
Advancing Access to Healthcare through Telehealth: A Brownsville Community Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- One-on-one meetings were held in person with hospital leaders, outpatient clinics, physician offices, and healthcare care clinics.
- Individual focus groups were conducted with patients, interested parties, and Industries.
- Follow-up calls were made to multiple individuals until conceptual saturation.
- Anonymous surveys of clinicians, patients, and stakeholders were broadly distributed in English and Spanish through community networks and collected through a Qualtrics database.
- Rio Grande Valley Health Information Exchange (RGVHIE)
- Physician Executive (practice owner), Chairman of local health organization, Executive Director, South Texas Physician Alliance
- Su Clinica, Federally Qualified Health Center, located in Brownsville and Harlingen
- Proyecto Juan Diego, Brownsville
- Physician Executive (practice owner) and Brownsville Commissioner at Large
- Valley Baptist Hospital
- Will the program require a significant expenditure for the provider?
- How will the program impact workflow?
- Does the provider organization have the technology to support an implementation?
- Will your patients be able to access and use the telemedicine services?
- What is on your wish list for implementing an ideal telemedicine program?
- City of Brownsville Public Health Department
- City of Brownsville EMS Unit
- Cameron County Health Department
- Brownsville Chamber of Commerce
- University of Texas Health Science Center at Houston
- Texas Southmost College
- Brownsville Independent School District
- Brownsville Wellness Coalition
- Industry
- Question 1: What is your experience with telehealth, and how does it impact your company or organization?
- Question 2: What do you think is the relevance or value of telehealth to your company or organization?
- Question 3: What obstacles does your company or organization face in providing telehealth and or healthcare to employees?
- Question 4: If given the option, list reasons for why you would (or would not) chose for your company or organization to participate in a regional telehealth plan?
3. Results
3.1. Infrastructure Assesment
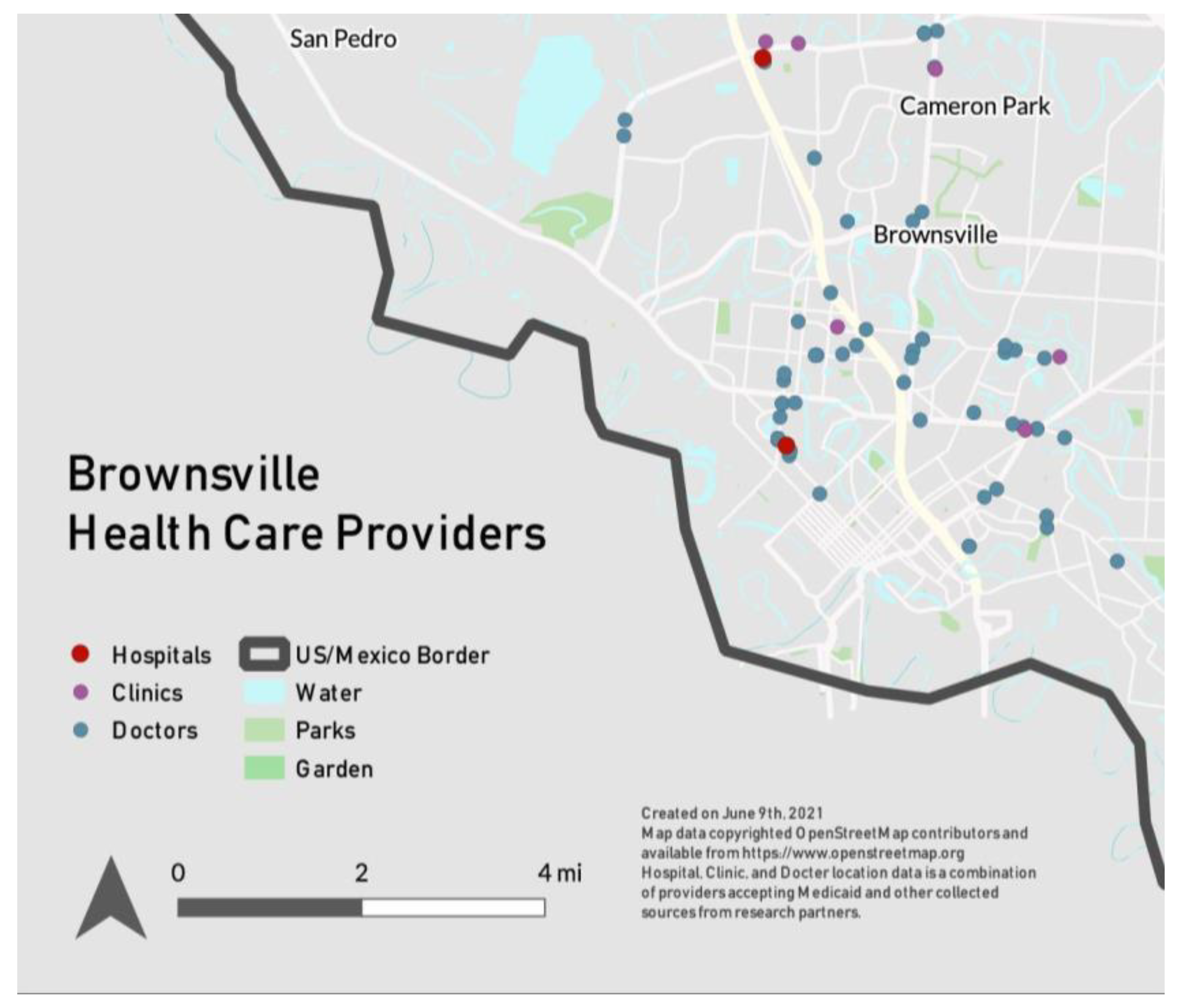
3.1.1. Provider Landscape
3.1.2. Intellectual Resources
3.2. Provider Assessment
- The primary use for telemedicine at this time is primary care followed by e-prescribing.
- Physicians do not have the technology, financial means, or staff to provide a comprehensive system for telemedicine.
- Due to language and literacy barriers, many patients are not able to use a web-based system of telemedicine.
- Many patients do not have a computer and their broadband is limited.
- Patients prefer to see their provider in person but would use the telephone to communicate healthcare issues with their physician.
- For both the provider and the patient, the use of a phone without video provides the most reliable tool to access remote care, but its utility for telemedicine is very limited.
3.2.1. Physical Barriers to Telemedicine
3.2.2. Physical Drivers of Telemedicine
3.3. Focus Group Findings
3.3.1. Community Partners’ Experience with Telehealth
“We recently had our annual health fair, and our insurance company contracted someone from San Antonio at another clinic… we set up the computers, we set up everything for them [employees], we told them just sit here and wait until the nurse connects with you. But otherwise, if we would have asked, just connect here, they [employees] wouldn’t have done it.”—Industry, CEO
3.3.2. Community Partners’ Perception of the Relevance of Telehealth
“Our students, most of the kids, I would say at least 70% or 80%, the closest to healthcare they have is contact with the nurses on campus. So that’s what telehealth could help with.”—Brownsville Independent School District (BISD), Administrator
“The biggest benefit is having the right care for the right patient, at the right time.”—Brownsville EMS, Chief
“It [telehealth] can be so valuable if people can be made to feel comfortable with it, and they have internet access. Obviously if they [patients] can’t access it, they [doctors] can’t make them access it.”—The University of Texas Health Science Center in Houston, Researcher
3.3.3. Community Partners’ Perception of Obstacles for Telehealth
“Even though it’s a privilege to have all these things [telehealth], people do not give them the importance that it has.”—Industry, CEO
“If we find some leaders of the community itself and if that person can relate to that person too… when it comes from your employer or your boss, it kind of feels like it’s direct, you know, it’s forced. Pero si la comadre te invita, y que vamos…it’s always that way. That’s also a kind of incentive.”—Brownsville Wellness Coalition, Director
3.3.4. Patient Drivers to Telemedicine
- Younger patients are more tech-savvy than older patients and thus more likely to utilize and benefit from telemedicine.
- Everyone has a smartphone, but they often use only the most basic features.
- Telemedicine can provide greater access to specialists out-of-town.
- Diabetic patients like the possibility of providing their blood or sugar levels to their provider remotely.
- Many patients would be willing to try telemedicine.
- Patients are happy with the program overall at Proyecto Juan Diego.
- The patients were more enthusiastic about a hybrid model, providing a balance between Telemedicine and in-person visits.
“It is a great option for follow up as it saves time just to be able to let the doctor know your child is doing better.”—Community patient
“Telemedicine is probably ok for pediatrics, but it is a lot more important to go in person or go for more serious occasions.”—Community patient
3.3.5. Patient Barriers to Telemedicine
“The signal in the Valley is not very good, so you lose connection, if you want a better cell connection, you will have to pay way more and it is not always beneficial.”—Community patient
4. Discussion: Lessons from an Interprofessional Approach to Developing a Community Assessment for Telehealth
- Additional support and education for diabetic patients.
- Flexible work shifts: several mentioned using a Hybrid Model (e.g., one visit in person followed by a telemedicine visit).
- Provide resources to address literacy and basic computer skills.
- Add behavioral health to telemedicine due to low numbers of behavioral health providers.
- Ability to take vitals, labs through telemedicine.
“Telemedicine provides seamless communication with providers regardless of where they are.”—physician
“Our healthcare system is so uncoordinated that it [a regional telehealth plan] could help coordinate our healthcare system and people could have their information consistent.”—University of Texas Health Science Center in Houston, Researcher
“A regional plan is a good idea, but if it’s being set up to benefit the many… We just have to make sure that regional really means ‘region that benefits everyone’… make sure we have the same goal…I think anytime you don’t want to regionalize, we’re hurting ourselves because the region itself is a powerful voice… so we need to make sure that our voice is loud enough to sit on those tables and those conversations, city, county and so forth and saying, ‘Hey, we really need mental health’. That [our] voice is always a part of it.”—City of Brownsville Public Health Department, Director
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Topol, E.J. State of Telehealth. N. Engl. J. Med. 2016, 375, 154–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatehi, F.; Samadbeik, M.; Kazemi, A. What is Digital Health? Review of Definitions. Stud. Health Technol. Inform. 2020, 275, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Center for Connected Health Policy. What is Telehealth? Available online: https://www.cchpca.org/what-is-telehealth/ (accessed on 21 July 2021).
- Lackie, M.E.; Parrilla, J.S.; Lavery, B.M.; Kennedy, A.L.; Ryan, D.; Shulman, B.; Brotto, L.A. Digital Health Needs of Women with Postpartum Depression: Focus Group Study. J. Med. Internet Res. 2021, 23, e18934. [Google Scholar] [CrossRef] [PubMed]
- Ozanne, E.M.; Noseworthy, P.A.; Cameron, K.A.; Schmidt, M.; Cavanaugh, K.; Pershing, M.L.; Guzman, A.; Sivly, A.; Fagerlin, A. Shared Decision Making in the Era of Telehealth: Implications for Practice and Research. MDM Policy Pract. 2020, 5, 2381468320976364. [Google Scholar] [CrossRef]
- Baker, J.; Stanley, A. Telemedicine Technology: A Review of Services, Equipment, and Other Aspects. Curr. Allergy Asthma Rep. 2018, 18, 60. [Google Scholar] [CrossRef]
- Enam, A.; Torres-Bonilla, J.; Eriksson, H. Evidence-Based Evaluation of eHealth Interventions: Systematic Literature Review. J. Med. Internet Res. 2018, 20, e10971. [Google Scholar] [CrossRef]
- Finkelstein, J.B.; Tremblay, E.S.; Van Cain, M.; Farber-Chen, A.; Schumann, C.; Brown, C.; Shah, A.S.; Rhodes, E.T. Pediatric Clinicians’ Use of Telemedicine: Qualitative Interview Study. JMIR Hum. Factors 2021, 8, e29941. [Google Scholar] [CrossRef]
- Champagne-Langabeer, T.; Langabeer, J.R.; Roberts, K.E.; Gross, J.S.; Gleisberg, G.R.; Gonzalez, M.G.; Persse, D. Telehealth Impact on Primary Care Related Ambulance Transports. Prehosp. Emerg. Care 2019, 23, 712–717. [Google Scholar] [CrossRef]
- Langabeer, J.R.; Gonzalez, M.; Alqusairi, D.; Champagne-Langabeer, T.; Jackson, A.; Mikhail, J.; Persse, D. Telehealth-Enabled Emergency Medical Services Program Reduces Ambulance Transport to Urban Emergency Departments. West J. Emerg. Med. 2016, 17, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Langabeer, J.R.; Champagne-Langabeer, T.; Alqusairi, D.; Kim, J.; Jackson, A.; Persse, D.; Gonzalez, M. Cost-benefit analysis of telehealth in pre-hospital care. J. Telemed. Telecare 2017, 23, 747–751. [Google Scholar] [CrossRef]
- Marcin, J.P.; Rimsza, M.E.; Moskowitz, W.B. The Use of Telemedicine to Address Access and Physician Workforce Shortages. Pediatrics 2015, 136, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eurofound. Living, Working and COVID-19; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- Nguyen, M.H.; Gruber, J.; Fuchs, J.; Marler, W.; Hunsaker, A.; Hargittai, E. Changes in Digital Communication During the COVID-19 Global Pandemic: Implications for Digital Inequality and Future Research. Soc. Media Soc. 2020, 6, 2056305120948255. [Google Scholar] [CrossRef] [PubMed]
- Pierce, B.S.; Perrin, P.B.; Tyler, C.M.; McKee, G.B.; Watson, J.D. The COVID-19 telepsychology revolution: A national study of pandemic-based changes in U.S. mental health care delivery. Am. Psychol. 2021, 76, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Wijesooriya, N.R.; Mishra, V.; Brand, P.L.P.; Rubin, B.K. COVID-19 and telehealth, education, and research adaptations. Paediatr. Respir. Rev. 2020, 35, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Looney, K.H.; Huffman, M.A. That Was Then and This Is Now—How the COVID-19 Crisis Changed Telehealth Services: Are the Changes Here to Stay? Health Law Connect. 2020, 1, 2020. [Google Scholar]
- Bhaskar, S.; Nurtazina, A.; Mittoo, S.; Banach, M.; Weissert, R. Telemedicine During and Beyond COVID-19. Front. Public Health 2021, 9, 662617. [Google Scholar] [CrossRef]
- Fields, N.L.; Miller, V.J.; Cronley, C.; Hyun, K.; Mattingly, S.P.; Khademi, S.; Nargesi, S.R.R.; Williams, J. Interprofessional collaboration to promote transportation equity for environmental justice populations: A mixed methods study of civil engineers, transportation planners, and social workers’ perspectives. Transp. Res. Interdiscip. Perspect. 2020, 5, 100110. [Google Scholar] [CrossRef]
- Oluyede, L.; Cochran, A.L.; Wolfe, M.; Prunkl, L.; McDonald, N. Addressing transportation barriers to health care during the COVID-19 pandemic: Perspectives of care coordinators. Transp. Res. Part A Policy Pract. 2022, 159, 157–168. [Google Scholar] [CrossRef]
- Laing, S.S.; Ocampo, P.; Ocampo, C.; Caravalho, J.; Perez, G.; Baugh, S. Provider perceptions of mHealth engagement for low-resourced, safety-net communities. Public Health Nurs. 2021, 38, 13–21. [Google Scholar] [CrossRef]
- Ceasar, J.; Peters-Lawrence, M.H.; Mitchell, V.; Powell-Wiley, T.M. The Communication, Awareness, Relationships and Empowerment (C.A.R.E.) Model: An Effective Tool for Engaging Urban Communities in Community-Based Participatory Research. Int. J. Environ. Res. Public Health 2017, 14, 1422. [Google Scholar] [CrossRef] [Green Version]
- Ely-Ledesma, E. Advancing Latino engagement methodologies in urban planning: Utilizing pláticas for local economic development. Lat. Stud. 2022, 20, 368–389. [Google Scholar] [CrossRef]
- Salimi, Y.; Shahandeh, K.; Malekafzali, H.; Loori, N.; Kheiltash, A.; Jamshidi, E.; Frouzan, A.S.; Majdzadeh, R. Is Community-based Participatory Research (CBPR) Useful? A Systematic Review on Papers in a Decade. Int. J. Prev. Med. 2012, 3, 386–393. [Google Scholar] [PubMed]
- Valerio, M.A.; Rodriguez, N.; Winkler, P.; Lopez, J.; Dennison, M.; Liang, Y.; Turner, B.J. Comparing two sampling methods to engage hard-to-reach communities in research priority setting. BMC Med. Res. Methodol. 2016, 16, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul Rashid, N.; Lee, K.; Jamil, N.A. Conducting qualitative research in the new norms: Are we ready? Nurs. Health Sci. 2021, 23, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Deterding, N.M.; Waters, M.C. Flexible Coding of In-depth Interviews: A Twenty-first-century Approach. Sociol. Methods Res. 2018, 50, 708–739. [Google Scholar] [CrossRef]
- Creswell, J.W. Qualitative Inquiry & Research Design: Choosing among Five Approaches, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Kim, H.; Sefcik, J.S.; Bradway, C. Characteristics of Qualitative Descriptive Studies: A Systematic Review. Res. Nurs. Health 2017, 40, 23–42. [Google Scholar] [CrossRef] [Green Version]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description—The poor cousin of health research? BMC Med. Res. Methodol. 2009, 9, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United States Census Bureau. QuickFacts: Cameron County, Texas. 2019. Available online: https://www.census.gov/quickfacts/brownsvillecitytexas. (accessed on 21 July 2019).
- County, C. Economic Development Demographics. Available online: https://www.cameroncountytx.gov/economic-development-demographics/ (accessed on 17 February 2021).
- Hellerstedt, J. The State of Health in Texas. Tex. Med. 2018, 114, 22–27. [Google Scholar]
- Manusov, E.G.; Gomez De Ziegler, C.; Diego, V.P.; Munoz-Monaco, G.; Williams-Blangero, S. Frailty Index in the Colonias on the US-Mexico Border: A Special Report. Front. Med. 2021, 8, 650259. [Google Scholar] [CrossRef]
- Reininger, B.M.; Wang, J.; Fisher-Hoch, S.P.; Boutte, A.; Vatcheva, K.; McCormick, J.B. Non-communicable diseases and preventive health behaviors: A comparison of Hispanics nationally and those living along the US-Mexico border. BMC Public Health 2015, 15, 564. [Google Scholar] [CrossRef] [Green Version]
- Fisher-Hoch, S.P.; Rentfro, A.R.; Salinas, J.J.; Pérez, A.; Brown, H.S.; Reininger, B.M.; Restrepo, B.I.; Wilson, J.G.; Hossain, M.M.; Rahbar, M.H.; et al. Socioeconomic status and prevalence of obesity and diabetes in a Mexican American community, Cameron County, Texas, 2004–2007. Prev. Chronic. Dis. 2010, 7, A53. [Google Scholar] [PubMed]
- Moya, E.M.; Chavez-Baray, S.M.; Loweree, J.; Mattera, B.; Martinez, N. Adults Experiencing Homelessness in the US-Mexico Border Region: A Photovoice Project. Front. Public Health 2017, 5, 113. [Google Scholar] [CrossRef] [PubMed]
- USA, D. Cameron County, Texas. Available online: https://datausa.io/profile/geo/cameron-county-tx/ (accessed on 15 July 2021).
- Indigent Health Care. Available online: https://www.cameroncountytx.gov/publichealth/indigent-health-care/ (accessed on 27 October 2020).
- Umstattd Meyer, M.R.; Sharkey, J.R.; Patterson, M.S.; Dean, W.R. Understanding contextual barriers, supports, and opportunities for physical activity among Mexican-origin children in Texas border colonias: A descriptive study. BMC Public Health 2013, 13, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, D.; Richardson, C.; Wen, M.; Pagán, J.A. Cross-Border Utilization of Health Care: Evidence from a Population-Based Study in South Texas. Health Serv. Res. 2011, 46, 859–876. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-N.; Mokhtarian, P.L.; Ahn, K.-H. The Seoul of Alonso: New Perspectives on Telecommuting and Residential Location from South Korea. Urban Geogr. 2012, 33, 1163–1191. [Google Scholar] [CrossRef]
- Vilhelmson, B.; Thulin, E. Who and where are the flexible workers? Exploring the current diffusion of telework in Sweden. New Technol. Work. Employ. 2016, 31, 77–96. [Google Scholar] [CrossRef]
- Mouratidis, K.; Peters, S. COVID-19 impact on teleactivities: Role of built environment and implications for mobility. Transp. Res. Part A Policy Pract. 2022, 158, 251–270. [Google Scholar] [CrossRef]
- Mouratidis, K.; Peters, S.; van Wee, B. Transportation technologies, sharing economy, and teleactivities: Implications for built environment and travel. Transp. Res. Part D Transp. Environ. 2021, 92, 102716. [Google Scholar] [CrossRef]
- Gössling, S.; Scott, D.; Hall, C.M. Pandemics, tourism and global change: A rapid assessment of COVID-19. J. Sustain. Tour. 2021, 29, 1–20. [Google Scholar] [CrossRef]
- Wolfe, M.K.; McDonald, N.C.; Holmes, G.M. Transportation Barriers to Health Care in the United States: Findings From the National Health Interview Survey, 1997–2017. Am. J. Public Health 2020, 110, 815–822. [Google Scholar] [CrossRef]
- Henning-Smith, C. The Public Health Case for Addressing Transportation-Related Barriers to Care. Am. J. Public Health 2020, 110, 763–764. [Google Scholar] [CrossRef] [PubMed]
- Kalicki, A.V.; Moody, K.A.; Franzosa, E.; Gliatto, P.M.; Ornstein, K.A. Barriers to telehealth access among homebound older adults. J. Am. Geriatr. Soc. 2021, 69, 2404–2411. [Google Scholar] [CrossRef]
- Hawley, C.E.; Genovese, N.; Owsiany, M.T.; Triantafylidis, L.K.; Moo, L.R.; Linsky, A.M.; Sullivan, J.L.; Paik, J.M. Rapid Integration of Home Telehealth Visits Amidst COVID-19: What Do Older Adults Need to Succeed? J. Am. Geriatr. Soc. 2020, 68, 2431–2439. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.W.; Orengo-Aguayo, R.; Wallace, M.; Metzger, I.W.; Rheingold, A.A. Leveraging Technology and Cultural Adaptations to Increase Access and Engagement Among Trauma-Exposed African American Youth: Exploratory Study of School-Based Telehealth Delivery of Trauma-Focused Cognitive Behavioral Therapy. J. Interpers. Violence 2021, 36, 7090–7109. [Google Scholar] [CrossRef] [PubMed]
- Flynn, M.A.; Rodriguez Lainz, A.; Lara, J.; Rosales, C.; Feldstein, F.; Dominguez, K.; Wolkin, A.; Sierra Medal, I.R.; Tonda, J.; Romero-Steiner, S.; et al. An Innovative United States-Mexico Community Outreach Initiative for Hispanic and Latino People in the United States: A Collaborative Public Health Network. Public Health Rep. 2021, 136, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Perski, O.; Short, C.E. Acceptability of digital health interventions: Embracing the complexity. Transl. Behav. Med. 2021, 11, 1473–1480. [Google Scholar] [CrossRef]
- Deo, S.; Singh, P. Community health worker-led, technology-enabled private sector intervention for diabetes and hypertension management among urban poor: A retrospective cohort study from large Indian metropolitan city. BMJ Open 2021, 11, e045246. [Google Scholar] [CrossRef] [PubMed]
- Braun, R.; Catalani, C.; Wimbush, J.; Israelski, D. Community health workers and mobile technology: A systematic review of the literature. PLoS ONE 2013, 8, e65772. [Google Scholar] [CrossRef]
- Hsiao, V.; Chandereng, T.; Lankton, R.L.; Huebner, J.A.; Baltus, J.J.; Flood, G.E.; Dean, S.M.; Tevaarwerk, A.J.; Schneider, D.F. Disparities in Telemedicine Access: A Cross-Sectional Study of a Newly Established Infrastructure during the COVID-19 Pandemic. Appl. Clin. Inform. 2021, 12, 445–458. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ely-Ledesma, E.; Champagne-Langabeer, T. Advancing Access to Healthcare through Telehealth: A Brownsville Community Assessment. Healthcare 2022, 10, 2509. https://doi.org/10.3390/healthcare10122509
Ely-Ledesma E, Champagne-Langabeer T. Advancing Access to Healthcare through Telehealth: A Brownsville Community Assessment. Healthcare. 2022; 10(12):2509. https://doi.org/10.3390/healthcare10122509
Chicago/Turabian StyleEly-Ledesma, Edna, and Tiffany Champagne-Langabeer. 2022. "Advancing Access to Healthcare through Telehealth: A Brownsville Community Assessment" Healthcare 10, no. 12: 2509. https://doi.org/10.3390/healthcare10122509