
Efficacy of Injury Prevention Using Functional Movement Screen Training in High-School Baseball Players: Secondary Outcomes of a Randomized Controlled Trial
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Questionnaire
2.5. Outcomes
2.5.1. Players Record
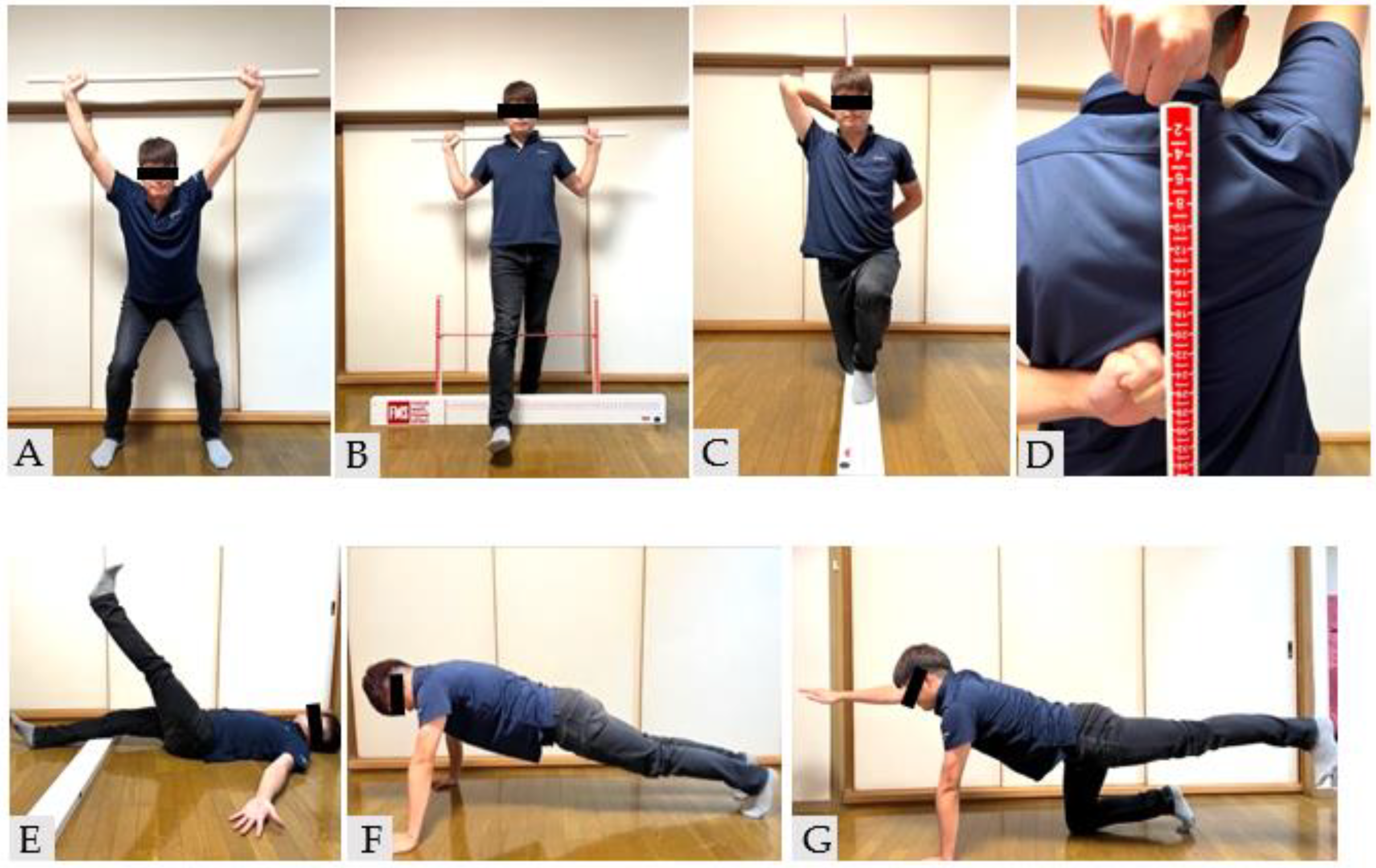
2.5.2. FMS
2.6. Intervention
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
3.1. Primary Outcome
3.1.1. Number of Injuries
3.1.2. RR and Lost Time to Injuries
3.1.3. Ancillary Analysis
3.2. Secondary Outcome
FMS Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleisig, G.S.; Barrentine, S.W.; Escamilla, R.F.; Andrews, J.R. Biomechanics of Overhand Throwing with Implications for Injuries. Sport. Med. 1996, 21, 421–437. [Google Scholar] [CrossRef] [PubMed]
- Saper, M.G.; Pierpoint, L.A.; Liu, W.; Comstock, R.D.; Polousky, J.D.; Andrews, J.R. Epidemiology of Shoulder and Elbow Injuries Among United States High School Baseball Players: School Years 2005–2006 Through 2014–2015. Am. J. Sport. Med. 2018, 46, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, J.; Nakamura, E.; Suzukawa, M.; Akaike, A.; Shimizu, K. Physical Risk Factors for a Medial Elbow Injury in Junior Baseball Players: A Prospective Cohort Study of 353 Players. Am. J. Sport. Med. 2017, 45, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Takagishi, K.; Matsuura, T.; Masatomi, T.; Chosa, E.; Tajika, T.; Iwama, T.; Watanabe, M.; Otani, T.; Inagaki, K.; Ikegami, H.; et al. Shoulder and Elbow Pain in Junior High School Baseball Players: Results of a Nationwide Survey. J. Orthop. Sci. 2019, 24, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Nakata, H.; Nagami, T.; Higuchi, T.; Sakamoto, K.; Kanosue, K. Relationship Between Performance Variables and Baseball Ability in Youth Baseball Players. J. Strength Cond. Res. 2013, 27, 2887–2897. [Google Scholar] [CrossRef] [PubMed]
- Aguinaldo, A.L.; Chambers, H. Correlation of Throwing Mechanics With Elbow Valgus Load in Adult Baseball Pitchers. Am. J. Sport. Med. 2009, 37, 2043–2048. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, A.M.W.; McKenzie, C.S.; Pan, X.; Oñate, J.A. Lumbopelvic Control and Days Missed Because of Injury in Professional Baseball Pitchers. Am. J. Sport. Med. 2014, 42, 2734–2740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M. Functional Movement Screening: The Use of Fundamental Movements as an Assessment of Function—Part 1. Int. J. Sport. Phys. Ther. 2014, 9, 396–409. [Google Scholar]
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M. Functional Movement Screening: The Use of Fundamental Movements as an Assessment of Function—Part 2. Int. J. Sport. Phys. Ther. 2014, 9, 549–563. [Google Scholar] [PubMed]
- Garrison, M.; Westrick, R.; Johnson, M.R.; Benenson, J. Association between the Functional Movement Screen and Injury Development in College Athletes. Int. J. Sport. Phys. Ther. 2015, 10, 21–28. [Google Scholar] [PubMed]
- Kiesel, K.; Plisky, P.J.; Voight, M.L. Can Serious Injury in Professional Football Be Predicted by a Preseason Functional Movement Screen? N. Am. J. Sport. Phys. Ther. 2007, 2, 147–158. [Google Scholar]
- Kiesel, K.; Plisky, P.; Butler, R. Functional Movement Test Scores Improve Following a Standardized Off-Season Intervention Program in Professional Football Players. Scand J. Med. Sci. Sport. 2011, 21, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Chorba, R.S.; Chorba, D.J.; Bouillon, L.E.; Overmyer, C.A.; Landis, J.A. Use of a Functional Movement Screening Tool to Determine Injury Risk in Female Collegiate Athletes. N. Am. J. Sport. Phys. Ther. 2010, 5, 47–54. [Google Scholar] [PubMed]
- Moran, R.W.; Schneiders, A.G.; Major, K.M.; Sullivan, S.J. How Reliable Are Functional Movement Screening Scores? A Systematic Review of Rater Reliability. Br. J. Sport. Med. 2016, 50, 527–536. [Google Scholar] [CrossRef]
- Bonazza, N.A.; Smuin, D.; Onks, C.A.; Silvis, M.L.; Dhawan, A. Reliability, Validity, and Injury Predictive Value of the Functional Movement Screen: A Systematic Review and Meta-Analysis. Am. J. Sport. Med. 2017, 45, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Leland, D.P.; Conte, S.; Flynn, N.; Conte, N.; Crenshaw, K.; Wilk, K.E.; Camp, C.L. Prevalence of Medial Ulnar Collateral Ligament Surgery in 6135 Current Professional Baseball Players: A 2018 Update. Orthop. J. Sport. Med. 2019, 7, 2325967119871442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camp, C.L.; Dines, J.S.; van der List, J.P.; Conte, S.; Conway, J.; Altchek, D.W.; Coleman, S.H.; Pearle, A.D. Summative Report on Time Out of Play for Major and Minor League Baseball: An Analysis of 49,955 Injuries From 2011 Through 2016. Am. J. Sport. Med. 2018, 46, 1727–1732. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Otoshi, K.-I.; Tominaga, R.; Kaga, T.; Igari, T.; Sato, R.; Konno, S.-I. Influences of Limited Flexibility of the Lower Extremities and Occurrence of Low Back Pain in Adolescent Baseball Players: A Prospective Cohort Study. J. Orthop. Sci. 2022, 27, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Akasaka, K.; Otsudo, T.; Sawada, Y.; Hattori, H.; Hasebe, Y.; Mizoguchi, Y.; Hall, T.M.; Yamamoto, M. Effects of Functional Movement Screen Training in High-School Baseball Players: A Randomized Controlled Clinical Trial. Medicine 2021, 100, e25423. [Google Scholar] [CrossRef] [PubMed]
- Kerr, Z.Y.; Lynall, R.C.; Roos, K.G.; Dalton, S.L.; Djoko, A.; Dompier, T.P. Descriptive Epidemiology of Non–Time-Loss Injuries in Collegiate and High School Student-Athletes. J. Athl. Train. 2017, 52, 446–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, J.; Nakamura, E.; Suzuki, T.; Suzukawa, M.; Akeda, M.; Yamazaki, T.; Ellenbecker, T.S.; Hirose, N. Throwing Injuries in Youth Baseball Players: Can a Prevention Program Help? A Randomized Controlled Trial. Am. J. Sport. Med. 2019, 47, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- Matsel, K.A.; Butler, R.J.; Malone, T.R.; Hoch, M.C.; Westgate, P.M.; Uhl, T.L. Current Concepts in Arm Care Exercise Programs and Injury Risk Reduction in Adolescent Baseball Players: A Clinical Review. Sport. Health A Multidiscip. Approach 2021, 13, 245–250. [Google Scholar] [CrossRef]
- Duke, S.R.; Martin, S.E.; Gaul, C.A. Preseason Functional Movement Screen Predicts Risk of Time-Loss Injury in Experienced Male Rugby Union Athletes. J. Strength Cond. Res. 2017, 31, 2740–2747. [Google Scholar] [CrossRef] [PubMed]
- Knowles, S.B.; Marshall, S.W.; Miller, T.; Spicer, R.; Bowling, J.M.; Loomis, D.; Millikan, R.W.; Yang, J.; Mueller, F.O. Cost of Injuries from a Prospective Cohort Study of North Carolina High School Athletes. Inj. Prev. 2007, 13, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Bodden, J.G.; Needham, R.A.; Chockalingam, N. The Effect of an Intervention Program on Functional Movement Screen Test Scores in Mixed Martial Arts Athletes. J. Strength Cond. Res. 2015, 29, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Campa, F.; Spiga, F.; Toselli, S. The Effect of a 20-Week Corrective Exercise Program on Functional Movement Patterns in Youth Elite Male Soccer Players. J. Sport Rehabil. 2019, 28, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Kovac, D.; Krkeljas, Z.; Venter, R. Effect of Six-Week Traditional Resistance and Functional Training on Functional Performance in Female Netball Players. BMC Sport. Sci. Med. Rehabil. 2022, 14, 10. [Google Scholar] [CrossRef]
- Dinc, E.; Kilinc, B.E.; Bulat, M.; Erten, Y.T.; Bayraktar, B. Effects of Special Exercise Programs on Functional Movement Screen Scores and Injury Prevention in Preprofessional Young Football Players. J. Exerc. Rehabil. 2017, 13, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Song, H.-S.; Woo, S.-S.; So, W.-Y.; Kim, K.-J.; Lee, J.; Kim, J.-Y. Effects of 16-Week Functional Movement Screen Training Program on Strength and Flexibility of Elite High School Baseball Players. J. Exerc. Rehabil. 2014, 10, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Dick, R.; Sauers, E.L.; Agel, J.; Keuter, G.; Marshall, S.W.; McCarty, K.; McFarland, E. Descriptive Epidemiology of Collegiate Men’s Baseball Injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J. Athl. Train. 2007, 42, 183–193. [Google Scholar]


{kind=link}
| Intervention (n = 37) | Control (n = 34) | p-Value | 1−β | ||
|---|---|---|---|---|---|
| Age (years) | 16.0 ± 0.1 (15–17) | 15.8 ± 0.1 (15–17) | 0.17 | 1.00 | |
| Height (cm) | 169.3 ± 0.9 (156–181) | 169.7 ± 1.0 (158.6–179) | 0.76 | 0.399 | |
| Body weight (kg) | 63.5 ± 1.4 (43–84) | 62.1 ± 1.2 (49–80) | 0.41 | 0.99 | |
| Body mass index | 22.1 (17.7–28.7) | 21.5 (18.1–26.1) | 0.27 | 0.18 | |
| Experience as a baseball player (years) | 7.7 ± 0.3 (2–10) | 7.3 ± 0.3 (3–10) | 0.37 | 0.99 | |
| Dominant hand (n) | Right/left | 34/3 | 28/6 | 0.29 | 0.66 |
| Position (n) | Pitcher | 6 | 9 | 0.38 | 0.38 |
| Catcher | 3 | 4 | 0.70 | 0.09 | |
| Infielder | 16 | 14 | 1.00 | 0.06 | |
| Outfielder | 12 | 7 | 0.29 | 0.34 | |
| mean ± SD (min–max) |
| None | Number of Injuries (n) | Lost Time (h) | Injury Rate RR (95% CI) | p-Value | 1 − β | |
|---|---|---|---|---|---|---|
| [0–12 weeks] | ||||||
| All injuries | ||||||
| Intervention | 32 | 5 | 72.5 | 0.98 (0.82–1.17) | 0.83 | 0.08 |
| Control | 30 | 4 | 111 | |||
| Noncontact | ||||||
| Intervention | 34 | 3 | 56.5 | 0.98 (0.86–1.11) | 0.71 | 0.11 |
| Control | 32 | 2 | 33 | |||
| [12–24 weeks] | ||||||
| All injuries | ||||||
| Intervention | 34 | 3 | 113 | 1.36 (1.06–1.75) | 0.01 | 0.99 |
| Control | 23 | 11 | 332.5 | |||
| Noncontact | ||||||
| Intervention | 34 | 3 | 113 | 1.30 (1.03–1.65) | 0.02 | 0.99 |
| Control | 24 | 10 | 325.5 | |||
| Intervention (n) | Control (n) | |||
|---|---|---|---|---|
| Contact | Noncontact | Contact | Noncontact | |
| [0–12 weeks] | ||||
| Fracture | 1 | 1 | ||
| Lumber | 1 | 1 | ||
| Shoulder | 1 | 1 | 1 | |
| Ankle | 1 | 1 | ||
| [12–24 weeks] | ||||
| Lumber | 5 | |||
| Shoulder | 3 | 1 | 5 | |
| Group | Before the Intervention | After 12 Weeks | After 24 Weeks | |
|---|---|---|---|---|
| Total FMS score | Intervention | 13.7 ± 2.6 (8–18) | 17.5 ± 1.5 (13–20) a,b,c | 15.3 ± 2.3 (9–19) b |
| Control | 13.8 ± 2.7 (8–18) | 14.7 ± 2.3 (9–18) b | 15.5 ± 1.6 (12–18) b | |
| Deep squat | Intervention | 2 (0–3) | 2 (2–3) b | 2 (1–3) |
| Control | 2 (0–3) | 2 (0–3) | 2 (0–3) | |
| Hurdle step | Intervention | 3 (1–3) | 3 (1–3) a,b,c | 2 (1–3) |
| Control | 2 (1–3) | 2 (1–3) | 2 (1–3) | |
| Inline lunge | Intervention | 3 (1–3) | 3 (2–3) a,b,c | 3 (1–3) |
| Control | 3 (0–3) | 2.5 (1–3) | 2 (1–3) | |
| Shoulder mobility | Intervention | 3 (1–3) | 3 (1–3) | 3 (1–3) |
| Control | 3 (1–3) | 3 (1–3) | 3 (1–3) | |
| Active straight leg raise | Intervention | 2 (1–3) | 2 (2–3) a,b,c | 2 (1–3) b |
| Control | 2 (1–3) | 2 (0–3) b | 2 (1–3) b | |
| Trunk stability push up | Intervention | 2 (0–3) | 3 (2–3) a,b,c | 2 (0–3) |
| Control | 2 (0–3) | 2 (1–3) | 2 (1–3) | |
| Rotary stability | Intervention | 2 (0–3) | 2 (2–2) b | 2 (1–3) |
| Control | 2 (1–2) | 2 (1–2) b | 2 (1–2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, K.; Mizoguchi, Y.; Kimura, F.; Sawada, Y.; Akasaka, K. Efficacy of Injury Prevention Using Functional Movement Screen Training in High-School Baseball Players: Secondary Outcomes of a Randomized Controlled Trial. Healthcare 2022, 10, 2409. https://doi.org/10.3390/healthcare10122409
Suzuki K, Mizoguchi Y, Kimura F, Sawada Y, Akasaka K. Efficacy of Injury Prevention Using Functional Movement Screen Training in High-School Baseball Players: Secondary Outcomes of a Randomized Controlled Trial. Healthcare. 2022; 10(12):2409. https://doi.org/10.3390/healthcare10122409
Chicago/Turabian StyleSuzuki, Kenta, Yasuaki Mizoguchi, Fumihiko Kimura, Yutaka Sawada, and Kiyokazu Akasaka. 2022. "Efficacy of Injury Prevention Using Functional Movement Screen Training in High-School Baseball Players: Secondary Outcomes of a Randomized Controlled Trial" Healthcare 10, no. 12: 2409. https://doi.org/10.3390/healthcare10122409