Greece | 1 | [83] | |
| Developing country | South Africa | 2 | [11,84] |
| India | 1 | [51] | |
| Indonesia | 1 | [85] |
| Type of Organization | Frequency | Citation |
|---|---|---|
| Hospitals only | 23 | [1,25,49,51,57,58,60,63,67,68,69,70,71,72,74,75,76,78,80,81,82,84,85] |
| Hospitals and other providers (clinics, health centers, etc.) | 5 | [61,65,66,73,83] |
| Healthcare organizations (unspecified) | 3 | [11,50,79] |
| Nursing schools | 2 | [64,77] |
| Academic medical centers | 2 | [26,62] |
| Respondents | Frequency | Citation |
|---|---|---|
| Clinical staff (physicians, nurses, pharmacists, etc.) | 25 | [1,11,25,49,57,58,60,61,62,63,65,66,67,68,70,73,74,75,76,78,80,81,83,84,85] |
| Non-clinical staff (Administration staff, top-level management, IT staff, etc.) | 21 | [1,11,25,26,50,51,57,60,61,65,71,72,73,74,75,76,80,81,82,83,85] |
| Temporary staff (nursing students, interns) | 5 | [64,65,77,79,82] |
| Patients | 1 | [69] |
| Research Method | Frequency | Citation |
|---|---|---|
| Quantitative (survey, experiment) | 26 | [1,25,26,57,58,60,61,62,63,64,65,66,69,70,71,72,73,74,75,76,77,78,79,80,81,85] |
| Qualitative (interview) | 3 | [50,82,83] |
| Literature review | 4 | [11,67,84,85] |
| Mixed methods (interview and survey) | 2 | [51,68] |
| Source | Name of Publication | Frequency |
|---|---|---|
| Journal article | Health Information Management Journal | 3 |
| Computers & Security | 3 | |
| INQUIRY: The Journal of Health Care Organization, Provision, and Financing | 2 | |
| Sustainability | 1 | |
| Symmetry | 1 | |
| International Journal of Environmental Research and Public Health | 1 | |
| International Journal of Medical Informatics | 1 | |
| Information Systems Research | 1 | |
| Information Management & Computer Security | 1 | |
| Health Informatics Journal | 1 | |
| BMC Medical Informatics and Decision Making | 1 | |
| International Journal of Health Care Quality Assurance | 1 | |
| Information Systems Frontiers | 1 | |
| Information Systems Journal | 1 | |
| Malaysian Journal of Computer Science | 1 | |
| European Journal of Information Systems | 1 | |
| JMIR Human Factors | 1 | |
| Journal of Medical Internet Research | 1 | |
| Security Journal | 1 | |
| Journal of Public Health | 1 | |
| Proceedings | Procedia Technology | 2 |
| Americas Conference on Information Systems (AMCIS) | 2 | |
| IEEE Conference on e-Learning, e-Management, and e-Services (IC3e) | 1 | |
| Hawaii International Conference on System Sciences | 1 | |
| International Conference on Information and Communication Systems (ICICS) | 1 | |
| International Conference on Availability, Reliability, and Security | 1 | |
| Conference on HCI for Cybersecurity, Privacy, and Trust | 1 | |
| Conference on Risks and Security of Internet and Systems | 1 |
| Foundational Theory | Frequency | Citation |
|---|---|---|
| Theory of planned behavior (TPB) | 10 | [1,49,51,57,60,61,62,70,74,80] |
| General deterrence theory (GDT) | 9 | [11,57,64,65,68,73,76,77,80] |
| Protection motivation theory (PMT) | 8 | [49,57,65,69,71,76,78,81] |
| Health belief model (HBM) | 5 | [49,62,72,74,75] |
| Theory acceptance model (TAM) | 4 | [61,65,70,81] |
| Social cognitive theory (SCT) | 1 | [84] |
| Norman’s action theory (NAT) | 1 | [50] |
| Concern for information privacy (CFIP) | 1 | [69] |
| Theory of reasoned action (TRA) | 1 | [71] |
| Power style theory (PST) | 1 | [51] |
| Social exchange theory (SET) | 1 | [51] |
| Technology threat avoidance theory (TTAT) | 1 | [63] |
| Unified theory of acceptance and use of technology (UTAUT) | 1 | [61] |
| Social control theory (SCoT) | 1 | [49] |
| Rational choice theory (RCT) | 1 | [57] |
| Social bond theory (SBT) | 1 | [58] |
| Cognitive moral development theory (CMDT) | 1 | [57] |
| Diffusion of innovation (DOI) | 1 | [57] |
| Prosocial rule breaking (PSRB) | 1 | [79] |
| Neutralization theory | 1 | [82] |
| Type of Security Behavior | Study Focus | Frequency | Citation |
|---|---|---|---|
| Desirable security behavior | Compliance with policy/regulations | 17 | [25,49,57,61,63,64,65,68,69,71,73,75,77,78,83,84] |
| Security protection | 8 | [25,49,62,63,69,70,72,78] | |
| Undesirable security behavior | Risky security practices | 4 | [64,77,79,85] |
| Violation/non-compliance | 3 | [50,68,82] | |
| Both security behaviors | Secure and insecure practices | 3 | [66,76,83] |
| Factor (n) | Key Points | User | DSB Study | USB Study |
|---|---|---|---|---|
| Self-efficacy (12) | Belief about self-capabilities to perform security practices | CS NS | [1,51,57,61,62,63,70,71,72,74,75,76] | N/A |
| Perceived severity (10) | Perception of adverse impacts from security incidents or threats | CS NS MS | [62,63,65,71,73,74,75,81] | [68,76] |
| Attitudes (7) | Positive or negative feelings about engaging in a specific behavior | CS NS | [51,58,60,62,70,80,81] | N/A |
| Subjective norms (7) | Perception of referent approval to exhibit or not exhibit a behavior | CS NS | [57,60,62,70,71,80,81] | N/A |
| Information security awareness (7) | Knowledge and understanding of health information security | CS NS MS | [57,65,76] | [64,76,77,83] |
| Perceived benefit/response efficacy (6) | Perception of positive outcomes from employing information security measures | CS NS | [62,71,74,75] | N/A |
| Perceived susceptibility/vulnerability (4) | Perception of the probability of being exposed to malicious threats | CS NS MS | [63,65,71,76] | N/A |
| Perceived behavioral control (4) | Perception of difficulty in displaying security behavior determined by internal or external constraints | CS NS | [60,62,70,80] | N/A |
| Perceived trust (4) | Belief that others’ actions can be instrumental to self-interest and provide benefits | CS NS | [1,51,60,74] | N/A |
| Perceived barriers (3) | Perception of the difficulty or cost of security practices, including money, time, or effort | CS NS | [72,74,75] | N/A |
| Perceived usefulness (2) | Protecting security and privacy is important and beneficial | CS NS | [70,81] | N/A |
| Perceived threat/risk (2) | Perceiving security threats as an inherent risk when using the HIS in a particular condition | CS NS | [63,65] | N/A |
| Safeguard cost (2) | Perception of inconvenience regarding the effort to employ security measures | CS NS | [63,65] | N/A |
| Perceived responsibility (2) | Personal characteristics prescribed in the code of ethics | CS MS | [62] | [79] |
| Personal norms (2) | Self-values and perspectives on information security | CS MS | [58] | [77] |
| Safeguard effectiveness (1) | Security safeguards can effectively mitigate the risks of utilizing the HIS in some circumstances | CS | [63] | N/A |
| Coping appraisal (1) | Examination of a person’s ability to deal with losses when faced with a threat | CS | [78] | N/A |
| Perceived work experience (1) | Perceptions of work experience that may help in enhancing information security competence and awareness | CS NS | [75] | N/A |
| Compatibility (1) | Perception of the protection is consistent with users’ needs, values, and experiences | CS | [70] | N/A |
| Controllability (1) | Perception of security measures can control the HIS | CS | [62] | N/A |
| Religion (1) | Religious values can influence perceptions and actions in protecting information security | CS NS | [57] | N/A |
| Personality traits (1) | Personality categories (e.g., extraversion, agreeableness, conscientiousness, neuroticism, intellect/imagination) | CS NS | [57] | N/A |
| Commitment (1) | Employee’s engagement to support information security in the organization | CS | [58] | N/A |
| Involvement (1) | Employee’s participation in supporting information security in the organization | CS | [58] | N/A |
| Perceived stress levels (1) | The mental state that can influence employees to use unfavorable security practices | CS NS | N/A | [85] |
| Situational empathy (1) | Personal characteristics in a situation that has sensitivity to the others’ emotional experiences to facilitate communication with patients and their families | MS | N/A | [79] |
| Perceived impact (1) | Impact levels of undesirable security practices that affect employees and others | MS | N/A | [79] |
| Self-control (1) | The process of self-regulation is such that the individual acts intentionally | MS | N/A | [77] |
| Lack of knowledge (1) | The employee does not have adequate knowledge of security requirements | NS | N/A | [50] |
| Poor skills (1) | The employee does not have adequate skills to carry out information security protection | NS | N/A | [50] |
| Poor discipline (1) | The employee does not have good discipline, e.g., laziness, arrogance, and indifference | NS | N/A | [50] |
| Factor (n) | Key Points | Organization | DSB Study | USB Study |
|---|---|---|---|---|
| Organizational/management support (4) | Top-level management or organizational commitment to protecting information security | HS AHF NHF | [1,26,61,74] | N/A |
| Cues to action (3) | Information security campaigns and other influences that can encourage proper security behavior | HS AHF | [62,72,75] | N/A |
| Organizational culture/climate (3) | Multidimensional construct with numerous features that might influence employee behavior | HS NHF | [66,82] | [66] |
| Punishment/detection certainty (2) | Act or process certain to be enforced in data protection within the organization | HS NHF | [73,80] | N/A |
| Peer influence (2) | Influence from coworkers who have the power to give rewards or impose penalties for security practices | HS | [70] | [82] |
| Superior influence (2) | Influence from superiors who have the power to give rewards or impose penalties for security practices | HS | [70] | [82] |
| Facilitating condition (1) | Assets in ensuring that privacy protection behaviors are consistent with existing assets in the organization | HS | [70] | N/A |
| Data collection (1) | Techniques used for data collection become patient privacy concerns | HS | [69] | N/A |
| Secondary use (1) | Information is collected from the individual for a specific purpose but is used for another without proper authorization | HS | [69] | N/A |
| Error (1) | Intended and unintended errors in information collected by the organization | HS | [69] | N/A |
| Incentives (1) | Monetary and non-monetary incentives as a motivational stimulant | HS | [51] | N/A |
| Nature of work (1) | The quality of work done by staff | HS | [51] | N/A |
| Social relations (1) | Interpersonal connections among employees | HS | [51] | N/A |
| Security system satisfaction (1) | Degree of user satisfaction with the security system | HS | [76] | N/A |
| Legal/punishment (1) | Legal consequences or punishment from the organization for employees who conduct security violations/non-compliance | HS | [57] | N/A |
| Internal auditing effectiveness (1) | Procedures to ensure that information security control complies with organizational requirements and related standards | HS NHF | [73] | N/A |
| Security education and training program (SETA) (1) | Program to provide information security knowledge/skills and inform about information security policy for health staff | HS NHF | [73] | N/A |
| Workload (1) | Employees’ amount of work, busyness, and pressure at work that might disrupt their compliance behavior | HS | [60] | N/A |
| Regulatory concerns (1) | The risk of violating regulations regarding security and privacy related to HIS use | HS NHF | [65] | N/A |
| Medical assessment (1) | The patient’s medical status should be reported to related parties | AHF | N/A | [64] |
| Shadow working process (1) | Security practices enable efficient working practices but are against the policy or even national laws | HS NHF | N/A | [83] |
| Organizational limitations (1) | Organizational conditions that might cause human error, such as high turnover, low morale, understaffing, and/or high workload | NHF | N/A | [50] |
| Inefficient business processes (1) | Inefficient workflow that might cause human error, such as redundancy, suboptimality, and/or bottlenecks | NHF | N/A | [50] |
| Poor monitoring and enforcement (1) | Ineffective security policy implementation, such as few incentives to comply or penalties for violations | NHF | N/A | [50] |
| Physical environmental limitations (1) | Inadequate physical environment to support security control, such as small rooms | NHF | N/A | [50] |
| Technological limitations (1) | Inadequate technology to support security control, such as outdated computer applications, slow networks, etc. | NHF | N/A | [50] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sari, P.K.; Handayani, P.W.; Hidayanto, A.N.; Yazid, S.; Aji, R.F. Information Security Behavior in Health Information Systems: A Review of Research Trends and Antecedent Factors. Healthcare 2022, 10, 2531. https://doi.org/10.3390/healthcare10122531
Sari PK, Handayani PW, Hidayanto AN, Yazid S, Aji RF. Information Security Behavior in Health Information Systems: A Review of Research Trends and Antecedent Factors. Healthcare. 2022; 10(12):2531. https://doi.org/10.3390/healthcare10122531
Chicago/Turabian StyleSari, Puspita Kencana, Putu Wuri Handayani, Achmad Nizar Hidayanto, Setiadi Yazid, and Rizal Fathoni Aji. 2022. "Information Security Behavior in Health Information Systems: A Review of Research Trends and Antecedent Factors" Healthcare 10, no. 12: 2531. https://doi.org/10.3390/healthcare10122531