
Effect of the Juggling-Based Motor Learning Physical Activity on Well-Being in Elderly: A Pre–Post Study with a Special Training Protocol

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment of the Attractiveness and Well-Being
2.3. J-BMLP Description
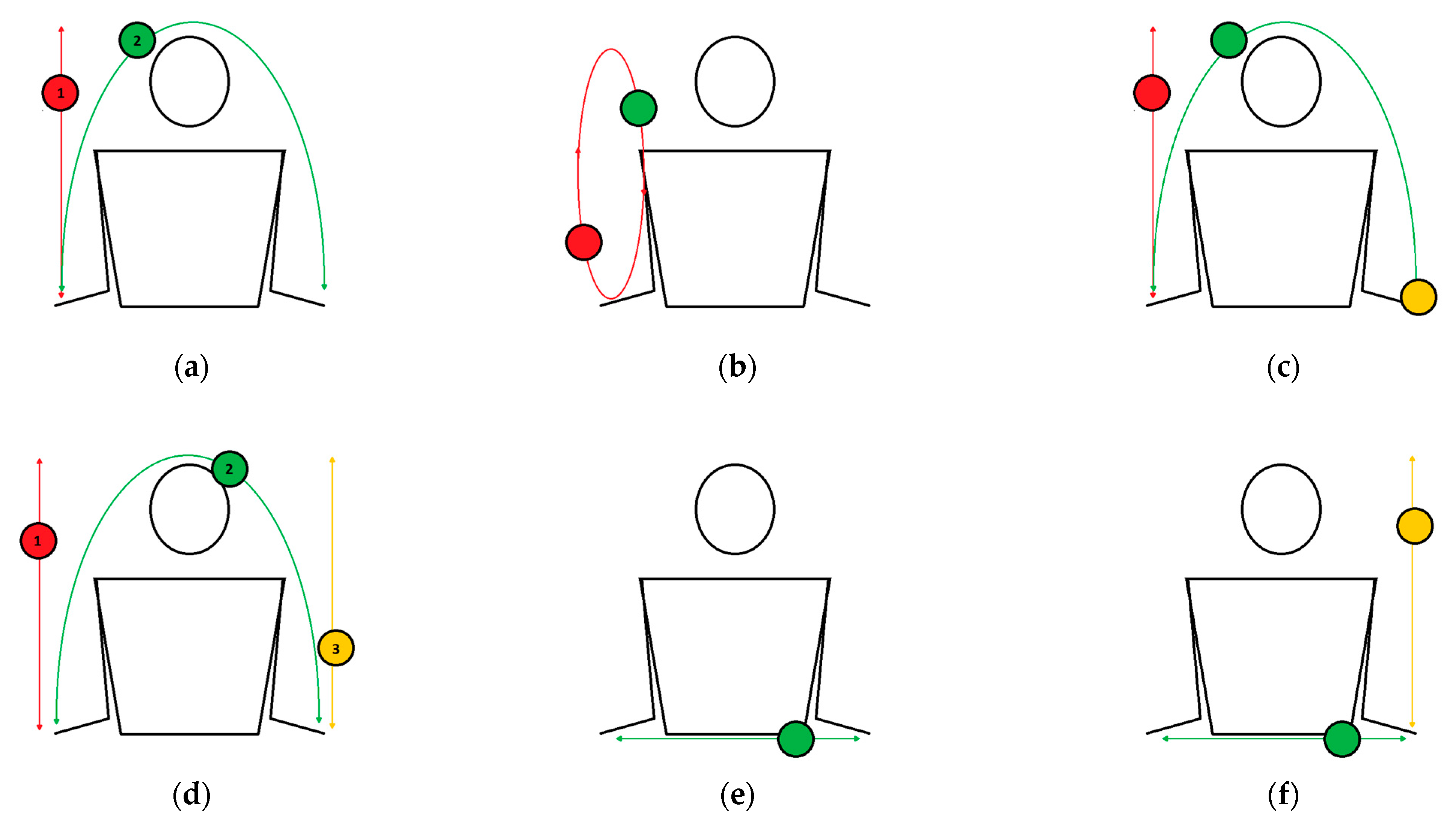
- The one-handed column is the simplest task of this type. Using one hand, practitioners should toss and catch one ball.
- The two-handed alternate-column task requires tossing balls in alternating order. The task should be performed smoothly; i.e., tossing one ball should occur when the other is at the peak of its trajectory.
- The two-handed simultaneous columns is a task in which exercisers should toss two balls using two hands simultaneously at the same level. Attention should be directed toward both balls at the same time.
- The two-handed simultaneous column task at three levels requires throwing balls using two hands at the same level in a specific order: (1) the first (low), (2) the second (medium, eye line); (3) the third (high) level.
- The two-handed simultaneous columns at different levels is a task in which practitioners should toss two balls in the following order: (1) the dominant hand—the first level; the non-dominant hand—the third level; (2) the dominant hand—the third level; the non-dominant hand—the first level.
- Fake columns are a group of similar tasks that require tossing and isolation exercises at the same time. Isolation is not throwing but guiding the ball using a hand along the trajectory of a column, just like a tossed ball. The ball, which is guided by a hand, can be next to, above or below the tossed ball. It is important to react with an isolated ball to the movements of the tossed ball.
- The two-balls-in-one-hand column task requires tossing two balls alternately in the same hand. Each toss should be performed when the previous ball is at the peak of its column trajectory.
- The one-handed column and the parabola task is a combination of the one-handed column and the one-handed parabola. Two balls are in one hand. During one repetition, exercisers should follow the correct order: (1) toss the first ball in a column trajectory; (2) throw the second ball in a parabolic trajectory; (3) catch the first ball; (4) catch the second ball.
- The two-balls-in-one-hand fountain is a task where balls move in an ellipse. Two balls are held in one hand. The rhythm of tossing is important: when one ball is at the peak of its trajectory, then the practitioner should toss the second ball. The purpose of this exercise is to master the correct rhythm of tossing the balls. It is not necessary to catch both balls in the same hand. If someone performs this exercise well, we encourage them to try to perform as many such tosses as possible in a series.
- The one-handed column and the parabola with three balls at pace is a task that differs from “the one-handed column and the parabola” with a third ball. Two balls should be held in one hand, with the third in the other. The task should start from the hand with two balls. The order of performing this task is as follows: (1) toss the first ball in a column trajectory; (2) throw the second ball in a parabolic trajectory; (3) catch the first ball; (4) catch the second ball with the hand in which the third ball is held.
- The three-ball “W” task is a more difficult version of the previous task and requires smooth movement so that none of the balls come into contact with each other.
- The zero throw is a simple task that involves the dynamic throwing of a ball in a horizontal line from hand to hand.
- The two-ball box task requires simultaneously moving two balls in the following order: (1) a column toss of the first ball and a zero throw of the second ball at the same time; (2) a zero throw of the second ball and a catch of the first ball at the same time. This task can be performed alternately on both sides at pace.
- The one-handed parabola is the simplest task of the parabola exercises and involves throwing the ball from hand to hand. Exercisers should avoid the direct transfer of the ball.
- The one-handed parabola with the second ball in the catching hand task requires throwing a ball from one hand to the other. The exercisers should complete one repetition of this exercise with two balls in one hand. An important progression in this exercise is to release the second ball before the first ball lands in the hand, as follows: (1) throw the first ball; (2) release the second ball on the ground; (3) catch the first ball.
- The two-handed parabolas with a different focus of attention is a group of tasks with two balls (each in one hand), where it is required to throw balls in the following order: (1) throw the first ball; (2) throw the second ball; (3) catch/ignore the first ball; (4) catch/ignore the second ball. The practitioner should focus their attention only on the first ball and ignore the second ball or on the second ball and then ignore the first ball. Ignoring is understood as letting the ball fall to the ground. It is necessary to have the perfect parabolic trajectory of both balls. The ball on which the participant focuses their attention must be caught. The goal of this task is to throw and catch both balls alternately at pace.
- The two-handed parabolas with three balls/throwing two balls is a more difficult version of the previous task. This task requires alternating the throwing and catching of both balls at pace with an additional ball constantly held in a hand. The practitioners should always start the task from the hand with two balls.
- The two-handed parabolas with three balls with a different focus of attention is a group of tasks that require exercisers to throw three balls along a perfect parabolic trajectory. In this task, practitioners should start from the hand with two balls. The order of movement in this task should be as follows: (1) throw the first ball; (2) throw the second ball; (3) throw the third ball; (4) catch/ignore the first ball; (5) catch the second ball; (6) catch/ignore the third ball. Ignoring is understood as mentioned previously—letting the ball fall to the ground. In one version of this task, the first two balls should be caught, and the third can fall; in the second version, the first ball can fall, and the second and the third should be caught. A difficult variance of this task is a “flash” cascade with three balls, which means that each ball should be thrown and caught once at pace. In this task, exercisers should try to throw the balls alternately along a parabolic trajectory and catch them all. One repetition of this task should proceed in the following order: (1) throw the first ball; (2) throw the second ball; (3) throw the third ball; (4) catch the first ball; (5) catch the second ball; (6) catch the third ball. This task is also the aim of this protocol. The next step in this task is to juggle continuously for a long sequence. An easier version of this task consists of throwing three balls in a parabolic trajectory but focusing on only one of them (the first, the second or the third), and this ball should be caught, while the other two may fall to the ground.
2.4. Statistical Methods
2.5. Sample Size Calculation
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van der Willik, K.D.; Licher, S.; Vinke, E.J.; Knol, M.J.; Darweesh, S.K.L.; van der Geest, J.N.; Schagen, S.B.; Ikram, M.K.; Luik, A.I.; Ikram, M.A. Trajectories of Cognitive and Motor Function between Ages 45 and 90 Years: A Population-Based Study. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear 2015, 36, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor Control and Aging: Links to Age-Related Brain Structural, Functional, and Biochemical Effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.; Moreno-Agostino, D.; Chua, K.-C.; Vitoratou, S.; Prina, A.M. Trajectories of Healthy Ageing among Older Adults with Multimorbidity: A Growth Mixture Model Using Harmonised Data from Eight ATHLOS Cohorts. PLoS ONE 2021, 16, e0248844. [Google Scholar] [CrossRef]
- Rovio, S.; Kåreholt, I.; Helkala, E.-L.; Viitanen, M.; Winblad, B.; Tuomilehto, J.; Soininen, H.; Nissinen, A.; Kivipelto, M. Leisure-Time Physical Activity at Midlife and the Risk of Dementia and Alzheimer’s Disease. Lancet Neurol. 2005, 4, 705–711. [Google Scholar] [CrossRef]
- Hernández-Mendo, A.; Reigal, R.E.; López-Walle, J.M.; Serpa, S.; Samdal, O.; Morales-Sánchez, V.; Juárez-Ruiz de Mier, R.; Tristán-Rodríguez, J.L.; Rosado, A.F.; Falco, C. Physical Activity, Sports Practice, and Cognitive Functioning: The Current Research Status. Front. Psychol. 2019, 10, 2658. [Google Scholar] [CrossRef] [Green Version]
- Hübner, L.; Voelcker-Rehage, C. Does Physical Activity Benefit Motor Performance and Learning of Upper Extremity Tasks in Older Adults?—A Systematic Review. Eur. Rev. Aging Phys. Act. 2017, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Wu, C.; Teng, C.; Hsu, W.; Chang, K.; Chen, P. Evolving Methods to Combine Cognitive and Physical Training for Individuals with Mild Cognitive Impairment: Study Protocol for a Randomized Controlled Study. Trials 2016, 17, 526. [Google Scholar] [CrossRef] [Green Version]
- Niemann, C.; Godde, B.; Voelcker-Rehage, C. Not Only Cardiovascular, but Also Coordinative Exercise Increases Hippocampal Volume in Older Adults. Front. Aging Neurosci. 2014, 6, 170. [Google Scholar] [CrossRef] [Green Version]
- Albouy, G.; Sterpenich, V.; Balteau, E.; Vandewalle, G.; Desseilles, M.; Dang-Vu, T.; Darsaud, A.; Ruby, P.; Luppi, P.-H.; Degueldre, C.; et al. Both the Hippocampus and Striatum Are Involved in Consolidation of Motor Sequence Memory. Neuron 2008, 58, 261–272. [Google Scholar] [CrossRef]
- Voelcker-Rehage, C.; Godde, B.; Staudinger, U.M. Cardiovascular and Coordination Training Differentially Improve Cognitive Performance and Neural Processing in Older Adults. Front. Hum. Neurosci. 2011, 5, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, G.; Herbsleb, M.; de la Cruz, F.; Schumann, A.; Köhler, S.; Puta, C.; Gabriel, H.W.; Reichenbach, J.R.; Bär, K.-J. Changes in FMRI Activation in Anterior Hippocampus and Motor Cortex during Memory Retrieval after an Intense Exercise Intervention. Biol. Psychol. 2017, 124, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Kattenstroth, J.-C.; Kalisch, T.; Holt, S.; Tegenthoff, M.; Dinse, H.R. Six Months of Dance Intervention Enhances Postural, Sensorimotor, and Cognitive Performance in Elderly without Affecting Cardio-Respiratory Functions. Front. Aging Neurosci. 2013, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, R.A.; Lee, T.D. Motor Control and Learning: A Behavioral Emphasis, 4th ed.; Human Kinetics: Champaign, IL, USA, 2005; pp. vi, 535. ISBN 978-0-7360-4258-1. [Google Scholar]
- Malik, J.; Stemplewski, R.; Maciaszek, J. The Effect of Juggling as Dual-Task Activity on Human Neuroplasticity: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 7102. [Google Scholar] [CrossRef] [PubMed]
- Driemeyer, J.; Boyke, J.; Gaser, C.; Büchel, C.; May, A. Changes in Gray Matter Induced by Learning—Revisited. PLoS ONE 2008, 3, e2669. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.L.; King, A.C. Evaluating the Efficacy of Physical Activity for Influencing Quality-of-Life Outcomes in Older Adults. Ann. Behav. Med. 1991, 13, 108–116. [Google Scholar]
- Steptoe, A. Depression and Physical Illness; Cambridge University Press: Cambridge, UK, 2006; ISBN 978-1-139-45930-3. [Google Scholar]
- Steptoe, A.; Deaton, A.; Stone, A.A. Psychological Wellbeing, Health and Ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef] [Green Version]
- Lyubomirsky, S.; King, L.; Diener, E. The Benefits of Frequent Positive Affect: Does Happiness Lead to Success? Psychol. Bull. 2005, 131, 803–855. [Google Scholar] [CrossRef] [Green Version]
- McAuley, E.; Rudolph, D. Physical Activity, Aging, and Psychological Well-Being. J. Aging Phys. Act. 1995, 3, 67–96. [Google Scholar] [CrossRef]
- Arent, S.; Landers, D.; Etnier, J. The Effects of Exercise on Mood in Older Adults: A Meta-Analytic Review. J. Aging Phys. Act. 2000, 8, 407–430. [Google Scholar] [CrossRef]
- Stathi, A.; McKenna, J.; Fox, K. Processes Associated with Participation and Adherence to a 12-Month Exercise Programme for Adults Aged 70 and Older. J. Health Psychol. 2010, 15, 838–847. [Google Scholar] [CrossRef] [PubMed]
- McMurdo, M.E.T.; Burnett, L. Randomised Controlled Trial of Exercise in the Elderly. GER 1992, 38, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Veale, J.F. Edinburgh Handedness Inventory—Short Form: A Revised Version Based on Confirmatory Factor Analysis. Laterality 2014, 19, 164–177. [Google Scholar] [CrossRef] [PubMed]
- Bonsignore, M.; Barkow, K.; Jessen, F.; Heun, R. Validity of the Five-Item WHO Well-Being Index (WHO-5) in an Elderly Population. Eur. Arch. Psychiatry Clin. Neurosci. 2001, 251, II27–II31. [Google Scholar] [PubMed]
- Cichoń, E.; Kiejna, A.; Kokoszka, A.; Gondek, T.; Rajba, B.; Lloyd, C.E.; Sartorius, N. Validation of the Polish Version of WHO-5 as a Screening Instrument for Depression in Adults with Diabetes. Diabetes Res. Clin. Pract. 2020, 159, 107970. [Google Scholar] [CrossRef]
- Boyke, J.; Driemeyer, J.; Gaser, C.; Büchel, C.; May, A. Training-Induced Brain Structure Changes in the Elderly. J. Neurosci. 2008, 28, 7031–7035. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Rosenbaum, S.; Richards, J.; Ward, P.B.; Veronese, N.; Solmi, M.; Cadore, E.L.; Stubbs, B. Exercise for Depression in Older Adults: A Meta-Analysis of Randomized Controlled Trials Adjusting for Publication Bias. Braz. J. Psychiatry 2016, 38, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E. The Status of Health Assessment 1994. Annu. Rev. Public Health 1995, 16, 327–354. [Google Scholar] [CrossRef]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Yarmohammadi, S.; Mozafar Saadati, H.; Ghaffari, M.; Ramezankhani, A. A Systematic Review of Barriers and Motivators to Physical Activity in Elderly Adults in Iran and Worldwide. Epidemiol. Health 2019, 41, e2019049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, W.; Brown, P.R. Motivators, Facilitators, and Barriers to Physical Activity in Older Adults: A Qualitative Study. Holist. Nurs. Pract. 2017, 31, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Nejati, V.; Kordi, R.; Shoaee, F. Evaluation of Effective Motivators and Barriers of Physical Activity in the Elderly. Iran. J. Ageing 2010, 4. Available online: http://salmandj.uswr.ac.ir/article-1-305-en.html (accessed on 30 November 2022).
- Mortazavi, S.S.; Eftekhar Ardebili, H.; Eshaghi, S.R.; Dorali Beni, R.; Shahsiah, M.; Botlani, S. The Effectiveness of Regular Physical Activity on Mental Health in Elderly. J. Isfahan Med. Sch. 2011, 29, 1805–1814. [Google Scholar]
- Voelcker-Rehage, C.; Willimczik, K. Motor Plasticity in a Juggling Task in Older Adults-a Developmental Study. Age Ageing 2006, 35, 422–427. [Google Scholar] [CrossRef] [Green Version]
- Moral-García, J.; García, D.; García, S.; Amatria, M.; Dios, R. Influence of Physical Activity on Self-Esteem and Risk of Dependence in Active and Sedentary Elderly People. An. Psicol. 2018, 34, 162–166. [Google Scholar] [CrossRef] [Green Version]
- Elavsky, S.; McAuley, E.; Motl, R.W.; Konopack, J.F.; Marquez, D.X.; Hu, L.; Jerome, G.J.; Diener, E. Physical Activity Enhances Long-Term Quality of Life in Older Adults: Efficacy, Esteem, and Affective Influences. Ann. Behav. Med. 2005, 30, 138–145. [Google Scholar] [CrossRef]
- Eliezer, D.; Major, B.; Mendes, W.B. The Costs of Caring: Gender Identification Increases Threat Following Exposure to Sexism. J. Exp. Soc. Psychol. 2010, 46, 159–165. [Google Scholar] [CrossRef]
- de Groot, G.C.L.; Fagerström, L. Older Adults’ Motivating Factors and Barriers to Exercise to Prevent Falls. Scand. J. Occup. Ther. 2011, 18, 153–160. [Google Scholar] [CrossRef]
- Yoo, S.; Kim, D.H. Perceived Urban Neighborhood Environment for Physical Activity of Older Adults in Seoul, Korea: A Multimethod Qualitative Study. Prev. Med. 2017, 103S, S90–S98. [Google Scholar] [CrossRef]
- Stevens, M.; Lieschke, J.; Cruwys, T.; Cárdenas, D.; Platow, M.J.; Reynolds, K.J. Better Together: How Group-Based Physical Activity Protects against Depression. Soc. Sci. Med. 2021, 286, 114337. [Google Scholar] [CrossRef] [PubMed]
- Chippendale, T.; Boltz, M. The Neighborhood Environment: Perceived Fall Risk, Resources, and Strategies for Fall Prevention. Gerontologist 2015, 55, 575–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowal, J.; Fortier, M.S. Physical Activity Behavior Change in Middle-Aged and Older Women: The Role of Barriers and of Environmental Characteristics. J. Behav. Med. 2007, 30, 233–242. [Google Scholar] [CrossRef]
- Faulkner, J.; O’Brien, W.J.; McGrane, B.; Wadsworth, D.; Batten, J.; Askew, C.D.; Badenhorst, C.; Byrd, E.; Coulter, M.; Draper, N.; et al. Physical Activity, Mental Health and Well-Being of Adults during Initial COVID-19 Containment Strategies: A Multi-Country Cross-Sectional Analysis. J. Sci. Med. Sport 2021, 24, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.G.P.; Crowe, S.M.; Tyndall, M.W. Planning for the Next Global Pandemic. Int. J. Infect. Dis. 2015, 38, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in Physical Activity and Sedentary Behaviours from before to during the COVID-19 Pandemic Lockdown: A Systematic Review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Jenkins, M.; Houge Mackenzie, S.; Hodge, K.; Hargreaves, E.A.; Calverley, J.R.; Lee, C. Physical Activity and Psychological Well-Being during the COVID-19 Lockdown: Relationships with Motivational Quality and Nature Contexts. Front. Sport. Act. Living 2021, 3, 637576. [Google Scholar] [CrossRef]
- Welburn, K. Juggling-Exposure Therapy: An Innovation in Trauma Treatment. J. Trauma Dissociation 2015, 16, 39–50. [Google Scholar] [CrossRef]
- Nakahara, T.; Nakahara, K.; Uehara, M.; Koyama, K.; Li, K.; Harada, T.; Yasuhara, D.; Taguchi, H.; Kojima, S.; Sagiyama, K.; et al. Effect of Juggling Therapy on Anxiety Disorders in Female Patients. BioPsychoSoc. Med. 2007, 1, 10. [Google Scholar] [CrossRef] [Green Version]
- Sazgar, M.; Carlen, P.L.; Wennberg, R. Panic Attack Semiology in Right Temporal Lobe Epilepsy. Epileptic Disord 2003, 5, 93–100. [Google Scholar]
- Scholz, J.; Klein, M.C.; Behrens, T.E.J.; Johansen-Berg, H. Training Induces Changes in White Matter Architecture. Nat. Neurosci. 2009, 12, 1370–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, T.; Gerber, P.; Schmidt-Wilcke, T. Juggling Increases Interhemispheric Brain Connectivity: A Visual and Quantitative DMRI Study. Vision 2012, VMV12, 217–218. [Google Scholar] [CrossRef]
- Draganski, B.; Gaser, C.; Busch, V.; Schuierer, G.; Bogdahn, U.; May, A. Neuroplasticity: Changes in Grey Matter Induced by Training. Nature 2004, 427, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Gerber, P.; Schlaffke, L.; Borowy, S.; Greenlee, M.; Schultz, T.; Schmidt-Wilcke, T. Juggling Revisited—A Voxel–Based Morphometry Study with Expert Jugglers. NeuroImage 2014, 95, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Carius, D.; Andrä, C.; Clauß, M.; Ragert, P.; Bunk, M.; Mehnert, J. Hemodynamic Response Alteration As a Function of Task Complexity and Expertise-An FNIRS Study in Jugglers. Front. Hum. Neurosci. 2016, 10, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voelcker-Rehage, C. Motor-Skill Learning in Older Adults—A Review of Studies on Age-Related Differences. Eur. Rev. Aging Phys. Act. 2008, 5, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Sampaio-Baptista, C.; Scholz, J.; Jenkinson, M.; Thomas, A.G.; Filippini, N.; Smit, G.; Douaud, G.; Johansen-Berg, H. Gray Matter Volume Is Associated with Rate of Subsequent Skill Learning after a Long Term Training Intervention. Neuroimage 2014, 96, 158–166. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | PRE Mean ± SD | POST Mean ± SD |
|---|---|---|
| Age | 70.55 ± 4.91 | - |
| Body mass [kg] | 67.55 ± 14.11 | 67.85 ± 13.58 |
| Height [cm] | 161.50 ± 8.79 | - |
| BMI [kg/m2] | 25.82 ± 3.77 | 25.97 ± 3.73 |
| Handedness 1 | 91.88 ± 13.27 | - |
| POST | |||
|---|---|---|---|
| PRE | WHO-5 < 13 Points [n] | WHO-5 ≥ 13 Points [n] | Total |
| WHO-5 < 13 points [n] | 1 | 9 * | 10 |
| WHO-5 ≥ 13 points [n] | 0 * | 10 | 10 |
| Total | 1 | 19 | 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malik, J.; Maciaszek, J. Effect of the Juggling-Based Motor Learning Physical Activity on Well-Being in Elderly: A Pre–Post Study with a Special Training Protocol. Healthcare 2022, 10, 2442. https://doi.org/10.3390/healthcare10122442
Malik J, Maciaszek J. Effect of the Juggling-Based Motor Learning Physical Activity on Well-Being in Elderly: A Pre–Post Study with a Special Training Protocol. Healthcare. 2022; 10(12):2442. https://doi.org/10.3390/healthcare10122442
Chicago/Turabian StyleMalik, Jakub, and Janusz Maciaszek. 2022. "Effect of the Juggling-Based Motor Learning Physical Activity on Well-Being in Elderly: A Pre–Post Study with a Special Training Protocol" Healthcare 10, no. 12: 2442. https://doi.org/10.3390/healthcare10122442