
Effects of Exercise Training on Peripheral Muscle Strength in Children and Adolescents with Cystic Fibrosis: A Meta-Analysis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Registration and Methodology
2.1.1. Data Search Strategy
2.1.2. Eligibility Criteria
2.1.3. Type of Intervention and Control
2.1.4. Type of Outcome Measures
2.2. Study Selection and Data Collection Process
2.3. Assessment of Risk of Bias in the Included Studies
2.4. Data Analysis
3. Results
3.1. Compliance with the Protocol Registration
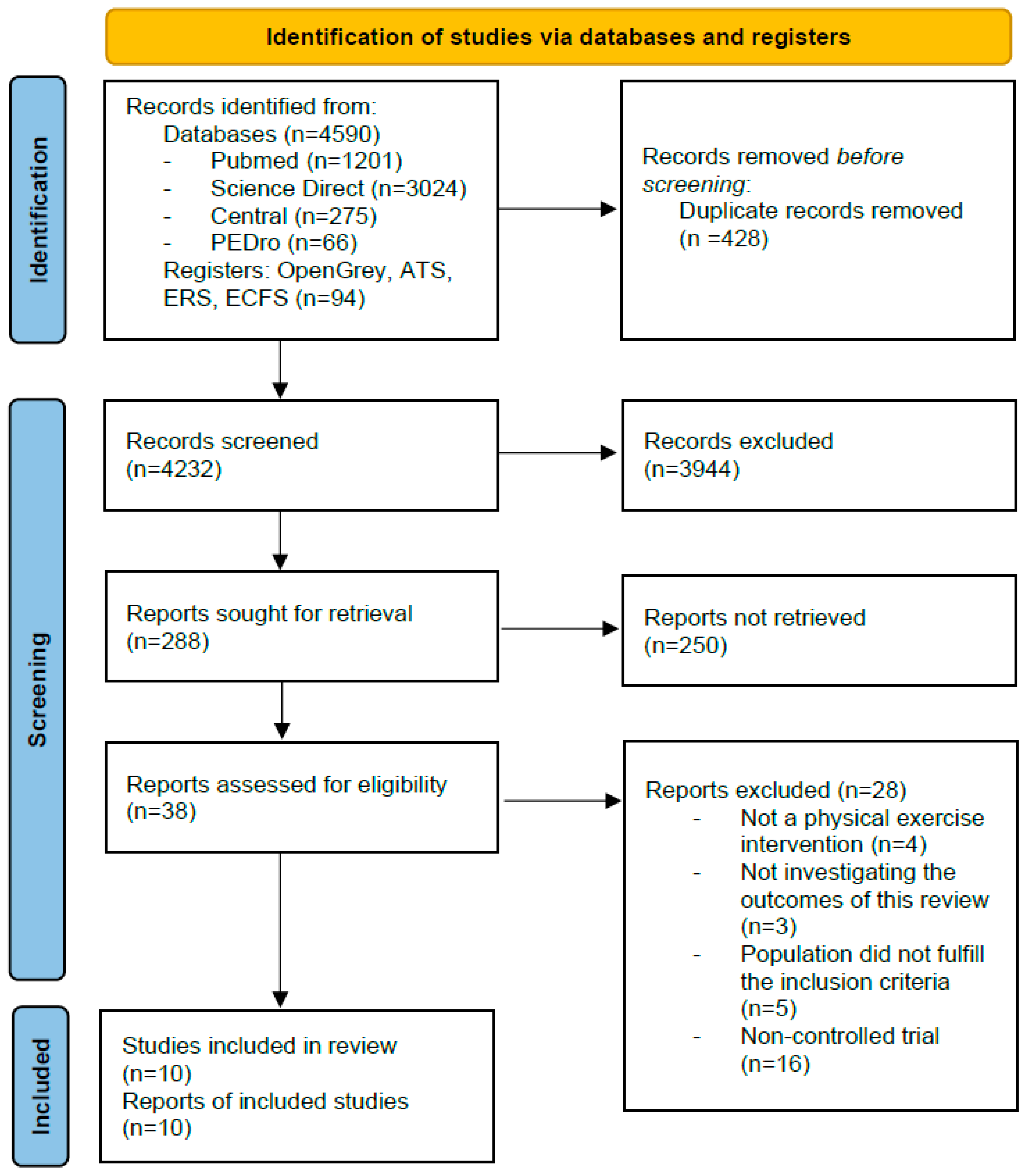
3.2. Selection and Characteristics of the Studies
3.3. Risk of Bias
3.4. Effect of the Intervention
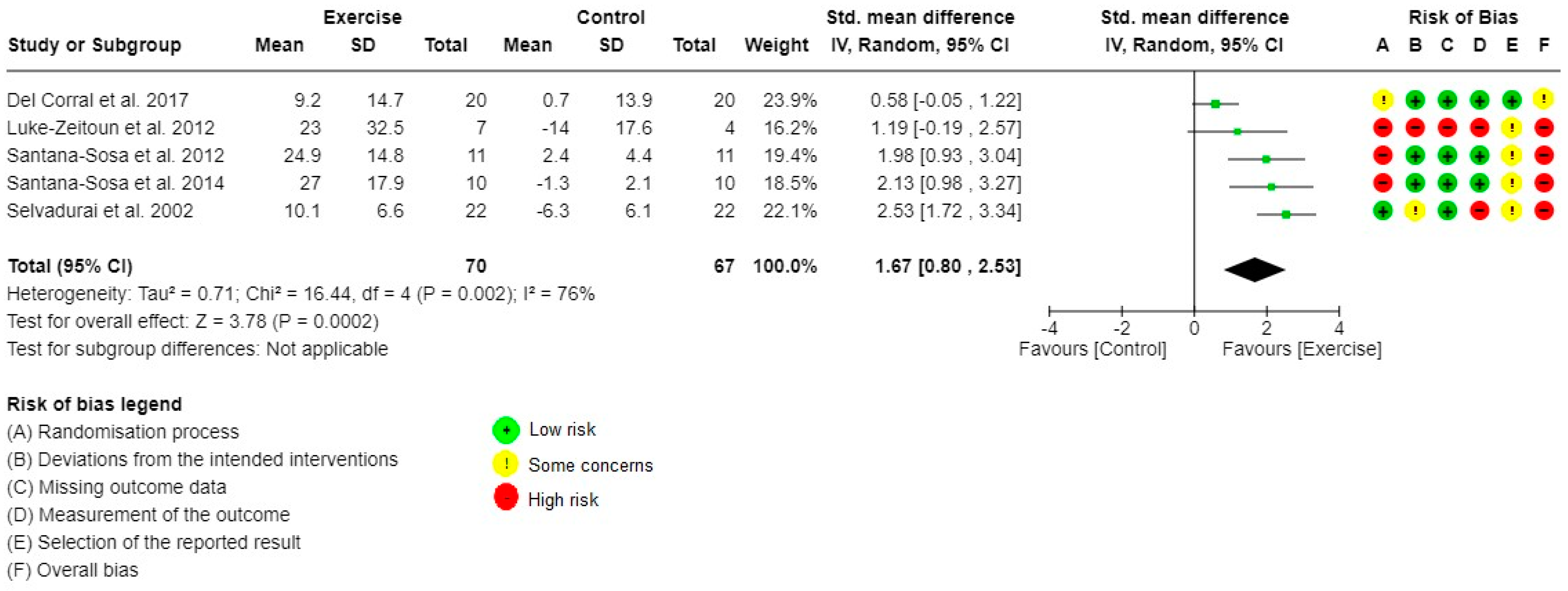
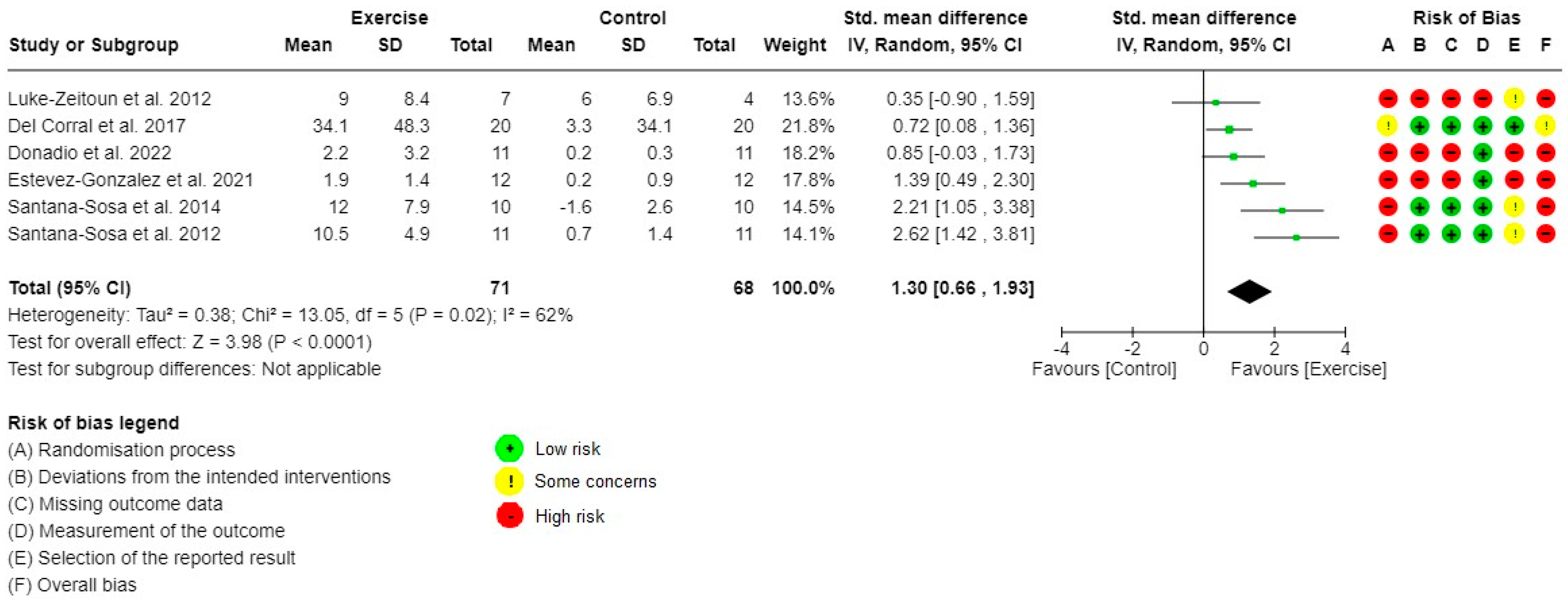
3.4.1. Primary Outcome: LLM and ULM Strength
3.4.2. Secondary Outcomes
4. Discussion
4.1. Limitations
4.2. Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Riordan, J.R.; Rommens, J.M.; Kerem, B.; Alon, N.; Rozmahel, R.; Grzelczak, Z.; Zielenski, J.; Lok, S.I.; Plavsic, N.; Chou, J.L.; et al. Identification of the cystic fibrosis gene: Cloning and characterization of complementary DNA. Science 1989, 245, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Dehillotte, C.; Lemonnier, L. French Register of Cystic Fibrosis (2018 data). Vaincre la Mucoviscidose. 2020. Available online: www.registredelamuco.org (accessed on 1 June 2022).
- Arikan, H.; Yatar, İ.; Calik-Kutukcu, E.; Aribas, Z.; Saglam, M.; Vardar-Yagli, N.; Savci, S.; Inal-Ince, D.; Ozcelik, U.; Kiper, N. A comparison of respiratory and peripheral muscle strength, functional exercise capacity, activities of daily living and physical fitness in patients with cystic fibrosis and healthy subjects. Res. Dev. Disabil. 2015, 45–46, 147–156. [Google Scholar] [CrossRef] [PubMed]
- de Meer, K.; Gulmans, V.A.; van Der Laag, J. Peripheral muscle weakness and exercise capacity in children with cystic fibrosis. Am. J. Respir. Crit. Care Med. 1999, 159, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Troosters, T.; Langer, D.; Vrijsen, B.; Segers, J.; Wouters, K.; Janssens, W.; Gosselink, R.; Decramer, M.; Dupont, L. Skeletal muscle weakness, exercise tolerance and physical activity in adults with cystic fibrosis. Eur. Respir. J. 2009, 33, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Mackintosh, K.A.; Ridgers, N.D.; Evans, R.E.; McNarry, M.A. Physical Activity and Sedentary Time Patterns in Children and Adolescents with Cystic Fibrosis and Age- and Sex-Matched Healthy Controls. J. Phys. Act. Health. 2018, 15, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Puppo, H.; Torres-Castro, R.; Vasconcello-Castillo, L.; Acosta-Dighero, R.; Sepúlveda-Cáceres, N.; Quiroga-Marabolí, P.; Romero, J.E.; Vilaro, J. Physical activity in children and adolescents with cystic fibrosis: A systematic review and meta-analysis. Pediatr. Pulmonol. 2020, 55, 2863–2876. [Google Scholar] [CrossRef]
- Barry, S.; Gallagher, C.G. Corticosteroids and skeletal muscle function in cystic fibrosis. J. Appl. Physiol. 2003, 95, 1379–1384. [Google Scholar] [CrossRef] [Green Version]
- Ruf, K.; Beer, M.; Köstler, H.; Weng, A.M.; Neubauer, H.; Klein, A.; Platek, K.; Roth, K.; Beneke, R.; Hebestreit, H. Size-adjusted muscle power and muscle metabolism in patients with cystic fibrosis are equal to healthy controls—A case control study. BMC Pulm. Med. 2019, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Hulzebos, H.J.; Jeneson, J.; Van Der Ent, C.K.; Takken, T. CrossTalk opposing view: Skeletal muscle oxidative capacity is not altered in cystic fibrosis patients. J. Physiol. 2017, 595, 1427–1428. [Google Scholar] [CrossRef]
- Lamhonwah, A.-M.; Bear, C.E.; Huan, L.J.; Chiaw, P.K.; Ackerley, C.A.; Tein, I. Cystic fibrosis transmembrane conductance regulator in human muscle: Dysfunction causes abnormal metabolic recovery in exercise. Ann. Neurol. 2010, 67, 802–808. [Google Scholar] [CrossRef]
- Reznikov, L.R. Cystic Fibrosis and the Nervous System. Chest 2017, 151, 1147–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, B.L. Evidence for a mitochondrial lesion in cystic fibrosis. Life Sci. 1989, 44, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Valdivieso, A.G.; Santa-Coloma, T.A. CFTR activity and mitochondrial function. Redox Biol. 2013, 1, 190–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Authority of Health. Health-Promoting Guidelines to Promote, to Check, and to Prescribe Sport and Physical Activity in Adults. 2019. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2018-10/guide_aps_vf.pdf (accessed on 1 February 2022).
- Radtke, T.; Nevitt, S.J.; Hebestreit, H.; Kriemler, S. Physical exercise training for cystic fibrosis. Cochrane Database Syst. Rev. 2017, 2017, CD002768. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. MetaArXiv 2020. Available online: https://osf.io/preprints/metaarxiv/v7gm2/ (accessed on 22 November 2022).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Available online: www.training.cochrane.org/handbook (accessed on 7 July 2021).
- World Health Organization. Adolescent Health and Development. 2015. Available online: https://www.who.int/maternal_child_adolescent/topics/adolescence/dev/fr/ (accessed on 7 July 2021).
- Higgins, J.; Savovic, J.; Page, M.; Elbers, R.; Sterne, J. Assessing Risk of Bias in a Randomized Trial. Cochrane Handbook for Systematic Reviews of Interventions. 2021. Available online: https://training.cochrane.org/handbook/current/chapter-08 (accessed on 22 November 2022).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Tianjing, L.; Jonathan, J.D. Choosing Effect Measures and Computing Estimates of Effect. 2021. Available online: https://training.cochrane.org/handbook/current/chapter-06 (accessed on 7 July 2021).
- Schünemann, H.J.; Higgins, J.P.; Glasziou, P.; Akl, E.A.; Skoetz, N.; Guyatt, G.H. Completing ‘Summary of Findings’ Tables and Grading the Certainty of the Evidence. 2021. Available online: /handbook/current/chapter-14 (accessed on 1 April 2022).
- Selvadurai, H.; Blimkie, C.; Meyers, N.; Mellis, C.; Cooper, P.; Van Asperen, P. Randomized controlled study of in-hospital exercise training programs in children with cystic fibrosis. Pediatr. Pulmonol. 2002, 33, 194–200. [Google Scholar] [CrossRef]
- Klijn, P.H.; Oudshoorn, A.; Van Der Ent, C.K.; Van Der Net, J.; Kimpen, J.L.; Helders, P.J. Effects of Anaerobic Training in Children with Cystic Fibrosis: A Randomized Controlled Study. Cardiopulm. Phys. Ther. J. 2004, 15, 1299–1305. [Google Scholar] [CrossRef]
- Luke-Zeitoun, M.; Nielson, D.; Desch, J.; Moss, R. Effectiveness of Individualized Non-Supervised Coached Exercise Program in Children with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2012, 185, A5263. [Google Scholar]
- Groeneveld, I.F.; Gonzalez-Saiz, L.; López-Mojares, L.M.; Villa-Asensi, J.R.; Barrio-Gonzalez, M.I.; Fleck, S.J.; Pérez, M.; Lucia, A. Intrahospital weight and aerobic training in children with cystic fibrosis: A randomized controlled trial. Med. Sci. Sport Exerc. 2012, 44, 2–11. [Google Scholar]
- Santana-Sosa, E.; Gonzalez-Saiz, L.; Groeneveld, I.F.; Villa-Asensi, J.R.; Aguero, M.I.B.G.D.; Fleck, S.J.; López-Mojares, L.M.; Pérez, M.; Lucia, A. Benefits of combining inspiratory muscle with ‘whole muscle’ training in children with cystic fibrosis: A randomised controlled trial. Br. J. Sports Med. 2013, 48, 1513–1517. [Google Scholar] [CrossRef] [PubMed]
- Ledger, S.; Wade, A.; Douglas, H.; Sarria, L.; Rayner, P.; Goldman, A.; Giardini, A.; Prasad, A.; Aurora, P.; Main, E. Interim results for INSPIRE-CF: A 24-month RCT evaluating effects of weekly supervised exercise in children with CF. Eur. Respir. J. 2016, 48, OA1493. [Google Scholar]
- Del Corral, T.; Cebrià, I.; Iranzo, M.À.; López-de-Uralde-Villanueva, I.; Martínez-Alejos, R.; Blanco, I.; Vilaró, J. Effectiveness of a Home-Based Active Video Game Programme in Young Cystic Fibrosis Patients. Respiration 2018, 95, 87–97. [Google Scholar] [CrossRef]
- Gupta, S.; Mukherjee, A.; Lodha, R.; Kabra, M.; Deepak, K.K.; Khadgawat, R.; Talwar, A.; Kabra, S.K. Effects of Exercise Intervention Program on Bone Mineral Accretion in Children and Adolescents with Cystic Fibrosis: A Randomized Controlled Trial. Indian J. Pediatr. 2019, 86, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Estévez-González, A.J.; Donadio, M.V.F.; Cobo-Vicente, F.; Fernández-Luna, Á.; Sanz-Santiago, V.; Villa Asensi, J.R.; Iturriaga Ramirez, T.; Fernández-del-Valle, M.; Diez-Vega, I.; Larumbe-Zabala, E.; et al. Effects of a Short-Term Resistance-Training Program on Heart Rate Variability in Children With Cystic Fibrosis—A Randomized Controlled Trial. Front. Physiol. 2021, 12, 652029. [Google Scholar] [CrossRef]
- Donadio, M.V.; Cobo-Vicente, F.; San Juan, A.F.; Sanz-Santiago, V.; Fernández-Luna, Á.; Iturriaga, T.; Asensi, J.R.; Pérez-Ruiz, M. Is exercise and electrostimulation effective in improving muscle strength and cardiorespiratory fitness in children with cystic fibrosis and mild-to-moderate pulmonary impairment?: Randomized controlled trial. Respir. Med. 2022, 196, 106798. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [Green Version]
- Swisher, A.; Lowman, J.D.; Mejia-Downs, A.; Nippins, M.; Gruber, W. Exercise and Habitual Physical Activity for People with Cystic Fibrosis: Expert Consensus, Evidence-Based Guide for Advising Patients. Cardiopulm. Phys. Ther. J. 2015, 26, 85–98. [Google Scholar] [CrossRef]
- Enright, S.; Unnithan, V.B.; Davies, D. Reproducibility of measurements of inspiratory work capacity in cystic fibrosis patients. Respir. Physiol. Neurobiol. 2006, 150, 35–43. [Google Scholar] [CrossRef]
- Combret, Y.; Medrinal, C.; Bonnevie, T.; Gravier, F.-E.; Le Roux, P.; Lamia, B.; Prieur, G.; Reychler, G. Clinimetric evaluation of muscle function tests for individuals with cystic fibrosis: A systematic review. J. Cyst. Fibros. 2020, 19, 981–995. [Google Scholar] [CrossRef]
- Gruet, M.; Saynor, Z. Assessment of Peripheral Muscle Function in Cystic Fibrosis: Why and How? Respir. Care 2019, 64, 238–240. [Google Scholar] [CrossRef] [Green Version]
- Engelen, M.P.; Schroder, R.; Van der Hoorn, K.; Deutz, N.; Com, G. Use of body mass index percentile to identify fat-free mass depletion in children with cystic fibrosis. Clin. Nutr. 2012, 31, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Stein, L.; Pacht, C.; Junge, S.; Kaeding, T.S.; Kück, M.; Maassen, N.; Wittke, T.; Shushakov, V. Skeletal Muscle Function in Young Patients with Cystic Fibrosis. Pediatr. Exerc. Sci. 2016, 28, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Hussey, J.; Gormley, J.; Leen, G.; Greally, P. Peripheral muscle strength in young males with cystic fibrosis. J. Cyst. Fibros. 2002, 1, 116–121. [Google Scholar] [CrossRef]
- Gruet, M.; Saynor, Z.L.; Urquhart, D.S.; Radtke, T. Rethinking physical exercise training in the modern era of cystic fibrosis: A step towards optimising short-term efficacy and long-term engagement. J. Cyst. Fibros. 2021, 21, e83–e98. [Google Scholar] [CrossRef]
- Curran, M.; Tierney, A.C.; Button, B.; Collins, L.; Kennedy, L.; McDonnell, C.; Cassrely, B.; Cahalan, R. The effectiveness of exercise interventions to increase physical activity in Cystic Fibrosis: A systematic review. J. Cyst. Fibros. 2022, 21, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Denford, S.; van Beurden, S.; O’Halloran, P.; Williams, C.A. Barriers and facilitators to physical activity among children, adolescents, and young adults with cystic fibrosis: A systematic review and thematic synthesis of qualitative research. BMJ Open 2020, 10, e035261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stallings, V.A.; Sainath, N.; Oberle, M.; Bertolaso, C.; Schall, J.I. Energy Balance and Mechanisms of Weight Gain with Ivacaftor Treatment of Cystic Fibrosis Gating Mutations. J. Pediatr. 2018, 201, 229–237.e4. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; You, X.; Ellis, M.; Urquhart, D.S.; Jha, L.; Duncan, M.; Tian, S.; Harris, R.A.; Kotsimbos, T.; Keating, D. VO2max as an exercise tolerance endpoint in people with cystic fibrosis: Lessons from a lumacaftor/ivacaftor trial. J. Cyst. Fibros. 2020, 20, 499–505. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Details | N | Characteristics | Study Design | Interventions | Main Findings (Between-Group Comparisons Only) | |
|---|---|---|---|---|---|---|
| Benefits of Exercise Training | Drawbacks or No Effects | |||||
| Selvadurai et al., 2002 [24] | 66 | Exacerbation FEV1: 57.4 (±17.4)%PV Age: 13.2 (±2) yo Age range: 5–16 | RCT, Inpatient, supervised, 1-week program, 5 times/week | I.1: aerobic exercise I.2: strength training (ULM and LLM) C: standard chest physiotherapy | - | LLM, FFM, VO2peak and PA level: not reported |
| Klijn et al., 2004 [25] | 20 | Stable FEV1: 78.7 (±19.9)%PV Age: 13.9 (±1.7) yo Age range: 9–18 | RCT, Outpatient, supervised, 12-weeks program, 2 times/week | I: anaerobic exercise (ULM and LLM) C: habitual CF care | - | ULM and LLM strength, FFM, VO2peak, PA level: no difference (unreported result details) |
| Luke-Zeitoun et al., 2012 [26] | 11 | Stable FEV1: 99.5 (±12)%PV Age: 12 (±2) yo Age range: 8–16 | RCT, Home-based, unsupervised, 6-months program, unknown frequency | I: individualized exercise program (not precise) C: habitual CF care | - | ULM, LLM and VO2peak: not reported |
| Santana Sosa et al., 2012 [27] | 22 | Stable FEV1: 1.8 (±0.2) L Age: 10.5 (±2.5) yo Age range: 5–15 | RCT, Inpatient, supervised, 8-weeks program, 3 times/week | I: aerobic and strength exercise (ULM, LLM and core) C: habitual CF care + PA information | ↗ULM (η2 = 0.44) and LLM (η2 = 0.50) strength ↗VO2peak (η2 = 0.15) | FFM: no difference (η2 = 0.11) |
| Santana Sosa et al., 2014 [28] | 20 | Stable FEV1: 1.6 (±0.2) L Age: 10.5 (±1) yo Age range: 6–17 | RCT, Inpatient, supervised, 8-weeks program, 3 times/week | I: aerobic and strength exercise (ULM, LLM and core) + IMT C: Sham IMT + PA information | ↗ULM (η2 = 0.72) and LLM (η2 = 0.62) strength ↗FFM (η2 = 0.34) ↗VO2peak (η2 = 0.51) | - |
| Ledger et al., 2016 [29] | 71 | Stable FEV1: 86.6 (±15.3)%PV Age: 10 (±3) yo Age range: 6–15 | RCT, Inpatient, supervised, 24-months program, 1/week | I: aerobic and strength exercise (ULM, LLM and core) C: habitual CF care | - | VO2peak: no difference (+1.4 mL/min/kg (95%CI: −1.8 to 4.5)) |
| Del Corral et al., 2018 [30] | 40 | Stable FEV1: 84.5 (±21)%PV Age: 11.8 (±3.2) yo Age range: 7–18 | RCT, Home-based, supervised (virtual coach), 6-weeks program, 5 times/week | I: active video game exercise C: habitual CF care | ↗ULM (MBT: 33.8 cm (95% CI 9.2 to 58.4; d = 1.2) and LLM (HJT: +9.2 cm (2.0 to 16.5; d = 1.2) strength | - |
| Gupta et al., 2019 [31] | 52 | Stable FEV1: 61.2 (±24.8)%PV Age: 12.5 (±3.1) yo Age range: 6–18 | RCT, Home-based, unsupervised, 1-year program, 3 times/week | I: strength exercise (ULM and LLM) + vitamin D and calcium supplementation C: habitual PA + vitamin D and calcium supplementation | ↗VO2peak (4.2 mL/min/kg (95%CI 1.2 to 7.1)) | PA level: no difference (unreported result details) |
| Estevez-Gonzalez et al., 2021 [32] | 24 | Stable FEV1: −1.7 (±1.6) z-score Age: 12.3 (±3.3) yo Age range: 6–17 | RCT, Inpatient, supervised, 8 weeks program, 3 times/week | I: strength exercise (ULM, LLM and core) C: habitual CF care | ↗ULM (d = 1.6) | VO2peak: no difference (d = 0.24) |
| Donadio et al., 2022 [33] | 33 | Stable FEV1: -1.5 (±1.5) z-score Age: 12.6 (±3) yo Age range: 6-17 | RCT, Inpatient, supervised, 8 weeks program, 3 times/week | I.1: strength exercise (ULM, LLM and core) I.2: strength exercise (ULM, LLM and core) + NMES (quadriceps and interscapular region) C: habitual CF care | ↗ULM (η2 = 0.40) | VO2peak: no difference (unreported result details) |
| Exercise Training Compared to Controls for Young pwCF | |||||
|---|---|---|---|---|---|
| Outcomes | Anticipated Absolute Effects * (95% CI) | № of Participants (Studies) | Certainty of the Evidence (GRADE) | Comments | |
| Risk with Control | Risk with Exercise Training | ||||
| 1.1. Lower limb muscle strength | SMD 1.67 higher (0.80 higher to 2.53 higher) | 137 (5 RCTs) | ⨁◯◯◯ VERY LOW a,b,c,e | Exercise training may have a positive effect on LLM strength but the evidence is very uncertain. Heterogeneity is very high (I2 = 76%), LLM strength measurements are heterogenous and risk of bias is high | |
| 1.2. Upper limb muscle strength | SMD 1.30 higher (0.66 higher to 1.93 higher) | 139 (6 RCTs) | ⨁◯◯◯ VERY LOW a,b,c,e | Exercise training may have a positive effect on ULM strength but the evidence is very uncertain. Heterogeneity is high (I2 = 62%), ULM strength measurements are heterogenous and risk of bias is high | |
| Muscle mass | SMD 1.33 higher (0.02 higher to 2.64 higher) | 86 (3 RCTs) | ⨁◯◯◯ VERY LOW a,b,c | Exercise training may have little to no effect on muscle mass, and the evidence is very uncertain. Heterogeneity is very high (I2 = 85%), baseline differences prevent clear interpretation and risk of bias is high | |
| VO2peak | MD 3.60 higher (1.74 higher to 5.47 higher) | 275 (8 RCTs) | ⨁⨁◯◯ LOW a,b,c | Exercise training may have a positive effect on VO2peak but the evidence is uncertain. Heterogeneity is high (I2 = 59%), baseline differences were retrieved on maximal aerobic capacities and risk of bias is high | |
| Physical activity level | SMD 0.40 higher (−0.03 lower to 0.84 higher) | 86 (2 RCTs) | ⨁◯◯◯ VERY LOW a,d,e | Exercise training may have little to no effect on physical activity level, and the evidence is very uncertain. Risk of bias is high (self-reported physical activity level) and methods of measurement are heterogenous | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thorel, A.; Machefert, M.; Gillot, T.; Gravier, F.-E.; Bonnevie, T.; Le Roux, P.; Medrinal, C.; Prieur, G.; Combret, Y. Effects of Exercise Training on Peripheral Muscle Strength in Children and Adolescents with Cystic Fibrosis: A Meta-Analysis. Healthcare 2022, 10, 2520. https://doi.org/10.3390/healthcare10122520
Thorel A, Machefert M, Gillot T, Gravier F-E, Bonnevie T, Le Roux P, Medrinal C, Prieur G, Combret Y. Effects of Exercise Training on Peripheral Muscle Strength in Children and Adolescents with Cystic Fibrosis: A Meta-Analysis. Healthcare. 2022; 10(12):2520. https://doi.org/10.3390/healthcare10122520
Chicago/Turabian StyleThorel, Anna, Margaux Machefert, Timothée Gillot, Francis-Edouard Gravier, Tristan Bonnevie, Pascal Le Roux, Clément Medrinal, Guillaume Prieur, and Yann Combret. 2022. "Effects of Exercise Training on Peripheral Muscle Strength in Children and Adolescents with Cystic Fibrosis: A Meta-Analysis" Healthcare 10, no. 12: 2520. https://doi.org/10.3390/healthcare10122520