
The Risk of SARS-CoV-2 Infection in Pregnant Women: An Observational Cohort Study Using the BIFAP Database

Abstract
:1. Introduction
2. Material and Methods
2.1. Data Source
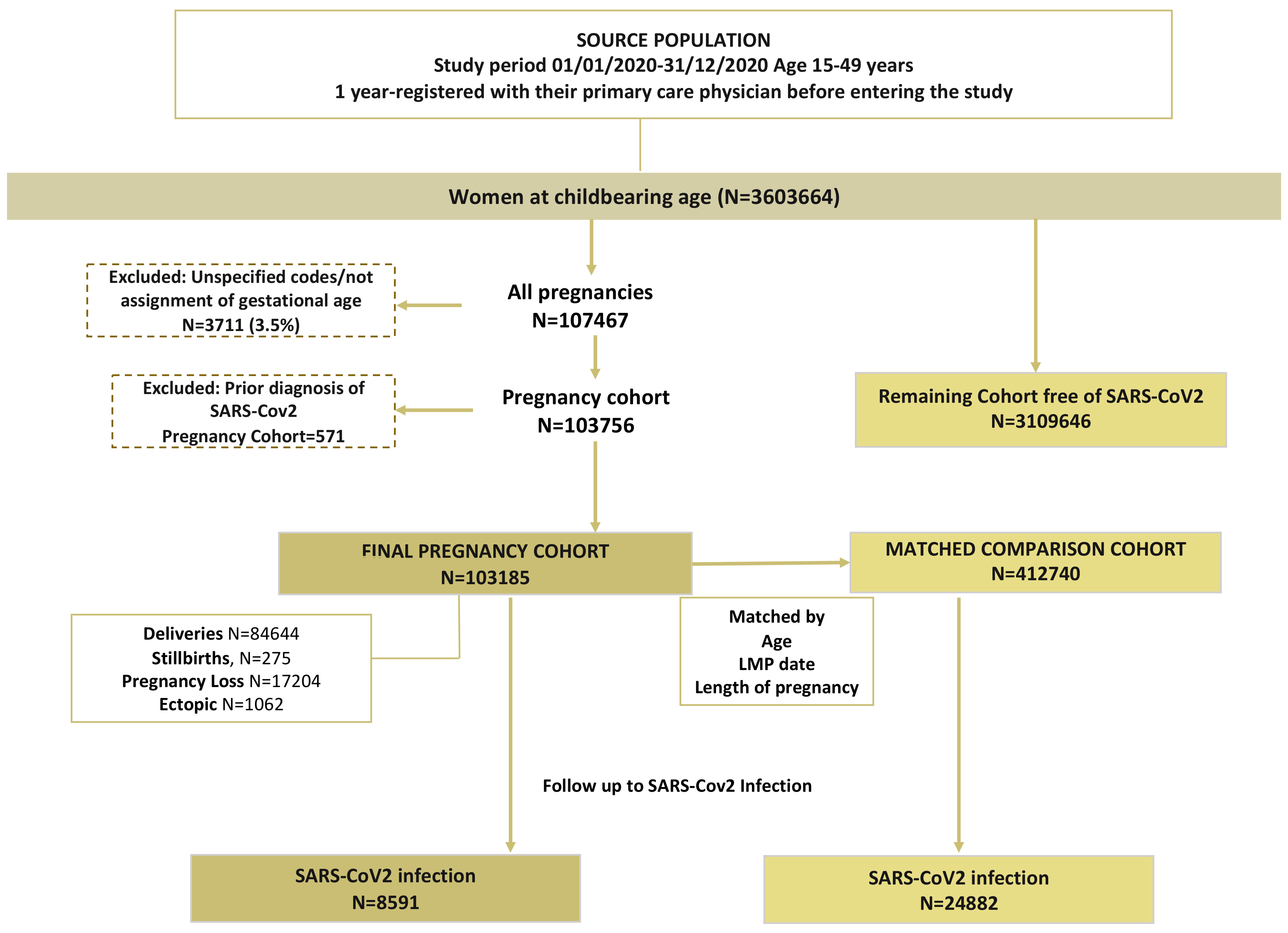
2.2. Source Population
2.3. Identification of the Cohort of Pregnant Women, Gestation Time and Comparison Cohort
2.4. Follow–Up and Outcome Identification
2.5. Covariables
2.6. Statistical Analysis
3. Results
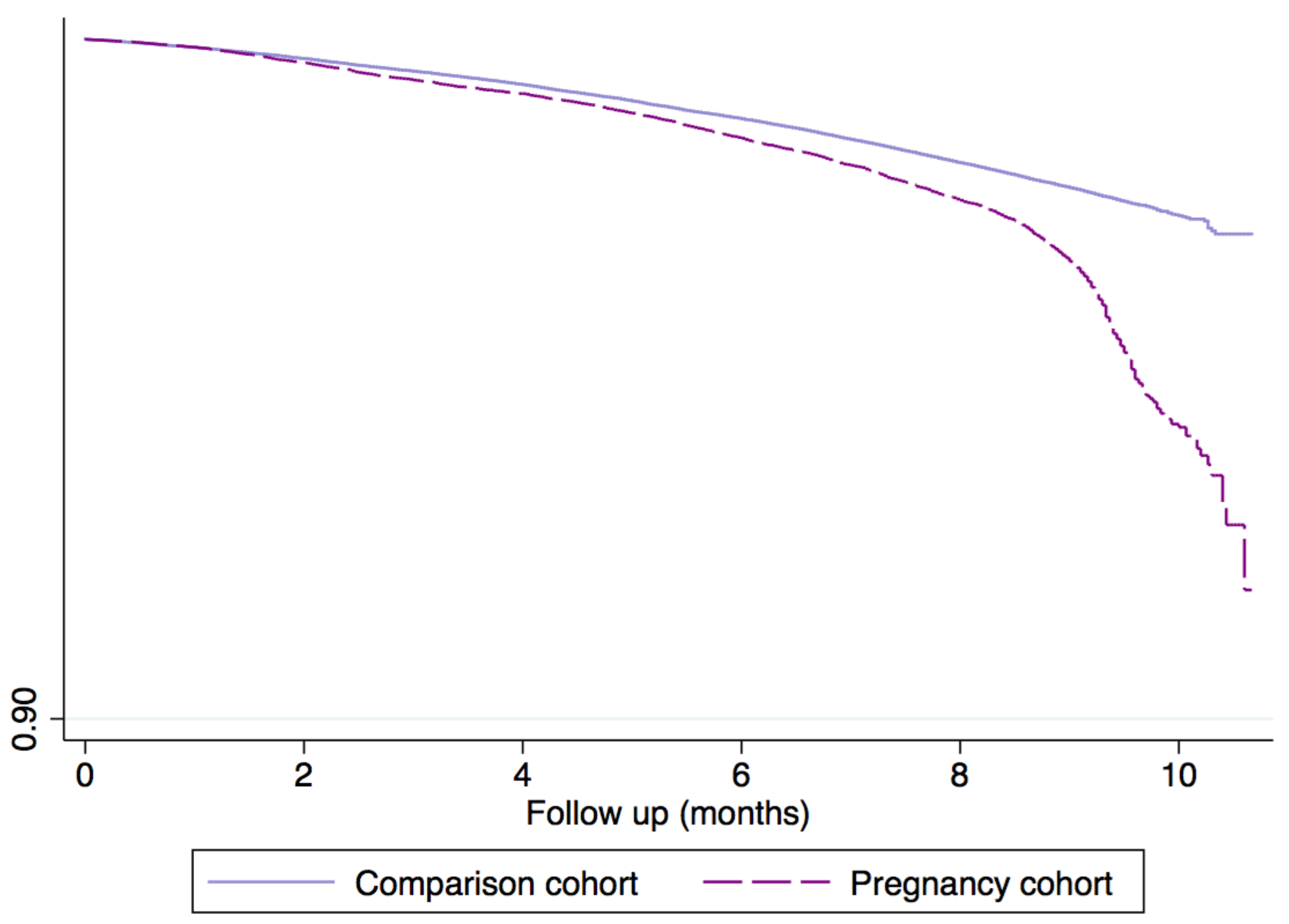
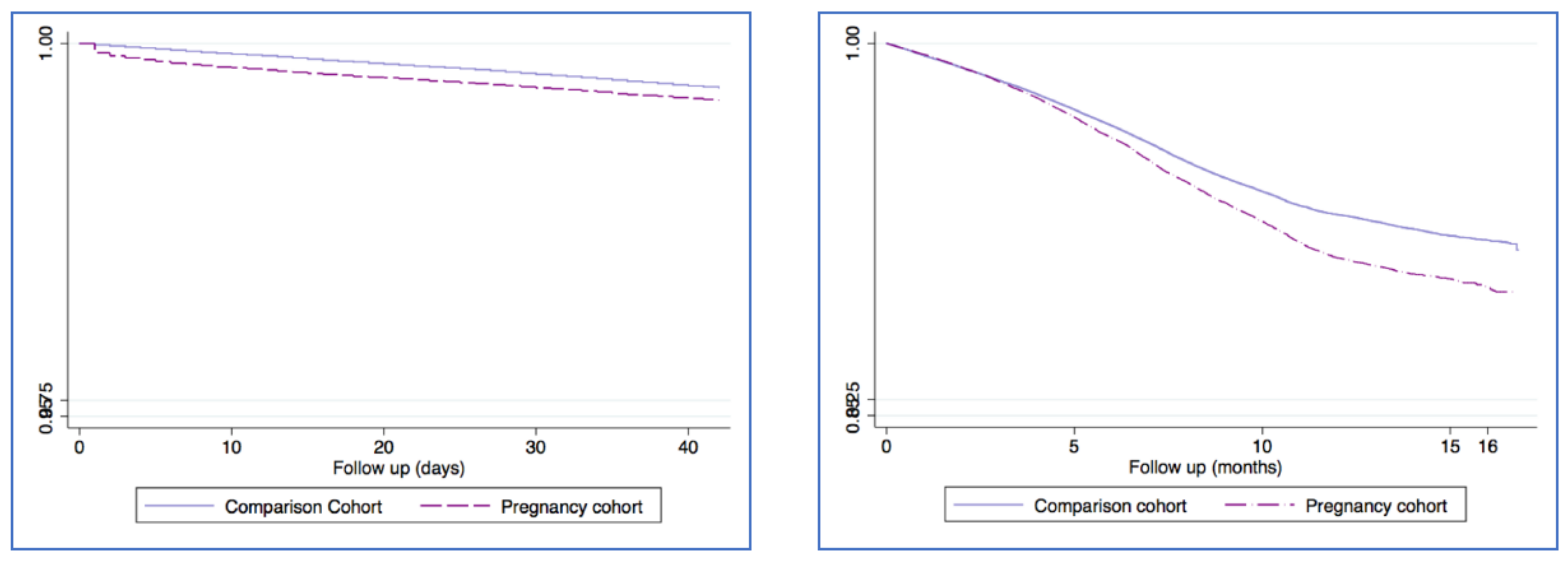
3.1. SAR-CoV-2 Infection Onset among Both Cohorts
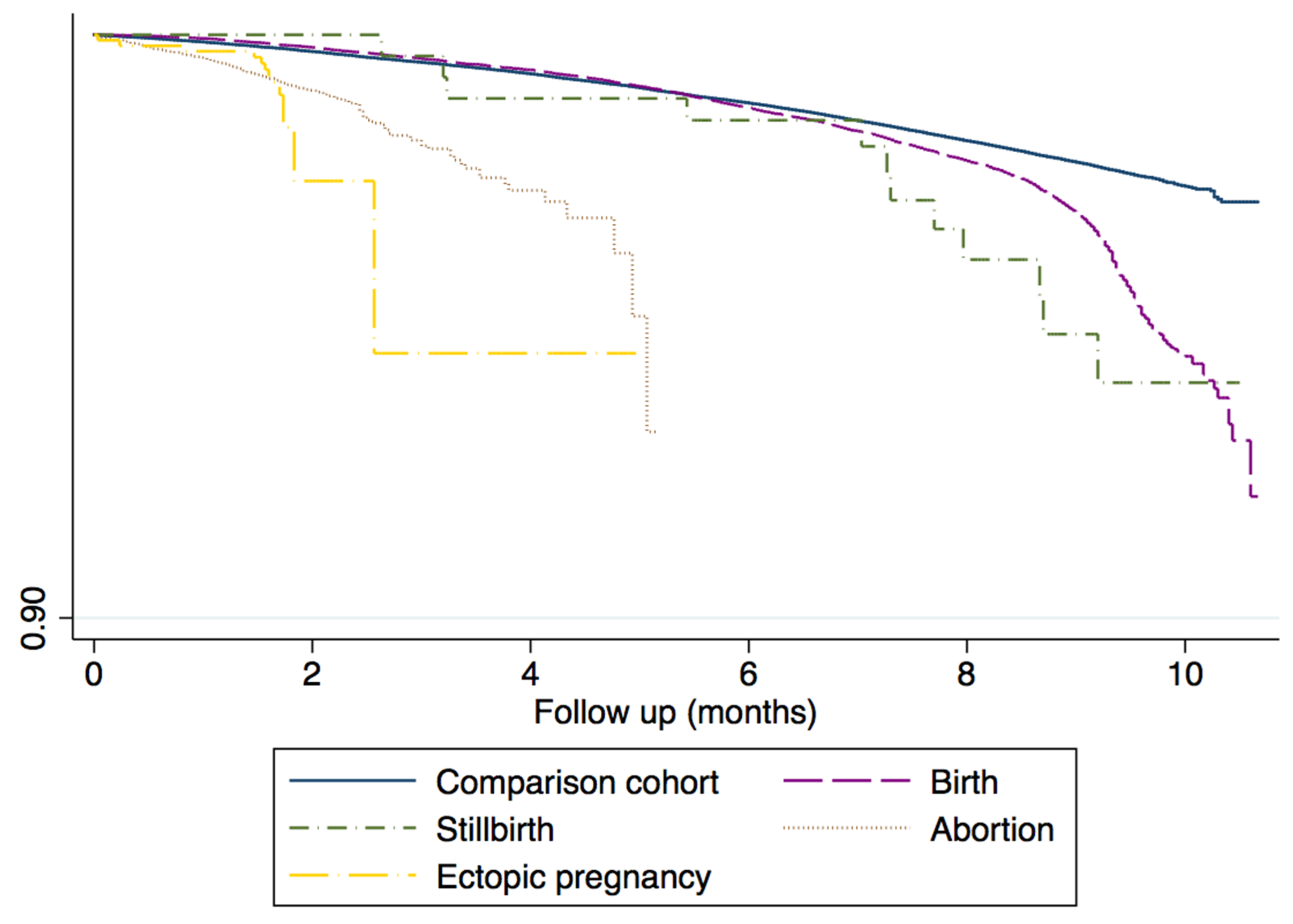
3.2. COVID-19 Onset According with Pregnancy Event
3.3. Clinical Course of SARS-CoV-2 Infection
3.4. Cox Regression Analysis: Risk Factors for SARS-CoV-2 Infection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silasi, M.; Cardenas, I.; Kwon, J.Y.; Racicot, K.; Aldo, P.; Mor, G. Viral infections during pregnancy. Am. J. Reprod. Immunol. 2015, 73, 199–213. Available online: https://pubmed.ncbi.nlm.nih.gov/25582523/ (accessed on 23 April 2022). [CrossRef] [PubMed] [Green Version]
- Wastnedge, E.A.N.; Reynolds, R.M.; Van Boeckel, S.R.; Stock, S.J.; Denison, F.C.; Maybin, J.A.; Critchley, H.O.D. Pregnancy and COVID-19. Physiol. Rev. 2021, 101, 303–318. Available online: https://journals.physiology.org/doi/full/10.1152/physrev.00024.2020 (accessed on 3 April 2022). [CrossRef] [PubMed]
- Favre, G.; Pomar, L.; Musso, D.; Baud, D. 2019-nCoV epidemic: What about pregnancies? Lancet 2020, 395, e40. Available online: https://pubmed.ncbi.nlm.nih.gov/32035511/ (accessed on 10 April 2022). [CrossRef] [PubMed] [Green Version]
- Schwartz, D.A.; Graham, A.L. Potential Maternal and Infant Outcomes from (Wuhan) Coronavirus 2019-nCoV Infecting Pregnant Women: Lessons from SARS, MERS, and Other Human Coronavirus Infections. Viruses 2020, 12, 194. Available online: https://pubmed.ncbi.nlm.nih.gov/32050635/ (accessed on 3 April 2022). [CrossRef] [PubMed] [Green Version]
- Goodnight, W.H.; Soper, D.E. Pneumonia in pregnancy. Crit. Care Med. 2005, 33, (Suppl. 10), S390–S397. Available online: https://pubmed.ncbi.nlm.nih.gov/16215363/ (accessed on 3 April 2022). [CrossRef]
- Di Renzo, G.C.; Giardina, I. Coronavirus disease 2019 in pregnancy: Consider thromboembolic disorders and thrombo-prophylaxis. Am. J. Obstet. Gynecol. 2020, 223, 135. Available online: https://pubmed.ncbi.nlm.nih.gov/32333857/ (accessed on 3 April 2022). [CrossRef]
- Poon, L.C.; Yang, H.; Lee, J.C.S.; Copel, J.A.; Leung, T.Y.; Zhang, Y.; Chen, D.; Prefumo, F. ISUOG Interim Guidance on 2019 novel coronavirus infection during pregnancy and puerperium: Information for healthcare professionals. Ultrasound Obstet. Gynecol. 2020, 55, 700–708. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-H.; Keller, J.; Wang, I.-T.; Lin, C.-C.; Lin, H.-C. Pneumonia and pregnancy outcomes: A nationwide population-based study. Am. J. Obstet. Gynecol. 2012, 207, 288.e1–288.e7. Available online: https://pubmed.ncbi.nlm.nih.gov/23021691/ (accessed on 23 April 2022). [CrossRef]
- Di Mascio, D.; Khalil, A.; Saccone, G.; Rizzo, G.; Buca, D.; Liberati, M.; Vecchiet, J.; Nappi, L.; Scambia, G.; Berghella, V.; et al. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100107. [Google Scholar] [CrossRef]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. Can. Med. Assoc. J. 2021, 193, E540–E548. Available online: https://pubmed.ncbi.nlm.nih.gov/33741725/ (accessed on 3 April 2022). [CrossRef]
- Di Toro, F.; Gjoka, M.; Di Lorenzo, G.; De Santo, D.; De Seta, F.; Maso, G.; Risso, F.M.; Romano, F.; Wiesenfeld, U.; Levi-D’Ancona, R.; et al. Impact of COVID-19 on maternal and neonatal outcomes: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 27, 36–46. [Google Scholar] [CrossRef]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.-F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. Available online: https://pubmed.ncbi.nlm.nih.gov/32283155/ (accessed on 3 April 2022). [CrossRef]
- Khalil, A.; Hill, R.; Ladhani, S.; Pattisson, K.; O’Brien, P. Severe acute respiratory syndrome coronavirus 2 in pregnancy: Symp-tomatic pregnant women are only the tip of the iceberg. Am. J. Obstet. Gynecol. 2020, 223, 296–297. Available online: https://pubmed.ncbi.nlm.nih.gov/32387327/ (accessed on 3 April 2022). [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, 3320. Available online: https://www.bmj.com/content/370/bmj.m3320 (accessed on 3 April 2022). [CrossRef]
- Jafari, M.; Pormohammad, A.; Neshin, S.A.S.; Ghorbani, S.; Bose, D.; Alimohammadi, S.; Basirjafari, S.; Mohammadi, M.; Rasmussen-Ivey, C.; Razizadeh, M.H.; et al. Clinical characteristics and outcomes of pregnant women with COVID-19 and comparison with control patients: A systematic review and meta-analysis. Rev. Med. Virol. 2021, 31, 1–16. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/rmv.2208 (accessed on 3 April 2022). [CrossRef]
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, January 22–June 7, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 769–775. Available online: https://pubmed.ncbi.nlm.nih.gov/32584795/ (accessed on 3 April 2022). [CrossRef]
- Lokken, E.M.; Taylor, G.G.; Huebner, E.M.; Vanderhoeven, J.; Hendrickson, S.; Coler, B.; Sheng, J.S.; Walker, C.L.; McCartney, S.A.; Kretzer, N.M.; et al. Higher severe acute respiratory syn-drome coronavirus 2 infection rate in pregnant patients. Am. J. Obstet. Gynecol.2021, 225, 75.e1–75.e16. Available online: https://pubmed.ncbi.nlm.nih.gov/33607103/ (accessed on 3 April 2022).
- Maciá-Martínez, M.; Gil, M.; Huerta, C.; Martín-Merino, E.; Álvarez, A.; Bryant, V.; Montero, D.; Bifap the BIFAP Team. Base de Datos para la Investigación Farmacoepidemiológica en Atención Primaria (BIFAP): A data resource for pharmacoepidemiology in Spain. Pharmacoepidemiol. Drug Saf. 2020, 29, 1236–1245. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/pds.5006 (accessed on 12 April 2022). [CrossRef]
- Gobernanza del Acceso a los Datos de BIFAP Agencia Española de Medicamentos y Productos Sanitarios (n.d.). 28 January 2021. Available online: http://bifap.aemps.es/docs/Gobernanza_acceso_datos_BIFAP_v1_Junio2017.pdf (accessed on 4 October 2022).
- World Organization of Family Doctors (WONCA) International Classification Committee. International Classification of Primary Care (ICPC), 2nd ed.; Oxford University Press, Oxford Medical Publications: Oxford, UK, 1998. [Google Scholar]
- eCIE-Maps—CIE-9-MC. Available online: https://eciemaps.mscbs.gob.es/ecieMaps/browser/index_9_mc.html (accessed on 3 April 2022).
- WHOCC—ATC/DDD Index. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 3 April 2022).
- Gil, M.; Rodríguez-Miguel, A.; Montoya-Catalá, H.; González, R.G.; Álvarez-Gutiérrez, A.; Rodríguez-Martín, S.; García-Rodríguez, L.A.; De Abajo, F.J. Validation study of colorectal cancer diagnosis in the Spanish primary care database, BIFAP. Pharmacoepidemiol. Drug Saf. 2019, 28, 209–216. Available online: https://pubmed.ncbi.nlm.nih.gov/30548462/ (accessed on 3 April 2022). [CrossRef]
- Sanchez Ortiz, S.; Llorente García, A.; Astasio, P.; Huerta, C.; Cea Soriano, L. An algorithm to identify pregnancies in BIFAP Primary Care database in Spain: Results from a cohort of 155,419 pregnancies. Pharmacoepidemiol. Drug Saf. 2020, 29, 57–68. Available online: https://pubmed.ncbi.nlm.nih.gov/31749191/ (accessed on 23 April 2022). [CrossRef]
- Vintzileos, W.S.; Muscat, J.; Hoffmann, E.; John, N.S.; Vertichio, R.; Vintzileos, A.M.; Vo, D. Screening all pregnant women admitted to labor and delivery for the virus responsible for coronavirus disease 2019. Am. J. Obstet. Gynecol. 2020, 223, 284–286. Available online: https://pubmed.ncbi.nlm.nih.gov/32348743/ (accessed on 3 April 2022). [CrossRef] [PubMed]
- Sutton, D.; Fuchs, K.; D’Alton, M.; Goffman, D. Universal Screening for SARS-CoV-2 in Women Admitted for Delivery. N. Engl. J. Med. 2020, 382, 2163–2164. Available online: https://pubmed.ncbi.nlm.nih.gov/32283004/ (accessed on 3 April 2022). [CrossRef] [PubMed]
- Pregnancy|COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/special-populations/pregnancy/ (accessed on 3 April 2022).
- Prochaska, E.; Jang, M.; Burd, I. COVID-19 in pregnancy: Placental and neonatal involvement. Am. J. Reprod. Immunol. 2020, 84, e13306. Available online: https://pubmed.ncbi.nlm.nih.gov/32779810/ (accessed on 3 April 2022). [CrossRef] [PubMed]
- Kazemi, S.N.; Hajikhani, B.; Didar, H.; Hosseini, S.S.; Haddadi, S.; Khalili, F.; Mirsaeidi, M.; Nasiri, M.J. COVID-19 and cause of pregnancy loss during the pandemic: A systematic review. PLoS ONE 2021, 16, e0255994. Available online: https://pubmed.ncbi.nlm.nih.gov/34379700/ (accessed on 23 April 2022). [CrossRef] [PubMed]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F., III; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, January 22–October 3, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm6944e3.htm (accessed on 3 April 2022). [CrossRef]
- Home—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 10 April 2022).
- Badr, D.A.; Mattern, J.; Carlin, A.; Cordier, A.-G.; Maillart, E.; El Hachem, L.; El Kenz, H.; Andronikof, M.; De Bels, D.; Damoisel, C.; et al. Are clinical outcomes worse for pregnant women at ≥20 weeks’ gestation infected with coronavirus disease 2019? A multicenter case-control study with propensity score matching. Am. J. Obstet. Gynecol. 2020, 223, 764–768. Available online: https://pubmed.ncbi.nlm.nih.gov/32730899/ (accessed on 9 April 2022). [CrossRef]
- Salehi, L.; Rahimzadeh, M.; Molaei, E.; Zaheri, H.; Esmaelzadeh-Saeieh, S. The relationship among fear and anxiety of COVID-19, pregnancy experience, and mental health disorder in pregnant women: A structural equation model. Brain Behav. 2020, 10, e01835. Available online: https://pubmed.ncbi.nlm.nih.gov/32969190/ (accessed on 3 April 2022). [CrossRef]
- Jia, X.; Yin, C.; Lu, S.; Chen, Y.; Liu, Q.; Bai, J.; Lu, Y. Two Things about COVID-19 Might Need Attention. 2020. Available online: https://www.preprints.org/manuscript/202002.0315/v1 (accessed on 3 April 2022).
- Peter, B.; Ree Ni Ferrer, K.; Younes, L.; Lepe, B.; Manhal, K.; Mydam, J. Risk Factors Associated with COVID-19 Symptoms and Potential Vertical Transmission during Pregnancy: A Retrospective Cohort Study. Cureus 2022, 14, e22900. Available online: https://www.cureus.com/articles/79301-risk-factors-associated-with-covid-19-symptoms-and-potential-vertical-transmission-during-pregnancy-a-retrospective-cohort-study (accessed on 3 April 2022). [CrossRef]
- Donath, M.Y.; Shoelson, S.E. Type 2 diabetes as an inflammatory disease. Nat. Rev. Immunol. 2011, 11, 98–107. [Google Scholar] [CrossRef]
- Grossmann, V.; Schmitt, V.H.; Zeller, T.; Panova-Noeva, M.; Schulz, A.; Laubert-Reh, D.; Juenger, C.; Schnabel, R.B.; Abt, T.G.; Laskowski, R.; et al. Profile of the Immune and Inflammatory Response in Individuals with Prediabetes and Type 2 Diabetes. Diabetes Care 2015, 38, 1356–1364. Available online: https://pubmed.ncbi.nlm.nih.gov/25877811/ (accessed on 3 April 2022). [CrossRef] [Green Version]
- Chris Pirschel|ONS Voice. Available online: https://voice.ons.org/author/chris-pirschel (accessed on 3 April 2022).
- ScienceDirect. International Immunopharmacology|Vol 90, January 2021. Available online: https://www.sciencedirect.com/journal/international-immunopharmacology/vol/90/suppl/C?page=2 (accessed on 3 April 2022).
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; de Larrea, N.F.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. Available online: http://www.thelancet.com/article/S0140673620314835/fulltext (accessed on 3 April 2022). [CrossRef]
- Rozenfeld, Y.; Beam, J.; Maier, H.; Haggerson, W.; Boudreau, K.; Carlson, J.; Medows, R. A model of disparities: Risk factors associated with COVID-19 infection. Int. J. Equity Health 2020, 19, 126. Available online: https://equityhealthj.biomedcentral.com/articles/10.1186/s12939-020-01242-z (accessed on 3 April 2022). [CrossRef]
- Karmakar, M.; Lantz, P.M.; Tipirneni, R. Association of Social and Demographic Factors with COVID-19 Incidence and Death Rates in the US. JAMA Netw. Open 2021, 4, e2036462. Available online: https://pubmed.ncbi.nlm.nih.gov/33512520/ (accessed on 3 April 2022). [CrossRef]
- Servicios Bifap. Available online: https://herramientas2bifap.aemps.es/ServiciosBifap/ (accessed on 23 April 2022).
- Ministerio de Sanidad. Portal Estadístico del SNS—Encuesta Nacional de Salud de España 2017. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/encuestaResDetall2017.htm (accessed on 23 April 2022).
- Martín-Merino, E.; Calderón-Larrañaga, A.; Hawley, S.; Poblador-Plou, B.; Llorente-García, A.; Petersen, I.; Prieto-Alhambra, D. The impact of different strategies to handle missing data on both precision and bias in a drug safety study: A multidatabase multinational population-based cohort study. Clin. Epidemiol. 2018, 10, 643. [Google Scholar] [CrossRef] [Green Version]
- León-Muñoz, L.M.; Duarte-Salles, T.; Llorente, A.; Díaz, Y.; Puente, D.; Pottegård, A.; Montero-Corominas, D.; Huerta, C. Use of hydrochlorothiazide and risk of skin cancer in a large nested case-control study in Spain. Pharmacoepidemiol. Drug Saf. 2021, 30, 1269–1278. Available online: https://pubmed.ncbi.nlm.nih.gov/34015159/ (accessed on 3 April 2022). [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Comparison Cohort N = 412,740 | Pregnancy Cohort N = 103,185 |
|---|---|---|
| During pregnancy | ||
| Cases, n | 8063 | 3522 |
| Total person-months | 3,291,191 | 821,374 |
| Months (median) | 9.3 (8.7–9.4) | 9.3 (8.6–9.4) |
| Incidence rate per 100 0person-ye (95% CI) | 2.44 (2.40–2.50) | 4.29 (4.15–4.43) |
| Incidence Rate Ratio (IRR) 95% CI | - | 1.76(1.69–1.83) |
| Puerperium | ||
| Cases, n | 2308 | 739 |
| Total, person-months | 542,756 | 133,495 |
| Median months | 1.4 (1.4–1.4) | 1.4 (1.4–1.4) |
| Incidence rate per 100 0person-ye (95% CI) | 4.25 (4.08–4.43) | 5.54 (5.15–5.95) |
| Incidence Rate Ratio (IRR) 95% CI | - | 1.30 (1.20–1.41) |
| After pregnancy | 370,273 | 91,244 |
| Cases, n | 14,511 | 4330 |
| Total, person-months | 2,542,165 | 634,852 |
| Median months | 5.9 (2.2–9.6) | 6 (2.3–9.7) |
| Incidence rate per 100 0person-ye (95% CI) | 5.71 (5.62–5.80) | 6.82 (6.62–7.03) |
| Incidence Rate Ratio (IRR) 95% CI | - | 1.19 (1.15–1.23) |
| Non COVID N = 504,340 | COVID N = 11,585 | ||||
|---|---|---|---|---|---|
| Comorbidities | N | % | N | % | |
| Pregnancies | 99,663 | 19.8 | 3522 | 30.4 | 1.76 (1.69–1.83) |
| Obesity | 25,512 | 5.1 | 760 | 6.6 | 1.33 (1.23–1.44) |
| Diabetes | 3615 | 0.7 | 96 | 0.8 | 1.23 (1.23–1.43) |
| HTA | 10,092 | 2.0 | 252 | 2.2 | 1.11 (0.98–1.26) |
| Asthma | 36,966 | 7.3 | 883 | 7.6 | 1.01 (0.94–1.08) |
| COPD | 417 | 0.1 | 11 | 0.1 | 1.26 (0.70–2.24) |
| Arrhythmia | 10,728 | 2.1 | 269 | 2.3 | 1.09 (0.97–1.23) |
| IHD | 1197 | 0.2 | 34 | 0.3 | 1.23 (0.88–1.72) |
| Hypothyroidism | 21,427 | 4.2 | 578 | 5.0 | 1.14 (1.05–1.24) |
| Depression | 23,779 | 4.7 | 565 | 4.9 | 1.09 (0.99–1.18) |
| Dyslipidemia | 24,602 | 4.9 | 610 | 5.3 | 1.11 (1.02–1.20) |
| HIV | 913 | 0.2 | 13 | 0.1 | 1.42 (0.89–2.25)) |
| Anemia year prior | 3850 | 0.8 | 100 | 0.9 | 1.09 (0.89–1.33) |
| Psoriasis | 509 | 0.1 | 6 | 0.1 | 0.51 (0.23–1.14) |
| Migraine | 19,605 | 3.9 | 517 | 4.5 | 1.14 (1.04–1.25) |
| Epilepsy | 3309 | 0.7 | 78 | 0.7 | 1.06 (0.85–1.32) |
| Gastritis | 25,089 | 5.0 | 626 | 5.4 | 1.07 (0.99–1.16) |
| Celiac | 2206 | 0.4 | 57 | 0.5 | 1.13 (0.87–1.47) |
| Rheumatoid Arthritis | 963 | 0.2 | 22 | 0.2 | 1.02 (0.67–1.55) |
| Multiple Sclerosis | 1076 | 0.2 | 19 | 0.2 | 0.84 (0.54–1.33) |
| Cancer | 2608 | 0.5 | 71 | 0.6 | 1.28 (1.01–1.61) |
| Stroke | 306 | 0.1 | 9 | 0.1 | 1.39 (0.72–2.67) |
| TIA | 99 | 0.0 | 4 | 0.0 | 1.66 (0.62–4.42) |
| Valvopathy | 673 | 0.1 | 14 | 0.1 | 0.95 (0.56–1.60) |
| Non COVID N = 504,340 | COVID N = 11,585 | ||||
|---|---|---|---|---|---|
| Treatment Pre-Pregnancy | N | % | N | % | |
| NSAIDs | 51,238 | 10.2 | 1334 | 11.5 | 1.11 (1.05–1.18) |
| Heparin | 1380 | 0.3 | 43 | 0.4 | 1.24 (0.92–1.68) |
| Antihypertensives | 175 | 0.0 | 6 | 0.1 | 1.27 (0.57–2.84) |
| Diuretics | 829 | 0.2 | 12 | 0.1 | 0.65 (0.37–1.15) |
| Calcium antagonists | 584 | 0.1 | 14 | 0.1 | 1.05 (0.62–1.80) |
| ARBs | 1326 | 0.3 | 26 | 0.2 | 0.89 (0.60–1.32) |
| ACEIs | 1607 | 0.3 | 30 | 0.3 | 0.79 (0.55–1.15) |
| Antiplatelets | 1619 | 0.3 | 50 | 0.4 | 1.26 (0.96–1.67) |
| Aspirin | 1584 | 0.3 | 50 | 0.4 | 1.29 (0.98–1.71) |
| Beta Blockers | 1861 | 0.4 | 43 | 0.4 | 1.07 (0.79–1.44) |
| PPIs | 17,502 | 3.5 | 508 | 4.4 | 1.30 (1.19–1.42) |
| H2 ANTAGONISTS | 1345 | 0.3 | 21 | 0.2 | 0.59 (0.38–0.90) |
| Antacids | 67 | 0.0 | 1 | 0.0 | 0.67 (0.09–4.77) |
| Vit K Antagonists | 333 | 0.1 | 5 | 0.0 | 0.75 (0.31–1.81) |
| Phenytoin | 30 | 0.0 | 3 | 0.0 | 4.34 (1.40–13.46) |
| Valproic acid | 719 | 0.1 | 18 | 0.2 | 1.22 (0.77–1.94) |
| Antibiotics | 38,542 | 7.6 | 1059 | 9.1 | 1.11 (1.04–1.19) |
| Respiratory drugs | 35,742 | 7.1 | 895 | 7.7 | 1.07 (0.99–1.14) |
| Opioids | 12,380 | 2.5 | 337 | 2.9 | 1.15 (1.03–1.28) |
| Migraines | 4009 | 0.8 | 100 | 0.9 | 1.14 (1.04–1.25) |
| Antiepileptics | 7202 | 1.4 | 159 | 1.4 | 1.04 (0.89–1.22) |
| Anxiolytics | 21,977 | 4.4 | 495 | 4.3 | 1.04 (0.95–1.14) |
| Allergy | 27,337 | 5.4 | 671 | 5.8 | 1.04 (0.96–1.12) |
| BZD | 22,827 | 4.5 | 523 | 4.5 | 1.07 (0.97–1.16) |
| Antidepressants | 14,054 | 2.8 | 332 | 2.9 | 1.10 (0.99–1.23) |
| SSRIs | 11,939 | 2.4 | 279 | 2.4 | 1.09 (0.97–1.23) |
| Insulin | 1593 | 0.3 | 37 | 0.3 | 0.83 (0.55–1.23) |
| Oral antidiabetics | 2078 | 0.4 | 64 | 0.6 | 1.21 (0.93–1.58) |
| Statins | 2226 | 0.4 | 66 | 0.6 | 1.42 (1.11–1.82) |
| Paracetamol | 22,448 | 4.5 | 637 | 5.5 | 1.18 (1.09–1.27) |
| Corticosteroids | 5163 | 1.0 | 146 | 1.3 | 1.18 (1.00–1.39) |
| Thyroid hormones | 14,312 | 2.8 | 354 | 3.1 | 1.04 (0.93–1.15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mota, M.; Huerta-Álvarez, C.; Llorente, A.; Cea-Soriano, L. The Risk of SARS-CoV-2 Infection in Pregnant Women: An Observational Cohort Study Using the BIFAP Database. Healthcare 2022, 10, 2429. https://doi.org/10.3390/healthcare10122429
Mota M, Huerta-Álvarez C, Llorente A, Cea-Soriano L. The Risk of SARS-CoV-2 Infection in Pregnant Women: An Observational Cohort Study Using the BIFAP Database. Healthcare. 2022; 10(12):2429. https://doi.org/10.3390/healthcare10122429
Chicago/Turabian StyleMota, Mercedes, Consuelo Huerta-Álvarez, Ana Llorente, and Lucia Cea-Soriano. 2022. "The Risk of SARS-CoV-2 Infection in Pregnant Women: An Observational Cohort Study Using the BIFAP Database" Healthcare 10, no. 12: 2429. https://doi.org/10.3390/healthcare10122429