
Event History Analysis of Factors Affecting Survival of Older Adults in Taiwan
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Statistical Analysis
- 1.
- The Cox time-dependent frailty survival model
- 2.
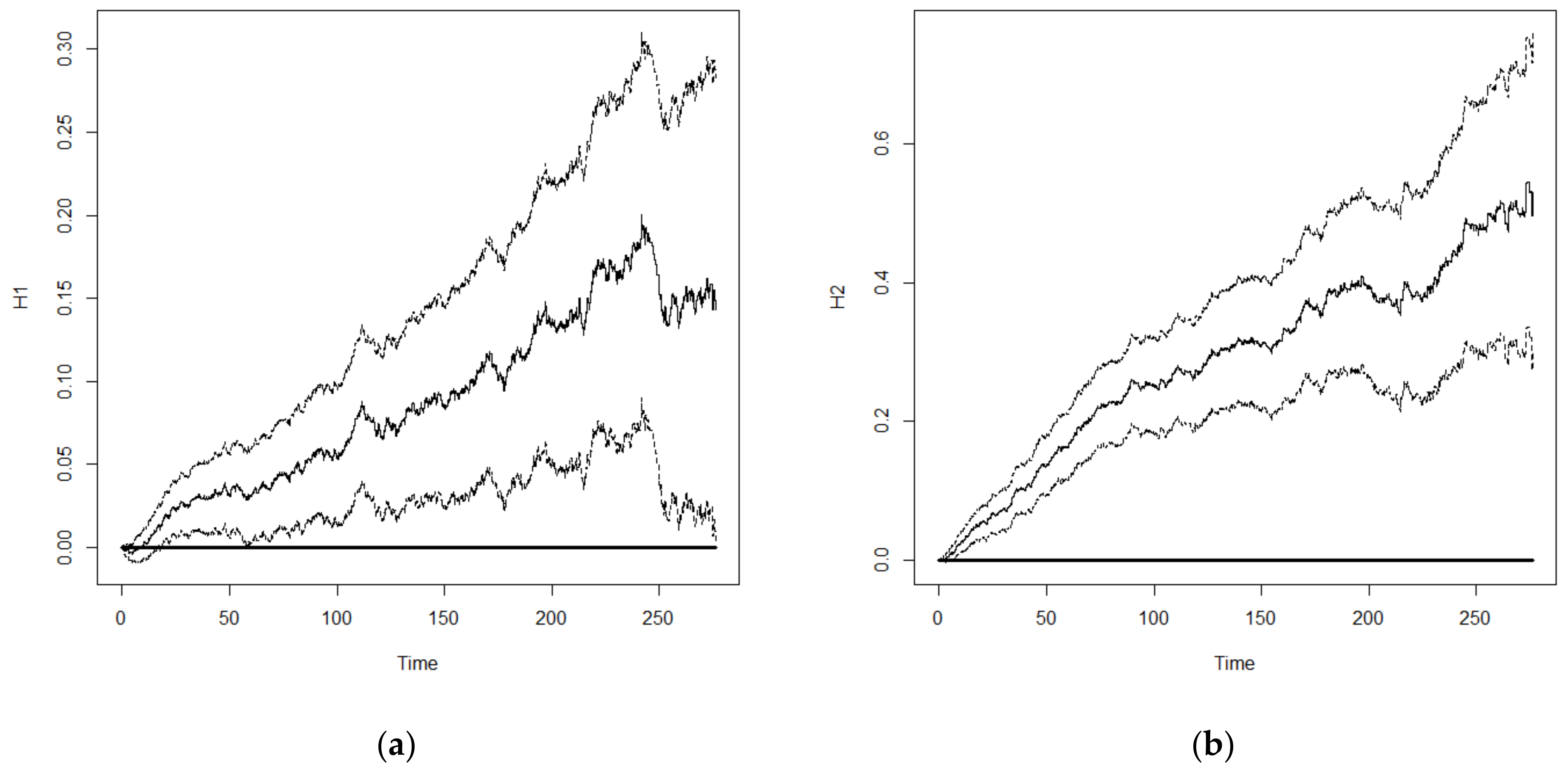
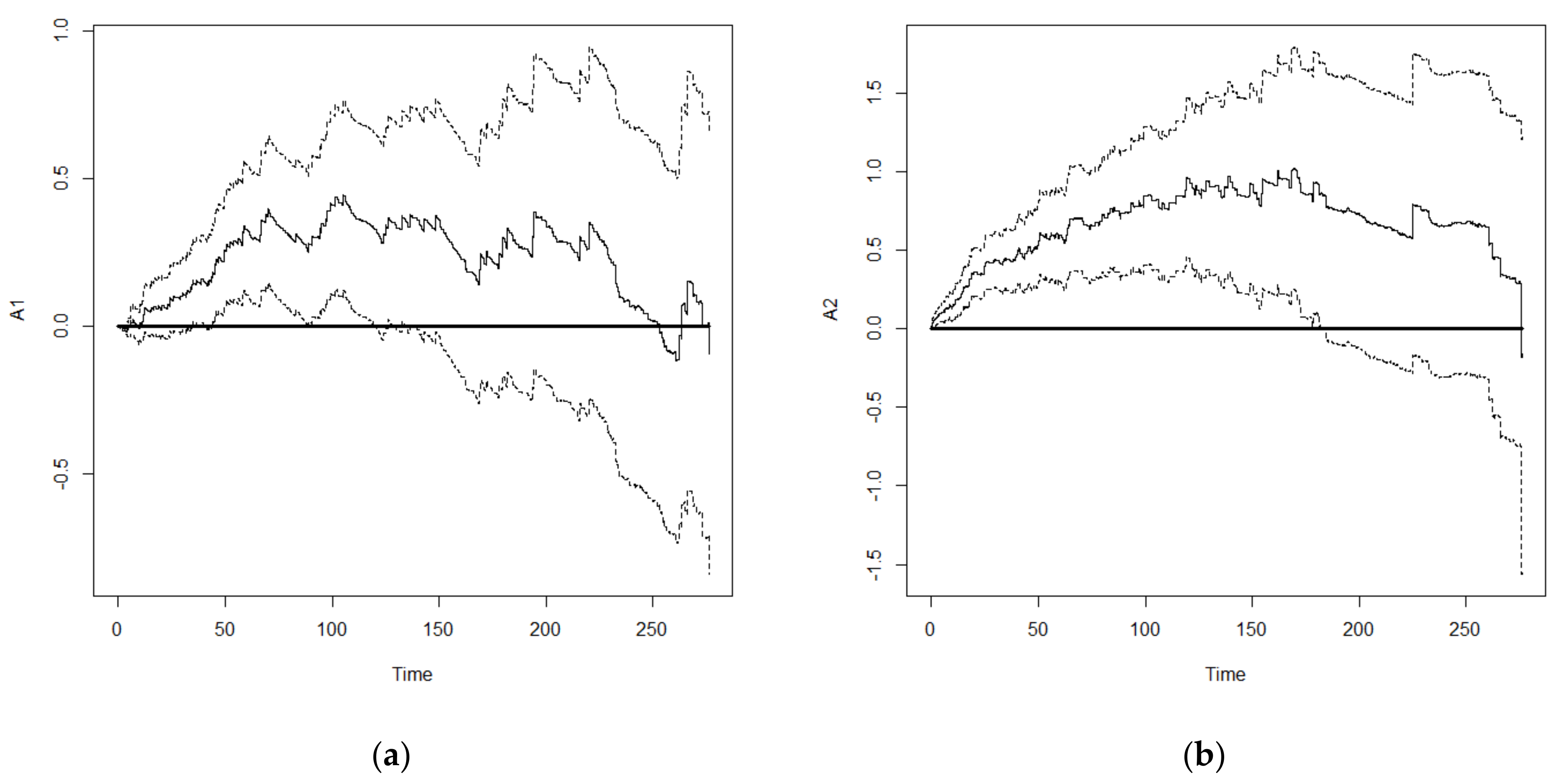
- Aalen’s nonparametric additive model
3. Results
- Age: The risk of death increased significantly with age and the risk of death was 4.071 times higher in subjects aged ≥70 years compared with that in those aged 60–64 years.
- Gender: The risk of death in males was 1.912 times higher than in females.
- Population: The risk of death in mainlanders was lower than in other populations and 0.814 times lower than that of the Fukien population.
- Education level: The risk of death for subjects with an education level of up to senior high school and above, junior high school, and elementary school was 0.728, 0.736, and 0.826 times, respectively, compared with that of illiterate subjects. There was no significant difference between subjects with an education level of up to junior high school and those with an education level of up to senior high school. This was due to the fact that most people at that time did not have a high education level.
- ADL status: There was no significant difference in subjects with independence and fair ADL; however, the risk of death was 2.399 times higher in subjects with poor ADL compared with those with independence in ADL.
- Physical performance: The risk of death for subjects with common and poor physical performance was 1.578 and 2.492 times higher than that of those with good physical performance.
- Self-rated health: The risk of death for subjects with fair and poor self-rated health was 1.207 and 1.815 times higher than that of those with good health.
- Current smoking status: The risk of death for smokers was 1.399 times higher than that for non-smokers.
- Current betel nut chewing status: The risk of death for betel nut chewers was 1.344 times higher than that for non-betel nut chewers.
- Spouse: The risk of death of subjects with no spouse was 1.395 times higher than that of those with a spouse.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nieddu, A.; Vindas, L.; Errigo, A.; Vindas, J.; Pes, G.M.; Dore, M.P. Dietary Habits, Anthropometric Features and Daily Performance in Two Independent Long-Lived Populations from Nicoya peninsula (Costa Rica) and Ogliastra (Sardinia). Nutrients 2020, 12, 1621. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J. A Study on Link Functions for Modelling and Forecasting Old-Age Survival Probabilities of Australia and New Zealand. Risks 2021, 9, 11. [Google Scholar] [CrossRef]
- Yang, S.; Wang, D.; Li, W.; Wang, C.; Yang, X.; Lo, K. Decoupling of Elderly Healthcare Demand and Expenditure in China. Healthcare 2021, 9, 1346. [Google Scholar] [CrossRef]
- Zhang, L.; Fu, S.; Fang, Y. Prediction the Contribution Rate of Long-Term Care Insurance for the Aged in China Based on the Balance of Supply and Demand. Sustainability 2020, 12, 3144. [Google Scholar] [CrossRef] [Green Version]
- Ye, L.; Luo, J.; Shia, B.-C.; Fang, Y. Multidimensional Health Groups and Healthcare Utilization Among Elderly Chinese: Based on the 2014 CLHLS Dataset. Int. J. Environ. Res. Public Health 2019, 16, 3884. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Meng, Y. Is China Moving toward Healthy Aging? A Tracking Study Based on 5 Phases of CLHLS Data. Int. J. Environ. Res. Public Health 2020, 17, 4343. [Google Scholar] [CrossRef]
- Feng, Y.; Liu, E.; Yue, Z.; Zhang, Q.; Han, T. The Evolutionary Trends of Health Behaviors in Chinese Elderly and the Influencing Factors of These Trends: 2005–2014. Int. J. Environ. Res. Public Health 2019, 16, 1687. [Google Scholar] [CrossRef] [Green Version]
- National Development Council. Population Projections for ROC (Taiwan): 2020~2070; National Development Council: Taipei, Taiwan, 2020. Available online: https://pop-proj.ndc.gov.tw/download.aspx?uid=70&pid=70 (accessed on 15 December 2021).
- Gove, W.R. Sex, Marital Status and Mortality. Am. J. Sociol. 1973, 79, 45–67. [Google Scholar] [CrossRef]
- Hu, Y.; Goldman, N. Mortality Differentials by Marital Status: An International Comparison. Demography 1990, 27, 233–250. [Google Scholar] [CrossRef]
- Preston, S. Mortality Patterns in National Populations; Academic: New York, NY, USA, 1976. [Google Scholar]
- Tu, J.C. On Long-term Mortality Trends in Taiwan, 1906–1980. Taiwan. J. Sociol. 1985, 9, 145–164. [Google Scholar]
- Liu, X.; Hermalin, A.I.; Chuang, Y.L. The Effect of Education on Mortality among Older Taiwanese and its Pathways. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1998, 53, S71–S82. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Lin, H.S. Factors Associated with Survival Status of Order Taiwanese Adults. Taiwan J. Public Health 2006, 25, 351–362. [Google Scholar]
- Liu, S.C.; Lin, C.H. Effect of Factors with Time-dependent Covariates on the Survival Status of the Elderly in Taiwan. Qual. Quant. 2012, 46, 237–249. [Google Scholar] [CrossRef]
- Lin, C.H.; Liu, S.C. Factors related to survival rates of the elderly in different cohorts in Taiwan. Taiwan J. Public Health 2012, 31, 597–611. [Google Scholar]
- Lin, C.H.; Liu, S.C. Healthy life expectancy for successful aging and active aging elderly in Taiwan. Taiwan J. Public Health 2013, 32, 562–575. [Google Scholar]
- Hsu, H.C.; Pwu, R.F. Too Late to Quit? Effect of Smoking and Smoking Cessation on Morbidity and Mortality among the Elderly in a Longitudinal Study. Kaohsiung J. Med. Sci. 2004, 20, 484–491. [Google Scholar] [CrossRef] [Green Version]
- Lan, T.Y.; Chang, W.C.; Tsai, Y.J.; Chuang, Y.L.; Lin, H.S.; Tai, T.Y. Areca Nut Chewing and Mortality in an Elderly Cohort Study. Am. J. Epidemiol. 2007, 165, 677–683. [Google Scholar] [CrossRef] [Green Version]
- Mete, C. Predictors of Elderly Mortality: Health Status, Socioeconomic Characteristics and Social Determinants of Health. Health Econ. 2005, 14, 135–148. [Google Scholar] [CrossRef]
- Ho, S.H. Survival Analysis of Living Arrangements and Health Care Utilization in Terms of Total Mortality among the Middle Aged and Elderly in Taiwan. J. Nurs. Res. 2008, 16, 160–168. [Google Scholar] [CrossRef]
- Wang, H.P. Gender Differences in Hazard Rate Affecting Death in the Elderly Population in Taiwan. Kaohsiung J. Med. Sci. 2006, 22, 277–285. [Google Scholar] [CrossRef] [Green Version]
- Gee, E.M.; Kimball, M.M. Women and Health. In Women and Aging; Gee, E.M., Kimball, M.M., Eds.; Butterworths: New York, NY, USA, 1987; pp. 29–52. [Google Scholar]
- Hsu, H.C. Does Social Participation by the Elderly Reduce Mortality and Cognitive Impairment? Aging Ment. Health 2007, 11, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Lan, T.Y.; Lan, T.H.; Wen, C.P. Nighttime Sleep, Chinese Afternoon Nap, and Mortality in the Elderly. Sleep 2007, 30, 1105–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.T.; James, M.K.; Miller, M.E. The Timing of Change: Patterns in Transitions in Functional Status among Elderly Persons. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1998, 53, S17–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molarius, A.; Janson, S. Self-rated, Chronic Disease, and Symptoms among Middle-aged and Elderly Men and Women. J. Clin. Epidemiol. 2002, 55, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.K.; Huang, Z.S.; Ng, S.K.; Chan, K.W.A.; Wang, Y.S.; Liu, H.W.; Lee, J.J. Impact of Alcohol Consumption and Cigarette Smoking on Stroke among the Elderly in Taiwan. Stroke 1995, 26, 790–794. [Google Scholar] [CrossRef]
- Tsai, A.C.; Liou, J.C.; Chang, M.C. Interview to Study the Determinants of Hypertension in Older Adults in Taiwan: A Population Based Cross-sectional Survey. Asia Pac. J. Clin. Nutr. 2007, 16, 338–345. [Google Scholar]
- Ho, S.H.; Li, C.S.; Liu, C.C. The Influence of Chronic Disease, Physical Function, and Lifestyle on Health Transition among the Middle-aged and Older Person in Taiwan. J. Nurs. Res. 2009, 17, 136–143. [Google Scholar] [CrossRef]
- Badawi, G.; Gariepy, G.; Page, V.; Schmitz, N. Indicators of Self-rated Health in the Canadian Population with Diabetes. Diabetic Med. 2012, 29, 1021–1028. [Google Scholar] [CrossRef]
- Adams, J.; Kuchibhatla, M.; Christopher, E.J.; Alexander, J.D.; Clary, G.L.; Cuffe, M.S.; Califf, R.M.; Krishnan, R.R.; O’Connor, C.M.; Jiang, W. Association of Depression and Survival in Patients with Chronic Heart Failure over 12 Years. Psychosomatics 2012, 53, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.H.; Cheng, W.F. The Effect of Educational Differentials on Mortality of the Elderly in Taiwan. Taiwan J. Public Health 2011, 30, 58–71. [Google Scholar]
- Wang, J.Y.; Tsai, A.C. The Short-form Mini-Nutritional Assessment is as Effective as the Full-Mini Nutritional Assessment in Predicting Follow-up 4-year Mortality in Elderly Taiwanese. J. Nutr. Health Aging 2013, 17, 594–598. [Google Scholar] [CrossRef]
- Wang, S.H.; Wang, J.Y. The Decline in Physical and Mental Health among Older Chronic Stroke Patients in Taiwan. Taiwan J. Public Health 2013, 32, 383–392. [Google Scholar]
- Chiu, H.P.; Tsai, A.C.; Wang, J.Y. Combined Effect of Body Mass Index and Physical Activity on the Decline in Walking Ability amongst Older Taiwanese. Taiwan J. Public Health 2014, 33, 637–648. [Google Scholar]
- Beckett, M.; Goldman, N.; Weinstein, M.; Lin, I.F.; Chuang, Y.L. Social Environment, Life Challenge, and Health among the Elderly in Taiwan. Soc. Sci. Med. 2002, 55, 191–209. [Google Scholar] [CrossRef]
- Bruce, B.; Fries, J.F.; Hubert, H. Regular Vigorous Physical Activity and Disability Development in Healthy Overweight and Normal-weight Seniors: A 13-year Study. Am. J. Public Health 2008, 98, 1294–1299. [Google Scholar] [CrossRef]
- Cornman, J.C.; Goldman, N.; Glei, D.A.; Weinstein, M.; Chang, M.C. Social Ties and Perceived Support: Two Dimensions of Social Relationships and Health among the Elderly in Taiwan. J. Aging Health 2003, 15, 616–644. [Google Scholar] [CrossRef]
- Glei, D.A.; Landau, D.A.; Goldman, N.; Chuang, Y.L.; Rodríguez, G.; Weinstein, M. Participating in Social Activities Helps Preserve Cognitive Function: An Analysis of a Longitudinal, Population-based Study of the Elderly. Int. J. Epidemiol. 2005, 34, 864–871. [Google Scholar] [CrossRef]
- Ofstedal, M.B.; Zimmer, Z.S.; Lin, H.S. A Comparison of Correlates of Cognitive Functioning in Older Persons in Taiwan and the United States. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1999, 54, S291–S301. [Google Scholar] [CrossRef]
- Seplaki, C.L.; Goldman, N.; Weinstein, M.; Lin, Y.H. Before and after the 1999 Chi-Chi Earthquake: Traumatic Events and Depressive Symptoms in an Older Population. Soc. Sci. Med. 2006, 62, 3121–3132. [Google Scholar] [CrossRef] [Green Version]
- Tsai, A.C.; Chi, S.H.; Wang, J.Y. Association of Perceived Stress with Depressive Symptoms in Older Taiwanese: Results of a Population-based Study. Geriatr. Gerontol. Int. 2015, 15, 535–543. [Google Scholar] [CrossRef]
- Wu, S.C.; Leu, S.Y.; Li, C.Y. Incidence of and Predictors for Chronic Disability in Activities of Daily Living among Older People in Taiwan. J. Am. Geriatr. Soc. 1999, 47, 1082–1086. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, Z.; Liu, X.; Hermalin, A.; Chuang, Y.L. Educational Attainment and Transitions in Functional Status among Older Taiwanese. Demography 1998, 35, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.J.; Wang, J.Y. Association between reading and cognitive decline in older Taiwanese people. Taiwan J. Public Health 2016, 35, 94–104. [Google Scholar]
- Cornman, J.C.; Lynch, S.M.; Goldman, N.; Weinstein, M.; Lin, H.S. Stability and Change in the Perceived Social Support of Older Taiwanese Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2004, 59, S350–S357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, S.H.; Wang, J.Y.; Tsai, A.C. Combined Association of Leisure-time Physical Activity and Fruit and Vegetable Consumption with Depressive Symptoms in Older Taiwanese: Results of a National Cohort Study. Geriatr. Gerontol. Int. 2016, 16, 244–251. [Google Scholar] [CrossRef]
- Glaser, K.; Agree, E.M.; Costenbader, E.; Camargo, A.; Trench, B.; Natividad, J.; Chuang, Y.L. Fertility Decline, Family Structure, and Support for Older Persons in Latin America and Asia. J. Aging Health 2006, 18, 259–291. [Google Scholar] [CrossRef]
- Hsu, W.C.; Chen, L.C.; Wang, J.Y. Predicting Emerging Care-need with Simple Functional Indicators-Findings from a National Cohort Study in Taiwan. Geriatr. Gerontol. Int. 2017, 17, 375–381. [Google Scholar] [CrossRef]
- Wu, S.C.; Liang, J.; Chang, M.C.; Lin, H.S.; Maloy, N. Utilization of Health Services among the Elderly in Taiwan. Chin. J. Public Health 1994, 13, 168–182. [Google Scholar]
- Zimmer, Z.; Martin, L.G.; Chang, M.C. Changes in functional limitation and survival among older Taiwanese, 1993, 1996, and 1999. Popul. Stud. 2002, 56, 265–276. [Google Scholar] [CrossRef]
- Kleinbaum, D.G.; Klein, M. Survival Analysis: A Self-Learning Text; Springer: New York, NY, USA, 2005. [Google Scholar]
- Aalen, O.O. A linear Regression Model for the Analysis of Lifetimes. Stat. Med. 1989, 8, 907–925. [Google Scholar] [CrossRef]
- Aalen, O.O. Further Results on the Nonparametric Linear Regression Model in Survival Analysis. Stat. Med. 1993, 12, 1569–1588. [Google Scholar] [CrossRef]
- Wu, S.C.; Chiang, T.L. Long-Term Care in Taiwan: Issues and Directions. Chin. J. Public Health 1995, 14, 246–255. [Google Scholar]
- Word Health Organization. The Use of Epidemiology in the Study of Elderly: Report of a WHO Scientific Group on the Epidemiology of Aging; Word Health Organization: Geneva, Switzerland, 1984. [Google Scholar]
- Idler, E.L.; Kasl, S. Health Perceptions and Survival: Do Global Evaluations of Health Status Really Predict Mortality? J. Gerontol. 1991, 46, S56–S65. [Google Scholar] [CrossRef]
- Fuller, T.D.; Edward, J.N.; Sermsri, S.; Vorakitphokatorn, S. Gender and Health: Some Asian Evidence. J. Health Soc. Behav. 1993, 34, 252–271. [Google Scholar] [CrossRef]
- Johnson, R.J.; Wolinsky, F.D. Gender, Race, and Health: The Structure of Health Status among Older Adults. Gerontologist 1994, 34, 24–35. [Google Scholar] [CrossRef]
- Liang, C.C.; Hsu, W.C.; Tsai, Y.T.; Weng, S.J.; Yang, H.P.; Liu, S.C. Healthy Life Expectancies by the Effects of Hypertension and Diabetes for the Middle Aged and Over in Taiwan. Int. J. Env. Res. Public Health 2020, 17, 4390. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n | % | Variable | n | % | ||
|---|---|---|---|---|---|---|---|
| Age | 60–64 | 1482 | 36.60 | ADL a | Independence | 3801 | 94.04 |
| 65–69 | 1152 | 28.45 | Function | Slight | 93 | 2.30 | |
| 70–74 | 725 | 17.91 | Severe | 148 | 3.66 | ||
| 75–79 | 438 | 10.82 | Physical b | Good | 3307 | 81.74 | |
| 80+ | 252 | 6.22 | Function | Common | 510 | 12.61 | |
| Gender | Male | 1738 | 42.92 | Poor | 229 | 5.66 | |
| Female | 2311 | 57.08 | Self-rated | Good | 1526 | 37.99 | |
| Ethnicity | Fukien | 2451 | 60.92 | Health | Fair | 1491 | 37.12 |
| Hakka | 603 | 14.99 | Poor | 1000 | 24.89 | ||
| Mainlander | 900 | 22.37 | Residential | City | 1917 | 47.35 | |
| Aborigine | 69 | 1.72 | Location | Town | 726 | 17.93 | |
| Education | Illiterate | 1676 | 41.58 | Countryside | 1406 | 34.72 | |
| Elementary | 1595 | 39.57 | Economic | Good | 1683 | 43.20 | |
| Junior High | 327 | 8.11 | Status | Fair | 1524 | 39.12 | |
| Senior High+ | 433 | 10.74 | Poor | 689 | 17.68 | ||
| Spouse | No | 1429 | 35.31 | Depression c | No | 3036 | 77.91 |
| Yes | 2618 | 64.69 | Yes | 861 | 22.09 | ||
| Current Smoking | No | 2649 | 65.44 | Outdoor | No | 143 | 3.53 |
| Yes | 1399 | 34.56 | Activity | Yes | 3906 | 96.47 | |
| Current Chewing | No | 3825 | 94.58 | Social | No | 2485 | 61.37 |
| Betel Nut | Yes | 219 | 5.42 | Activity | Yes | 1564 | 38.63 |
| Model | Description |
|---|---|
| Model 1 | Demographic (Age group, Gender, Ethnicity, Education) |
| Model 2 | Model 1 + Physical and Mental health statuses (ADL, Physical Function, Self-rated Health, Depression) |
| Model 3 | Model 1+ Health behavior (Current Smoking, Current Chewing Betel Nut, Outdoor Activity) |
| Model 4 | Model 1 + Family environment + Social participation (Spouse, Residential Location, Economic Status, Social Activity) |
| Model 5 | Full Model: Demographic + Physical and Mental health statuses + Family environment + Social participation + Health behavior |
| Model 6 | Reduced Model: Age group + Gender + Ethnicity+ Education +ADL+ Physical Function + Self-rated Health + Current Smoking, Current Chewing Betel Nut+ Spouse |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | ||
|---|---|---|---|---|---|---|---|
| Variable | HR | HR | HR | HR | HR | HR | |
| Age | 60–64 | 1 | 1 | 1 | 1 | 1 | 1 |
| 65–69 | 1.632 *** | 1.694 *** | 1.662 *** | 1.627 *** | 1.682 *** | 1.721 *** | |
| 70+ | 3.935 *** | 3.951 *** | 4.162 *** | 3.688 *** | 3.935 *** | 4.071 *** | |
| Gender | Male | 1 | 1 | 1 | 1 | 1 | 1 |
| Female | 1.714 *** | 2.085 *** | 1.542 *** | 1.874 *** | 1.919 *** | 1.912 *** | |
| Ethnicity | Fukien | 1 | 1 | 1 | 1 | 1 | 1 |
| Hakka | 1.001 | 1.007 | 1.027 | 1.008 | 1.031 | 1.027 | |
| Mainlander | 0.856 ** | 0.828 ** | 0.882 * | 0.821 *** | 0.813 ** | 0.814 ** | |
| Aborigine | 1.355 * | 1.287 | 1.149 | 1.384 * | 1.115 | 1.113 | |
| Education | Illiterate | 1 | 1 | 1 | 1 | 1 | 1 |
| Elementary | 0.806 *** | 0.852 ** | 0.799 *** | 0.850 ** | 0.847 ** | 0.826 *** | |
| Junior High | 0.640 *** | 0.712 *** | 0.649 *** | 0.712 *** | 0.760 ** | 0.736 ** | |
| Senior High+ | 0.604 *** | 0.658 *** | 0.636 *** | 0.666 *** | 0.728 *** | 0.728 *** | |
| ADL | Independence | 1 | 1 | 1 | |||
| Function | Slight | 1.326 | 1.266 | 1.318 | |||
| Severe | 1.677 ** | 1.749 ** | 2.399 *** | ||||
| Physical | Good | 1 | 1 | 1 | |||
| Function | Common | 1.564 *** | 1.565 *** | 1.578 *** | |||
| Poor | 2.404 *** | 2.445 *** | 2.492 *** | ||||
| Depression | No | 1 | 1 | ||||
| Yes | 1.102 | 1.077 | |||||
| Self-rated | Good | 1 | 1 | 1 | |||
| Health | Fair | 1.186 *** | 1.189 ** | 1.207 *** | |||
| Poor | 1.632 *** | 1.659 *** | 1.815 *** | ||||
| Current Smoking | No | 1 | 1 | 1 | |||
| Yes | 1.275 *** | 1.374 *** | 1.399 *** | ||||
| Current Chewing | No | 1 | 1 | 1 | |||
| Betel Nut | Yes | 1.394 *** | 1.335 ** | 1.344 ** | |||
| Outdoor | No | 1 | 1 | ||||
| Activity | Yes | 2.404 *** | 0.969 | ||||
| Spouse | No | 1 | 1 | 1 | |||
| Yes | 1.297 *** | 1.338 *** | 1.395 *** | ||||
| Residential | City | 1 | 1 | ||||
| Location | Town | 1.004 | 0.964 | ||||
| Countryside | 1.029 | 0.978 | |||||
| Economic | Good | 1 | 1 | ||||
| Status | Fair | 1.105 * | 1.022 | ||||
| Poor | 1.310 *** | 0.992 | |||||
| Social | No | 1 | 1 | ||||
| Activity | Yes | 1.122 ** | 1.089 |
| Rank | Age | Gender | Spouse | HR a |
|---|---|---|---|---|
| 1 | 60~64 | Female | Yes | 1.000 |
| 2 | 60~64 | Female | No | 1.395 |
| 3 | 65~69 | Female | Yes | 1.721 |
| 4 | 60~64 | Male | Yes | 1.912 |
| 5 | 65~69 | Female | No | 2.401 |
| 6 | 60~64 | Male | No | 2.667 |
| 7 | 65~69 | Male | Yes | 3.290 |
| 8 | 70~ | Female | Yes | 4.071 |
| 9 | 65~69 | Male | No | 4.591 |
| 10 | 70~ | Female | No | 5.680 |
| 11 | 70~ | Male | Yes | 7.783 |
| 12 | 70~ | Male | No | 10.85 |
| Cox Model | Aalen Model | |||||
|---|---|---|---|---|---|---|
| Variable | Coeff | SE | p-Value | |Z| | p-Value | |
| Age | 60–64 (ref) | |||||
| 65–69 | 0.543 | 0.058 | <0.001 | 8.590 | <0.001 | |
| 70+ | 1.404 | 0.060 | <0.001 | 20.300 | <0.001 | |
| Gender | Male | 0.648 | 0.062 | <0.001 | 9.790 | <0.001 |
| Female (ref) | ||||||
| Ethnicity | Fukien (ref) | |||||
| Hakka | 0.027 | 0.064 | 0.668 | 0.403 | 0.687 | |
| Mainlander | -0.206 | 0.064 | 0.001 | 3.580 | <0.001 | |
| Aborigine | 0.107 | 0.178 | 0.546 | 0.228 | 0.820 | |
| Education | Illiterate (ref) | |||||
| Elementary | -0.191 | 0.056 | <0.001 | 2.990 | 0.003 | |
| Junior High | -0.307 | 0.096 | 0.001 | 3.130 | 0.002 | |
| Senior High+ | -0.318 | 0.092 | <0.001 | 3.590 | <0.001 | |
| ADL | Independence (ref) | |||||
| Function | Slight | 0.276 | 0.154 | 0.072 | 1.810 | 0.070 |
| Severe | 0.875 | 0.163 | <0.001 | 4.200 | <0.001 | |
| Physical | Good (ref) | |||||
| Function | Common | 0.456 | 0.074 | <0.001 | 5.130 | <0.001 |
| Poor | 0.913 | 0.132 | <0.001 | 4.920 | <0.001 | |
| Self-rated | Good (ref) | |||||
| Health | Fair | 0.188 | 0.053 | <0.001 | 3.220 | 0.001 |
| Poor | 0.596 | 0.065 | <0.001 | 7.280 | <0.001 | |
| Current Smoking | No (ref) | |||||
| Yes | 0.336 | 0.056 | <0.001 | 5.820 | <0.001 | |
| Current Chewing | No (ref) | |||||
| Betel Nut | Yes | 0.296 | 0.102 | 0.004 | 2.630 | 0.009 |
| Spouse | No | |||||
| Yes (ref) | 0.333 | 0.050 | <0.001 | 5.130 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, Y.-C.; Hsu, W.-C.; Weng, S.-J.; Tsai, Y.-T.; Liu, S.-C.; Lin, C.-H. Event History Analysis of Factors Affecting Survival of Older Adults in Taiwan. Healthcare 2022, 10, 2439. https://doi.org/10.3390/healthcare10122439
Lo Y-C, Hsu W-C, Weng S-J, Tsai Y-T, Liu S-C, Lin C-H. Event History Analysis of Factors Affecting Survival of Older Adults in Taiwan. Healthcare. 2022; 10(12):2439. https://doi.org/10.3390/healthcare10122439
Chicago/Turabian StyleLo, Yuan-Chen, Wei-Chung Hsu, Shao-Jen Weng, Yao-Te Tsai, Shih-Chia Liu, and Cheng-Hsiang Lin. 2022. "Event History Analysis of Factors Affecting Survival of Older Adults in Taiwan" Healthcare 10, no. 12: 2439. https://doi.org/10.3390/healthcare10122439